
Can the Addition of Maintenance Electroconvulsive Therapy to Pharmacotherapy Improve Relapse Prevention in Severe Major Depressive Disorder? A Randomized Controlled Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Recruitment
- (1)
- M-Pharm/ECT group, consisting of pharmacotherapy plus ECT for nine months;
- (2)
- M-Pharm group, pharmacotherapy alone.
2.2. Subjects
2.3. Intervention/Treatment
2.3.1. M-ECT
2.3.2. Pharmacotherapy
2.4. Variables and Measures
2.5. Statistics
2.6. Sample Size
2.7. Dropout from Statistical Analysis
3. Results
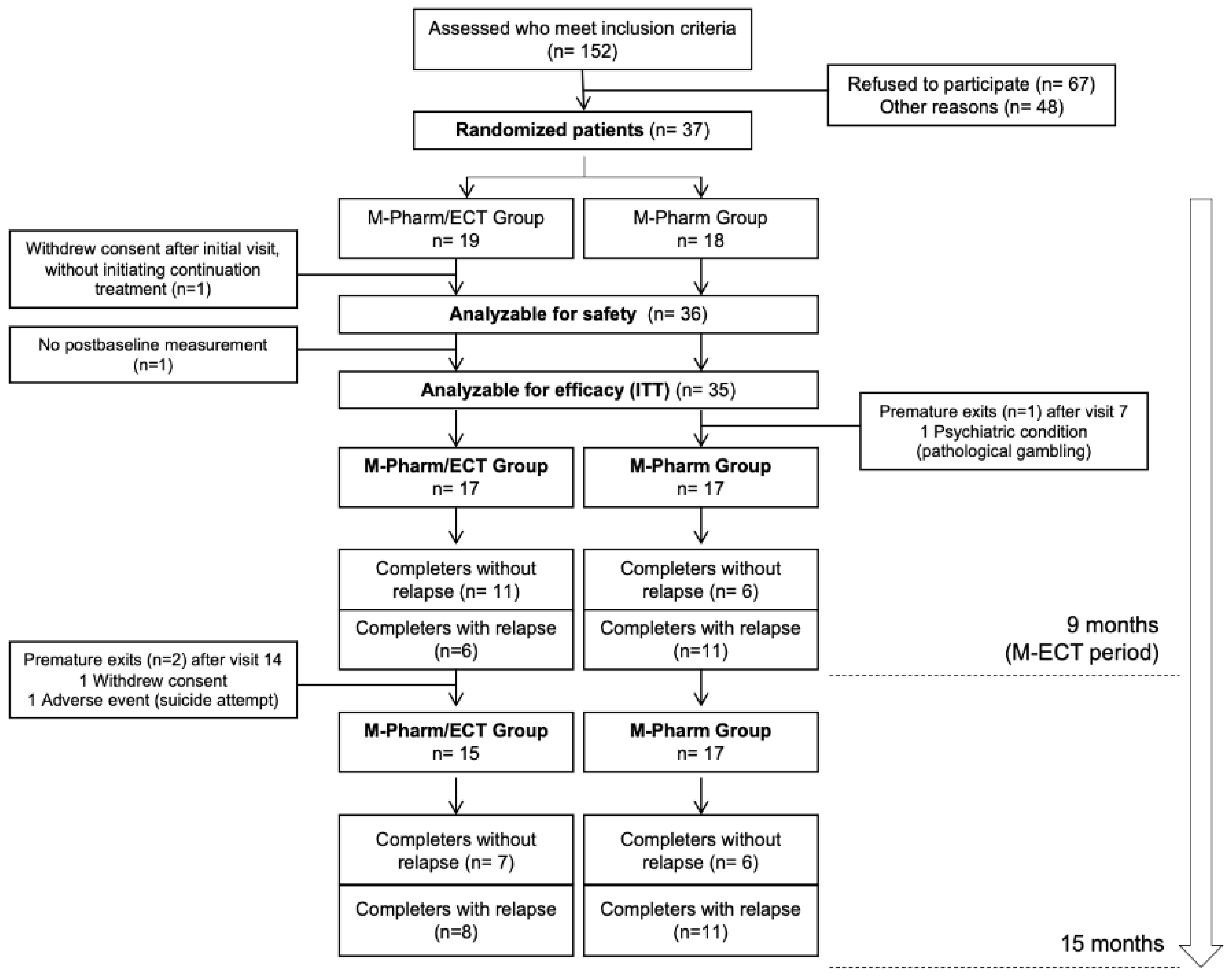
3.1. Subject Disposition
3.2. Study Sample Characteristics
3.3. Efficacy Results
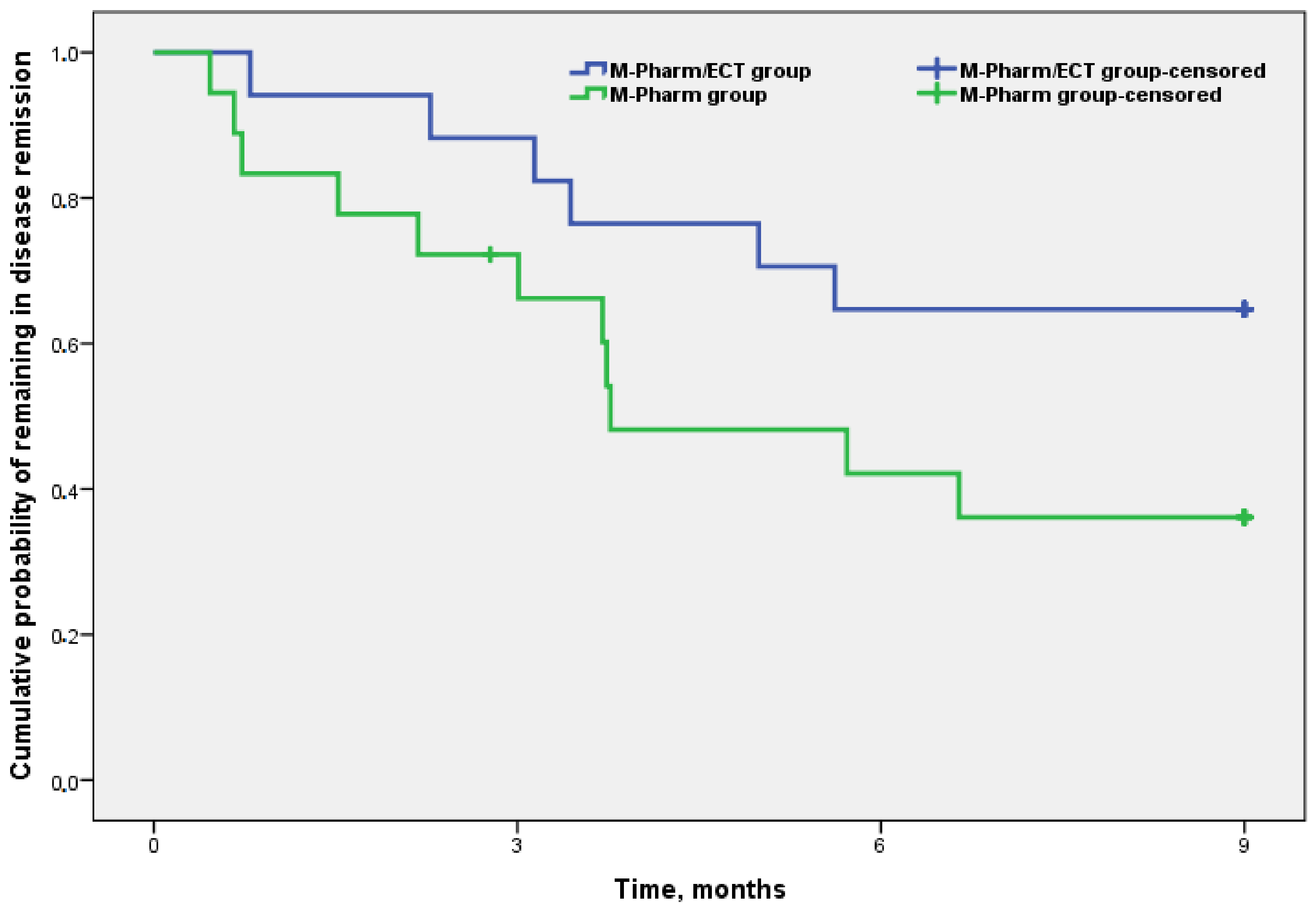
3.3.1. Relapse in the Intention-to-Treat Sample at Nine Months
3.3.2. Relapses at the End of the Study (at 15 Months)
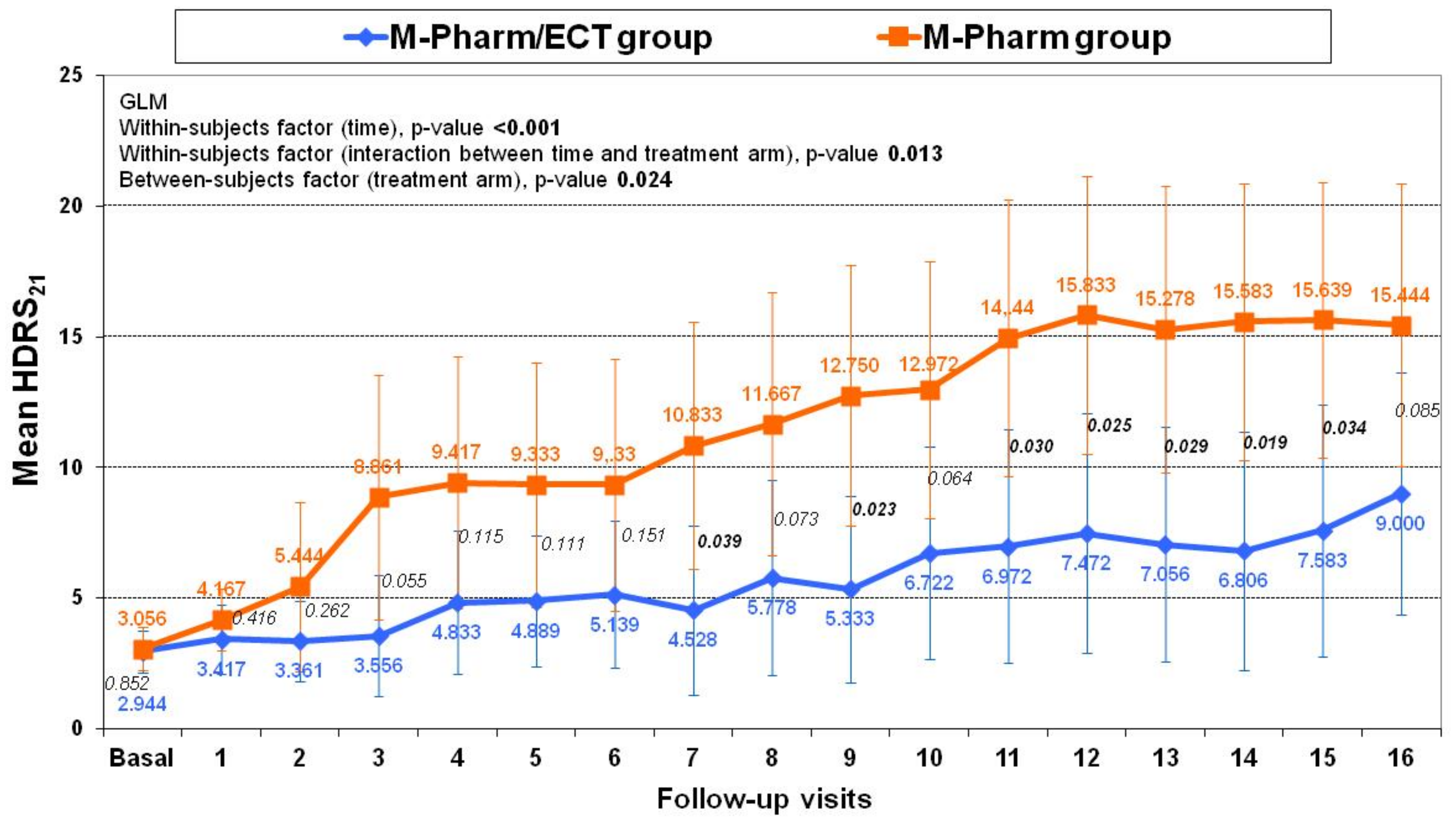
3.4. Changes in Clinical Scales (HDRS-21 and CGI-S)
3.5. Adverse Events and Cognitive Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. The Practice of Electroconvulsive Therapy. Recommendations for Treatment, Training, and Privileging, 2nd ed.; A Task Force Report of the American Psychiatric Association; American Psychiatric Association: Washington, DC, USA, 2001. [Google Scholar]
- UK ECT Review Group. Efficacy and safety of electroconvulsive therapy in depressive disorders: A systematic review and meta-analysis. Lancet 2003, 361, 799–808. [Google Scholar] [CrossRef]
- Sociedad Española de Psiquiatría Biológica (SEPB). Consenso Español Sobre la Terapia Electroconvusliva; Sociedad Española de Psiquiatría Biológica: Madrid, Spain, 2018; Available online: http://www.sepsiq.org/file/Enlaces/SEPB%20-%20Consenso%20Espa%C3%B1ol%20sobre%20la%20Terapia%20Electroconvulsiva.pdf (accessed on 25 April 2021).
- Jelovac, A.; Kolshus, E.; McLoughlin, D.M. Relapse following successful electroconvulsive therapy for major depression: A meta-analysis. Neuropsychopharmacology 2013, 38, 2467–2474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, N.P. The Maintenance Treatment of Chronic Psychotics by Electrically Induced Convulsions. J. Ment. Sci. 1943, 89, 257–269. [Google Scholar] [CrossRef]
- Kalinowsky, L.B. Electric convulsive therapy, with emphasis on importance of adequate treatment. Arch. Neurol. Psychiatry 1943, 50, 652–660. [Google Scholar] [CrossRef]
- Karliner, W.; Wehrheim, H.K. Maintenance convulsive tretaments. Am. J. Psychiatry 1965, 121, 1113–1115. [Google Scholar] [CrossRef] [PubMed]
- Geoghegan, J.J.; Stevenson, G.H. Prophylactic electroshock. Am. J. Psychiatry 1949, 105, 494–496. [Google Scholar] [CrossRef]
- Kerman, E.F. Prevention of recurrence of mental illness with modified prophylactic electroshock therapy. Dis. Nerv. Syst. 1957, 18, 189–191. [Google Scholar]
- Bourne, H. Convulsion Dependence. Lancet 1954, 264, 1193–1196. [Google Scholar] [CrossRef]
- Kellner, C.H.; Knapp, R.G.; Petrides, G.; Rummans, T.A.; Husain, M.M.; Rasmussen, K.; Mueller, M.; Bernstein, H.J.; O’Connor, K.; Smith, G.; et al. Continuation electroconvulsive therapy vs pharmacotherapy for relapse prevention in major depression: A multisite study from the Consortium for Research in Electroconvulsive Therapy (CORE). Arch. Gen. Psychiatry 2006, 63, 1337–1344. [Google Scholar] [CrossRef]
- Kellner, C.H.; Husain, M.M.; Knapp, R.G.; McCall, W.V.; Petrides, G.; Rudorfer, M.V.; Young, R.C.; Sampson, S.; McClintock, S.M.; Mueller, M.; et al. A Novel Strategy for Continuation ECT in Geriatric Depression: Phase 2 of the PRIDE Study. Am. J. Psychiatry 2016, 173, 1110–1118. [Google Scholar] [CrossRef]
- Navarro, V.; Gastó, C.; Torres, X.; Masana, G.; Penadés, R.; Guarch, J.; Vázquez, M.; Serra, M.; Pujol, N.; Pintor, L.; et al. Continuation/maintenance treatment with nortriptyline versus combined nortriptyline and ECT in late-life psychotic depression: A two-year randomized study. Am. J. Geriatr. Psychiatry 2008, 16, 498–505. [Google Scholar] [CrossRef]
- Nordenskjold, A.; Von Knorring, L.; Ljung, T.; Carlborg, A.; Brus, O.; Engstrom, I. Continuation electroconvulsive therapy with pharmacotherapy versus pharmacotherapy alone for prevention of relapse of depression: A randomized controlled trial. J. ECT 2013, 29, 86–92. [Google Scholar] [CrossRef]
- Andrade, C.; Kurinji, S. Continuation and maintenance ECT: A review of recent research. J. ECT 2002, 18, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Frederikse, M.; Petrides, G.; Kellner, C. Continuation and maintenance electroconvulsive therapy for the treatment of depressive illness: A response to the National Institute for Clinical Excellence report. J. ECT 2006, 22, 13–17. [Google Scholar] [CrossRef]
- Trevino, K.; McClintock, S.M.; Husain, M.M. A review of continuation electroconvulsive therapy: Application, safety, and efficacy. J. ECT 2010, 26, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Petrides, G.; Tobias, K.G.; Kellner, C.H.; Rudorfer, M.V. Continuation and maintenance electroconvulsive therapy for mood disorders: Review of the literature. Neuropsychobiology 2011, 64, 129–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Amorós, E.; Cardoner, N.; Gálvez, V.; Urretavizcaya, M. Effectiveness and pattern of use of continuation and maintenance electroconvulsive therapy. Rev. Psiquiatr. Salud Ment. 2012, 5, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Rabheru, K. Maintenance electroconvulsive therapy (M-ECT) after acute response: Examining the evidence for who, what, when, and how? J. ECT 2012, 28, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Van Schaik, A.M.; Comijs, H.C.; Sonnenberg, C.M.; Beekman, A.T.; Sienaert, P.; Stek, M.L. Efficacy and safety of continuation and maintenance electroconvulsive therapy in depressed elderly patients: A systematic review. Am. J. Geriatr. Psychiatry 2012, 20, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.D.; Lee, H.; Scott, D.; Cummings, G.G. Efficacy of Continuation/Maintenance Electroconvulsive Therapy for the Prevention of Recurrence of a Major Depressive Episode in Adults with Unipolar Depression. J. ECT 2014, 30, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Elias, A.; Phutane, V.H.; Clarke, S.; Prudic, J. Electroconvulsive therapy in the continuation and maintenance treatment of depression: Systematic review and meta-analyses. Aust. N. Z. J. Psychiatry 2018, 52, 415–424. [Google Scholar] [CrossRef]
- Greenhalgh, J.; Knight, C.; Hind, D.; Beverley, C.; Walters, S. Clinical and cost-effectiveness of electroconvulsive therapy for depressive illness, schizophrenia, catatonia and mania: Systematic reviews and economic modelling studies. Health Technol. Assess. 2005, 9, 1–156. [Google Scholar] [CrossRef]
- Aziz, M.; Mehringer, A.M.; Mozurkewich, E.; Razik, G.N. Cost-utility of 2 maintenance treatments for older adults with depression who responded to a course of electroconvulsive therapy: Results from a decision analytic model. Can. J. Psychiatry 2005, 50, 389–397. [Google Scholar] [PubMed]
- Rodriguez-Jimenez, R.; Bagney, A.; Torio, I.; Caballero, M.; Ruiz, P.; Rivas, F.D.P.J.; Jimenez-Arriero, M.A. Clinical usefulness and economic implications of continuation/maintenance electroconvulsive therapy in a Spanish National Health System public hospital: A case series. Rev. Psiquiatr. Salud Ment. 2015, 8, 75–82. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Clinical Excellence (NICE). Guidance on the Use of Electroconvulsive Therapy; Technology Appraisal Guidance 59; Last Modified: October 2009; NICE: London, UK, 2003; Available online: http://www.nice.org.uk/guidance/ta59 (accessed on 25 April 2021).
- Andrade, C.; Arumugham, S.S.; Thirthalli, J. Adverse Effects of Electroconvulsive Therapy. Psychiatr. Clin. N. Am. 2016, 39, 513–530. [Google Scholar] [CrossRef] [PubMed]
- Tørring, N.; Sanghani, S.N.; Petrides, G.; Kellner, C.H.; Østergaard, S.D. The mortality rate of electroconvulsive therapy: A systematic review and pooled analysis. Acta Psychiatr. Scand. 2017, 135, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.E.; Rasmussen, K.G.; Cullum, C.M.; Felmlee-Devine, M.D.; Petrides, G.; Rummans, T.A.; Husain, M.M.; Mueller, M.; Bernstein, H.J.; Knapp, R.G.; et al. A randomized controlled trial comparing the memory effects of continuation electroconvulsive therapy versus continuation pharmacotherapy: Results from the Consortium for Research in ECT (CORE) study. J. Clin. Psychiatry 2010, 71, 185–193. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; Revised; DSM-IV-R; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Sociedad Española de Psiquiatría. Consenso Español Sobre la Terapia Electroconvulsiva TEC. 1999. Available online: http://www.sepsiq.org/file/ConsensoTEC.pdf (accessed on 25 April 2021).
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Prien, R.F.; Jarrett, R.B.; Keller, M.B.; Kupfer, D.J.; Lavori, P.W.; Rush, A.J.; Weissman, M.M. Conceptualization and rationale for consensus definitions of terms in major depressive disorder. Remission, recovery, relapse, and recurrence. Arch. Gen. Psychiatry 1991, 48, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Hadzi-Pavlovic, D. Melancholia. A Disorder of Movement and Mood; Cambridge University Press: New York, NY, USA, 1996. [Google Scholar]
- Soria, V.; Vives, M.; Martínez-Amorós, E.; Gálvez, V.; Monzónn, S.; Crespo, J.M.; Gili, M.; Menchón, J.M.; Roca, M.; Parker, G.; et al. The CORE system for sub-typing melancholic depression: Adaptation and psychometric properties of the Spanish version. Psychiatry Res. 2016, 239, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Thase, M.E.; Rush, A.J. When at first you don’t succeed: Sequential strategies for antidepressant nonresponders. J. Clin. Psychiatry 1997, 58, 23–29. [Google Scholar] [PubMed]
- Okazaki, M.; Tominaga, K.; Higuchi, H.; Utagawa, I.; Nakamura, E.; Noguchi, M.; Itaya, M.; Hashimoto, C.; Yamaguchi, N. Predictors of response to electroconvulsive therapy obtained using the three-factor structure of the Montgomery and Asberg Depression Rating Scale for treatment-resistant depressed patients. J. ECT 2010, 26, 87–90. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; Revised; DSM-III-R; American Psychiatric Association: Washington, DC, USA, 1987. [Google Scholar]
- Guy, W. Early Clinical Drug Evaluation (ECDEU) Assessment Manual for Psychopharmacology; National Institute of Mental Health: Rockville, MD, USA, 1976; pp. 217–222. [Google Scholar]
- Knobel, H.; Alonso, J.; Casado, J.L.; Collazos, J.; González, J.; Ruiz, I.; Kindelan, J.M.; Carmona, A.; Juega, J.; Ocampo, A. Validation of a simplified medication adherence questionnaire in a large cohort of HIV-infected patients: The GEEMA study. AIDS 2002, 16, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Lingjærde, O.; Ahlfors, U.G.; Bech, P.; Dencker, S.J.; Elgen, K. The UKU side effect rating scale: A new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic-treated patients. Acta Psychiatr. Scand. 1987, 76, 1–100. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.L.; De La Cámara, C.; Ventura, T.; Asín, F.M.; Pascual, L.F.; Montañés, J.Á.; Aznar, S. Revalidación y normalización del mini-examen cognoscitivo (primera version en castellano del mini-mental status examination) en la población general geriátrica. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Swoboda, E.; Conca, A.; König, P.; Waanders, R.; Hansen, M. Maintenance electroconvulsive therapy in affective and schizoaffective disorder. Neuropsychobiology 2001, 43, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Sackeim, H.A.; Haskett, R.F.; Mulsant, B.H.; Thase, M.E.; Mann, J.J.; Pettinati, H.M.; Greenberg, R.M.; Crowe, R.R.; Cooper, T.B.; Prudic, J. Continuation pharmacotherapy in the prevention of relapse following electroconvulsive therapy: A randomized controlled trial. JAMA 2001, 285, 1299–1307. [Google Scholar] [CrossRef]
- Petrides, G.; Fink, M.; Husain, M.M.; Knapp, R.G.; Rush, A.J.; Mueller, M.; Rummans, T.A.; O’Connor, K.M.; Rasmussen, K.G.; Bernstein, H.J.; et al. ECT remission rates in psychotic versus nonpsychotic depressed patients: A report from CORE. J. ECT 2001, 17, 244–253. [Google Scholar] [CrossRef]
- Van Diermen, L.; Van Den Ameele, S.; Kamperman, A.M.; Sabbe, B.C.G.; Vermeulen, T.; Schrijvers, D.; Birkenhäger, T.K. Prediction of electroconvulsive therapy response and remission in major depression: Meta-analysis. Br. J. Psychiatry 2018, 212, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Huuhka, K.; Viikki, M.; Tammentie, T.; Tuohimaa, K.; Björkqvist, M.; Alanen, H.-M.; Leinonen, E.; Kampman, O. One-year follow-up after discontinuing maintenance electroconvulsive therapy. J. ECT 2012, 28, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Amorós, E.; Serra, P.; Goldberg, X.; Urraca, L.; Palao, D.J.; Urretavizcaya, M.; Cardoner, N. Clinical outcome after discontinuation of maintenance Electroconvulsive Therapy. A retrospective follow-up study. Rev. Psiquiatr. Salud Ment. 2020, 13, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Lisanby, S.H.; Sampson, S.; Husain, M.M.; Petrides, G.; Knapp, R.G.; McCall, V.; Young, R.C.; Prudic, J.; Kellner, C.H. Toward individualized post-electroconvulsive therapy care: Piloting the symptom-titrated, algorithm-based longitudinal ECT (STABLE) intervention. J. ECT 2008, 24, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.P.; Kellner, C.H. Clinical Practice Recommendations for Continuation and Maintenance Electroconvulsive Therapy for Depression: Outcomes from a Review of the Evidence and a Consensus Workshop Held in Australia in May 2017. J. ECT 2019, 35, 14–20. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| M-Pharm/ECT Group n = 18 | M-Pharm Group n = 18 | p-Value | |
|---|---|---|---|
| Serotonin selective reuptake inhibitor, % (n) | 5.6 (1) | 16.7 (3) | 0.603 b |
| Serotonin norepinephrine reuptake inhibitor, % (n) | 77.8 (14) | 83.3 (15) | 1.000 b |
| Noradrenergic and specific serotonergic antidepressant, % (n) | 44.4 (8) | 38.9 (7) | 0.735 a |
| Tricyclics, % (n) | 33.3 (6) | 27.8 (5) | 0.717 a |
| Other antidepressants, % (n) | 22.2 (4) | 11.1 (2) | 0.658 b |
| Lithium, % (n) | 5.6 (1) | 0 (0) | 1.000 b |
| Antipsychotics, % (n) | 44.4 (8) | 83.3 (15) | 0.035 b |
| Benzodiazepines, % (n) | 77.8 (14) | 61.1 (11) | 0.471 b |
| M-Pharm/ECT Group (n = 18) | M-Pharm Group (n = 18) | p-Value | |
|---|---|---|---|
| Demographic and course of the disorder characteristics | |||
| Sex (female), % (n) | 72.2 (13) | 61.1 (11) | 0.480 a |
| Age, median (min-max), years | 69 (34–81) | 67 (52–77) | 0.889 d |
| Age at illness onset *, mean (SD), years | 49.9 (15.2) | 50.8 (18) | 0.877 c |
| Recurrent MDD, % (n) | 94.4 (17) | 66.7 (12) | 0.088 a |
| Prior episodes, median (min-max) | 3.0 (1–10) | 3.0 (1–12) | 0.591 d |
| Use of ECT in previous episodes, % (n) | 38.9 (7) | 27.8 (5) | 0.480 b |
| Characteristics of the index episode | |||
| Melancholic symptoms, % (n) | 94.4 (17) | 100 (18) | 1.000 b |
| Psychotic symptoms, % (n) | 44.5 (8) | 72.3 (13) | 1.000 b |
| Catatonic symptoms, % (n) | 11.1 (2) | 5.6 (1) | 1.000 b |
| Duration of current episode, median (min-max), years | 0.4 (0.1–2.7) | 0.5 (0.1–4.1) | 0.527 d |
| Treatment-resistant depression, % (n) | 55.6 (10) | 33.3 (6) | 0.180 b |
| Acute ECT sessions, median (min-max) | 10.5 (7.0–17.0) | 12.0 (7.0–21.0) | 0.191 d |
| Characteristics at baseline | |||
| HDRS21, median (min-max) | 3.0 (0.0–6.0) | 2.0 (0.0–6.0) | 0.834 d |
| CGI-S, median (min-max) | 1 (1–2) | 1 (1–2) | 0.971 d |
| CORE system, median (min-max) | 1.0 (0.0–4.0) | 1.0 (0.0–6.0) | 0.268 d |
| GAF, median (min-max) | 80 (70–90) | 80 (70–90) | 0.739 d |
| MMSE, mean (SD) | 25.67 (3.87) | 24.75 (4.19) | 0.512 c |
| Model | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value * |
|---|---|---|---|---|
| Model 1 Treatment (Pharm) | 2.3 (0.85–6.23) | 0.102 | ||
| Model 2 Treatment (Pharm) Psychosis (without) Age (>67 years) | 2.79 (0.998–7.771) 3.57 (1.226–10.382) 0.44 (0.146–1.306) | 0.050 0.020 0.138 | 3.17 (1.141–8.781) 4.56 (1.622–12.822) - - - - | 0.027 0.004 - - - - |
| Active M-ECT | Stop M-ECT * | ||||
|---|---|---|---|---|---|
| 3 Months | 6 Months | 9 Months | 12 Months | 15 Months | |
| M-Pharm/ECT group | 88.2 (72.9–103.5) | 64.7 (42.0–87.4) | 64.7 (42.0–87.4) | 57.5 (33.3–81.7) | 38.3 (3.6–73) |
| M-Pharm group | 72.2 (51.5–92.9) | 42.1 (18.6–65.6) | 36.1 (13.2–59.0) | 36.1 (13.2–59) | 36.1 (13.2–59) |
| M-Pharm/ECT Group (n = 17) | M-Pharm Group (n = 18) | p-Value | |
|---|---|---|---|
| Mean (SD); Median (Min-Max) | Mean (SD); Median (Min-Max) | ||
| HDRS-21 at baseline | 3.1 (1.6); 3.0 (0.5–5.5) | 3.1 (1.8); 3.0 (0.0–6.0) | 0.915 a |
| HDRS-21 at 15 months | 9.5 (10.1); 3.0 (0.0–25.0) | 15.4 (11.7); 17.5 (0.0–35.0) | 0.209 b |
| p-Value * | 0.125 d | < 0.001 c | |
| CGI-S at baseline | 1.4 (0.4); 1.0 (1.0–2.0) | 1.4 (0.5); 1.0 (1.0–2.0) | 0.926 b |
| CGI-S at 15 months | 2.5 (1.6); 1.5 (1.0–5.0) | 3.4 (1.8); 4.0 (1.0–6.0) | 0.171 b |
| p-Value * | 0.016 d | 0.001 d |
| M-Pharm/ECT Group (n = 5) | M-Pharm Group (n = 7) | p-Value | |
|---|---|---|---|
| MMSE at baseline, mean (SD) | 25.00 (5.1) | 24.20 (3.96) | 0.776 a |
| MMSE at 9 months, mean (SD) | 24.57 (5.35) | 27.40 (1.14) | 0.277 a |
| MMSE at 15 months, mean (SD) | 25.14 (4.34) | 27.80 (1.64) | 0.226 a |
| p-Value 1 p-Value 2 | 0.482 b | 0.145 b | |
| 0.924 b | 0.125 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Amorós, E.; Cardoner, N.; Gálvez, V.; de Arriba-Arnau, A.; Soria, V.; Palao, D.J.; Menchón, J.M.; Urretavizcaya, M. Can the Addition of Maintenance Electroconvulsive Therapy to Pharmacotherapy Improve Relapse Prevention in Severe Major Depressive Disorder? A Randomized Controlled Trial. Brain Sci. 2021, 11, 1340. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101340
Martínez-Amorós E, Cardoner N, Gálvez V, de Arriba-Arnau A, Soria V, Palao DJ, Menchón JM, Urretavizcaya M. Can the Addition of Maintenance Electroconvulsive Therapy to Pharmacotherapy Improve Relapse Prevention in Severe Major Depressive Disorder? A Randomized Controlled Trial. Brain Sciences. 2021; 11(10):1340. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101340
Chicago/Turabian StyleMartínez-Amorós, Erika, Narcís Cardoner, Verònica Gálvez, Aida de Arriba-Arnau, Virginia Soria, Diego J. Palao, José M. Menchón, and Mikel Urretavizcaya. 2021. "Can the Addition of Maintenance Electroconvulsive Therapy to Pharmacotherapy Improve Relapse Prevention in Severe Major Depressive Disorder? A Randomized Controlled Trial" Brain Sciences 11, no. 10: 1340. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101340