
An Effortful Approach to Social Affiliation in Schizophrenia: Preliminary Evidence of Increased Theta and Alpha Connectivity during a Live Social Interaction


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Materials
2.2.1. Psychosis Symptoms
2.2.2. Social Interaction Task
2.2.3. Post-Interaction Ratings
2.3. EEG Recording and Preprocessing
2.4. Functional Connectivity
2.5. Statistical Analyses
3. Results
3.1. Post-Interaction Ratings
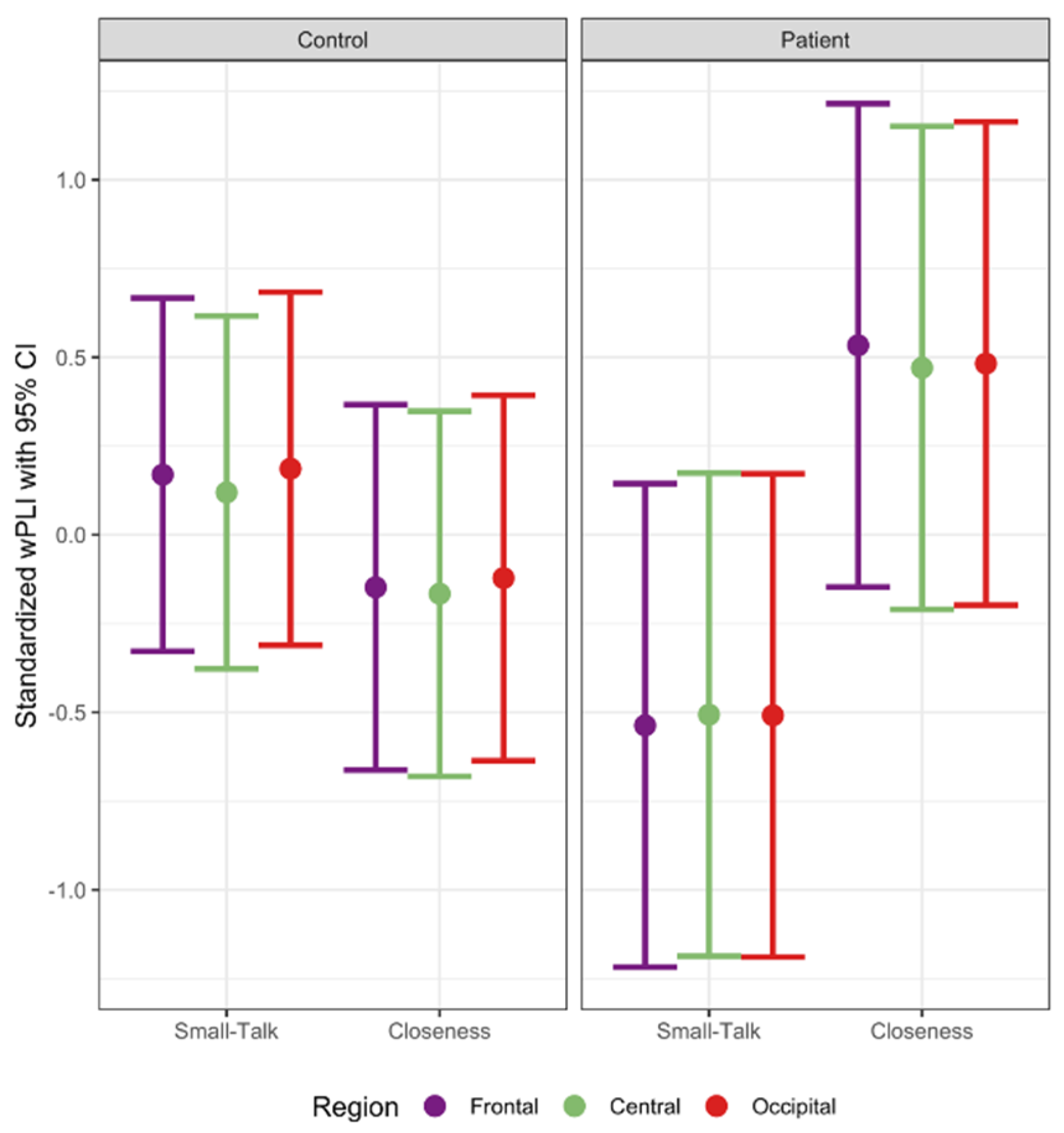
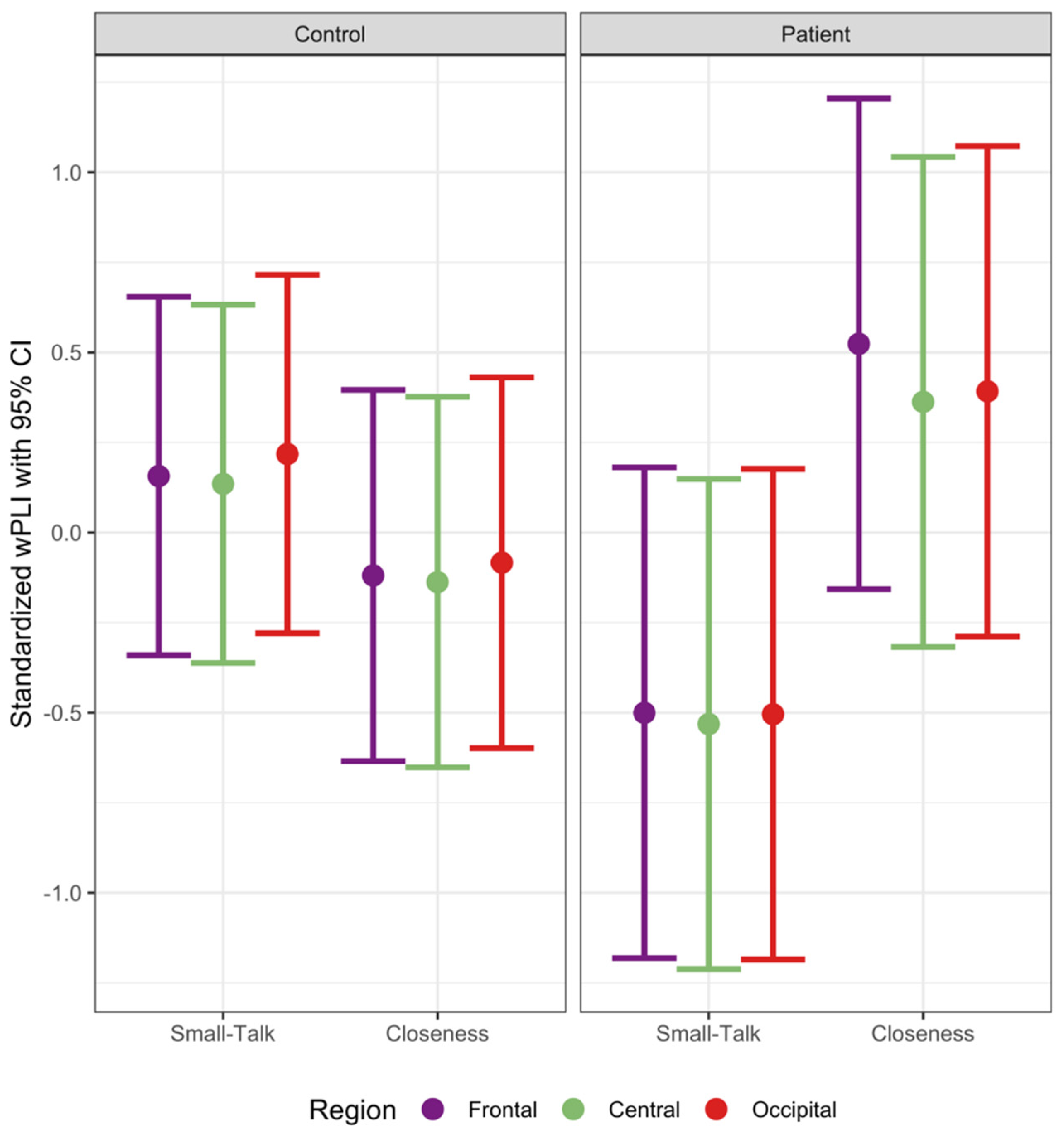
3.2. Functional Connectivity
3.3. Association of Functional Connectivity with Symptom and Post-Interaction Ratings in Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McClelland, D.C. Human Motivation; Cambridge University Press: New York, NY, USA, 1987. [Google Scholar]
- Correll, C.U.; Schooler, N.R. Negative symptoms in schizophrenia: A review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr. Dis. Treat. 2020, 16, 519–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchard, J.J.; Shan, L.; Andrea, A.; Savage, C.; Kring, A.M.; Weittenhiller, L. Negative symptoms and their assessment in schizophrenia and related disorders. In A Clinical Introduction to Psychosis; Elsevier: Amsterdam, The Netherlands, 2020; pp. 153–175. [Google Scholar]
- Kotov, R.; Foti, D.; Li, K.; Bromet, E.J.; Hajcak, G.; Ruggero, C.J. Validating dimensions of psychosis symptomatology: Neural correlates and 20-year outcomes. J. Abnorm. Psychol. 2016, 125, 1103–1119. [Google Scholar] [CrossRef] [PubMed]
- Fulford, D.; Campellone, T.; Gard, D.E. Social motivation in schizophrenia: How research on basic reward processes informs and limits our understanding. Clin. Psychol. Rev. 2018, 63, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Strauss, G.P.; Waltz, J.A.; Gold, J.M. A review of reward processing and motivational impairment in schizophrenia. Schizophr. Bull. 2014, 40, S107–S116. [Google Scholar] [CrossRef] [Green Version]
- Green, M.F.; Horan, W.P.; Lee, J. Social cognition in schizophrenia. Nat. Rev. Neurosci. 2015, 16, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, A.J.; Lieberman, J.A.; Jarskog, L.F. Oxytocin, Dopamine, and the Amygdala: A Neurofunctional Model of Social Cognitive Deficits in Schizophrenia. Schizophr. Bull. 2011, 37, 1077–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCleery, A.; Lee, J.; Joshi, A.; Wynn, J.K.; Hellemann, G.S.; Green, M.F. Meta-analysis of face processing event-related potentials in schizophrenia. Biol. Psychiatry 2015, 77, 116–126. [Google Scholar] [CrossRef]
- Taylor, S.F.; Kang, J.; Brege, I.S.; Tso, I.F.; Hosanagar, A.; Johnson, T.D. Meta-analysis of functional neuroimaging studies of emotion perception and experience in schizophrenia. Biol. Psychiatry 2012, 71, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Delvecchio, G.; Sugranyes, G.; Frangou, S. Evidence of diagnostic specificity in the neural correlates of facial affect processing in bipolar disorder and schizophrenia: A meta-analysis of functional imaging studies. Psychol. Med. 2013, 43, 553–569. [Google Scholar] [CrossRef]
- Fries, P. A Mechanism for cognitive dynamics: Neuronal communication through neuronal coherence. Trends Cogn. Sci. 2005, 9, 474–480. [Google Scholar] [CrossRef]
- Fries, P. Rhythms for cognition: Communication through coherence. Neuron 2015, 88, 220–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varela, F.; Lachaux, J.P.; Rodriguez, E.; Martinerie, J. The brainweb: Phase synchronization and large-scale integration. Nat. Rev. Neurosci. 2001, 2, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Uhlhaas, P.J. Dysconnectivity, large-scale networks and neuronal dynamics in schizophrenia. Curr. Opin. Neurobiol. 2013, 23, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Maran, M.; Grent-‘t-Jong, T.; Uhlhaas, P.J. Electrophysiological insights into connectivity anomalies in schizophrenia: A systematic review. Neuropsychiatr. Electrophysiol. 2016, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Popov, T.G.; Rockstroh, B.S.; Popova, P.; Carolus, A.M.; Miller, G.A. Dynamics of alpha oscillations elucidate facial affect recognition in schizophrenia. Cogn. Affect. Behav. Neurosci. 2014, 14, 364–377. [Google Scholar] [CrossRef] [Green Version]
- Uhlhaas, P.J.; Linden, D.E.J.; Singer, W.; Haenschel, C.; Lindner, M.; Maurer, K.; Rodriguez, E. Dysfunctional long-range coordination of neural activity during gestalt perception in schizophrenia. J. Neurosci. 2006, 26, 8168–8175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Kim, D.W.; Kim, E.Y.; Kim, S.; Im, C.H. Dysfunctional gamma-band activity during face structural processing in schizophrenia patients. Schizophr. Res. 2010, 119, 191–197. [Google Scholar] [CrossRef]
- Grove, T.B.; Lasagna, C.A.; Martínez-Cancino, R.; Pamidighantam, P.; Deldin, P.J.; Tso, I.F. Neural oscillatory abnormalities during gaze processing in schizophrenia: Evidence of reduced theta phase consistency and inter-areal theta-gamma coupling. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 370–379. [Google Scholar] [CrossRef]
- Csukly, G.; Stefanics, G.; Komlósi, S.; Czigler, I.; Czobor, P. Event-related theta synchronization predicts deficit in facial affect recognition in schizophrenia. J. Abnorm. Psychol. 2014, 123, 178–189. [Google Scholar] [CrossRef] [Green Version]
- Adolphs, R.; Damasio, H.; Tranel, D.; Cooper, G.; Damasio, A.R. A role for somatosensory cortices in the visual recognition of emotion as revealed by three-dimensional lesion mapping. J. Neurosci. 2000, 20, 2683–2690. [Google Scholar] [CrossRef] [PubMed]
- Klimesch, W.; Sauseng, P.; Hanslmayr, S. EEG Alpha oscillations: The inhibition-timing hypothesis. Brain Res. Rev. 2007, 53, 63–88. [Google Scholar] [CrossRef]
- Blanchard, J.J.; Park, S.G.; Catalano, L.T.; Bennett, M.E. Social affiliation and negative symptoms in schizophrenia: Examining the role of behavioral skills and subjective responding. Schizophr. Res. 2015, 168, 491–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarthy, J.M.; Bradshaw, K.R.; Catalano, L.T.; Garcia, C.P.; Malik, A.; Bennett, M.E.; Blanchard, J.J. Negative symptoms and the formation of social affiliative bonds in schizophrenia. Schizophr. Res. 2018, 193, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Campellone, T.R.; Truong, B.; Gard, D.; Schlosser, D.A. Social motivation in people with recent-onset schizophrenia spectrum disorders. J. Psychiatr. Res. 2018, 99, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Campellone, T.R.; Kring, A.M. Anticipated pleasure for positive and negative social interaction outcomes in schizophrenia. Psychiatry Res. 2018, 259, 203–209. [Google Scholar] [CrossRef]
- Engel, M.; Fritzsche, A.; Lincoln, T.M. Anticipation and experience of emotions in patients with schizophrenia and negative symptoms. An experimental study in a social context. Schizophr. Res. 2016, 170, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Horan, W.P.; Blanchard, J.J. Emotional responses to psychosocial stress in schizophrenia: The role of individual differences in affective traits and coping. Schizophr. Res. 2003, 60, 271–283. [Google Scholar] [CrossRef]
- Aron, A.; Melinat, E.; Aron, E.N.; Vallone, R.D.; Bator, R.J. The experimental generation of interpersonal closeness: A procedure and some preliminary findings. Personal. Soc. Psychol. Bull. 1997, 23, 363–377. [Google Scholar] [CrossRef]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5—Research Version (SCID-5 for DSM-5, Research Version; SCID-5-RV); American Psychiatric Association: Arlington, VA, USA, 2015; ISBN 9781585625246. [Google Scholar]
- Nelson, H.E.; Willison, J. National Adult Reading Test. (NART); NFER-Nelson: Windsor, UK, 1991. [Google Scholar]
- Andreasen, N.C. The Scale for the Assessment of Negative Symptoms (SANS); The University of Iowa: Iowa City, IA, USA, 1983. [Google Scholar]
- Andreasen, N.C. The Scale for the Assessment of Positive Symptoms (SAPS); The University of Iowa: Iowa City, IA, USA, 1984. [Google Scholar]
- Berry, D.S.; Hansen, J.S. Personality, nonverbal behavior, and interaction quality in female dyads. Personal. Soc. Psychol. Bull. 2000, 26, 278–292. [Google Scholar] [CrossRef]
- Byrne, D.E. The Attraction Paradigm; Academic Press: New York, NY, USA, 1971. [Google Scholar]
- Aron, A.; Aron, E.N.; Smollan, D. Inclusion of other in the self scale and the structure of interpersonal closeness. J. Pers. Soc. Psychol. 1992, 63, 596–612. [Google Scholar] [CrossRef]
- American Electroencephalographic Society. Guideline thirteen: Guidelines for standard electrode position nomenclature. J. Clin. Neurophysiol. 1994, 11, 111–113. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Bigdely-Shamlo, N.; Mullen, T.; Kothe, C.; Su, K.M.; Robbins, K.A. The PREP Pipeline: Standardized Preprocessing for Large-Scale EEG Analysis. Front. Neuroinform. 2015, 9, 16. [Google Scholar] [CrossRef]
- Miyakoshi, M. Makoto’s Preprocessing Pipeline. Available online: https://sccn.ucsd.edu/wiki/Makoto’s_preprocessing_pipeline (accessed on 13 May 2020).
- Kothe, C.A.; Makeig, S. BCILAB: A platform for brain-computer interface development. J. Neural Eng. 2013, 10, 56014–56031. [Google Scholar] [CrossRef] [Green Version]
- Pion-Tonachini, L.; Kreutz-Delgado, K.; Makeig, S. ICLabel: An automated electroencephalographic independent component classifier, dataset, and website. Neuroimage 2019, 198, 181–197. [Google Scholar] [CrossRef] [Green Version]
- Stam, C.J.; Nolte, G.; Daffertshofer, A. Phase lag index: Assessment of functional connectivity from multi channel EEG and MEG with diminished bias from common sources. Hum. Brain Mapp. 2007, 28, 1178–1193. [Google Scholar] [CrossRef] [PubMed]
- Vinck, M.; Oostenveld, R.; Van Wingerden, M.; Battaglia, F.; Pennartz, C.M.A. An improved index of phase-synchronization for electrophysiological data in the presence of volume-conduction, noise and sample-size bias. Neuroimage 2011, 55, 1548–1565. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Cho, H.; Gonzalez, R.; Lavaysse, L.M.; Pence, S.; Fulford, D.; Gard, D.E. Do People with schizophrenia experience more negative emotion and less positive emotion in their daily lives? A meta-analysis of experience sampling studies. Schizophr. Res. 2017, 183, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Hirvonen, J.; Wibral, M.; Palva, J.M.; Singer, W.; Uhlhaas, P.; Palva, S. Whole-brain source-reconstructed MEG-data reveal reduced long-range synchronization in chronic schizophrenia. eNeuro 2017, 4, ENEURO.0338-17.2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grützner, C.; Wibral, M.; Sun, L.; Rivolta, D.; Singer, W.; Maurer, K.; Uhlhaas, P.J. Deficits in high- (>60 Hz) gamma-band oscillations during visual processing in schizophrenia. Front. Neuroeng. 2013, 7, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauseng, P.; Griesmayr, B.; Freunberger, R.; Klimesch, W. Control mechanisms in working memory: A possible function of EEG theta oscillations. Neurosci. Biobehav. Rev. 2010, 34, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Sauseng, P.; Hoppe, J.; Klimesch, W.; Gerloff, C.; Hummel, F.C. Dissociation of sustained attention from central executive functions: Local activity and interregional connectivity in the theta range. Eur. J. Neurosci. 2007, 25, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Symons, A.E.; El-Deredy, W.; Schwartze, M.; Kotz, S.A. The functional role of neural oscillations in non-verbal emotional communication. Front. Hum. Neurosci. 2016, 10, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossi, F.; Premoli, I.; Pizzamiglio, S.; Balaban, S.; Ricciardelli, P.; Rivolta, D. Theta-and gamma-band activity discriminates face, body and object perception. Front. Hum. Neurosci. 2020, 14, 74. [Google Scholar] [CrossRef] [PubMed]
- Sauseng, P.; Klimesch, W.; Gruber, W.; Doppelmayr, M.; Stadler, W.; Schabus, M. The interplay between theta and alpha oscillations in the human electroencephalogram reflects the transfer of information between memory systems. Neurosci. Lett. 2002, 324, 121–124. [Google Scholar] [CrossRef]
- Freunberger, R.; Klimesch, W.; Griesmayr, B.; Sauseng, P.; Gruber, W. Alpha phase coupling reflects object recognition. Neuroimage 2008, 42, 928–935. [Google Scholar] [CrossRef]
- Jensen, O.; Mazaheri, A. Shaping functional architecture by oscillatory alpha activity: Gating by inhibition. Front. Hum. Neurosci. 2010, 4, 186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshua, N.; Rossell, S. Configural face processing in schizophrenia. Schizophr. Res. 2009, 112, 99–103. [Google Scholar] [CrossRef]
- Fakra, E.; Salgado-Pineda, P.; Delaveau, P.; Hariri, A.R.; Blin, O. Neural bases of different cognitive strategies for facial affect processing in schizophrenia. Schizophr. Res. 2008, 100, 191–205. [Google Scholar] [CrossRef]
- Rudman, L.A.; Goodwin, S.A. Gender differences in automatic in-group bias: Why do women like women more than men like men? J. Pers. Soc. Psychol. 2004, 87, 494–509. [Google Scholar] [CrossRef] [Green Version]
- Weittenhiller, L.P.; Mikhail, M.E.; Mote, J.; Campellone, T.R.; Kring, A.M. What gets in the way of social engagement in schizophrenia? World J. Psychiatry 2021, 11, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Gard, D.E.; Sanchez, A.H.; Cooper, K.; Fisher, M.; Garrett, C.; Vinogradov, S. Do people with schizophrenia have difficulty anticipating pleasure, engaging in effortful behavior, or both? J. Abnorm. Psychol. 2014, 123, 771–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Patient n = 16 | Control n = 29 | Test Statistics |
|---|---|---|---|
| Female n (%) | 7 (43.75) | 18 (62.07) | χ2(1, N = 45) = 0.76, p = 0.38, V = 0.13 |
| Age M (SD) | 49.31 (13.33) | 42.17 (13.16) | t(43) = 1.73, p = 0.090, d = 0.55 |
| Race n (%) | p = 0.20 (two-tailed Fisher′s exact test), V = 0.34 | ||
| Black | 5 (31.25) | 2 (6.90) | |
| White | 7 (43.75) | 14 (48.28) | |
| Latinx | 2 (12.50) | 5 (17.24) | |
| Other | 2 (12.50) | 8 (27.59) | |
| Education M (SD) | 13.62 (2.12) | 15.48 (1.99) | t(43) = −2.92, p = 0.0055, d = 0.93 |
| Psychosis symptoms M (SD) | |||
| Reality distortion | 0.96 (0.85) | - | |
| Disorganization | 0.16 (0.32) | - | |
| Inexpressivity | 0.34 (0.61) | - | |
| Apathy/Asociality a | 1.26 (1.39) | - | |
| Measures | Patient | Control | ||
|---|---|---|---|---|
| Closeness n = 8 | Small-Talk n = 8 | Closeness n = 14 | Small-Talk n = 15 | |
| Interaction evaluation | ||||
| Emotional experience | 6.41 (1.01) | 6.44 (1.66) | 7.14 (0.61) | 7.08 (0.60) |
| Engagement | 6.71 (1.20) | 5.79 (2.09) | 6.67 (1.18) | 5.78 (0.95) |
| Quality | 7.08 (0.92) | 6.79 (1.72) | 6.76 (1.12) | 7.16 (0.74) |
| Disclosure | 6.81 (1.16) | 7.06 (1.15) | 6.86 (0.93) | 7.03 (0.83) |
| Partner liking | 6.75 (0.71) | 6.25 (1.16) | 6.93 (0.18) | 6.43 (0.78) |
| Closeness | 4.12 (1.55) | 3.75 (1.91) | 5.21 (0.97) | 4.60 (1.24) |
| Future motivation | 6.75 (0.46) | 6.12 (1.12) | 6.36 (1.34) | 6.73 (0.59) |
| Measures | Theta | Alpha | ||||
|---|---|---|---|---|---|---|
| Frontal | Central | Occipital | Frontal | Central | Occipital | |
| Psychosis symptoms | ||||||
| Reality distortion | 0.15 (0.27) | 0.16 (0.27) | 0.16 (0.27) | −0.11 (0.27) | −0.10 (0.27) | −0.13 (0.27) |
| Disorganization | −0.27 (0.26) | −0.26 (0.26) | −0.27 (0.26) | −0.47 (0.24) † | −0.44 (0.24) † | −0.46 (0.24) † |
| Inexpressivity | 0.20 (0.27) | 0.17 (0.27) | 0.17 (0.27) | 0.48 (0.25) † | 0.38 (0.25) | 0.39 (0.25) |
| Apathy/Asociality | 0.22 (0.27) | 0.21 (0.27) | 0.21 (0.27) | 0.37 (0.26) | 0.29 (0.26) | 0.29 (0.26) |
| Interaction evaluation | ||||||
| Emotional experience | 0.31 (0.26) | 0.30 (0.26) | 0.31 (0.26) | 0.18 (0.27) | 0.17 (0.27) | 0.19 (0.27) |
| Engagement | 0.33 (0.26) | 0.30 (0.26) | 0.30 (0.26) | 0.31 (0.26) | 0.27 (0.26) | 0.29 (0.26) |
| Quality | 0.34 (0.26) | 0.31 (0.26) | 0.33 (0.26) | 0.44 (0.25) | 0.39 (0.25) | 0.42 (0.25) |
| Disclosure | 0.22 (0.27) | 0.20 (0.27) | 0.21 (0.27) | 0.35 (0.26) | 0.29 (0.26) | 0.33 (0.26) |
| Partner liking | 0.54 (0.24) * | 0.50 (0.24) † | 0.53 (0.24) * | 0.47 (0.24) † | 0.43 (0.24) † | 0.45 (0.24) |
| Closeness | 0.44 (0.25) † | 0.42 (0.25) | 0.44 (0.25) † | 0.28 (0.26) | 0.30 (0.26) | 0.31 (0.26) |
| Future motivation | 0.43 (0.25) | 0.39 (0.25) | 0.42 (0.25) | 0.39 (0.25) | 0.35 (0.25) | 0.36 (0.25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.Y.; Schiffman, J.; Hu, D.K.; Lopour, B.A.; Martin, E.A. An Effortful Approach to Social Affiliation in Schizophrenia: Preliminary Evidence of Increased Theta and Alpha Connectivity during a Live Social Interaction. Brain Sci. 2021, 11, 1346. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101346
Li LY, Schiffman J, Hu DK, Lopour BA, Martin EA. An Effortful Approach to Social Affiliation in Schizophrenia: Preliminary Evidence of Increased Theta and Alpha Connectivity during a Live Social Interaction. Brain Sciences. 2021; 11(10):1346. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101346
Chicago/Turabian StyleLi, Lilian Y., Jason Schiffman, Derek K. Hu, Beth A. Lopour, and Elizabeth A. Martin. 2021. "An Effortful Approach to Social Affiliation in Schizophrenia: Preliminary Evidence of Increased Theta and Alpha Connectivity during a Live Social Interaction" Brain Sciences 11, no. 10: 1346. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101346