Using Plasma Autoantibodies of Central Nervous System Proteins to Distinguish Veterans with Gulf War Illness from Healthy and Symptomatic Controls

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Procedures
2.3. Calculations
2.4. Neurodegeneration Index (NDI)
2.5. Statistical Methodology
3. Results
3.1. Specificity of Serum Autoantibodies
3.2. Participant Demographics
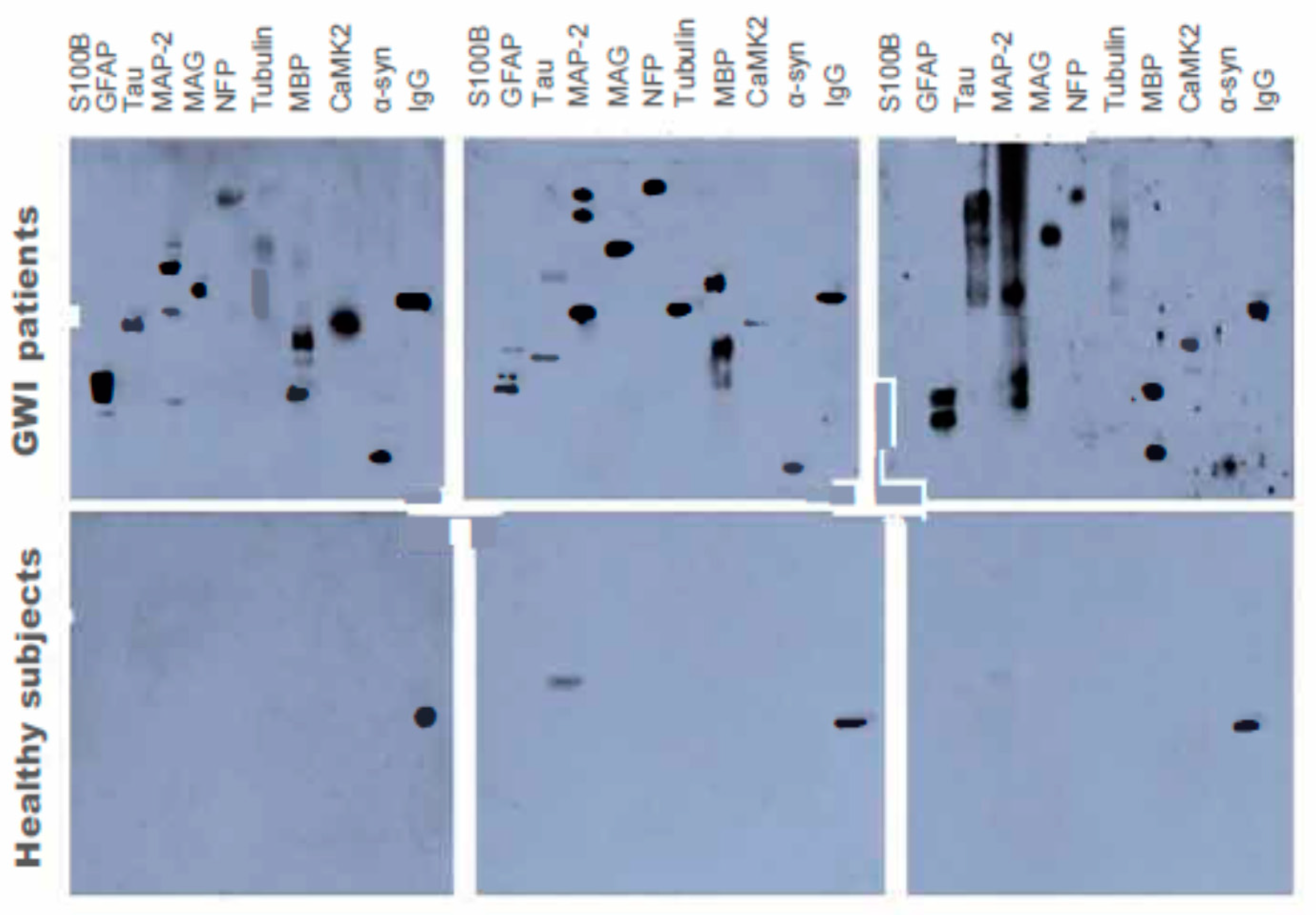
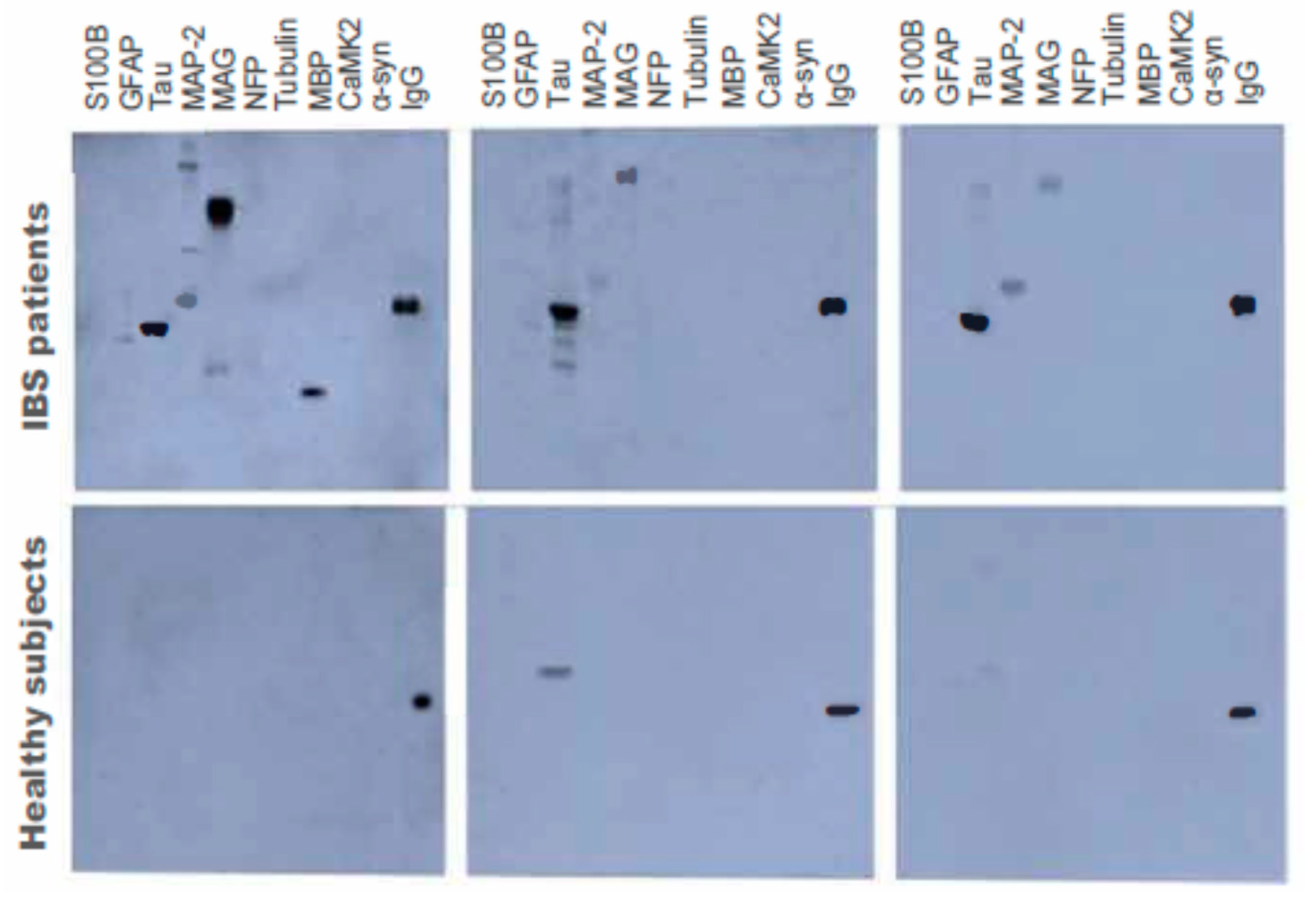
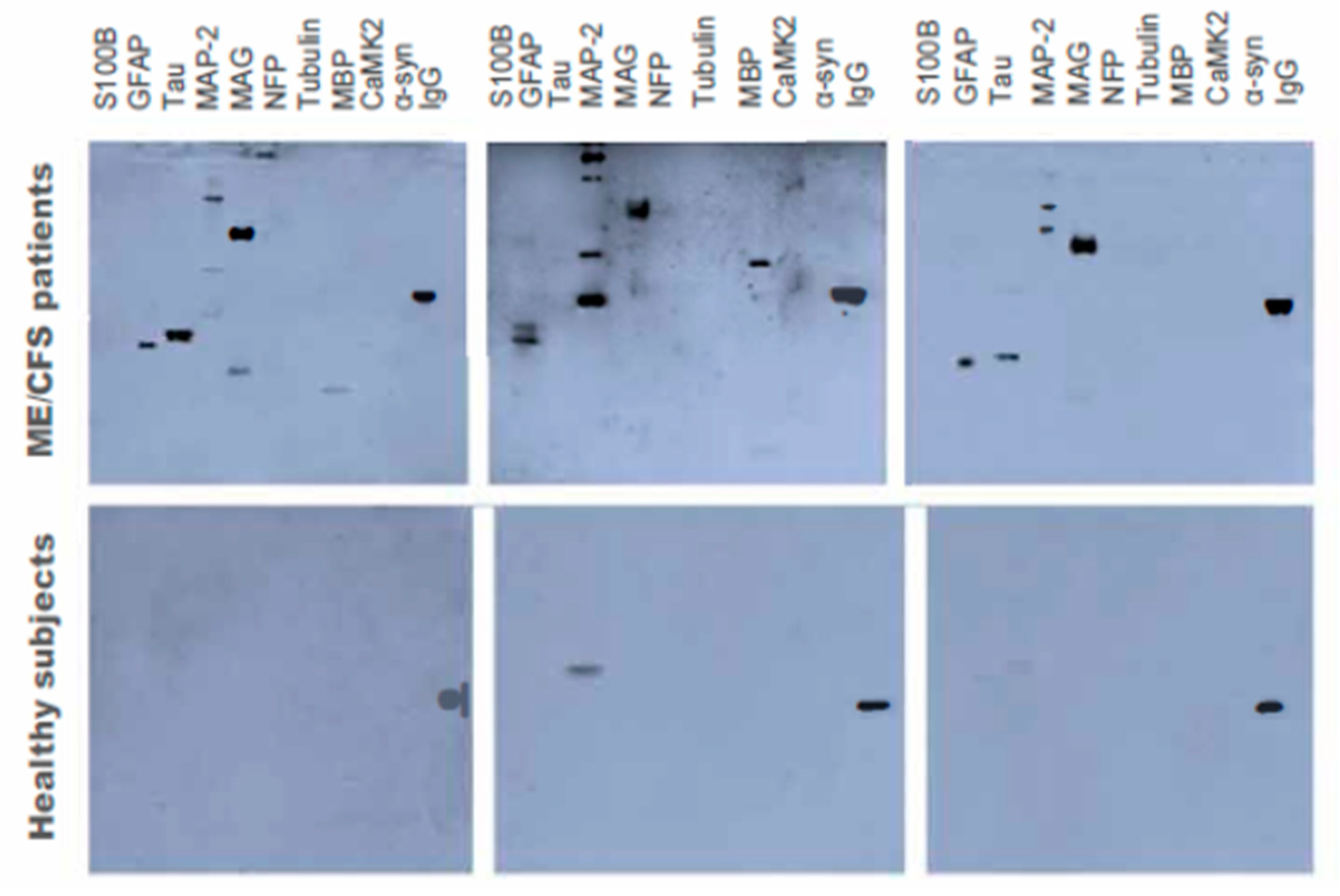
3.3. Autoantibody Levels for Neuronal and Glial Proteins using Western Blot
3.4. Neurodegeneration Index (NDI)
4. Discussion
Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kang, H.K.; Li, B.; Mahan, C.M.; Eisen, S.A.; Engel, C.C. Health of US veterans of 1991 Gulf War: A follow-up survey in 10 years. J. Occup. Environ. Med. 2009, 51, 401–410. [Google Scholar] [CrossRef]
- RAC-GWVI (Research Advisory Committee on Gulf War Veterans’ Illnesses). Gulf War Illness and the Health of Gulf War Veterans; U.S. Government Printing Office: Washington, DC, USA, 2008.
- Proctor, S.P.; Heeren, T.; White, R.F.; Wolfe, J.; Borgos, M.S.; Davis, J.D.; Pepper, L.; Clapp, R.; Sutker, P.B.; Vasterling, J.J.; et al. Health status of Persian Gulf War veterans: Self-reported symptoms, environmental exposures and the effect of stress. Int. J. Epidemiol. 1998, 6, 1000–1010. [Google Scholar] [CrossRef]
- Janulewicz, P.; Krengel, M.; Quinn, E.; Heeren, T.; Toomey, R.; Killiany, R.; Zundel, C.; Ajama, J.; O’Callaghan, J.; Steele, L.; et al. The Multiple Hit Hypothesis for Gulf War Illness: Self-Reported Chemical/Biological Weapons Exposure and Mild Traumatic Brain Injury. Brain Sci. 2018, 8, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Smylie, A.L.; Broderick, G.; Fernandes, H.; Razdan, S.; Barnes, Z.; Collado, F.; Sol, C.; Fletcher, M.A.; Klimas, N. A comparison of sex-specific immune signatures in Gulf War illness and chronic fatigue syndrome. BMC Immunol. 2013, 14, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayhan, R.U.; Ravindran, M.K.; Baraniuk, J.N. Migraine in gulf war illness and chronic fatigue syndrome: Prevalence, potential mechanisms, and evaluation. Front. Physiol. 2013, 4, 181. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Zhou, X.D.; Denny, T.; Ottenweller, J.E.; Lange, G.; LaManca, J.J.; Lavietes, M.H.; Pollet, C.; Gause, W.C.; Natelson, B.H. Changes in immune parameters seen in Gulf War veterans but not in civilians with chronic fatigue syndrome. Clin. Diagn. Lab. Immunol. 1999, 6, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Rayhan, R.U.; Stevens, B.W.; Raksit, M.P.; Ripple, J.A.; Timbol, C.R.; Adewuyi, O.; VanMeter, J.W.; Baraniuk, J.N. Exercise challenge in Gulf War Illness reveals two subgroups with altered brain structure and function. PLoS ONE 2013, 8, e63903. [Google Scholar] [CrossRef]
- Butterick, T.A.; Trembley, J.H.; Hocum Stone, L.L.; Muller, C.J.; Rudquist, R.R.; Bach, R.R. Gulf War Illness-associated increases in blood levels of interleukin 6 and C-reactive protein: Biomarker evidence of inflammation. BMC Res. Notes 2019, 12, 816. [Google Scholar] [CrossRef]
- Johnson, G.J.; Slater, B.C.; Leis, L.A.; Rector, T.S.; Bach, R.R. Blood Biomarkers of Chronic Inflammation in Gulf War Illness. PLoS ONE 2016, 11, e0157855. [Google Scholar] [CrossRef] [Green Version]
- Abou-Donia, M.B.; Conboy, L.A.; Kokkotou, E.; Jacobson, E.; Elmasry, E.M.; Elkafrawy, P.; Neely, M.; Bass CRSullivan, K. Screening for novel central nervous system biomarkers in veterans with Gulf War Illness. Neurotoxicol. Teratol. 2017, 61, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Tuteja, A.K.; Talley, N.J.; Stoddard, G.J.; Verne, G.N. Double-Blind Placebo-Controlled Study of Rifaximin and Lactulose Hydrogen Breath Test in Gulf War Veterans with Irritable Bowel Syndrome. Randomized Control. Trial Dig. Dis. Sci. 2019, 64, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Janulewicz, P.A.; Seth, R.K.; Carlson, J.M.; Ajama, J.; Quinn, E.; Heeren, T.; Klimas, N.; Lasley, S.M.; Horner, R.D.; Sullivan, K.; et al. The Gut-Microbiome in Gulf War Veterans: A Preliminary Report. Int. J. Environ. Res. Public Health 2019, 16, 3751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimono, D.; Sarkar, S.; Albadrani, M.; Seth, R.; Bose, D.; Mondal, A.; Li, Y.; Kar, A.N.; Nagarkatti, M.; Nagarkatti, P.; et al. Dysbiosis-Associated Enteric Glial Cell Immune-Activation and Redox Imbalance Modulate Tight Junction Protein Expression in Gulf War Illness Pathology. Front. Physiol. 2019, 10, 1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keating, J.A.; Shaughnessy, C.; Baubie, K.; Kates, A.E.; Putman-Buehler, N.; Watson, L.; Dominguez NWatson, K.; Cook, D.; Rabago, D.; Suen, G.; et al. Characterising the gut microbiome in veterans with Gulf War Illness Effects of toxicant exposures during deployment. BMJ Open. 2019, 9, e031114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golomb, B.A. Acetylcholinesterase inhibitors and Gulf War illnesses. Proc. Natl. Acad. Sci. USA 2008, 105, 4295–4300. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, K.; Krengel, M.; Bradford, W.; Stone, C.; Thompson, T.; Heeren, T.; White, R.F. Neuropsychological Functioning in Military Pesticide Applicators from the Gulf War: Effects on Information Processing Speed, Attention and Visual Memory. Neurotoxicol. Teratol. 2017, 65, 1–13. [Google Scholar] [CrossRef]
- Abou-Donia, M.B.; Wilmarth, K.R.; Jensen, K.F.; Oehme, F.W.; Kurt, T.L. Neurotoxicity resulting from co-exposure to pyridostigmine bromide, DEET, and permethrin: Implications of Gulf War chemical exposures. J. Toxicol. Environ. Health 1996, 48, 35–56. [Google Scholar] [CrossRef]
- Abou-Donia, M.B.; Wilmarth, K.R.; Abdel-Rahman, A.A.; Jensen, K.W.; Oehme, F.W.; Kurt, T.L. Increased neurotoxicity following simultaneous exposure to pyridostigmine bromide, DEET, and chlorpyrifos. Fundam. Appl. Toxicol. 1996, 34, 201–220. [Google Scholar] [CrossRef]
- O’Callaghan, J.P. Assessment of neurotoxicity: Use of glial fibrillary acidic protein as a biomarker. Biomed. Environ. Sci. 1991, BES4, 197–206. [Google Scholar]
- Abou-Donia, M.B.; Abou-Donia, M.M.; ElMasry, E.M.; Monro, J.A.; Mulder, M.F. Autoantibodies to nervous system-specific proteins are elevated in sera of flight crew members: Biomarkers for nervous system injury. J. Toxicol. Environ. Health Part A 2013, 76, 363–380. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Defense. Environmental Exposure Report: Pesticides, Final Report; Office of the Special Assistant to the Undersecretary of Defense for Gulf War Illnesses, Medical Readiness, and Military Deployments: Washington, DC, USA, 2003.
- Smith, M.I.; Elvove, I.; Valaer, P.J.; Frazier, W.H.; Mallory, G.E. Pharmacologic and chemical studies of the cause of the so-called ginger paralysis. US Public Health Rep. 1930, 45, 1703–1716. [Google Scholar] [CrossRef]
- Abou-Donia, M.B. Involvement of cytoskeletal proteins in the mechanisms of organophosphorus ester-induced delayed neurotoxicity. Clin. Exp. Pharmacol. Physiol. 1995, 22, 358–359. [Google Scholar] [CrossRef] [PubMed]
- Torres-Altoro, M.I.; Mathur, B.N.; Drerup, J.M.; Thomas, R.; Lovinger, D.M.; O’Callaghan, J.P.; Bibb, J.A. Organophosphates Dysregulate Dopamine Signaling, Glutamatergic Neurotransmission, and Induce Neuronal Injury Markers in Striatum. J. Neurochem. 2011, 119, 303–313. [Google Scholar] [CrossRef]
- Belgrad, J.; Dutta, D.J.; Bromley-Coolidge, S.; Kelly, K.A.; Michalovicz, L.T.; Sullivan, K.; O’Callaghan, J.P.; Fields, R.D. Oligodendrocyte involvement in Gulf War Illness. Glia 2019, 67, 2107–2124. [Google Scholar] [CrossRef] [Green Version]
- Abou-Donia, M.B.; Lapadula, D.M.; Suwita, E. Cytoskeletal proteins as targets for organophosphorus compound and aliphatic hexacarbon-induced neurotoxicity. Toxicology 1988, 49, 469–477. [Google Scholar] [CrossRef]
- Donato, R. S100: A multigenetic family of calcium-modulated proteins of the EF-hand type with intracellular and extracellular functional roles. Int. Biochem. Cell Biol. 2001, 33, 637–668. [Google Scholar] [CrossRef]
- Zurek, J.; Fedora, M. The usefulness of S100B, NSE, GFAP, NFH, secretagogin and Hsp70 as a predetive biomarker of outcome in children with traumatic brain injury. Acta Neurochir. 2012, 154, 93–103. [Google Scholar] [CrossRef]
- Steele, L. Prevalence and patterns of Gulf War illness in Kansas veterans: Association of symptoms with characteristics of person, place, and time of military service. Am. J. Epidemiol. 2000, 152, 992–1002. [Google Scholar] [CrossRef]
- Longstreth, G.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef]
- Conboy, L.; Gerke, T.; Hsu, K.Y.; St John, M.; Goldstein, M.; Schnyer, R. The Effectiveness of Individualized Acupuncture Protocols in the Treatment of Gulf War Illness: A Pragmatic Randomized Clinical Trial. PLoS ONE 2016, 11, e0149161. [Google Scholar] [CrossRef] [Green Version]
- Conboy, L.; St John, M.; Schnyer, R. The effectiveness of acupuncture in the treatment of Gulf War Illness. Contemp. Clin. Trials 2012, 33, 557–562. [Google Scholar] [CrossRef]
- Maule, A.L.; Janulewicz, P.A.; Sullivan, K.A.; Krengel, M.H.; Yee, M.K.; McClean, M.; White, R.F. Meta-analysis of self-reported health symptoms in 1990-1991 Gulf War and Gulf War-era veterans. BMJ Open. 2018, 8, e016086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahmanyar, S.; Moreau-Dubois, M.-C.; Brown, P.; Cathala, F.; Gajdusek, D.C. Serum antibodies to neurofilament antigens in patients with neurological and other diseases and in healthy controls. J. Neuroimmun. 1983, 5, 191–196. [Google Scholar] [CrossRef]
- Chao, L.; Abadjian, H.; Lavin, J.; Meyerhoff, D.J.; Weiner, M.W. Effects of low-level sarin and cyclosarin exposure and Gulf War Illness on brain structure and function: A study at 4T. Neurotoxicology 2011, 32, 814–822. [Google Scholar] [CrossRef]
- White, R.F.; Steele, L.; O’Callaghan, J.P.; Sullivan, K.; Binns, J.H.; Golomb, B.A.; Bloom, F.E.; Bunker, J.A.; Crawford, F.; Graves, J.C.; et al. Recent research on Gulf War illness and other health problems in veterans of the 1991 Gulf War: Effects of toxicant exposures during deployment. Cortex 2016, 74, 449–475. [Google Scholar] [CrossRef] [Green Version]
- Chao, L.; Rothlind, V.A.; Cardenas, D.J.; Meyerhoff Weiner, M.W. Effects of low-level exposure to sarin and cyclosarin during the 1991 Gulf War on brain function and brain structure in US veterans. Neurotoxicology 2010, 31, 493. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Rahman, A.; Shetty, A.K.; Abou-Donia, M.B. Subchronic dermal application of N,N-diethyl m-toluamide (DEET) and permethrin to adult rats, alone or in combination, causes diffuse neuronal cell death and cytoskeletal abnormalities in the cerebral cortex and the hippocampus, and Purkinje neuron loss in the cerebellum. Exp. Neurol. 2001, 172, 153–171. [Google Scholar]
- Abou-Donia, M.B. Organophosphorus ester-induced chronic neurotoxicity. Arch. Environ. Health 2003, 58, 484–497. [Google Scholar] [CrossRef]
- Naughton, S.X.; Beck, W.D.; Wei, Z.; Wu, G.; Terry, A.V., Jr. Multifunctional compounds lithium chloride and methylene Blue attenuate the negative effects of diisopropylfluorophosphate on axonal transport in rat cortical neurons. Toxicology 2020, 431, 152379. [Google Scholar] [CrossRef]
- Naughton, S.X.; Terry, A.V., Jr. Neurotoxicity in acute and repeated organophosphate exposure. Toxicology 2018, 408, 101–112. [Google Scholar] [CrossRef]
- Naughton, S.X.; Hernandez, C.M.; Beck, W.D.; Poddar, I.; Yanasak, N.; Lin, P.C.; Terry, A.V., Jr. Repeated exposures to diisopropylfluorophosphate result in structural disruptions of myelinated axons and persistent impairments of axonal transport in the brains of rats. Toxicology 2018, 406, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Naughton, S.X.; Beck, W.D.; Hernandez, C.M.; Wu, G.; Wei, Z.; Yang, X.; Bartlett, M.G.; Terry, A.V., Jr. Chlorpyrifos and chlorpyrifos oxon impair the transport of membrane bound organelles in rat cortical axons. Neurotoxicology 2017, 62, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Reneman, L.; Schagen, S.; Mulder, M.; Mulsaerts, H.J.H.; Hageman, G.; de Ruiter, M.B. Cognitive impairment and associated loss in brain white microstructure in aircrew members exposed to engine oil fumes. Brain Immag. Behav. 2016, 10, 417–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshelh, Z.; Albrecht, D.S.; Bergan, C.; Akeju, O.; Clauw, D.J.; Conboy, L.; Edwards, R.R.; Kim, M.; Lee, Y.; Protsenko, E.; et al. In-vivo imaging of neuroinflammation in Veterans with Gulf War Illness. Brain Behav. Immun. 2020, 87, 498–507. [Google Scholar] [CrossRef]
- Elkon, K.; Casali, P. Nature and functions of autoantibodies. Nat. Clin. Pract. Rheumatol. 2008, 4, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Terry, A.V., Jr. Functional consequences of repeated organophosphate exposure: Potential non-cholinergic mechanisms. Pharmacol. Ther. 2012, 134, 355–365. [Google Scholar] [CrossRef] [Green Version]
- Wirth, K.; Scheibenbogen, C. A Unifying Hypothesis of the Pathophysiology of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/ME/CFS): Recognitions from the finding of autoantibodies against ß2-adrenergic receptors. Autoimmun. Rev. 2020, 19, 102527. [Google Scholar] [CrossRef]
- Giannoccaro, M.P.; Cossins, J.; Sørland, K.; Fluge, Ø.; Vincent, A. Searching for Serum Antibodies to Neuronal Proteins in Patients With Myalgic Encephalopathy/Chronic Fatigue Syndrome. Clin. Ther. 2019, 41, 836–847. [Google Scholar] [CrossRef] [Green Version]
- Qiang, L.; Rao, A.N.; Mostoslavsky, G.; James, M.F.; Comfort, N.; Sullivan, K.; Baas, P.W. Reprogramming cells from Gulf War veterans into neurons to study Gulf War illness. Neurology 2017, 88, 1968–1975. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, C.M.; Beck, W.D.; Naughton, S.X.; Poddar, I.; Adam, B.L.; Yanasak, N.; Middleton, C.; Terry, A.V., Jr. Repeated exposure to chlorpyrifos leads to prolonged impairments of axonal transport in the living rodent brain. Neurotoxicology 2015, 47, 17–26. [Google Scholar] [CrossRef]
- Rao, A.N.; Patil, A.; Brodnik, Z.D.; Qiang, L.; España, R.A.; Sullivan, K.A.; Black, M.M.; Baas, P.W. Pharmacologically increasing microtubule acetylation corrects stress-exacerbated effects of organophosphates on neurons. Traffic 2017, 18, 433–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, U.; Pearson, A.; Evans, J.E.; Langlois, H.; Saltiel, N.; Ojo, J.; Klimas, N.; Sullivan, K.; Keegan, A.P.; Oberlin, S.; et al. A permethrin metabolite is associated with adaptive immune responses in Gulf War Illness. Brain Behav. Immun. 2019, 81, 545–559. [Google Scholar] [CrossRef] [PubMed]
- Hokama, Y.; Empey-Campora, C.; Hara, C.; Higa, N.; Siu, N.; Lau, R.; Kuribayashi, T.; Yabusaki, K. Acute phase phospholipids related to the cardiolipin of mitochondria in the sera of patients with chronic fatigue syndrome (ME/CFS), chronic Ciguatera fish poisoning (CCFP), and other diseases attributed to chemicals, Gulf War, and marine toxins. J. Clin. Lab. Anal. 2008, 22, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Vojdani, A.; Thrasher, J.D. Cellular and humoral immune abnormalities in Gulf War veterans. Environ. Health Perspect. 2004, 112, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Skowera, A.; Stewart, E.; Davis, E.T.; Cleare, A.J.; Unwin, C.; Hull, L.; Ismail, K.; Hossain, G.; Wessely, S.C.; Peakman, M. Antinuclear autoantibodies (ANA) in Gulf War-related illness and chronic fatigue syndrome (ME/CFS) patients. Clin. Exp. Immunol. 2002, 129, 354–358. [Google Scholar] [CrossRef]
- Bowyer, J.F.; Sarkar, S.; Burks, S.M.; Hess, J.N.; Tolani, S.; O’Callaghan, J.P.; Hanig, J.P. Microglial activation and responses to vasculature that result from an acute LPS exposure. Neurotoxicology 2020, 77, 181–192. [Google Scholar] [CrossRef]
- Abdel-Rahman, A.; Shetty, A.K.; Abou-Donia, M.B. Acute exposure to sarin increases blood brain barrier permeability and induces neuropathological changes in the rat brain: Dose response relationship. Neuroscience 2002, 113, 721–741. [Google Scholar] [CrossRef]
- Abdel-Rahman, H.A.; Salama, M.; Seham, A.; El-Hak, G.; El-Harouny, M.A.; ElKafrawy, P.; Abou-Donia, M.B. A Panel of Autoantibodies Against Neural Proteins as Peripheral Biomarker for Pesticide-Induced. Neurotox. Res. 2018, 33, 316–336. [Google Scholar] [CrossRef]
- Salama, M.; Shalash, A.; Magdy, A.; Makar, M.; Roushdy, T.; Elbalkimy, M.; Elrassas, H.; Elkafrawy, P.; Mohamed, W.; Abou Donia, M.B. Tubulin and Tau: Possible targets for diagnosis of Parkinson’s and Alzheimer’s diseases. PLoS ONE 2018, 13, e0196436. [Google Scholar] [CrossRef]
- Zundel, C.G.; Krengel, M.H.; Heeren, T.; Yee, M.K.; Grasso, C.M.; Lloyd, P.A.J.; Coughlin, S.S.; Sullivan, K. Rates of Chronic Medical Conditions in 1991 Gulf War Veterans Compared to the General Population. Int. J. Environ. Res. Public Health 2019, 16, 949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, L. Do Gulf War veterans with high levels of deployment-related exposures display symptoms suggestive of Parkinson’s disease? Int. J. Occup. Med. Environ. Health 2019, 32, 503–526. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | GWI Cases | GW Healthy Controls | IBS Controls | ME/CFS Controls |
|---|---|---|---|---|
| N | 175 | 60 | 37 | 50 |
| Age * (Mean ± SD) | 48.7 ± 7.8 | 50.92 ± 7.48 | 39.40 ± 13.93 | 46.74 ± 10.24 |
| Sex * | ||||
| Male (%) | 80.2% | 93.3% | 8.6% | 10% |
| Female (%) | 19.8% | 6.7% | 91.4% | 90% |
| Race * | ||||
| Caucasian (%) | 81.3% | 73.7% | 85.7% | 91.3% |
| African American (%) | 12.9% | 23% | 8.6% | 8.7% |
| Other/Multiracial (%) | 5.8% | 3.3% | 5.7% | 0.0% |
| GWI vs. All Controls | GWI vs. GW Controls | GWI vs. IBS Controls | GWI vs. ME/CFS Controls | ||
|---|---|---|---|---|---|
| A. Neuronal Proteins | |||||
| Neurofilament Triplet | Mean (SE) | 3.42 (0.19) *** | 1.88 (0.26) *** | 0.86 (0.02) *** | 1.18 (0.05) *** |
| Proteins (NFP) | Range | 2.6–15.15 | 0.16–9.74 | 0.64–1.23 | 0.51–2.25 |
| Tubulin | Mean (SE) | 4.13 (0.25) *** | 2.36 (0.30) *** | 1.14 (0.03) *** | 2.71 (0.24) ** |
| Range | 0.32–15.15 | 0.09–10.76 | 0.62–15.36 | 0.63–7.39 | |
| Microtubule Associated Protein Tau (Tau) | Mean (SE) | 2.92 (0.22) *** | 1.57 (0.17) *** | 1.24 (0.13) *** | 1.02 (0.07) *** |
| Range | 0.33–10.55 | 0.34–5.13 | 0.52–4.11 | 0.40–3.36 | |
| Microtubule Associated Protein-2 (MAP-2) | Mean (SE) | 9.66 (0.73) *** | 5.04 (0.76) *** | 1.05 (0.07) *** | 6.97 (0.35) ** |
| Range | 0.88–27.42 | 0.24–23.00 | 0.64–2.45 | 1.40–14.02 | |
| Calcium/Calmodulin | Mean (SE) | 2.04 (0.15) *** | 1.20 (0.13) *** | 0.70 (0.03) *** | 1.16 (0.05) *** |
| Kinase 2 (CaMKII) | Range | 0.10–5.50 | 0.15–4.50 | 0.37–1.43 | 1.11–1.92 |
| Alpha Synuclein (α-syn) | Mean (SE) | 2.52 (0.19) *** | 1.46 (0.02) *** | 0.78 (0.06) *** | 1.13 (0.05) *** |
| Range | 0.17–11.77 | 0.37–6.45 | 0.51–1.93 | 0.41–1.93 | |
| B. Glial Proteins: Oligodendrocytes | |||||
| Myelin Basic Protein (MBP) | Mean (SE) | 4.28 (0.18) *** | 2.17 (0.32) *** | 1.19 (0.03) *** | 1.52 (0.09) *** |
| Range | 0.09–17.34 | 0.42–11.83 | 0.74–1.7 | 0.44–4.33 | |
| Myelin Associated Glycoprotein (MAG) | Mean (SE) | 4.94 (0.28) *** | 2.12 (0.25) *** | 3.20 (0.21) * | 1.58 (0.11) *** |
| Range | 0.24–20.94 | 0.38–6.51 | 1.03–6.51 | 0.26–4/48 | |
| Glial Proteins: Astrocytes | |||||
| Glial Fibrillary Associated Protein (GFAP) | Mean (SE) | 4.27 (0.18) *** | 2.34 (0.30) *** | 0.84 (0.03) *** | 4.86 (0.26) |
| Range | 0.39–13.14 | 0.35–14.98 | 0.45–1.38 | 0.66–8.44 | |
| Glial S100B (S100B) | Mean (SE) | 1.17 (0.04) | 1.16 (0.03) | 0.95 (0.03) | 1.34 (0.06) * |
| Range | 2.60–2.41 | 0.37–2.74 | 0.53–1.34 | 0.49–2.26 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abou-Donia, M.B.; Lapadula, E.S.; Krengel, M.H.; Quinn, E.; LeClair, J.; Massaro, J.; Conboy, L.A.; Kokkotou, E.; Abreu, M.; Klimas, N.G.; et al. Using Plasma Autoantibodies of Central Nervous System Proteins to Distinguish Veterans with Gulf War Illness from Healthy and Symptomatic Controls. Brain Sci. 2020, 10, 610. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10090610
Abou-Donia MB, Lapadula ES, Krengel MH, Quinn E, LeClair J, Massaro J, Conboy LA, Kokkotou E, Abreu M, Klimas NG, et al. Using Plasma Autoantibodies of Central Nervous System Proteins to Distinguish Veterans with Gulf War Illness from Healthy and Symptomatic Controls. Brain Sciences. 2020; 10(9):610. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10090610
Chicago/Turabian StyleAbou-Donia, Mohamed B., Elizabeth S. Lapadula, Maxine H. Krengel, Emily Quinn, Jessica LeClair, Joseph Massaro, Lisa A. Conboy, Efi Kokkotou, Maria Abreu, Nancy G. Klimas, and et al. 2020. "Using Plasma Autoantibodies of Central Nervous System Proteins to Distinguish Veterans with Gulf War Illness from Healthy and Symptomatic Controls" Brain Sciences 10, no. 9: 610. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10090610