Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Treatments and Randomization Procedure
2.1.1. The Overground Robot-Assisted Gait Training
2.1.2. The Conventional Gait Training
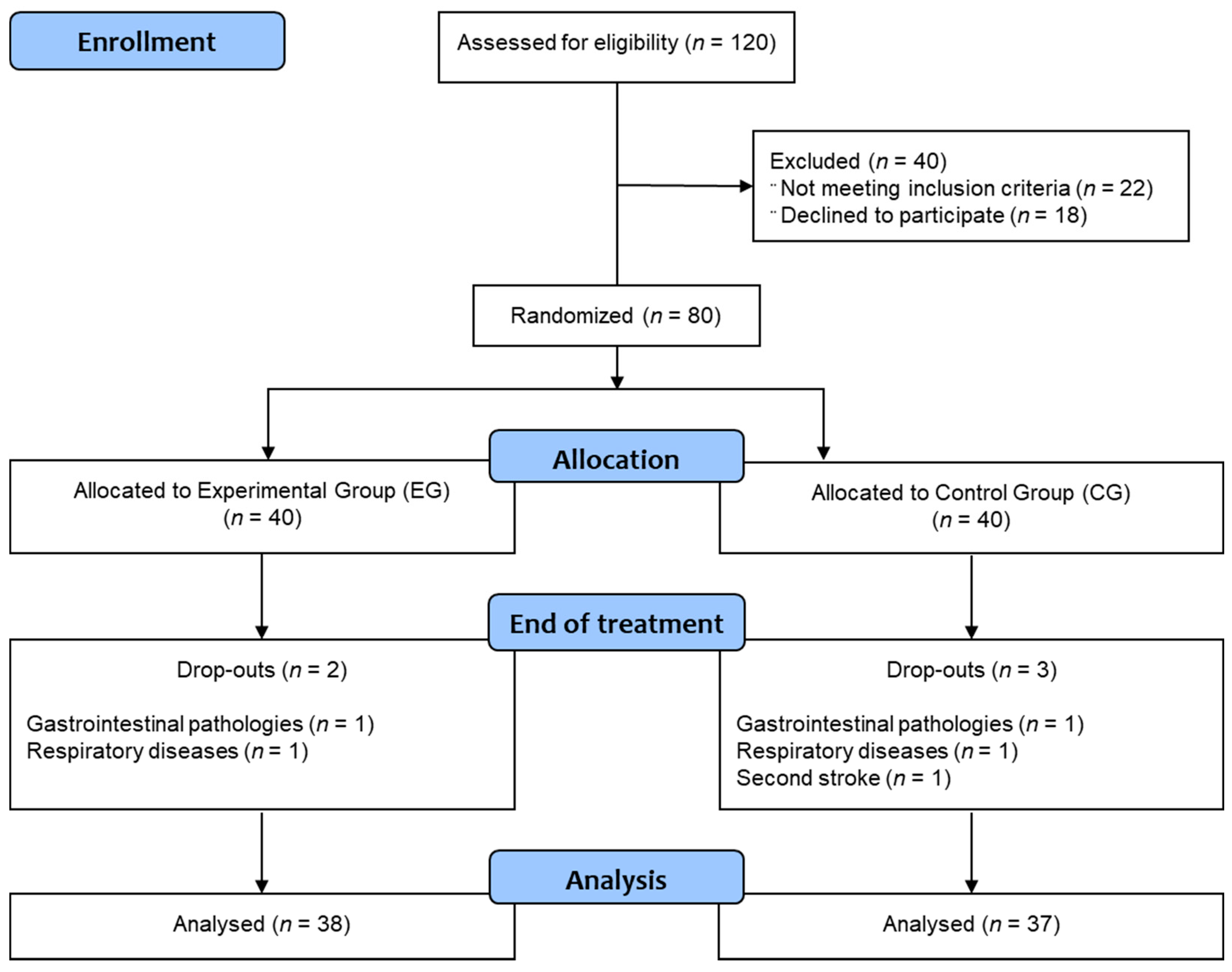
2.2. Recruitment
2.3. The Clinical Outcomes
2.4. Usability and Acceptance
2.5. Data Analysis and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hong, E. Comparison of quality of life according to community walking in stroke patients. J. Phys. Ther. Sci. 2015, 27, 2391–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seccia, R.; Boresta, M.; Fusco, F.; Tronci, E.; Di Gemma, E.; Palagi, L.; Mangone, M.; Agostini, F.; Bernetti, A.; Santilli, V.; et al. Data of patients undergoing rehabilitation programs. Data Brief 2020, 30, 105419. [Google Scholar] [CrossRef] [PubMed]
- Louie, D.R.; Eng, J.J. Powered robotic exoskeletons in post-stroke rehabilitation of gait: A scoping review. J. Neuroeng. Rehabil. 2016, 13, 53. [Google Scholar] [CrossRef] [Green Version]
- Molteni, F.; Gasperini, G.; Cannaviello, G.; Guanziroli, E. Exoskeleton and end-effector robots for upper and lower limbs rehabilitation: Narrative review. PmR 2018, 10, 174–188. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.; Handy, T.C.; Lakhani, B.; Boyd, L.A.; Garland, S.J. Motor and visuospatial attention and motor planning after stroke: Considerations for the rehabilitation of standing balance and gait. Phys. Ther. 2015, 95, 1423–1432. [Google Scholar] [CrossRef] [Green Version]
- Pons, J.L. Rehabilitation exoskeletal robotics. IEEE Eng. Med. Biol. Mag. 2010, 29, 57–63. [Google Scholar] [CrossRef]
- Bruni, M.F.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. What does best evidence tell us about robotic gait rehabilitation in stroke patients: A systematic review and meta-analysis. J. Clin. Neurosci. 2018, 48, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Cheng, Y.H.; Lai, C.H.; Lin, Y.N. Clinical non-superiority of technology-assisted gait training with body weight support in patients with subacute stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2019, 63, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2017, 10, CD006185. [Google Scholar] [CrossRef]
- Capecci, M.; Pournajaf, S.; Galafate, D.; Sale, P.; Le Pera, D.; Goffredo, M.; de Pandis, F.M.; Andrenelli, E.; Pennacchioni, M.; Ceravolo, M.G.; et al. Clinical effects of robot-assisted gait training and treadmill training for Parkinson’s disease. A randomized controlled trial. Ann. Phys. Rehabil. Med. 2019, 62, 303–312. [Google Scholar] [CrossRef]
- Aprile, I.; Iacovelli, C.; Goffredo, M.; Cruciani, A.; Galli, M.; Simbolotti, C.; Pecchioli, C.; Padua, L.; Galafate, D.; Pournajaf, S.; et al. Efficacy of end-effector robot-assisted gait training in subacute stroke patients: Clinical and gait outcomes from a pilot bi-centre study. Neurorehabilitation 2019, 45, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Paolucci, S.; Cherubini, A.; De Angelis, D.; Venturiero, V.; Coiro, P.; Iosa, M. Robot-assisted gait training for stroke patients: Current state of the art and perspectives of robotics. Neuropsychiatr. Dis. Treat. 2017, 13, 1303–1311. [Google Scholar] [CrossRef] [Green Version]
- Calabrò, R.S.; Naro, A.; Russo, M.; Bramanti, P.; Carioti, L.; Balletta, T.; Buda, A.; Manuli, A.; Filoni, S.; Bramanti, A. Shaping neuroplasticity by using powered exoskeletons in patients with stroke: A randomized clinical trial. J. Neuroeng. Rehabil. 2018, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Rojek, A.; Mika, A.; Oleksy, Ł.; Stolarczyk, A.; Kielnar, R. Effects of Exoskeleton Gait Training on Balance; Load Distribution; and Functional Status in Stroke: A Randomized Controlled Trial. Front. Neurol. 2020, 10, 1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.-J.; Lee, S.-H.; Seo, K.; Lee, M.; Chang, W.H.; Choi, B.-O.; Ryu, G.-H.; Kim, Y.-H. Training for walking efficiency with a wearable hip-assist robot in patients with stroke: A pilot randomized controlled trial. Stroke 2019, 50, 3545–3552. [Google Scholar] [CrossRef] [PubMed]
- Goffredo, M.; Iacovelli, C.; Russo, E.; Pournajaf, S.; Di Blasi, C.; Galafate, D.; Pellicciari, L.; Agosti, M.; Filoni, S.; Aprile, I.; et al. Stroke Gait Rehabilitation: A Comparison of End-Effector; Overground Exoskeleton; and Conventional Gait Training. Appl. Sci. 2019, 9, 2627. [Google Scholar] [CrossRef] [Green Version]
- Cirstea, C.M. Are Wearable Robots Effective for Gait Recovery after Stroke? Stroke 2019, 50, 3337–3338. [Google Scholar] [CrossRef] [PubMed]
- Nolan, K.J.; Karunakaran, K.K.; Chervin, K.; Monfett, M.R.; Bapineedu, R.K.; Jasey, N.N.; Oh-Park, M. Robotic Exoskeleton Gait Training During Acute Stroke Inpatient Rehabilitation. Front. Neurorobotics 2020, 14, 581815. [Google Scholar] [CrossRef] [PubMed]
- Wall, A.; Borg, J.; Vreede, K.; Palmcrantz, S. A randomized controlled study incorporating an electromechanical gait machine; The Hybrid Assistive Limb; In gait training of patients with severe limitations in walking in the subacute phase after stroke. PLoS ONE 2020, 15, e0229707. [Google Scholar] [CrossRef] [Green Version]
- Gasperini, G.; Gaffuri, M.; Guanziroli, E.; Goffredo, M.; Puornajaf, S.; Galafate, D.; Russo, E.; Filoni, S.; Franceschini, M.; Molteni, F. Recovery of gait function with a wearable powered exoskeleton in sub-acute stroke patients using SEMG for fine tuning: Preliminary results. Ann. Phys. Rehabil. Med. 2018, 61, e93. [Google Scholar] [CrossRef]
- Molteni, F.; Gasperini, G.; Gaffuri, M.; Colombo, M.; Giovanzana, C.; Lorenzon, C.; Farina, N.; Cannaviello, G.; Scarano, S.; Proserpio, D.; et al. Wearable robotic exoskeleton for overground gait training in sub-acute and chronic hemiparetic stroke patients: Preliminary results. Eur. J. Phys. Rehabil. Med. 2017, 53, 676–684. [Google Scholar]
- Goffredo, M.; Guanziroli, E.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Damiani, C.; Franceschini, M.; Molteni, F.; et al. Overground wearable powered exoskeleton for gait training in subacute stroke subjects: Clinical and gait assessments. Eur. J. Phys. Rehabil. Med. 2019, 55, 710–721. [Google Scholar] [CrossRef] [PubMed]
- Gandolla, M.; Guanziroli, E.; D’Angelo, A.; Cannaviello, G.; Molteni, F.; Pedrocchi, A. Automatic Setting Procedure for Exoskeleton-Assisted Overground Gait: Proof of Concept on Stroke Population. Front Neurorobot. 2018, 19, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef] [PubMed]
- Dadgoo, M.; Salehi, M. Test-retest reliability of Motricity Index strength assessments for lower extremity in post stroke hemiparesis. Med. J. Islam. Repub. Iran 2012, 26, 27–30. [Google Scholar]
- Franchignoni, F.P.; Tesio, L.; Ricupero, C.; Martino, M.T. Trunk control test as an early predictor of stroke rehabilitation outcome. Stroke 1997, 28, 1382–1385. [Google Scholar] [CrossRef]
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L. Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Tyson, S.; Connell, L. The psychometric properties and clinical utility of measures of walking and mobility in neurological conditions: A systematic review. Clin. Rehabil. 2009, 23, 1018–1033. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Hsueh, I.P.; Lin, J.H.; Jeng, J.S.; Hsieh, C.L. Comparison of the psychometric characteristics of the functional independence measure; 5 item Barthel index; And 10 item Barthel index in patients with stroke. J. Neurol. Neurosurg. Psychiatry 2002, 73, 188–190. [Google Scholar] [CrossRef]
- Perry, J.; Garrett, M.; Gronley, J.K.; Mulroy, S.J. Classification of walking handicap in the stroke population. Stroke 1995, 26, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Mazzoleni, S.; Turchetti, G.; Palla, I.; Posteraro, F.; Dario, P. Acceptability of robotic technology in neuro-rehabilitation: Preliminary results on chronic stroke patients. Comput. Methods Programs Biomed. 2014, 116, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Song, X.Y. Evaluation of the Bayesian and Maximum Likelihood Approaches in Analyzing Structural Equation Models with Small Sample Sizes. Multivar. Behav. Res. 2004, 39, 653–686. [Google Scholar] [CrossRef] [PubMed]
- Hox, J.; Van de Schoot, R.; Matthijsse, S. How few countries will do? Comparative survey analysis from a Bayesian perspective. Surv. Res. Methods 2012, 6, 87–93. [Google Scholar]
- Lee, M.D.; Wagenmakers, E.-J. Bayesian Cognitive Modeling: A Practical Course; Cambridge University Press: Cambridge, UK, 2013. [Google Scholar]
- Franceschini, M.; Mazzoleni, S.; Goffredo, M.; Pournajaf, S.; Galafate, D.; Criscuolo, S.; Agosti, M.; Posteraro, F. Upper limb robot-assisted rehabilitation versus physical therapy on subacute stroke patients: A follow-up study. J. Bodyw. Mov. Ther. 2019, 24, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Pournajaf, S.; Goffredo, M.; Agosti, M.; Massucci, M.; Ferro, S.; Franceschini, M. Community ambulation of stroke survivors at 6 months follow-up: An observational study on sociodemographic and sub-acute clinical indicators. Eur. J. Phys. Rehabil. Med. 2019, 55, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-B.; Wang, Y.-Y.; Zhang, Q.-E.; Wu, S.-L.; Ng, C.H.; Ungvari, G.S.; Chen, L.; Wang, C.; Jia, F.; Xiang, Y.-T. Cognitive behavioral therapy for post-stroke depression: A meta-analysis. J. Affect. Disord. 2018, 235, 589–596. [Google Scholar] [CrossRef]
- Giusino, D.; Fraboni, F.; Rainieri, G.; De Angelis, M.; Tria, A.; La Bara, L.M.A.; Pietrantoni, L. Human Factors in Interfaces for Rehabilitation-Assistive Exoskeletons: A Critical Review and Research Agenda. In International Conference on Human Interaction and Emerging Technologies; Springer: Cham, Germany, 2020; pp. 356–362. [Google Scholar]
- Esquenazi, A.; Lee, S.; Wikoff, A.; Packel, A.; Toczylowski, T.; Feeley, J. A Comparison of Locomotor Therapy Interventions: Partial-Body Weight−Supported Treadmill; Lokomat; and G-EO Training in People with Traumatic Brain Injury. PMR 2017, 9, 839–846. [Google Scholar] [CrossRef]
- Goffredo, M.; Infarinato, F.; Pournajaf, S.; Romano, P.; Ottaviani, M.; Pellicciari, L.; Galafate, D.; Gabbani, D.; Gison, A.; Franceschini, M. Barriers to sEMG Assessment During Overground Robot-Assisted Gait Training in Subacute Stroke Patients. Front. Neurol. 2020, 11, 1263. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EG (N = 38) | CG (N = 37) | p-Value | BF01 | |
|---|---|---|---|---|
| Age (years) | 62.13 ± 8.75 | 68.24 ± 8.58 | 0.003 1 | 0.08 |
| Gender (female or male) | 17(45%)/21(55%) | 19(51%)/21(49%) | 0.896 2 | 1.82 |
| Etiology (ischemic or hemorrhagic) | 30(79%)/8(21%) | 33(89%)/4(11%) | 0.291 2 | 1.42 |
| Affected side (right or left) | 19(50%)/19(50%) | 11(30%)/26(70%) | 0.073 2 | 0.39 |
| Delay since stroke (days) | 35.68 ± 10.70 | 34.14 ± 16.07 | 0.626 1 | 3.78 |
| 6MWT (m) | 48.60 ± 42.39 | 44.29 ± 59.15 | 0.906 1 | 4.18 |
| MI-AL | 46.08 ± 14.80 | 48.97 ± 22.58 | 0.434 1 | 3.19 |
| TCT | 48.37 ± 25.78 | 48.75 ± 20.54 | 0.849 1 | 4.14 |
| 10MWT (m/s) | 0.25 ± 0.19 | 0.20 ± 0.26 | 0.590 1 | 3.67 |
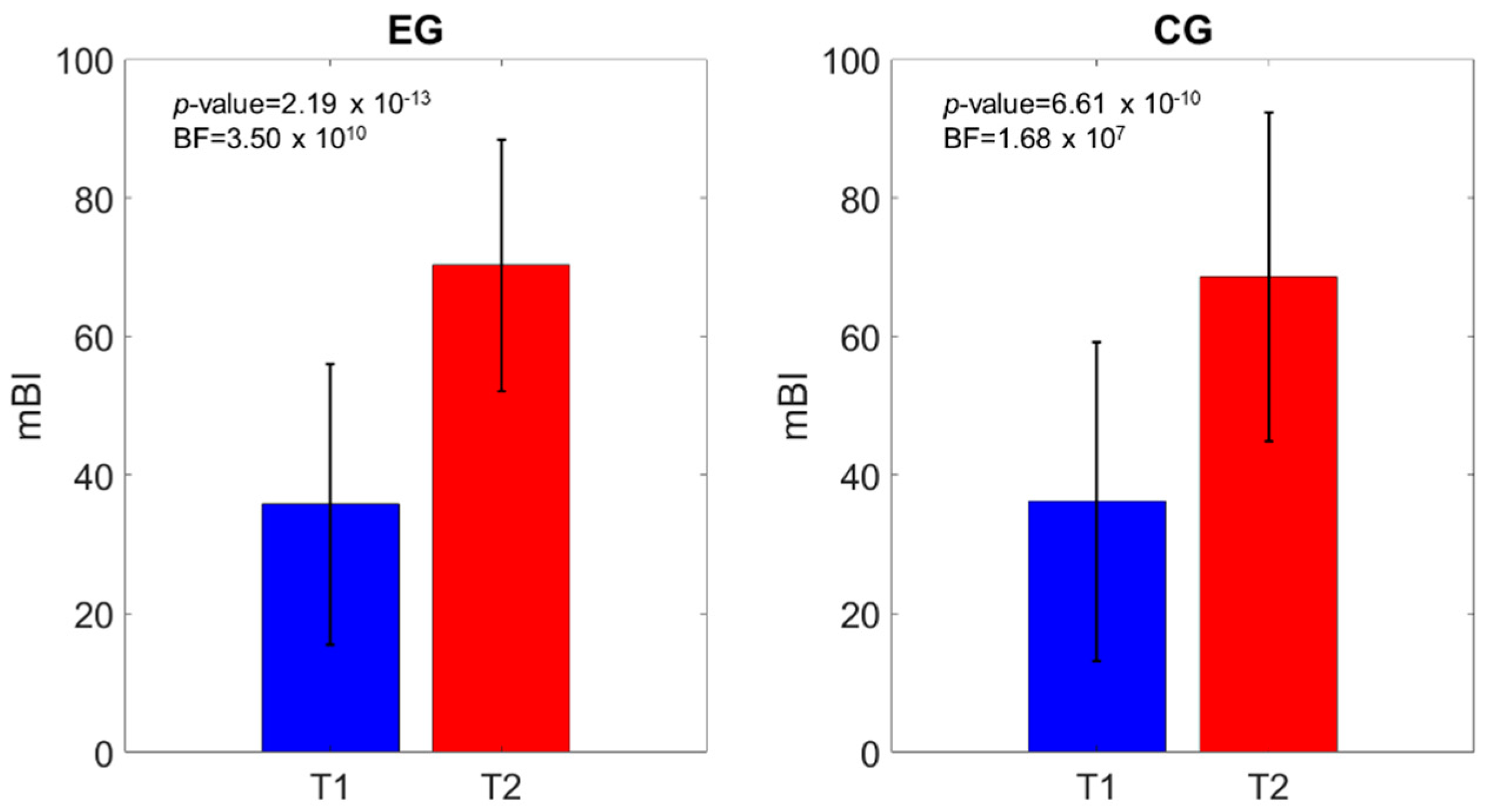
| mBI | 35.78 ± 20.24 | 36.20 ± 22.98 | 0.891 1 | 3.97 |
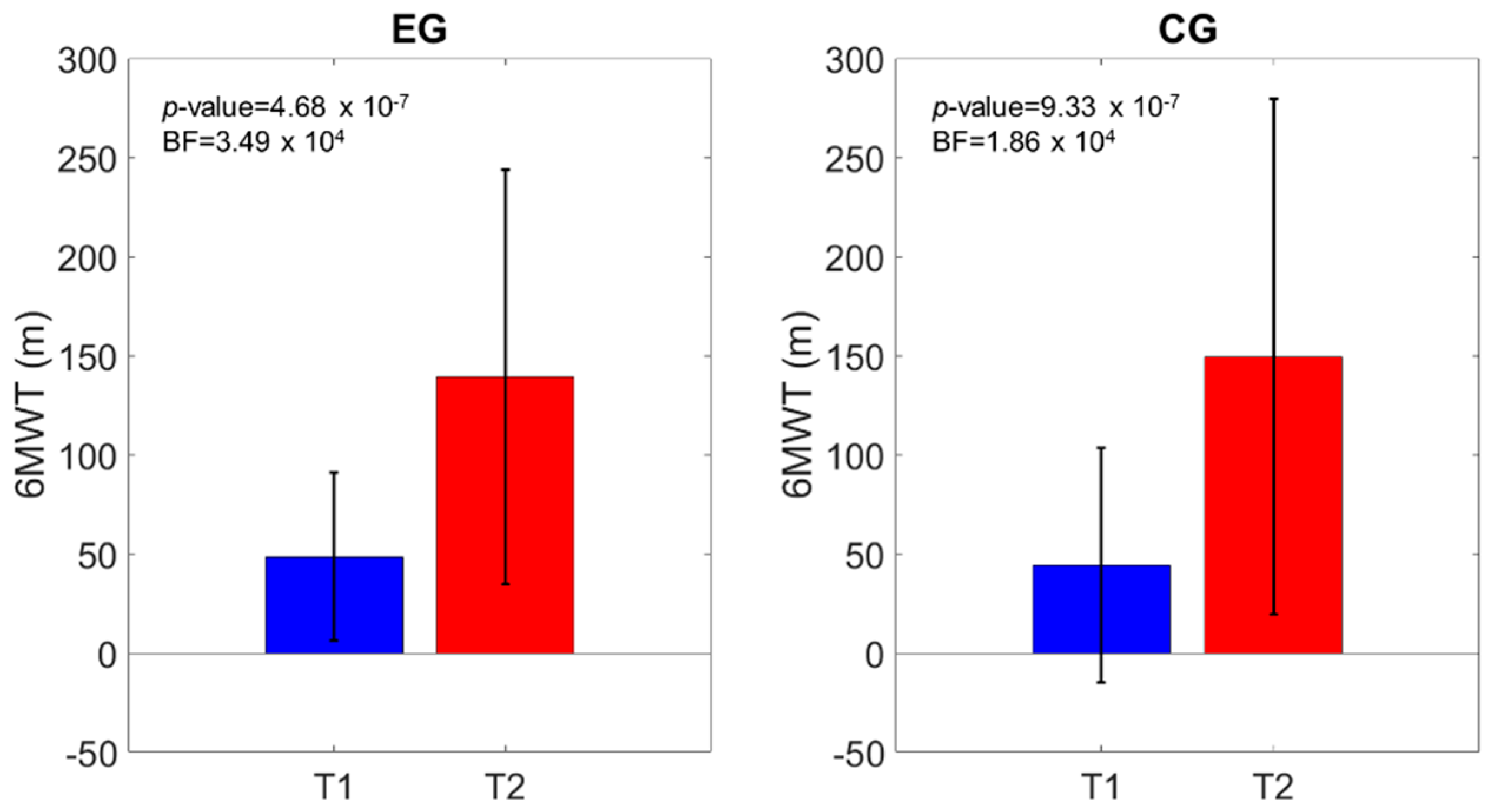
| 6MWT | |||||
| Model Comparison | P (M) | P (M|Data) | BFM | BF10 | Error % |
| Null model (including age, subject) | 0.200 | 4.346 × 10−11 | 1.738 × 10−10 | 1.000 | - |
| Group | 0.200 | 1.077 × 10−11 | 4.306 × 10−11 | 0.248 | 5.499 |
| Time | 0.200 | 0.725 | 10.571 | 1.669 × 1010 | 2.109 |
| Group + Time | 0.200 | 0.212 | 1.075 | 4.874 × 109 | 3.048 |
| Group + Time + Group ✻ Time | 0.200 | 0.063 | 0.268 | 1.443 × 109 | 4.104 |
| Effects | P (incl) | P (incl|Data) | BFInclusion | ||
| Group | 0.600 | 0.275 | 0.252 | - | - |
| Time | 0.600 | 1.000 | 1.230 × 1010 | - | - |
| Group ✻ Time | 0.200 | 0.063 | 0.268 | - | - |
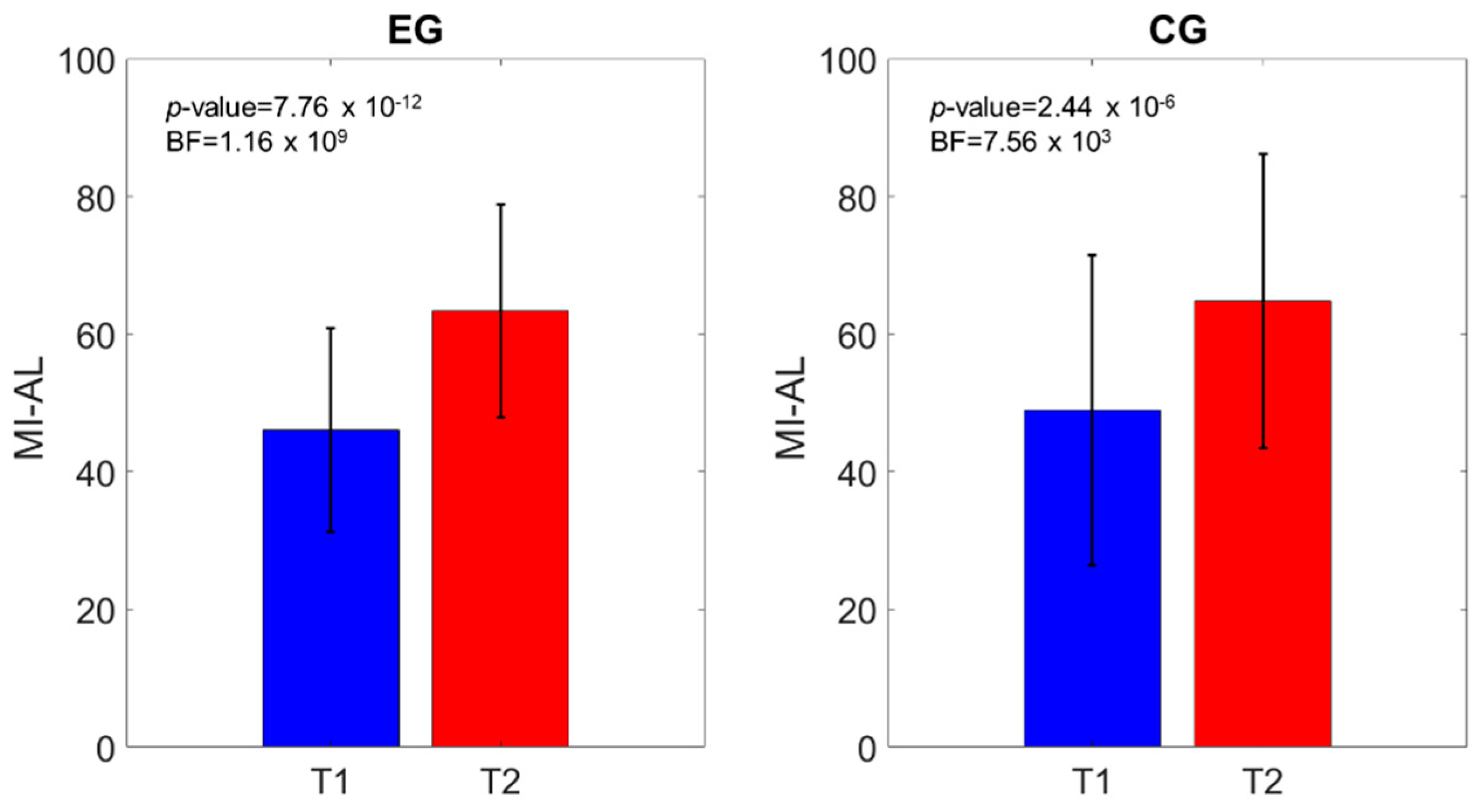
| MI-AL | |||||
| Model Comparison | P (M) | P (M|Data) | BFM | BF10 | Error % |
| Null model (including age, subject) | 0.200 | 1.434 × 10−13 | 5.736 × 10−13 | 1.000 | - |
| Group | 0.200 | 4.132 × 10−14 | 1.653 × 10−13 | 0.288 | 1.873 |
| Time | 0.200 | 0.656 | 7.619 | 4.573 × 1012 | 1.722 |
| Group + Time | 0.200 | 0.279 | 1.547 | 1.945 × 1012 | 3.550 |
| Group + Time + Group ✻ Time | 0.200 | 0.065 | 0.280 | 4.559 × 1012 | 4.303 |
| Effects | P (incl) | P (incl|Data) | BFInclusion | ||
| Group | 0.600 | 0.344 | 0.350 | - | - |
| Time | 0.600 | 1.000 | 3.609 × 1012 | - | - |
| Group ✻ Time | 0.200 | 0.065 | 0.280 | - | - |
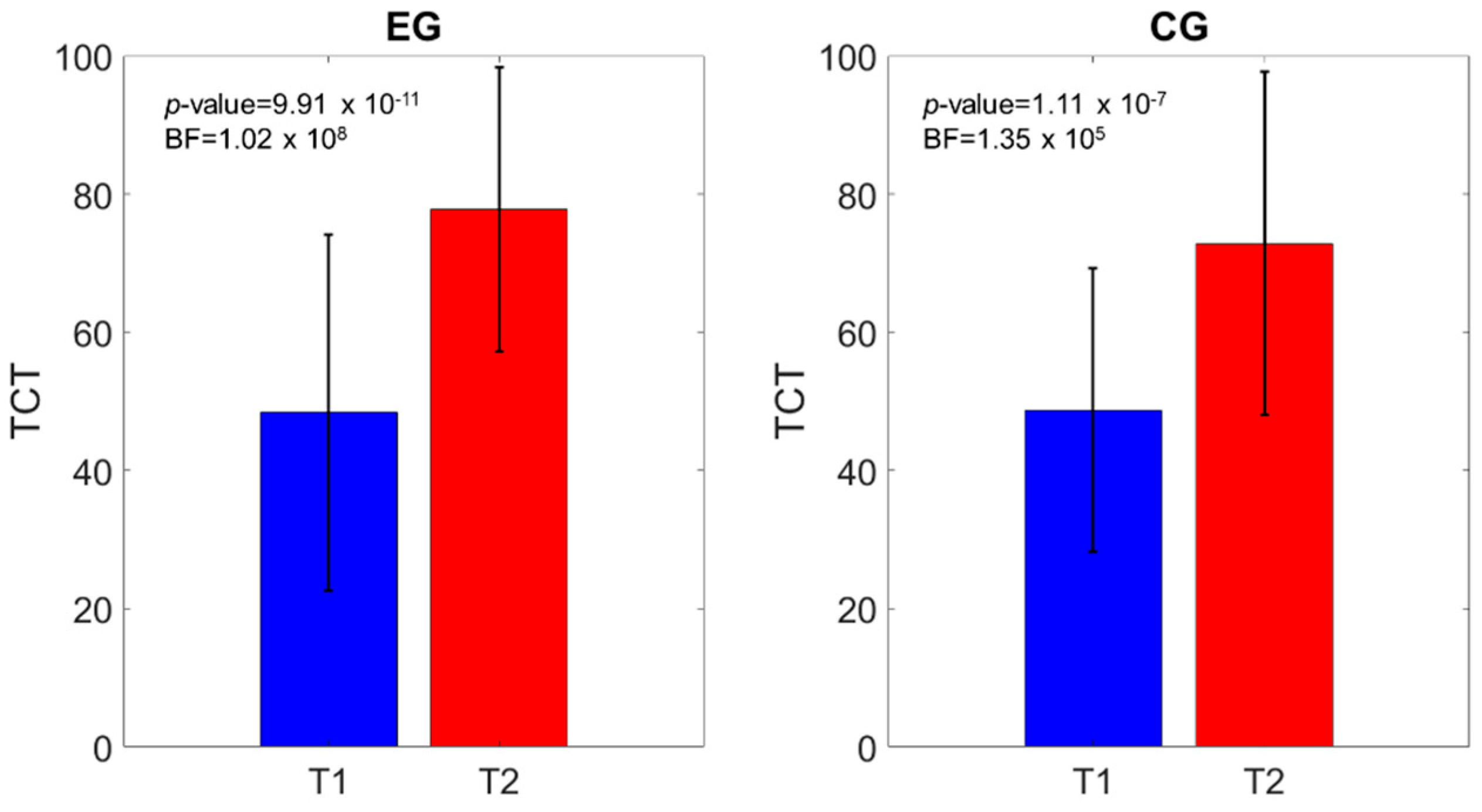
| TCT | |||||
| Model Comparison | P (M) | P (M|Data) | BFM | BF10 | Error % |
| Null model (including age, subject) | 0.200 | 4.045 × 10−15 | 1.618 × 10−14 | 1.000 | - |
| Group | 0.200 | 1.003 × 10−15 | 4.012 × 10−15 | 0.248 | 2.076 |
| Time | 0.200 | 0.658 | 7.709 | 1.628 × 1014 | 2.044 |
| Group + Time | 0.200 | 0.247 | 1.310 | 6.098 × 1013 | 4.351 |
| Group + Time + Group ✻ Time | 0.200 | 0.095 | 0.420 | 2.348 × 1013 | 3.005 |
| Effects | P (incl) | P (incl|Data) | BFInclusion | ||
| Group | 0.600 | 0.342 | 0.346 | - | - |
| Time | 0.600 | 1.000 | 1.334 × 1014 | - | - |
| Group ✻ Time | 0.200 | 0.095 | 0.420 | - | - |
| 10MWT | |||||
| Model Comparison | P (M) | P (M|Data) | BFM | BF10 | Error % |
| Null model (including age, subject) | 0.200 | 2.295 × 10−9 | 9.179 × 10−9 | 1.000 | - |
| Group | 0.200 | 6.818 × 10−10 | 2.727 × 10−9 | 0.297 | 3.271 |
| Time | 0.200 | 0.569 | 5.285 | 2.480 × 108 | 2.906 |
| Group + Time | 0.200 | 0.186 | 0.914 | 8.103e × 107 | 2.771 |
| Group + Time + Group ✻ Time | 0.200 | 0.245 | 1.297 | 1.067 x 108 | 3.498 |
| Effects | P (incl) | P (incl|Data) | BFInclusion | ||
| Group | 0.600 | 0.431 | 0.505 | - | - |
| Time | 0.600 | 1.000 | 2.240 × 108 | - | - |
| Group ✻ Time | 0.200 | 0.245 | 1.297 | - | - |
| mBI | |||||
| Model Comparison | P (M) | P (M|Data) | BFM | BF10 | Error % |
| Null model (including age, subject) | 0.200 | 7.951 × 10−21 | 3.180 × 10−20 | 1.000 | - |
| Group | 0.200 | 1.887 × 10−21 | 7.548 × 10−21 | 0.237 | 2.206 |
| Time | 0.200 | 0.683 | 8.618 | 8.590 × 1019 | 1.547 |
| Group + Time | 0.200 | 0.251 | 1.338 | 3.152 × 1019 | 2.263 |
| Group + Time + Group ✻ Time | 0.200 | 0.066 | 0.285 | 8.353 × 1018 | 2.239 |
| Effects | P (incl) | P (incl|Data) | BFInclusion | ||
| Group | 0.600 | 0.317 | 0.309 | - | - |
| Time | 0.600 | 1.000 | ∞ | - | - |
| Group ✻ Time | 0.200 | 0.066 | 0.285 | - | - |
| T1 | T2 | |||||
|---|---|---|---|---|---|---|
| EG (N = 38) | CG (N = 37) | p-Value | EG (N = 38) | CG (N = 37) | p-Value | |
| MAS-AL | ||||||
| 0.0 | 15 | 19 | 0.154 | 12 | 19 | 0.239 |
| 1.0 | 5 | 10 | 8 | 9 | ||
| 1.5 | 1 | 0 | 1 | 0 | ||
| 2.0 | 7 | 4 | 7 | 6 | ||
| 2.5 | 1 | 1 | 2 | 0 | ||
| 3.0 | 2 | 2 | 4 | 2 | ||
| 3.5 | 0 | 0 | 3 | 0 | ||
| 4.0 | 6 | 0 | 0 | 1 | ||
| 4.5 | 1 | 0 | 1 | 0 | ||
| 5.0 | 0 | 1 | 0 | 0 | ||
| 5.5 | 6 | 0 | 0 | 0 | ||
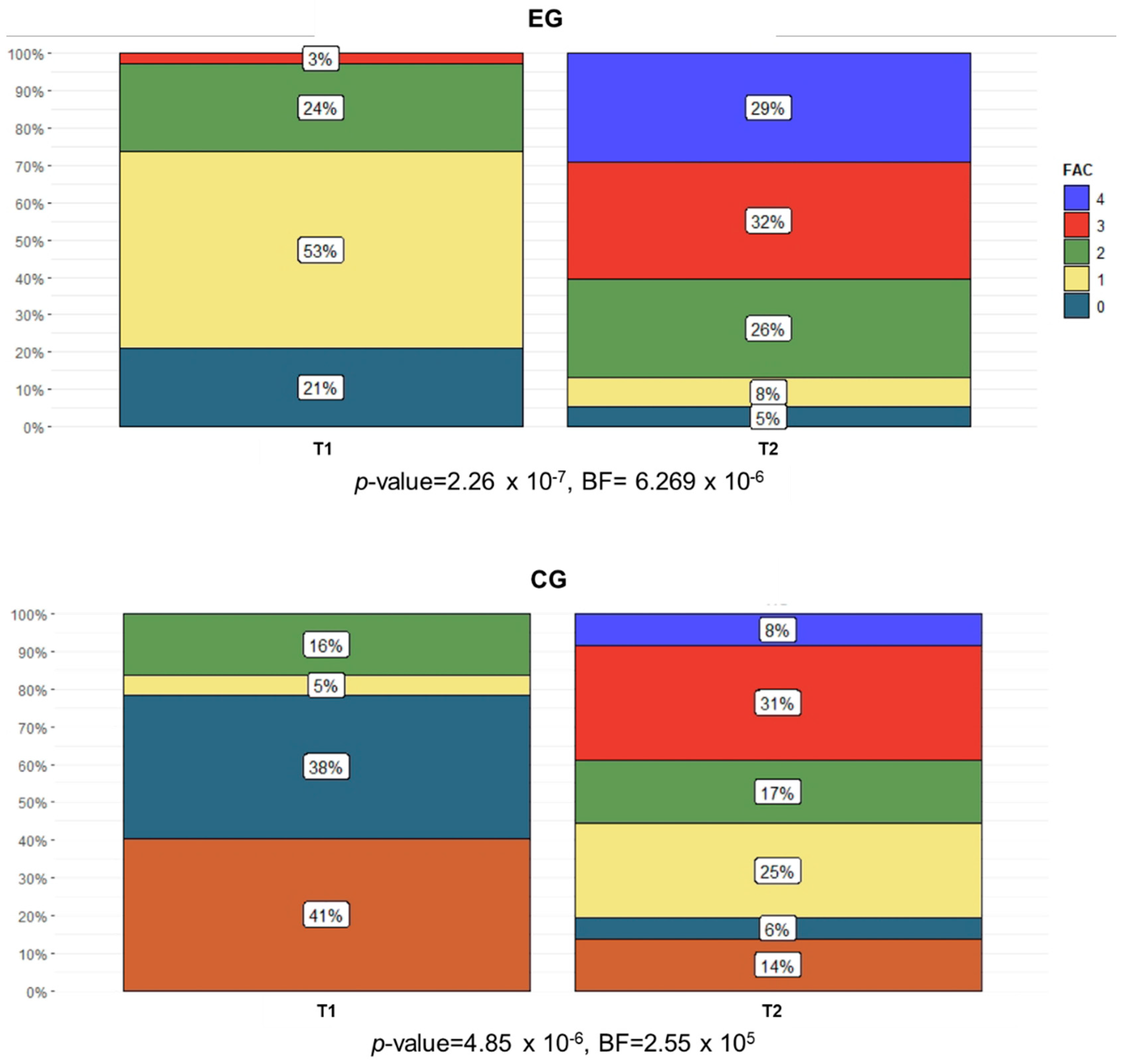
| FAC | ||||||
| 0 | 8 | 15 | 0.010 | 2 | 5 | 0.261 |
| 1 | 20 | 14 | 3 | 2 | ||
| 2 | 9 | 2 | 10 | 9 | ||
| 3 | 1 | 6 | 12 | 6 | ||
| 4 | 0 | 0 | 11 | 11 | ||
| 5 | 0 | 0 | 0 | 3 | ||
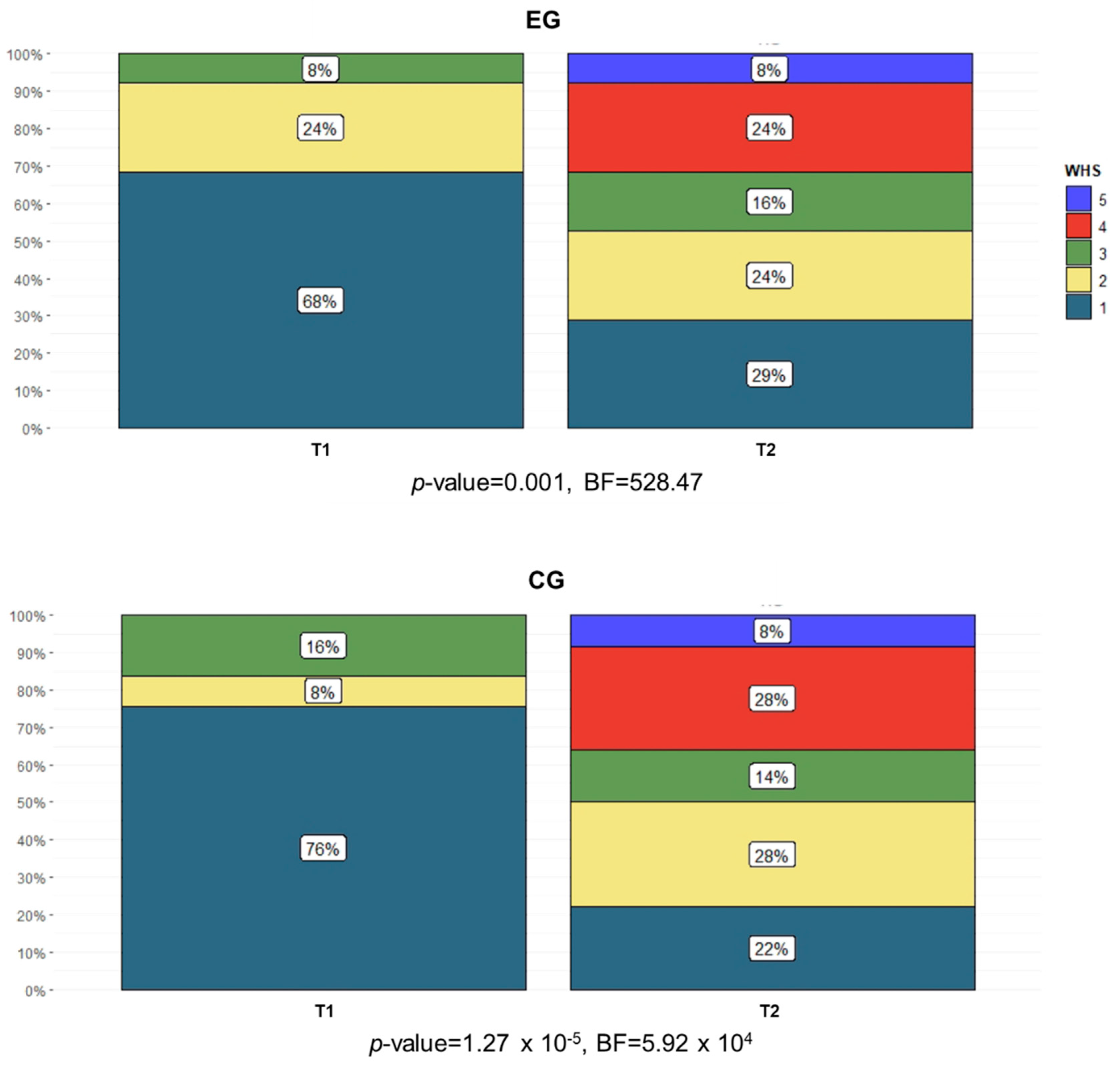
| WHS | ||||||
| 1 | 26 | 28 | 0.961 | 11 | 8 | 0.001 |
| 2 | 9 | 3 | 9 | 10 | ||
| 3 | 3 | 6 | 6 | 5 | ||
| 4 | 0 | 0 | 9 | 10 | ||
| 5 | 0 | 0 | 3 | 3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molteni, F.; Guanziroli, E.; Goffredo, M.; Calabrò, R.S.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Galafate, D.; et al. Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects. Brain Sci. 2021, 11, 104. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11010104
Molteni F, Guanziroli E, Goffredo M, Calabrò RS, Pournajaf S, Gaffuri M, Gasperini G, Filoni S, Baratta S, Galafate D, et al. Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects. Brain Sciences. 2021; 11(1):104. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11010104
Chicago/Turabian StyleMolteni, Franco, Eleonora Guanziroli, Michela Goffredo, Rocco Salvatore Calabrò, Sanaz Pournajaf, Marina Gaffuri, Giulio Gasperini, Serena Filoni, Silvano Baratta, Daniele Galafate, and et al. 2021. "Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects" Brain Sciences 11, no. 1: 104. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11010104