
Reflexive Gaze Shifts and Fear Recognition Deficits in Children with Callous-Unemotional Traits and Impulsivity/Conduct Problems

 ,
,
Abstract
:1. Introduction
1.1. Fearful Expressions Are Determined by Looking at Eye Regions
1.2. Reflexive Shifts in Eye Gaze as Automatic Attention
1.3. Current Study
2. Experiment 1
Directing Eye Gaze
3. Materials and Methods
3.1. Participants
3.2. Measures
3.2.1. Callous-Unemotional Traits
3.2.2. Anxiety
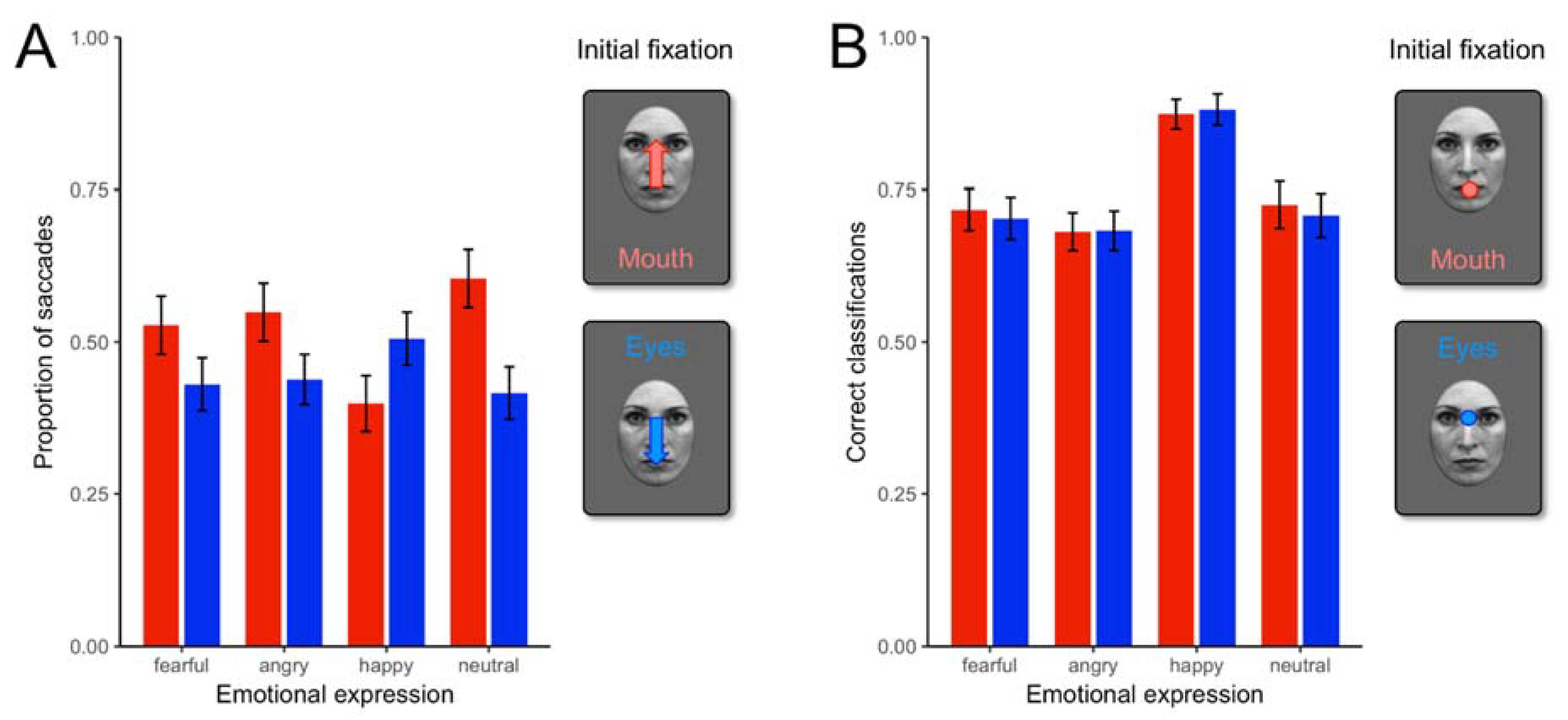
3.2.3. Face Perception Task
3.3. Procedure
4. Results
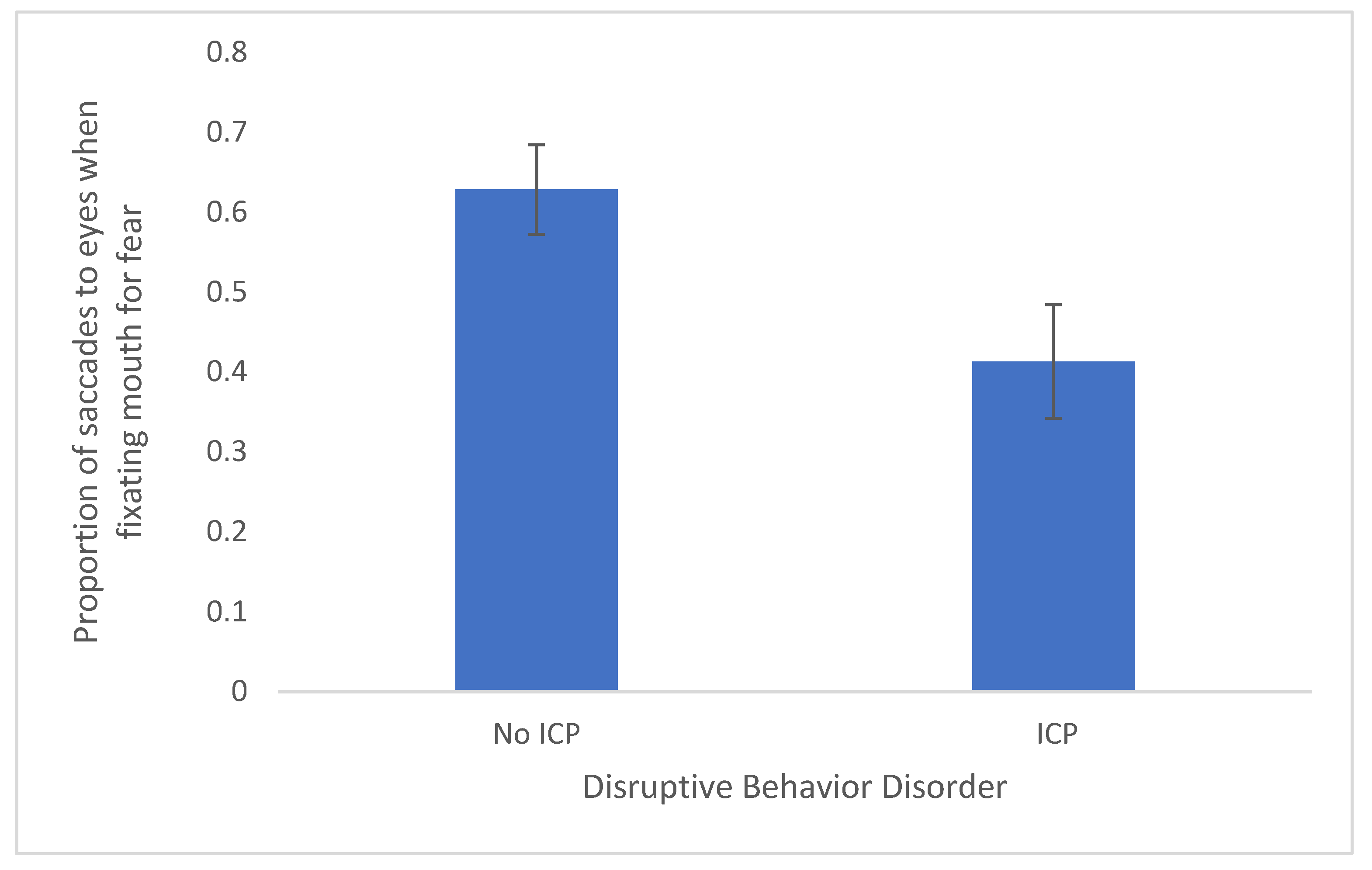
4.1. Are CU Traits and ICP Related to Lower Proportion of Reflexive Saccades toward the Eye Region When the Initial Fixation Is on the Mouth?
4.2. Are CU Traits Related to Fear Recognition Deficits?
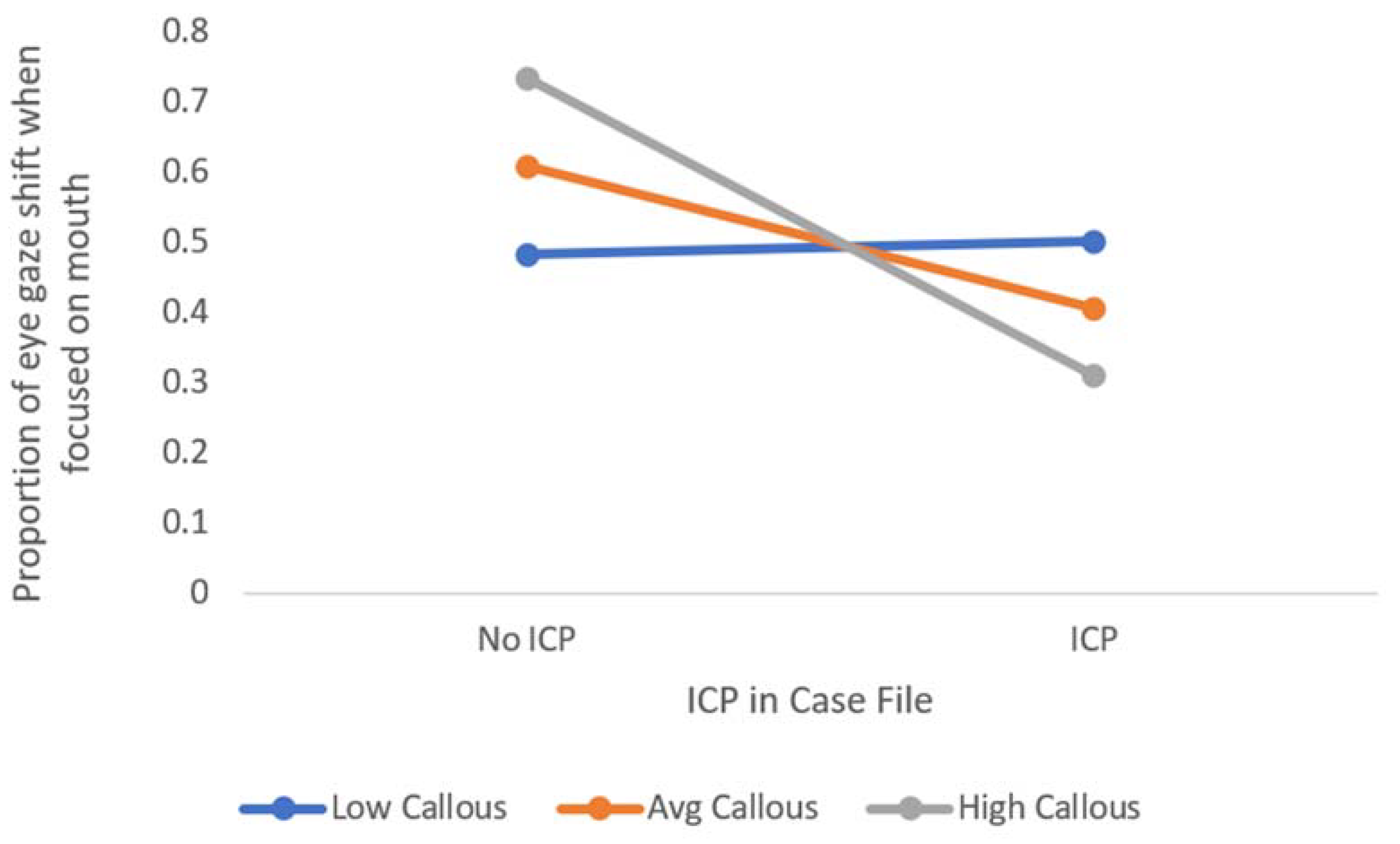
4.3. Do CU Traits Moderate the Relation between Impulsivity/Conduct Problems and Reflexive Gaze toward the Eye Region of Fearful Faces?
5. Discussion
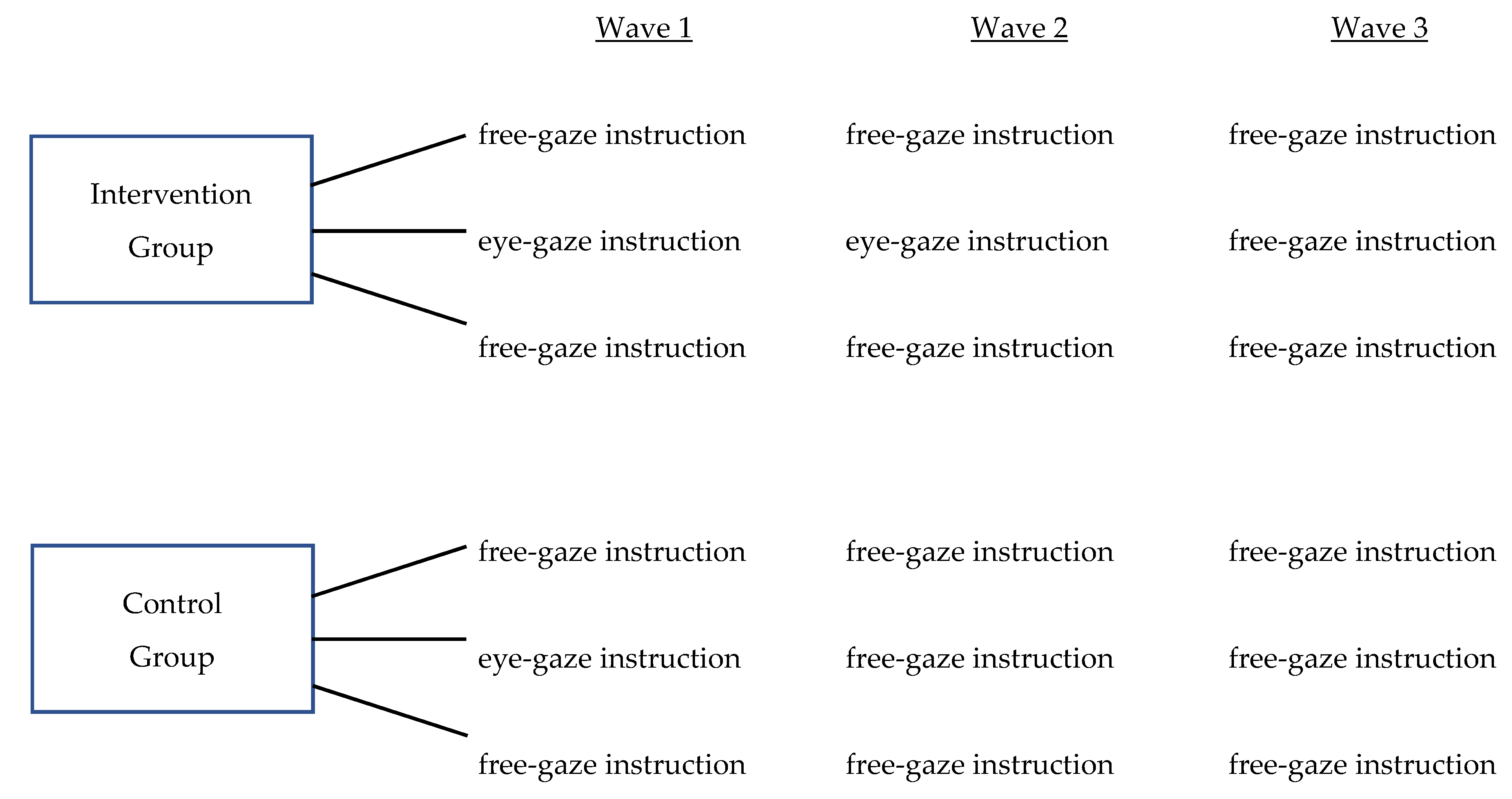
6. Experiment 2
7. Materials and Methods
7.1. Participants
7.2. Measures
7.2.1. Anxiety and Depression
7.2.2. Impulsivity/Conduct Problems (ICP)
7.2.3. Callous-Unemotional Traits
7.2.4. Empathy
7.2.5. Attention to Emotional Cues
7.2.6. Facial Emotion Recognition and Learning
7.3. Procedure
8. Results
8.1. Preliminary Analyses and Data Analytic Strategy
Missing Data
8.2. Descriptive Statistics
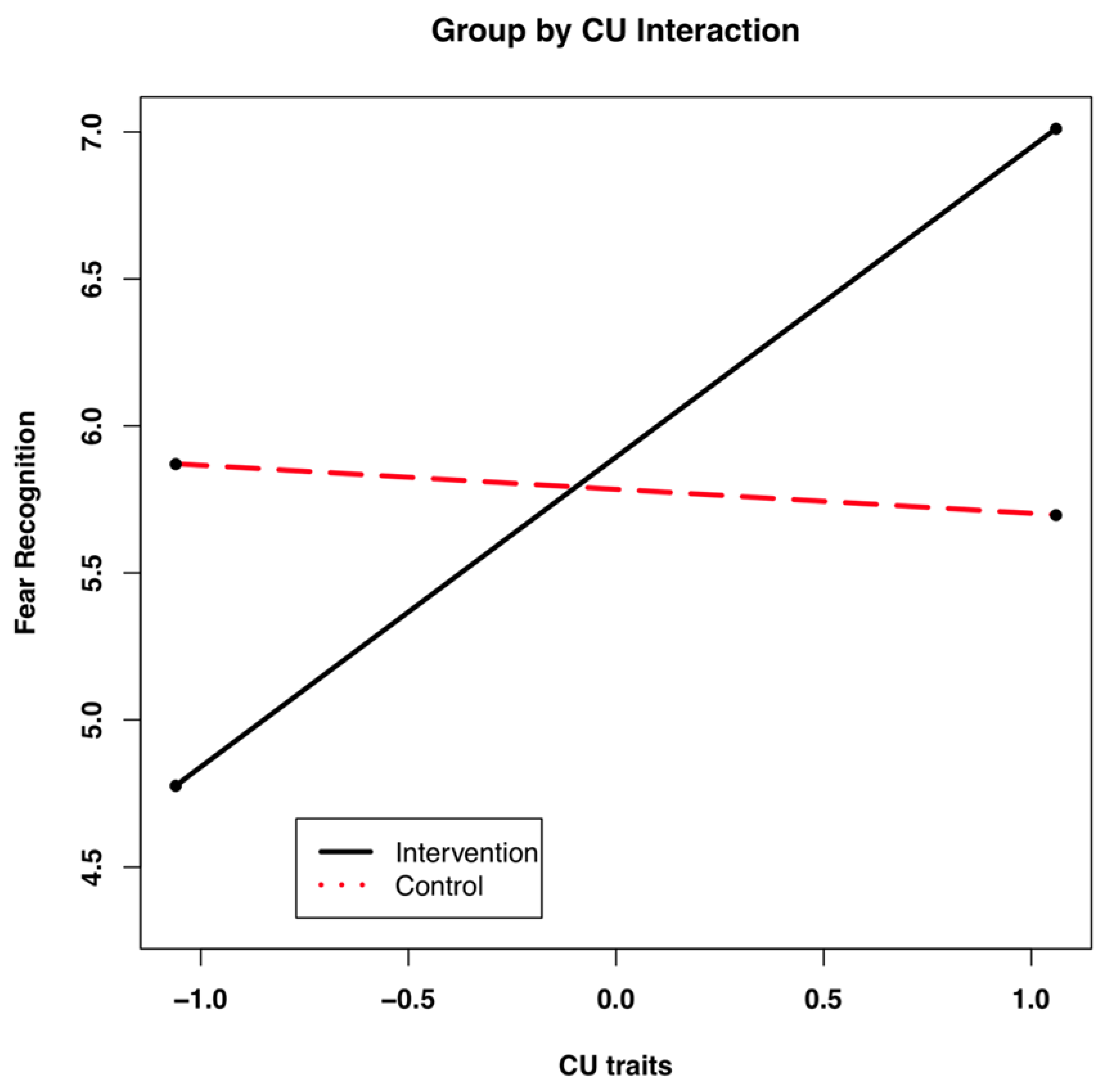
8.3. Trajectories of Fear Recognition Accuracy
8.4. CU Traits and Trajectories of Attention to Emotional Cues
8.5. CU Traits and Trajectories of Empathy
9. Discussion
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Dadds, M.R.; Perry, Y.; Hawes, D.J.; Merz, S.; Riddell, A.C.; Haines, D.J.; Solak, E.; Abeygunawardane, A.I. Attention to the eyes and fear-recognition deficits in child psychopathy. Br. J. Psychiatry 2006, 189, 280–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blair, R.J.R.; Colledge, E.; Murray, L.; Mitchell, D.G.V. A selective impairment in the processing of sad and fearful expressions in children with psychopathic tendencies. J. Abnorm. Child Psychol. 2001, 29, 491–498. [Google Scholar] [CrossRef]
- Muñoz, L.C. Callous-unemotional traits are related to combined deficits in recognizing afraid faces and body poses. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 554–562. [Google Scholar] [CrossRef] [Green Version]
- Bowen, K.L.; Morgan, J.E.; Moore, S.C.; van Goozen, S.H.M. Young Offenders’ Emotion Recognition Dysfunction Across Emotion Intensities: Explaining Variation Using Psychopathic Traits, Conduct Disorder and Offense Severity. J. Psychopathol. Behav. Assess. 2014, 36, 60–73. [Google Scholar] [CrossRef] [Green Version]
- Brook, M.; Brieman, C.L.; Kosson, D.S. Emotion processing in Psychopathy Checklist—Assessed psychopathy: A review of the literature. Clin. Psychol. Rev. 2013, 33, 979–995. [Google Scholar] [CrossRef]
- Milone, A.; Cerniglia, L.; Cristofani, C.; Inguaggiato, E.; Levantini, V.; Masi, G.; Paciello, M.; Simone, F.; Muratori, P. Empathy in Youths with Conduct Disorder and Callous-Unemotional Traits. Neural Plast. 2019, 2019, 9638973. [Google Scholar] [CrossRef] [Green Version]
- Boll, S.; Gamer, M. Psychopathic traits affect the visual exploration of facial expressions. Biol. Psychol. 2016, 117, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Gamer, M.; Büchel, C. Amygdala activation predicts gaze toward fearful eyes. J. Neurosci. Off. J. Soc. Neurosci. 2009, 29, 9123–9126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.L.; Cottrell, G.W.; Gosselin, F.; Schyns, P.G. Transmitting and Decoding Facial Expressions. Psychol. Sci. 2005, 16, 184–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adolphs, R. Neural systems for recognizing emotion. Curr. Opin. Neurobiol. 2002, 12, 169–177. [Google Scholar] [CrossRef]
- Jhou, T.C.; Fields, H.L.; Baxter, M.G.; Saper, C.B.; Holland, P.C. The rostromedial tegmental nucleus (RMTg), a major GABAergic afferent to midbrain dopamine neurons, selectively encodes aversive stimuli and promotes behavioral inhibition. Neuron 2009, 61, 786–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adolphs, R.; Gosselin, F.; Buchanan, T.W.; Tranel, D.; Schyns, P.; Damasio, A.R. A mechanism for impaired fear recognition after amygdala damage. Nature 2005, 433, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Gamer, M.; Schmitz, A.K.; Tittgemeyer, M.; Schilbach, L. The human amygdala drives reflexive orienting towards facial features. Curr. Biol. 2013, 23, R917–R918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adolphs, R.; Tranel, D.; Damasio, H.; Damasio, A. Impaired recognition of emotion in facial expressions following bilateral damage to the human amygdala. Nature 1994, 372, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Blair, R.J.R. The amygdala and ventromedial prefrontal cortex in morality and psychopathy. Trends Cogn. Sci. 2007, 11, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Moul, C.; Killcross, S.; Dadds, M.R. A Model of Differential Amygdala Activation in Psychopathy. Psychol. Rev. 2012, 119, 789–806. [Google Scholar] [CrossRef]
- Scheller, E.; Büchel, C.; Gamer, M. Diagnostic Features of Emotional Expressions Are Processed Preferentially. PLoS ONE 2012, 7, e41792. [Google Scholar] [CrossRef]
- Jones, A.P.; Laurens, K.R.; Herba, C.M.; Barker, G.J.; Viding, E. Amygdala hypoactivity to fearful faces in boys with conduct problems and callous-unemotional traits. Am. J. Psychiatry 2009, 166, 95–102. [Google Scholar] [CrossRef]
- Cardinale, E.M.; O’Connell, K.; Robertson, E.L.; Meena, L.B.; Breeden, A.L.; Lozier, L.M.; VanMeter, J.W.; Marsh, A.A. Callous and uncaring traits are associated with reductions in amygdala volume among youths with varying levels of conduct problems. Psychol. Med. 2018, 49, 1–10. [Google Scholar] [CrossRef]
- Sebastian, C.L.; McCrory, E.J.; Dadds, M.R.; Cecil, C.A.M.; Lockwood, P.L.; Hyde, Z.H.; De Brito, S.A.; Viding, E. Neural responses to fearful eyes in children with conduct problems and varying levels of callous–unemotional traits. Psychol. Med. 2013, 44, 99–109. [Google Scholar] [CrossRef] [Green Version]
- Frick, P.J. The Inventory of Callous-Unemotional Traits; The University of New Orleans: New Orleans, LA, USA, 2004. [Google Scholar]
- Kimonis, E.R.; Frick, P.J.; Skeem, J.L.; Marsee, M.A.; Cruise, K.; Muñoz, L.C.; Aucoin, K.J.; Morris, A.S. Assessing callous-unemotional traits in adolescent offenders: Validation of the Inventory of Callous-Unemotional Traits. Int. J. Law Psychiatry 2008, 31, 241–252. [Google Scholar] [CrossRef] [Green Version]
- Lui, J.H.L.; Barry, C.T.; Sacco, D.F. Callous-unemotional traits and empathy deficits: Mediating effects of affective perspective-taking and facial emotion recognition. Cogn. Emot. 2015, 30, 1049–1062. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, L.C.; Qualter, P.; Padgett, G. Empathy and bullying: Exploring the influence of callous-unemotional traits. Child Psychiatry Hum. Dev. 2010, 42, 183–196. [Google Scholar] [CrossRef]
- Reynolds, C.; Kamphaus, R. BASC-2 Behavior Assessment for Children Manual; American Guidance Service: Circle Pines, MN, USA, 2004. [Google Scholar]
- Frick, P.; Barry, C.; Kamphaus, R. Clinical Assessment of Child and Adolescent Personality and Behavior; Springer Science + Business Media: New York, NY, USA, 2010. [Google Scholar]
- Ekman, P.; Friesen, W.V.; Tomkins, S.S. Facial Affect Scoring Technique: A First Validity Study. Semiotica 1971, 3, 37–58. [Google Scholar] [CrossRef]
- Ebner, N.C.; Riediger, M.; Lindenberger, U. FACES—A database of facial expressions in young, middle-aged, and older women and men: Development and validation. Behav. Res. Methods 2010, 42, 351–362. [Google Scholar] [CrossRef]
- JASP Team. JASP (Version 0.14.1). 2020. [Google Scholar]
- Hayes, A.F. The PROCESS macro for SPSS and SAS (version 2.13). 2015.
- Eisenberg, N.; Wentzel, M.; Harris, J.D. The Role of Emotionality and Regulation in Empathy-Related Responding. Sch. Psychol. Rev. 1998, 27, 506–521. [Google Scholar] [CrossRef]
- Centifanti, L.C.M.; Gillespie, S.M.; Thomson, N.D. Skin conductance responses to a discrete threat in virtual reality: Associations with psychopathy and anxiety. J. Psychopathol. Behav. Assess. In press.
- Cardinale, E.M.; Ryan, R.M.; Marsh, A.A. Maladaptive Fearlessness: An Examination of the Association Between Subjective Fear Experience and Antisocial Behaviors Linked With Callous Unemotional Traits. J. Personal. Disord. 2021, 35 (Suppl. A), 39–56. [Google Scholar] [CrossRef] [PubMed]
- Dadds, M.R.; El masry, Y.; Wimalaweera, S.; Guastella, A.J. Reduced Eye Gaze Explains “Fear Blindness” in Childhood Psychopathic Traits. J. Am. Acad. Child. Adolesc. Psychiatry 2008, 47, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Chorpita, B.F.; Yim, L.; Moffitt, C.; Umemoto, L.A.; Francis, S.E. Assessment of symptoms of DSM-IV anxiety and depression in children: A revised child anxiety and depression scale. Behav. Res. Ther. 2000, 38, 835–855. [Google Scholar] [CrossRef]
- Frick, P.J.; Hare, R.D. The Antisocial Process Screening Device; Multi-Health Systems: Toronto, ON, Canada, 2001. [Google Scholar]
- Essau, C.A.; Sasagawa, S.; Frick, P.J. Callous-unemotional traits in a community sample of adolescents. Assessment 2006, 13, 454–469. [Google Scholar] [CrossRef] [PubMed]
- Frick, P.J.; O’Brien, B.S.; Wootton, J.M.; McBurnett, K. Psychopathy and conduct problems in children. J. Abnorm. Psychol. 1994, 103, 700–707. [Google Scholar] [CrossRef]
- Poythress, N.G.; Douglas, K.S.; Falkenbach, D.; Cruise, K.; Lee, Z.; Murrie, D.C.; Vitacco, M. Internal Consistency Reliability of the Self-Report Antisocial Process Screening Device. Assessment 2006, 13, 107–113. [Google Scholar] [CrossRef]
- Muñoz, L.C.; Frick, P.J. The reliability, stability, and predictive utility of the self-report version of the Antisocial Process Screening Device. Scand. J. Psychol. 2007, 48, 299–312. [Google Scholar] [CrossRef] [Green Version]
- Stickle, T.R.; Kirkpatrick, N.M.; Brush, L.N. Callous-unemotional traits and social information processing: Multiple risk-factor models for understanding aggressive behavior in antisocial youth. Law Hum. Behav. 2009, 33, 515–529. [Google Scholar] [CrossRef] [PubMed]
- Eysenck, S.B.G.; Easting, G.; Pearson, P.R. Age norms for impulsiveness, venturesomeness and empathy in children. Personal. Individ Differ. 1984, 5, 315–321. [Google Scholar] [CrossRef]
- Crowley, T.J.; Raymond, K.M.; Mikulich-Gilbertson, S.K.; Thompson, L.L.; Lejuez, C.W. A risk-taking “set” in a novel task among adolescents with serious conduct and substance problems. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 175–183. [Google Scholar] [CrossRef]
- Davis, M.H. A multidimensional approach to individual differences in empathy. JSAS Cat Sel. Doc. Psychol. 1980, 10, 85–104. [Google Scholar]
- Davis, M.H. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Personal. Soc Psychol. 1983, 44, 113–126. [Google Scholar] [CrossRef]
- Davis, M.H.; Franzoi, S.L. Stability and change in adolescent self-consciousness and empathy. J. Res. Personal. 1991, 25, 70–87. [Google Scholar] [CrossRef]
- Loney, B.R.; Frick, P.J.; Clements, C.B.; Ellis, M.L.; Kerlin, K. Callous-unemotional traits, impulsivity, and emotional processing in antisocial adolescents. J. Clin. Child. Adolesc. Psychol. 2003, 32, 139–152. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, C.; Mathews, A.; Tata, P. Attentional bias in emotional disorders. J. Abnorm. Psychol. 1986, 95, 15. [Google Scholar] [CrossRef]
- Vasey, M.W.; Daleidon, E.L.; Williams, L.L.; Brown, L.M. Biased attention in childhood anxiety disorders: A preliminary study. J. Abnorm. Child Psychol. 1995, 23, 267–279. [Google Scholar] [CrossRef]
- Mogg, K.; Bradley, B.P. Orienting of Attention to Threatening Facial Expressions Presented under Conditions of Restricted Awareness. Cogn. Emot. 1999, 13, 713–740. [Google Scholar] [CrossRef]
- Schippell, P.L.; Vasey, M.W.; Cravens-Brown, L.M.; Bretveld, R.A. Suppressed attention to rejection, ridicule, and failure cues: A unique correlate of reactive but not proactive aggression in youth. J. Clin. Child. Adolesc. Psychol. 2003, 32, 40–55. [Google Scholar] [CrossRef] [PubMed]
- Kimonis, E.R.; Frick, P.J.; Fazekas, H.; Loney, B.R. Psychopathy, aggression, and the processing of emotional stimuli in non-referred children. Behav. Sci. Law 2006, 24, 21–37. [Google Scholar] [CrossRef]
- Lang, P.J.; Bradley, M.M.; Cuthbert, B.N. International Affective Picture System (IAPS): Technical Manual and Affective Ratings; NIMH Center for the Study of Emotion and Attention: Gainesville, FL, USA, 1997. [Google Scholar]
- Kimonis, E.R.; Frick, P.J.; Boris, N.W.; Smyke, A.T.; Cornell, A.H.; Farrell, J.M.; Zeanah, C.H. Callous-unemotional features, behavioral inhibition, and parenting: Independent predictors of aggression in a high-risk preschool sample. J. Child Fam. Stud. 2006, 15, 741–752. [Google Scholar] [CrossRef]
- MacLeod, C.; Mathews, A. Anxiety and the allocation of attention to threat. J. Exp. Psychol. Hum. Exp. Psychol. 1988, 40, 653–670. [Google Scholar] [CrossRef]
- Dadds, M.; Hawes, D.; Merz, S. The UNSW Facial Emotion Task; University of New South Wales: Sydney, Australia, 2004. [Google Scholar]
- Marini, V.A.; Stickle, T.R. Evidence for deficits in reward responsivity in antisocial youth with callous-unemotional traits. Personal. Disord. Theory Res. Treat. 2010, 1, 218–229. [Google Scholar] [CrossRef] [PubMed]
- Stickle, T.R.; Marini, V.A.; Thomas, J.N. Gender differences in psychopathic traits, types, and correlates of aggression among adjudicated youth. J. Abnorm. Child Psychol. 2011, 40, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Allison, P.D. Multiple Imputation for Missing Data. Sociol. Methods Res. 2000, 28, 301–309. [Google Scholar] [CrossRef] [Green Version]
- Little, R.J.A.; Rubin, D.B. The Analysis of Social Science Data with Missing Values. Sociol. Methods Res. 1989, 18, 292–326. [Google Scholar] [CrossRef]
- Schafer, J.L.; Graham, J.W. Missing data: Our view of the state of the art. Psychol. Methods 2002, 7, 147–177. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.W. Missing data analysis: Making it work in the real world. Annu. Rev. Psychol. 2009, 60, 549–576. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.B. The calculation of posterior distributions by data augmentation: Comment: A noniterative sampling/importance resampling alternative to the data augmentation algorithm for creating a few imputations when fractions of missing information are modest: The SIR algorithm. J. Am. Stat. Assoc. 1987, 82, 543–546. [Google Scholar]
- Bollen, K.A.; Curran, P.J. Latent Curve Models: A Structural Equation Perspective; Wiley-Interscience; John Wiley & Sons: Hoboken, NJ, USA, 2006; 285p. [Google Scholar]
- Frick, P.J.; Stickle, T.R.; Dandreaux, D.M.; Farrell, J.M.; Kimonis, E.R. Callous-unemotional traits in predicting the severity and stability of conduct problems and delinquency. J. Abnorm. Child Psychol. 2005, 33, 471–487. [Google Scholar] [CrossRef]
- West, B.T. Analyzing Longitudinal Data With the Linear Mixed Models Procedure in SPSS. Eval Health Prof. 2009, 32, 207–228. [Google Scholar] [CrossRef]
- Preacher, K.J.; Curran, P.J.; Bauer, D.J. Computational Tools for Probing Interactions in Multiple Linear Regression, Multilevel Modeling, and Latent Curve Analysis. J. Educ. Behav. Stat. 2006, 31, 437–448. [Google Scholar] [CrossRef]
- Schwenck, C.; Gensthaler, A.; Romanos, M.; Freitag, C.M.; Schneider, W.; Taurines, R. Emotion recognition in girls with conduct problems. Eur. Child Adolesc. Psychiatry 2013, 23, 13–22. [Google Scholar] [CrossRef]
- Aniskiewicz, A.S. Autonomic components of vicarious conditioning and psychopathy. J. Clin. Psychol. 1979, 35, 60–67. [Google Scholar] [CrossRef]
- House, T.H.; Milligan, W.L. Autonomic responses to modeled distress in prison psychopaths. J. Personal. Soc Psychol. 1976, 34, 556–560. [Google Scholar] [CrossRef]
- Hare, R.D. Temporal gradient of fear arousal in psychopathy. J. Abnorm. Psychol. 1965, 7, 442–445. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Baker, L.A.; Gao, Y.; Raine, A.; Lozano, D.I. Psychopathic Traits and Physiological Responses to Aversive Stimuli in Children Aged 9–11 Years. J. Abnorm. Child Psychol. 2012, 40, 759–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sethi, A.; O’Nions, E.; McCrory, E.; Bird, G.; Viding, E. An fMRI investigation of empathic processing in boys with conduct problems and varying levels of callous-unemotional traits. NeuroImage Clin. 2018, 18, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Dadds, M.R.; English, T.; Wimalaweera, S.; Schollar-Root, O.; Hawes, D.J. Can reciprocated parent–child eye gaze and emotional engagement enhance treatment for children with conduct problems and callous-unemotional traits: A proof-of-concept trial. J. Child Psychol. Psychiatry 2018, 60, 676–685. [Google Scholar] [CrossRef]
- Kleberg, J.L.; Selbing, I.; Lundqvist, D.; Hofvander, B.; Olsson, A. Spontaneous eye movements and trait empathy predict vicarious learning of fear. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2015, 98, 577–583. [Google Scholar] [CrossRef] [PubMed]
- White, S.F.; Cruise, K.R.; Frick, P.J. Differential correlates to self-report and parent-report of callous–unemotional traits in a sample of juvenile sexual offenders. Behav. Sci. Law 2009, 27, 910–928. [Google Scholar] [CrossRef]
- de Wied, M.; van Boxtel, A.; Matthys, W.; Meeus, W. Verbal, facial and autonomic responses to empathy-eliciting film clips by disruptive male adolescents with high versus low callous-unemotional traits. J. Abnorm. Child. Psychol. 2012, 40, 211–223. [Google Scholar] [CrossRef] [Green Version]
- Meffert, H.; Gazzola, V.; den Boer, J.A.; Bartels, A.A.J.; Keysers, C. Reduced spontaneous but relatively normal deliberate vicarious representations in psychopathy. Brain 2013, 136, 2550–2562. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Anger-fix eye | — | ||||||||||||||||
| 2. Anger-fix mouth | −0.29 | ** | — | ||||||||||||||
| 3. Fear-fix eye | 0.63 | *** | −0.25 | ** | — | ||||||||||||
| 4. Fear-fix mouth | −0.29 | ** | 0.65 | *** | −0.27 | ** | — | ||||||||||
| 5. Happy-fix eye | 0.56 | *** | −0.12 | 0.56 | *** | −0.15 | — | ||||||||||
| 6. Happy-fix mouth | −0.32 | *** | 0.66 | *** | −0.28 | ** | 0.58 | *** | −0.18 | — | |||||||
| 7. Neutral-fix eye | 0.54 | *** | −0.33 | *** | 0.61 | *** | −0.35 | *** | 0.54 | *** | −0.33 | *** | — | ||||
| 8. Neutral-fix mouth | −0.33 | *** | 0.65 | *** | −0.25 | ** | 0.62 | *** | −0.18 | 0.51 | *** | −0.32 | *** | — | |||
| 9. ICU total | 0.004 | −0.08 | −0.09 | −0.08 | −0.13 | −0.01 | 0.02 | −0.06 | — | ||||||||
| 10. Anxiety | −0.18 | 0.11 | −0.10 | 0.10 | −0.06 | 0.13 | 0.02 | 0.03 | 0.05 | — | |||||||
| 11. Age | −0.03 | 0.09 | −0.07 | −0.05 | 0.05 | 0.07 | −0.11 | −0.08 | 0.09 | −0.14 | |||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Anger-fix eye | — | ||||||||||||||
| 2. Anger-fix mouth | 0.47 | *** | — | ||||||||||||
| 3. Fear-fix eye | 0.26 | ** | 0.26 | ** | — | ||||||||||
| 4. Fear-fix mouth | 0.24 | * | 0.14 | 0.47 | *** | — | |||||||||
| 5. Happy-fix eye | 0.10 | 0.02 | 0.23 | * | 0.15 | — | |||||||||
| 6. Happy-fix mouth | 0.26 | * | 0.16 | 0.15 | 0.10 | 0.16 | — | ||||||||
| 7. Neutral-fix eye | 0.28 | ** | 0.35 | *** | 0.43 | *** | 0.2 | * | 0.17 | 0.09 | — | ||||
| 8. Neutral-fix mouth | 0.18 | 0.08 | 0.31 | ** | 0.33 | *** | 0.15 | −0.06 | 0.43 | *** | — | ||||
| 9. ICU total | 0.02 | 0.08 | −0.13 | −0.20 | * | −0.16 | −0.07 | −0.03 | −0.18 | — | |||||
| 10. Anxiety | 0.04 | −0.04 | 0.01 | 0.11 | −0.03 | −0.09 | 0.03 | 0.06 | 0.05 | — | |||||
| 11. Age | −0.01 | −0.06 | −0.12 | 0.082 | 0.19 | 0.27 | −0.11 | −0.10 | 0.09 | −0.14 | |||||
| CU Traits | Imp (APSD) | Imp (EIS) | W1 FACES Fear | W2 FACES Fear | W3 FACES Fear | W1 Fac Threat | W2 Fac Threat | W3 Fac Threat | IRI PT | IRI EC | M (SD) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CU Traits | -- | 27.65 (9.84) | ||||||||||
| Imp (APSD) | 0.51 ** | -- | 6.77 (2.06) | |||||||||
| Imp (EIS) | 0.24 | 0.61 ** | -- | 15.47 (2.92) | ||||||||
| W1 FACES Fear | −0.16 | −0.03 | −0.01 | -- | 5.30 (0.99) | |||||||
| W2 FACES Fear | 0.22 | 0.39 * | 0.17 | 0.63 ** | -- | 5.73 (0.69) | ||||||
| W3 FACES Fear | 0.14 | 0.33 | 0.10 | 0.73 ** | 0.90 ** | -- | 5.83 (0.65) | |||||
| W1 Fac Threat | 0.06 | 0.05 | 0.06 | 0.00 | 0.00 | −0.01 | -- | 17.62 (89.23) | ||||
| W2 Fac Threat | 0.07 | 0.21 | −0.04 | 0.62 ** | 0.77 ** | 0.76 ** | −0.04 | -- | −4.00 (107.91) | |||
| W3 Fac Threat | −0.04 | −0.27 | −0.14 | −0.31 | −0.55 ** | −0.55 ** | 0.04 | −0.41 * | -- | −9.38 (133.57) | ||
| IRI PT | −0.45 * | −0.46 * | −0.23 | 0.32 | 0.04 | 0.12 | 0.29 | 0.18 | 0.14 | -- | 12.83 (4.92) | |
| IRI EC | −0.56 ** | −0.43 * | −0.20 | −0.02 | −0.15 | −0.10 | 0.11 | 0.00 | 0.11 | 0.62 ** | -- | 15.60 (6.20) |
| Fixed Effects | Model A | Model B | Model C |
|---|---|---|---|
| Intercept | 5.56 *** | 5.56 *** | 5.98 *** |
| Time | 0.13 ** | 0.01 | 0.12 |
| Group | −0.00 | −0.37 | |
| CU Traits | 2.64 * | ||
| ICP: APSD | 0.25 * | ||
| Impulsivity: EIS | −0.12 | ||
| Sex | 0.38 | ||
| Group × Time | 0.08 | −0.02 | |
| Group × CU Traits | −1.51 * | ||
| CU Traits × Time | −0.29 | ||
| Group × Time × CU Traits | 0.19 | ||
| Model Comparisons | |||
| ∆ deviance (AIC) from Model A | −2.90 | 31.23 | |
| ∆ deviance (AIC) from Model B | 34.13 | ||
| ∆ deviance (BIC) from Model A | −2.76 | 33.74 | |
| ∆ deviance (BIC) from Model B | 36.50 | ||
| Parameters | Estimate | S.E. | z-Score |
|---|---|---|---|
| Simple Intercepts: | |||
| Intervention Group | 5.72 | 0.23 | 24.87 *** |
| Control Group | 1.22 | 0.56 | 2.19 * |
| Simple Slopes: | |||
| Intervention Group | 5.80 | 0.24 | 24.54 *** |
| Control Group | −0.10 | 0.42 | 0.22 + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz Centifanti, L.C.; Stickle, T.R.; Thomas, J.; Falcón, A.; Thomson, N.D.; Gamer, M. Reflexive Gaze Shifts and Fear Recognition Deficits in Children with Callous-Unemotional Traits and Impulsivity/Conduct Problems. Brain Sci. 2021, 11, 1342. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101342
Muñoz Centifanti LC, Stickle TR, Thomas J, Falcón A, Thomson ND, Gamer M. Reflexive Gaze Shifts and Fear Recognition Deficits in Children with Callous-Unemotional Traits and Impulsivity/Conduct Problems. Brain Sciences. 2021; 11(10):1342. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101342
Chicago/Turabian StyleMuñoz Centifanti, Luna C., Timothy R. Stickle, Jamila Thomas, Amanda Falcón, Nicholas D. Thomson, and Matthias Gamer. 2021. "Reflexive Gaze Shifts and Fear Recognition Deficits in Children with Callous-Unemotional Traits and Impulsivity/Conduct Problems" Brain Sciences 11, no. 10: 1342. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101342