
Relevance of CSF, Serum and Neuroimaging Markers in CNS and PNS Manifestation in COVID-19: A Systematic Review of Case Report and Case Series

 , , ,
, , ,
Abstract
:1. Introduction
- CNS-related manifestations such as acute cerebrovascular disease (ACvD), including ischemic stroke, dural sinus venous thrombosis and hemorrhages, seizures, meningoencephalitis/encephalitis, acute disseminated encephalopathies (ADEM), acute hemorrhagic necrotizing encephalopathy (AHNE), transverse myelitis and cytotoxic lesion of corpus callosum/mild encephalopathy with reversible splenium lesion CLOCC/MERS [2,3,4,5,6,7,8,9,10,11,12,13].
- Peripheral nervous system (PNS)-related manifestations such as Guillain-Barré syndrome (GBS) and its Var. (including acute inflammatory demyelinating polyneuropathy (AIDP), acute motor-sensory axonal neuropathy (AMSAN), acute motor axonal neuropathy (AMAN), Miller Fisher syndrome (MFS), bifacial diplegia (BFP) and other cranial nerve deficits, including polyneuritis cranialis and myasthenia gravis (MG) [14,15,16,17,18,19,20].
2. Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Quality Assessment
2.5. Data Extraction
2.6. Data Acquisition
2.7. Statistical Analysis Methods
3. Results
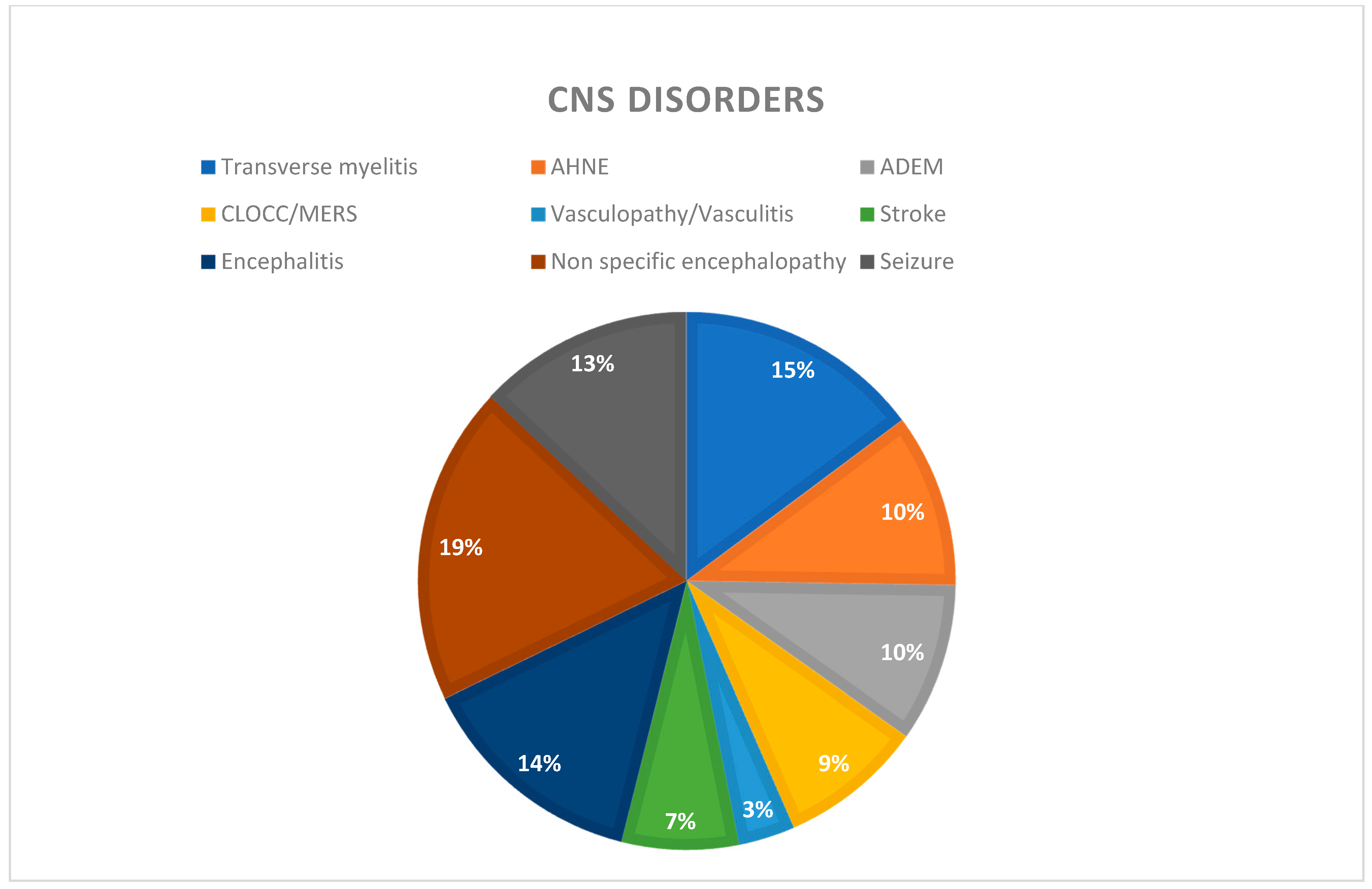
3.1. CNS Manifestations
3.1.1. Demographics
3.1.2. CSF Analysis
3.1.3. Severity
3.1.4. Fatality
3.1.5. Serum Markers
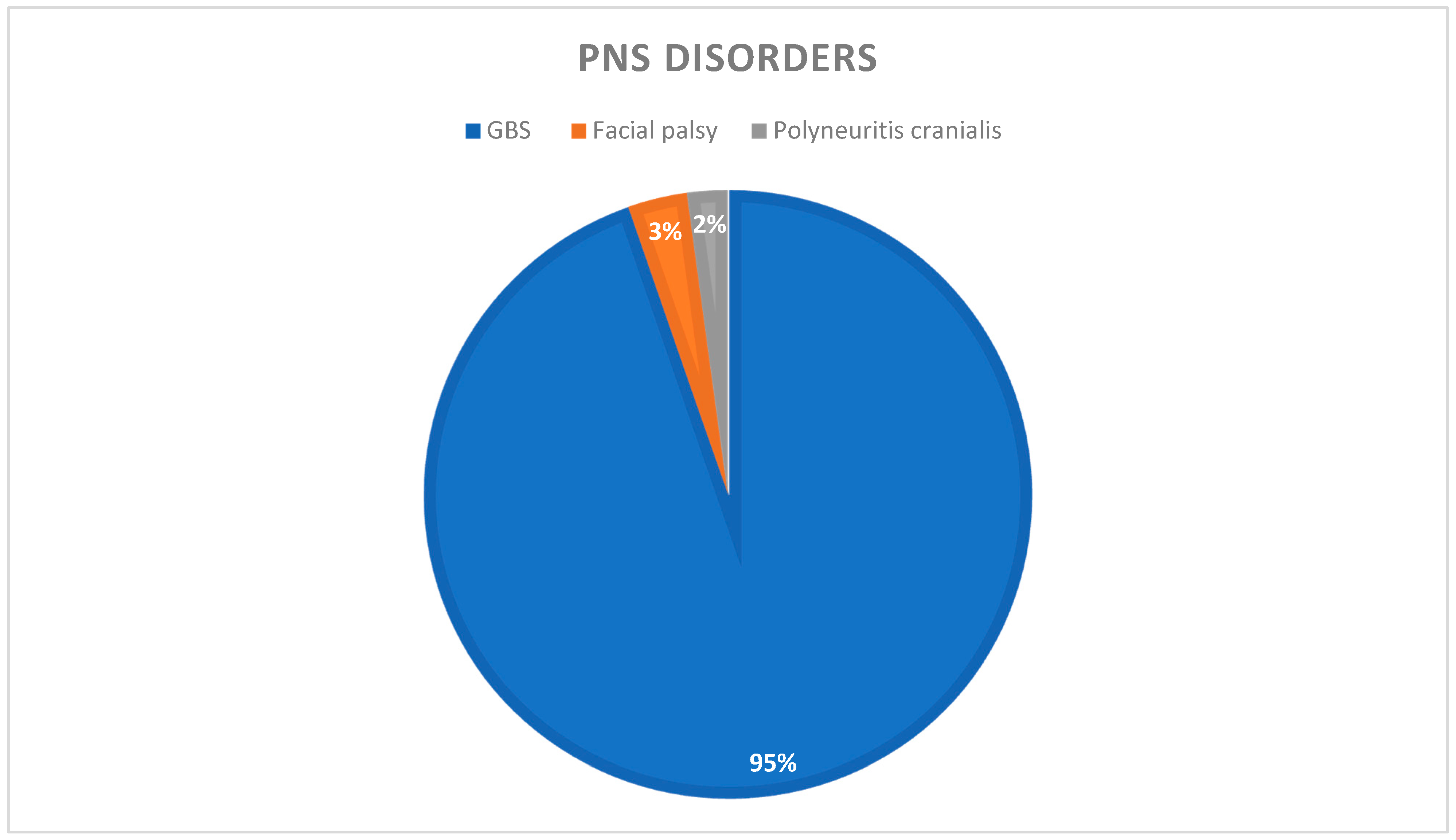
3.2. PNS Manifestations
3.2.1. Demographics
3.2.2. CSF Analysis
3.2.3. Serum Markers
3.2.4. Severity
3.2.5. Fatality
4. Neuroimaging Findings
4.1. CNS Disorders
4.2. PNS Disorders
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- WHO. COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 15 July 2021).
- Al Saiegh, F.; Ghosh, R.; Leibold, A.; Avery, M.B.; Schmidt, R.F.; Theofanis, T.; Mouchtouris, N.; Philipp, L.; Peiper, S.C.; Wang, Z.X.; et al. Status of SARS-CoV-2 in cerebrospinal fluid of patients with COVID-19 and stroke. J. Neurol. Neurosurg. Psychiatry 2020, 91, 846–848. [Google Scholar] [CrossRef]
- Avula, A.; Nalleballe, K.; Narula, N.; Sapozhnikov, S.; Dandu, V.; Toom, S.; Glaser, A.; Elsayegh, D. COVID-19 presenting as stroke. Brain Behav. Immun. 2020, 87, 115–119. [Google Scholar] [CrossRef]
- Li, Y.; Li, M.; Wang, M.; Zhou, Y.; Chang, J.; Xian, Y.; Wang, D.; Mao, L.; Jin, H.; Hu, B. Acute cerebrovascular disease following COVID-19: A single center, retrospective, observational study. Stroke Vasc. Neurol. 2020, 5, 279–284. [Google Scholar] [CrossRef]
- Yaghi, S.; Ishida, K.; Torres, J.; Mac Grory, B.; Raz, E.; Humbert, K.; Henninger, N.; Trivedi, T.; Lillemoe, K.; Alam, S.; et al. SARS-CoV-2 and stroke in a New York healthcare system. Stroke 2020, 51, 2002–2011. [Google Scholar] [CrossRef] [PubMed]
- McCuddy, M.; Kelkar, P.; Zhao, Y.; Wicklund, D. Acute demyelinating encephalomyelitis (ADEM) in COVID-19 infection: A case series. MedRxiv 2020, 68, 1192–1195. [Google Scholar] [CrossRef]
- Parsons, T.; Banks, S.; Bae, C.; Gelber, J.; Alahmadi, H.; Tichauer, M. COVID-19-associated acute disseminated encephalomyelitis (ADEM). J. Neurol. 2020, 267, 2799–2802. [Google Scholar] [CrossRef] [PubMed]
- Assunção, F.B.; Fragoso, D.C.; Donoso Scoppetta, T.L.P.; Martins Maia, A.C. COVID-19-associated acute disseminated encephalomyelitis-like disease. AJNR Am. J Neuroradiol. 2021, 42, E21–E23. [Google Scholar] [CrossRef] [PubMed]
- Poyiadji, N.; Shahin, G.; Noujaim, D.; Stone, M.; Patel, S.; Griffith, B. COVID-19-associated acute hemorrhagic necrotizing encephalopathy: Imaging features. Radiology 2020, 296, E119–E120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morvan, A.C.; Kerambrun, H. Fatal necrotizing encephalitis associated with COVID-19. Neurol. Clin. Pract. 2021, 11, e214–e215. [Google Scholar] [CrossRef] [PubMed]
- Delamarre, L.; Gollion, C.; Grouteau, G.; Rousset, D.; Jimena, G.; Roustan, J.; Gaussiat, F.; Aldigé, E.; Gaffard, C.; Duplantier, J.; et al. COVID-19-associated acute necrotising encephalopathy successfully treated with steroids and polyvalent immunoglobulin with unusual IgG targeting the cerebral fibre network. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1004–1006. [Google Scholar] [CrossRef] [PubMed]
- Moreau, A.; Ego, A.; Vandergheynst, F.; Taccone, F.S.; Sadeghi, N.; Montesinos, I.; Gaspard, N.; Gorham, J. Cytotoxic lesions of the corpus callosum (CLOCCs) associated with SARS-CoV-2 infection. J. Neurol. 2021, 268, 1592–1594. [Google Scholar] [CrossRef]
- Kakadia, B.; Ahmed, J.; Siegal, T.; Jovin, T.G.; Thon, J.M. Mild encephalopathy with reversible splenium lesion (MERS) in a patient with COVID-19. J. Clin. Neurosci. 2020, 79, 272–274. [Google Scholar] [CrossRef]
- Virani, A.; Rabold, E.; Hanson, T.; Haag, A.; Elrufay, R.; Cheema, T.; Balaan, M.; Bhanot, N. Guillain-barré syndrome associated with SARS-CoV-2 infection. IDCases 2020, 20, e00771. [Google Scholar] [CrossRef] [PubMed]
- Toscano, G.; Palmerini, F.; Ravaglia, S.; Ruiz, L.; Invernizzi, P.; Cuzzoni, M.G.; Franciotta, D.; Baldanti, F.; Daturi, R.; Postorino, P.; et al. Guillain-barré syndrome associated with SARS-CoV-2. N. Engl. J. Med. 2020, 382, 2574–2576. [Google Scholar] [CrossRef]
- Sriwastava, S.; Kataria, S.; Tandon, M.; Patel, J.; Patel, R.; Jowkar, A.; Daimee, M.; Bernitsas, E.; Jaiswal, P.; Lisak, R.P. Guillain barré syndrome and its variants as a manifestation of COVID-19: A systematic review of case reports and case series. J. Neurol. Sci. 2021, 420, 117263. [Google Scholar] [CrossRef]
- Gutiérrez-Ortiz, C.; Méndez-Guerrero, A.; Rodrigo-Rey, S.; San Pedro-Murillo, E.; Bermejo-Guerrero, L.; Gordo-Mañas, R.; de Aragón-Gómez, F.; Benito-León, J. Miller Fisher syndrome and polyneuritis cranialis in COVID-19. Neurology 2020, 95, e601–e605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restivo, D.A.; Centonze, D.; Alesina, A.; Marchese-Ragona, R. Myasthenia gravis associated with SARS-CoV-2 infection. Ann. Intern. Med. 2020, 173, 1027–1028. [Google Scholar] [CrossRef] [PubMed]
- Sriwastava, S.; Tandon, M.; Kataria, S.; Daimee, M.; Sultan, S. New onset of ocular myasthenia gravis in a patient with COVID-19: A novel case report and literature review. J. Neurol. 2021, 268, 2690–2696. [Google Scholar] [CrossRef]
- Sedaghat, Z.; Karimi, N. Guillain Barre syndrome associated with COVID-19 infection: A case report. J. Clin. Neurosci. 2020, 76, 233–235. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Aragão, M.D.F.V.V.; Leal, M.C.; Cartaxo Filho, O.Q.; Fonseca, T.M.; Valença, M.M. Anosmia in COVID-19 associated with injury to the olfactory bulbs evident on MRI. AJNR Am. J. Neuroradiol. 2020, 41, 1703–1706. [Google Scholar] [CrossRef]
- Paliwal, V.K.; Garg, R.K.; Gupta, A.; Tejan, N. Neuromuscular presentations in patients with COVID-19. Neurol. Sci. 2020, 41, 3039–3056. [Google Scholar] [CrossRef]
- Beydon, M.; Chevalier, K.; Al Tabaa, O.; Hamroun, S.; Delettre, A.S.; Thomas, M.; Herrou, J.; Riviere, E.; Mariette, X. Myositis as a manifestation of SARS-CoV-2. Ann. Rheum. Dis. 2021, 80, e42. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Charmchi, Z.; Seidman, R.J.; Anziska, Y.; Velayudhan, V.; Perk, J. COVID-19-associated myositis with severe proximal and bulbar weakness. Muscle Nerve 2020, 62, E57–E60. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Caress, J.B.; Castoro, R.J.; Simmons, Z.; Scelsa, S.N.; Lewis, R.A.; Ahlawat, A.; Narayanaswami, P. COVID-19-associated Guillain-Barré syndrome: The early pandemic experience. Muscle Nerve 2020, 62, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C. Guillain-Barré syndrome: The first documented COVID-19-triggered autoimmune neurologic disease: More to come with myositis in the offing. Neurol. -Neuroimmunol. Neuroinflamm. 2020, 7, e781. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American thoracic society and infectious diseases society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Taherifard, E.; Taherifard, E. Neurological complications of COVID-19: A systematic review. Neurol. Res. 2020, 42, 905–912. [Google Scholar] [CrossRef]
- Virhammar, J.; Kumlien, E.; Fällmar, D.; Frithiof, R.; Jackmann, S.; Sköld, M.K.; Kadir, M.; Frick, J.; Lindeberg, J.; Olivero-Reinius, H.; et al. Acute necrotizing encephalopathy with SARS-CoV-2 RNA confirmed in cerebrospinal fluid. Neurology 2020, 95, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Moriguchi, T.; Harii, N.; Goto, J.; Harada, D.; Sugawara, H.; Takamino, J.; Ueno, M.; Sakata, H.; Kondo, K.; Myose, N.; et al. A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int. J. Infect. Dis. 2020, 94, 55–58. [Google Scholar] [CrossRef]
- Fadakar, N.; Ghaemmaghami, S.; Masoompour, S.M.; Shirazi Yeganeh, B.; Akbari, A.; Hooshmandi, S.; Ostovan, V.R. A first case of acute cerebellitis associated with coronavirus disease (COVID-19): A case report and literature review. Cerebellum 2020, 19, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Domingues, R.B.; Mendes-Correa, M.C.; de Moura Leite, F.B.V.; Sabino, E.C.; Salarini, D.Z.; Claro, I.; Santos, D.W.; de Jesus, J.G.; Ferreira, N.E.; Romano, C.M.; et al. First case of SARS-CoV-2 sequencing in cerebrospinal fluid of a patient with suspected demyelinating disease. J. Neurol. 2020, 267, 3154–3156. [Google Scholar] [CrossRef] [PubMed]
- Novi, G.; Mikulska, M.; Briano, F.; Toscanini, F.; Tazza, F.; Uccelli, A.; Inglese, M. COVID-19 in a MS patient treated with ocrelizumab: Does immunosuppression have a protective role? Mult. Scler. Relat. Disord. 2020, 42, 102120. [Google Scholar] [CrossRef] [PubMed]
- Benameur, K.; Agarwal, A.; Auld, S.C.; Butters, M.P.; Webster, A.S.; Ozturk, T.; Howell, J.C.; Bassit, L.C.; Velasquez, A.; Schinazi, R.F.; et al. Encephalopathy and encephalitis associated with cerebrospinal fluid cytokine alterations and coronavirus disease, Atlanta, Georgia, USA, 2020. Emerg. Infect. Dis. 2020, 26, 2016–2021. [Google Scholar] [CrossRef]
- Cavalcanti, D.D.; Raz, E.; Shapiro, M.; Dehkharghani, S.; Yaghi, S.; Lillemoe, K.; Nossek, E.; Torres, J.; Jain, R.; Riina, H.A.; et al. Cerebral venous thrombosis associated with COVID-19. AJNR Am. J. Neuroradiol. 2020, 41, 1370–1376. [Google Scholar] [CrossRef]
- Varadan, B.; Shankar, A.; Rajakumar, A.; Subramanian, S.; Sathya, A.C.; Hakeem, A.R.; Kalyanasundaram, S. Acute hemorrhagic leukoencephalitis in a COVID-19 patient-a case report with literature review. Neuroradiology 2021, 63, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Dixon, L.; Varley, J.; Gontsarova, A.; Mallon, D.; Tona, F.; Muir, D.; Luqmani, A.; Jenkins, I.H.; Nicholas, R.; Jones, B.; et al. COVID-19-related acute necrotizing encephalopathy with brain stem involvement in a patient with aplastic anemia. Neurol. -Neuroimmunol. Neuroinflamm. 2020, 7, e789. [Google Scholar] [CrossRef] [PubMed]
- Gigli, G.L.; Bax, F.; Marini, A.; Pellitteri, G.; Scalise, A.; Surcinelli, A.; Valente, M. Guillain-Barré syndrome in the COVID-19 era: Just an occasional cluster? J. Neurol. 2021, 268, 1195–1197. [Google Scholar] [CrossRef]
- Abolmaali, M.; Heidari, M.; Zeinali, M.; Moghaddam, P.; Ramezani Ghamsari, M.; Jamshidi Makiani, M.; Mirzaasgari, Z. Guillain-Barré syndrome as a parainfectious manifestation of SARS-CoV-2 infection: A case series. J. Clin. Neurosci. 2021, 83, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Krett, J.D.; Jewett, G.A.E.; Elton-Lacasse, C.; Fonseca, K.; Hahn, C.; Au, S.; Koch, M.W. Hemorrhagic encephalopathy associated with COVID-19. J. Neuroimmunol. 2020, 346, 577326. [Google Scholar] [CrossRef] [PubMed]
- Zoghi, A.; Ramezani, M.; Roozbeh, M.; Darazam, I.A.; Sahraian, M.A. A case of possible atypical demyelinating event of the central nervous system following COVID-19. Mult. Scler. Relat. Disord. 2020, 44, 102324. [Google Scholar] [CrossRef] [PubMed]
- Princiotta Cariddi, L.; Tabaee Damavandi, P.; Carimati, F.; Banfi, P.; Clemenzi, A.; Marelli, M.; Giorgianni, A.; Vinacci, G.; Mauri, M.; Versino, M. Reversible encephalopathy syndrome (PRES) in a COVID-19 patient. J. Neurol. 2020, 267, 3157–3160. [Google Scholar] [CrossRef] [PubMed]
- Zachariadis, A.; Tulbu, A.; Strambo, D.; Dumoulin, A.; Di Virgilio, G. Transverse myelitis related to COVID-19 infection. J. Neurol. 2020, 267, 3459–3461. [Google Scholar] [CrossRef] [PubMed]
- Elkady, A.; Rabinstein, A.A. Acute necrotizing encephalopathy and myocarditis in a young patient with COVID-19. Neurol. -Neuroimmunol. Neuroinflamm. 2020, 7. [Google Scholar] [CrossRef]
- Chalil, A.; Baker, C.S.; Johnston, R.B.; Just, C.; Debicki, D.B.; Mayich, M.S.; Bosma, K.J.; Steven, D.A. Acute hemorrhagic encephalitis related to COVID-19. Neurol. Clin. Pract. 2020, 11, e147–e151. [Google Scholar] [CrossRef]
- Pfefferkorn, T.; Dabitz, R.; Von Wernitz-Keibel, T.; Aufenanger, J.; Nowak-Machen, M.; Janssen, H. Acute polyradiculoneuritis with locked-in syndrome in a patient with COVID-19. J. Neurol. 2020, 267, 1883–1884. [Google Scholar] [CrossRef]
- Lascano, A.M.; Epiney, J.; Coen, M.; Serratrice, J.; Bernard-Valnet, R.; Lalive, P.H.; Kuntzer, T.; Hübers, A. SARS-CoV-2 and Guillain–Barré syndrome: AIDP variant with a favourable outcome. Eur. J. Neurol. 2020, 27, 1751–1753. [Google Scholar] [CrossRef] [PubMed]
- Mostel, Z.; Ayat, P.; Capric, V.; Trimmingham, A.; McFarlane, S.I. Guillain-Barré syndrome in a COVID-19 patient: A case report and review of management strategies. Am. J. Med. Case Rep. 2021, 9, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Guilmot, A.; Slootjes, S.M.; Sellimi, A.; Bronchain, M.; Hanseeuw, B.; Belkhir, L.; Yombi, J.C.; De Greef, J.; Pothen, L.; Yildiz, H.; et al. Immune-mediated neurological syndromes in SARS-CoV-2-infected patients. J. Neurol. 2020, 268, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Bigaut, K.; Mallaret, M.; Baloglu, S.; Nemoz, B.; Morand, P.; Baicry, F.; Godon, A.; Voulleminot, P.; Kremer, L.; Chanson, J.-B.; et al. Guillain-Barré syndrome related to SARS-CoV-2 infection. Neurol.-Neuroimmunol. Neuroinflamm. 2020, 7, e785. [Google Scholar] [CrossRef] [PubMed]
- Oguz-Akarsu, E.; Ozpar, R.; Mirzayev, H.; Acet-Ozturk, N.A.; Hakyemez, B.; Ediger, D.; Karli, N.; Pandemic Study Team. Guillain-Barré syndrome in a patient with minimal symptoms of COVID -19 infection. Muscle Nerve 2020, 62. [Google Scholar] [CrossRef]
- Chan, J.L.; Ebadi, H.; Sarna, J.R. Guillain-Barré syndrome with facial diplegia related to SARS-CoV-2 infection. Can. J. Neurol. Sci. 2020, 47, 852–854. [Google Scholar] [CrossRef]
- Dinkin, M.; Gao, V.; Kahan, J.; Bobker, S.; Simonetto, M.; Wechsler, P.; Harpe, J.; Greer, C.; Mints, G.; Salama, G.; et al. COVID-19 presenting with ophthalmoparesis from cranial nerve palsy. Neurology 2020, 95, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Lantos, J.; Strauss, S.; Lin, E. COVID-19-associated Miller Fisher syndrome: MRI findings. Am. J. Neuroradiol. 2020, 41, 1184–1186. [Google Scholar] [CrossRef]
- Hutchins, K.; Jansen, J.; Comer, A.; Scheer, R.; Zahn, G.; Capps, A.; Weaver, L.; Koontz, N. COVID-19-associated bifacial weakness with paresthesia subtype of Guillain-Barré syndrome. Am. J. Neuroradiol. 2020, 41, 1707–1711. [Google Scholar] [CrossRef] [PubMed]
- Sancho-Saldaña, A.; Lambea-Gil, Á.; Liesa, J.L.C.; Caballo, M.R.B.; Garay, M.H.; Celada, D.R.; Serrano-Ponz, M. Guillain-Barré syndrome associated with leptomeningeal enhancement following SARS-CoV-2 infection. Clin. Med. 2020, 20, e93–e94. [Google Scholar] [CrossRef]
- Iadecola, C.; Anrather, J.; Kamel, H. Effects of COVID-19 on the nervous system. Cell 2020, 183, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Marchioni, E.; Ravaglia, S.; Piccolo, G.; Furione, M.; Zardini, E.; Franciotta, D.; Alfonsi, E.; Minoli, L.; Romani, A.; Todeschini, A.; et al. Postinfectious inflammatory disorders: Subgroups based on prospective follow-up. Neurology 2005, 65, 1057–1065. [Google Scholar] [CrossRef]
- Sinha, P.; Matthay, M.A.; Calfee, C.S. Is a “cytokine storm” relevant to COVID-19? JAMA Intern. Med. 2020, 180, 1152–1154. [Google Scholar] [CrossRef]
- Khodamoradi, Z.; Hosseini, S.A.; Saadi, M.H.G.; Mehrabi, Z.; Sasani, M.R.; Yaghoubi, S. COVID-19 meningitis without pulmonary involvement with positive cerebrospinal fluid PCR. Eur. J. Neurol. 2020, 27, 2668–2669. [Google Scholar] [CrossRef] [PubMed]
- Westhoff, T.H.; Seibert, F.S.; Bauer, F.; Stervbo, U.; Anft, M.; Doevelaar, A.A.N.; Rohn, B.J.; Winnekendonk, G.; Dittmer, U.; Schenker, P.; et al. Allograft infiltration and meningoencephalitis by SARS-CoV-2 in a pancreas-kidney transplant recipient. Arab. Archaeol. Epigr. 2020, 20, 3216–3220. [Google Scholar] [CrossRef]
- Mardani, M.; Nadji, S.A.; Sarhangipor, K.A.; Sharifi-Razavi, A.; Baziboroun, M. COVID-19 infection recurrence presenting with meningoencephalitis. New Microbes New Infect. 2020, 37, 100732. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.-K.; Yu, W.-C.; Chu, C.M.; Lau, S.-T.; Sheng, B.; Yuen, K.-Y. Possible central nervous system infection by SARS coronavirus. Emerg. Infect. Dis. 2004, 10, 342–344. [Google Scholar] [CrossRef] [PubMed]
- Hung, E.C.; Chim, S.; Chan, P.; Tong, Y.K.; Ng, E.K.-O.; Chiu, R.W.; Leung, C.-B.; Sung, J.J.Y.; Tam, J.S.; Lo, Y.D. Detection of SARS coronavirus RNA in the cerebrospinal fluid of a patient with severe acute respiratory syndrome. Clin. Chem. 2003, 49, 2108–2109. [Google Scholar] [CrossRef] [Green Version]
- Cebrián, J.; Gonzalez-Martinez, A.; García-Blanco, M.J.; Celdrán-Vivancos, D.; Palacios, E.L.; Reig-Roselló, G.; Casado-Fernández, L.; Vivancos, J.; Gago-Veiga, A.B. Headache and impaired consciousness level associated with SARS-CoV-2 in CSF. Neurology 2020, 95, 266–268. [Google Scholar] [CrossRef] [PubMed]
- Panciani, P.P.; Saraceno, G.; Zanin, L.; Renisi, G.; Signorini, L.; Battaglia, L.; Fontanella, M. SARS-CoV-2: “Three-steps” infection model and CSF diagnostic implication. Brain Behav. Immun. 2020, 87, 128–129. [Google Scholar] [CrossRef] [PubMed]
- Needham, E.J.; Chou, S.H.-Y.; Coles, A.J.; Menon, D.K. Neurological implications of COVID-19 infections. Neurocritical Care 2020, 32, 667–671. [Google Scholar] [CrossRef]
- Bodro, M.; Compta, Y.; Llansó, L.; Esteller, D.; Doncel-Moriano, A.; Mesa, A.; Rodríguez, A.; Sarto, J.; Martínez-Hernandez, E.; Vlagea, A.; et al. Increased CSF levels of IL-1β, IL-6, and ACE in SARS-CoV-2-associated encephalitis. Neurol.-Neuroimmunol. Neuroinflamm. 2020, 7, e821. [Google Scholar] [CrossRef]
- Cheng, Q.; Yang, Y.; Gao, J. Infectivity of human coronavirus in the brain. EBioMedicine 2020, 56, 102799. [Google Scholar] [CrossRef]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 virus targeting the CNS: Tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bevan, C.J.; Cree, B. Fulminant demyelinating diseases of the central nervous system. Semin. Neurol. 2015, 35, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.G.; Kim, J.H.; Lee, M.; Lee, J. Clinical outcome of acute necrotizing encephalopathy in related to involving the brain stem of single institution in Korea. Korean J. Pediatr. 2014, 57, 264–270. [Google Scholar] [CrossRef] [Green Version]
- El-Zein, R.S.; Cardinali, S.; Murphy, C.; Keeling, T. COVID-19-associated meningoencephalitis treated with intravenous immunoglobulin. BMJ Case Rep. 2020, 13, e237364. [Google Scholar] [CrossRef] [PubMed]
- Naz, S.; Hanif, M.; Haider, M.A.; Ali, M.J.; Ahmed, M.U.; Saleem, S. Meningitis as an initial presentation of COVID-19: A case report. Front. Public Health 2020, 8, 474. [Google Scholar] [CrossRef]
- Hafizi, F.; Kherani, S.; Shams, M. Meningoencephalitis from SARS-CoV-2 infection. IDCases 2020, 21, e00919. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Subedi, R.; Tandon, M.; Wen, S.; Patel, J.; Kataria, S.; Peterson, S.; Gwinn, R.; Elkhooly, M.; Prasad, A.; et al. Relevance and clinical significance of magnetic resonance imaging of neurological manifestations in COVID-19: A systematic review of case reports and case series. Brain Sci. 2020, 10, 1017. [Google Scholar] [CrossRef]
- Chow, C.C.N.; Magnussen, J.; Ip, J.; Su, Y. Acute transverse myelitis in COVID-19 infection. BMJ Case Rep. 2020, 13, e236720. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, U.; Chandra, A.; Ray, A.K.; Biswas, P. COVID-19-associated acute transverse myelitis: A rare entity. BMJ Case Rep. 2020, 13, e238668. [Google Scholar] [CrossRef] [PubMed]
- Valiuddin, H.; Skwirsk, B.; Paz-Arabo, P. Acute transverse myelitis associated with SARS-CoV-2: A case-report. Brain Behav. Immun.-Health 2020, 5, 100091. [Google Scholar] [CrossRef]
- Sotoca, J.; Rodríguez-Álvarez, Y. COVID-19-associated acute necrotizing myelitis. Neurol.-Neuroimmunol. Neuroinflammation 2020, 7, e803. [Google Scholar] [CrossRef]
- Nemţan, V.; Manole, E.; Hacina, E.; Topciu, G.; Lisnic, V.; Thurnher, M.; Kummer, R.V. Acute transverse myelitis in a HIV-positive patient with COVID-19. Mold. Med. J. 2020, 63, 51–53. [Google Scholar] [CrossRef]
- Moreno-Escobar, M.C.; Kataria, S.; Khan, E.; Subedi, R.; Tandon, M.; Peshwe, K.; Kramer, J.; Niaze, F.; Sriwastava, S. Acute transverse myelitis with Dysautonomia following SARS-CoV-2 infection: A case report and review of literature. J. Neuroimmunol. 2021, 353, 577523. [Google Scholar] [CrossRef] [PubMed]
- Sarma, D.; Bilello, L.A. A case report of acute transverse myelitis following novel coronavirus infection. Clin. Pract. Cases Emerg. Med. 2020, 4, 321–323. [Google Scholar] [CrossRef]
- Transverse Myelitis Consortium Working Group. Proposed diagnostic criteria and nosology of acute transverse myelitis. Neurology 2002, 59, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Simani, L. Central nervous system manifestations of COVID-19: A systematic review. J. Neurol. Sci. 2020, 413, 116832. [Google Scholar] [CrossRef]
- Munhoz, R.P.; Pedroso, J.L.; Nascimento, F.A.; De Almeida, S.M.; Barsottini, O.G.P.; Cardoso, F.E.C.; Teive, H.A.G. Neurological complications in patients with SARS-CoV-2 infection: A systematic review. Arq. Neuro-Psiquiatr. 2020, 78, 290–300. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683. [Google Scholar] [CrossRef] [Green Version]
- Klok, F.; Kruip, M.; van der Meer, N.; Arbous, M.; Gommers, D.; Kant, K.; Kaptein, F.; van Paassen, J.; Stals, M.; Huisman, M.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Guillan, M.; Villacieros-Alvarez, J.; Bellido, S.; Peremarch, C.P.-J.; Suarez-Vega, V.M.; Aragones-Garcia, M.; Cabrera-Rojo, C.; Fernandez-Ferro, J. Unusual simultaneous cerebral infarcts in multiple arterial territories in a COVID-19 patient. Thromb. Res. 2020, 193, 107–109. [Google Scholar] [CrossRef]
- Rasmussen, C.; Niculescu, I.; Patel, S.; Krishnan, A. COVID-19 and involvement of the corpus callosum: Potential effect of the cytokine storm? Am. J. Neuroradiol. 2020. [Google Scholar] [CrossRef]
- Elkhaled, W.; Ben Abid, F.; Akhtar, N.; AbuKamar, M.R.; Ibrahim, W.H. A 23-year-old man with SARS-CoV-2 infection who presented with auditory hallucinations and imaging findings of cytotoxic lesions of the corpus callosum (CLOCC). Am. J. Case Rep. 2020, 21, e928798-1–e928798-6. [Google Scholar] [CrossRef]
- Agarwal, N.; Martini, R.; Pedrotti, G.; Della Sala, S.W. Unusual lesion in the splenium of the corpus callosum and coronavirus infectious disease-19. BJR Case Rep. 2020, 6, 20200068. [Google Scholar] [CrossRef]
- Lin, J.; Lawson, E.; Verma, S.; Peterson, R.; Sidhu, R. Cytotoxic lesion of the corpus callosum in an adolescent with multisystem inflammatory syndrome and SARS-CoV-2 infection. Am. J. Neuroradiol. 2020, 41, 2017–2019. [Google Scholar] [CrossRef]
- Vaschetto, R.; Cena, T.; Sainaghi, P.P.; Meneghetti, G.; Bazzano, S.; Vecchio, D.; Pirisi, M.; Brustia, D.; Barini, M.; Cammarota, G.; et al. Cerebral nervous system vasculitis in a COVID-19 patient with pneumonia. J. Clin. Neurosci. 2020, 79, 71–73. [Google Scholar] [CrossRef]
- Matos, A.R.; Quintas-Neves, M.; Oliveira, A.I.A.; Dias, L.; Marques, S.; Carvalho, R.; Alves, J.N. COVID-19 associated central nervous system vasculopathy. Can. J. Neurol. Sci. 2020, 48, 139–140. [Google Scholar] [CrossRef]
- Terraneo, L.; Samaja, M. Comparative response of brain to chronic hypoxia and hyperoxia. Int. J. Mol. Sci. 2017, 18, 1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Lazartigues, E. Expression of ACE2 in human neurons supports the neuro-invasive potential of COVID-19 virus. Cell. Mol. Neurobiol. 2020, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Shen, D.; Zhou, H.; Liu, J.; Chen, S. Guillain-Barré syndrome associated with SARS-CoV-2 infection: Causality or coincidence? Lancet Neurol. 2020, 19, 383–384. [Google Scholar] [CrossRef]
- Mozhdehipanah, H.; Paybast, S.; Gorji, R. Guillain-Barré syndrome as a neurological complication of COVID-19 infection: A case series and review of the literature. Int. Clin. Neurosci. J. 2020, 7, 156–161. [Google Scholar] [CrossRef]
- Ebrahimzadeh, S.A.; Ghoreishi, A.; Rahimian, N. Guillain-Barré syndrome associated with COVID-19. Neurol. Clin. Pract. 2020, 11, e196–e198. [Google Scholar] [CrossRef] [PubMed]
- Assini, A.; Benedetti, L.; Di Maio, S.; Schirinzi, E.; Del Sette, M. New clinical manifestation of COVID-19 related Guillain-Barrè syndrome highly responsive to intravenous immunoglobulins: Two Italian cases. Neurol. Sci. 2020, 41, 1657–1658. [Google Scholar] [CrossRef]
- Reyes-Bueno, J.A.; García-Trujillo, L.; Urbaneja, P.; Ciano-Petersen, N.L.; Postigo-Pozo, M.J.; Martínez-Tomás, C.; Serrano-Castro, P.J. Miller-Fisher syndrome after SARS-CoV-2 infection. Eur. J. Neurol. 2020, 27, 1759–1761. [Google Scholar] [CrossRef] [PubMed]
- Manganotti, P.; Bellavita, G.; D’Acunto, L.; Tommasini, V.; Fabris, M.; Sartori, A.; Bonzi, L.; Stella, A.B.; Pesavento, V. Clinical neurophysiology and cerebrospinal liquor analysis to detect Guillain-Barré syndrome and polyneuritis cranialis in COVID-19 patients: A case series. J. Med. Virol. 2020, 93, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Garnero, M.; Del Sette, M.; Assini, A.; Beronio, A.; Capello, E.; Cabona, C.; Reni, L.; Serrati, C.; Bandini, F.; Granata, A.; et al. COVID-19-related and not related Guillain-Barré syndromes share the same management pitfalls during lock down: The experience of Liguria region in Italy. J. Neurol. Sci. 2020, 418, 117114. [Google Scholar] [CrossRef] [PubMed]
- Senel, M.; Abu-Rumeileh, S.; Michel, D.; Garibashvili, T.; Althaus, K.; Kassubek, J.; Otto, M. Miller-Fisher syndrome after COVID-19: Neurochemical markers as an early sign of nervous system involvement. Eur. J. Neurol. 2020, 27, 2378–2380. [Google Scholar] [CrossRef]
- Caamaño, D.S.J.; Beato, R.A. Facial diplegia, a possible atypical variant of Guillain-Barré syndrome as a rare neurological complication of SARS-CoV-2. J. Clin. Neurosci. 2020, 77, 230–232. [Google Scholar] [CrossRef]
- Chan, M.; Han, S.C.; Kelly, S.; Tamimi, M.; Giglio, B.; Lewis, A. A case series of Guillain-Barré syndrome after COVID-19 infection in New York. Neurol. Clin. Pract. 2020, 11, e576–e578. [Google Scholar] [CrossRef]
- Diez-Porras, L.; Vergés, E.; Gil-López, F.J.; Vidal, M.J.; Massons, J.; Arboix, A. Guillain-Barré-Strohl syndrome and COVID-19: Case report and literature review. Neuromuscul. Disord. 2020, 30, 859–861. [Google Scholar] [CrossRef]
- Khaja, M.; Gomez, G.P.R.; Santana, Y.; Hernandez, N.; Haider, A.; Lara, J.L.P.; Elkin, R. A 44-year-old hispanic man with loss of taste and bilateral facial weakness diagnosed with Guillain-Barré syndrome and Bell’s palsy associated with SARS-CoV-2 infection treated with intravenous immunoglobulin. Am. J. Case Rep. 2020, 21, e927956. [Google Scholar] [CrossRef] [PubMed]
- Nanda, S.; Handa, R.; Prasad, A.; Anand, R.; Zutshi, D.; Dass, S.K.; Bedi, P.K.; Pahuja, A.; Shah, P.K.; Sharma, B. Covid-19 associated Guillain-Barre syndrome: Contrasting tale of four patients from a tertiary care centre in India. Am. J. Emerg. Med. 2020, 39, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Galán, A.V.; Saucedo, P.D.S.; Postigo, F.P.; Paniagua, E.B. Síndrome de Guillain-Barré asociado a infección por SARS-CoV-2. Neurology 2020, 35, 268–269. [Google Scholar] [CrossRef]
- Aasfara, J.; Hajjij, A.; Bensouda, H.; Ouhabi, H.; Benariba, F. A unique association of bifacial weakness, paresthesia and vestibulocochlear neuritis as post COVID 19 manifestation in pregnant women. Pan Afr. Med. J. 2021, 38, 30. [Google Scholar] [CrossRef] [PubMed]
- Homma, Y.; Watanabe, M.; Inoue, K.; Moritaka, T. Coronavirus disease-19 pneumonia with facial nerve palsy and olfactory disturbance. Intern. Med. 2020, 59, 1773–1775. [Google Scholar] [CrossRef]
- Willison, H.J.; Jacobs, B.C.; van Doorn, P.A. Guillain-Barré syndrome. Lancet 2016, 388, 717–727. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | N (%) |
|---|---|
| Age | |
| >50 | 75 (70.8) |
| ≤50 | 31 (29.2) |
| * Sex | |
| Male | 64 (65.3) |
| Female | 34 (34.7) |
| ● CNS manifestation | |
| Transverse myelitis | 17 (14.7) |
| AHNE | 12 (10.4) |
| ADEM | 11 (9.5) |
| CLOCC/MERS | 10 (8.6) |
| Vasculopathy/ Vasculitis | 4 (3.4) |
| Stroke | 8 (7) |
| Encephalitis | 16 (13.8) |
| Non-specific Encephalopathy | 22 (19.1) |
| Seizure | 15 (12.9) |
| ** COVID-19 Severity | |
| Non-severe | 34 (36.6) |
| Severe | 59 (63.4) |
| ♦ Outcome | |
| Non-fatal | 82 (82) |
| Fatal | 18 (18) |
| Stroke | Encephalitis | Non-Specific Encephalopathy | Seizures | Vasculopathy/Vasculitis | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| * Variables | 0 | 1 | Total | Fisher Test | 0 | 1 | Total | Fisher Test | 0 | 1 | Total | Fisher Test | 0 | 1 | Total | Fisher Test | 0 | 1 | Total | Fisher Test |
| n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | |
| CSF protein | ||||||||||||||||||||
| >45 | 54(57) | 5(62) | 59(57.3) | 1 | 50(56) | 10(71) | 60(57.7) | 0.385 | 52(63) | 7(33) | 59(57.3) | 0.024 | 53(60) | 7(47) | 60(57.7) | 0.404 | 58(57) | 2(67) | 60(57.7) | 1 |
| ≤45 | 41(43) | 3(38) | 44(42.7) | 40(44) | 4(29) | 44(42.3) | 30(37) | 14(67) | 44(42.7) | 36(40) | 8(53) | 44(42.3) | 43(43) | 1(33) | 44(42.3) | |||||
| CSF cell count | ||||||||||||||||||||
| >5 | 25(28) | 2(25) | 27(27.8) | 1 | 25(30) | 2(14) | 27(27.6) | 0.338 | 23(29) | 3(17) | 26(26.8) | 0.383 | 24(28) | 3(25) | 27(27.6) | 1 | 26(28) | 1(25) | 27(27.6) | 1 |
| ≤5 | 64(72) | 6(75) | 70(72.2) | 59(70) | 12(86) | 71(72.4) | 56(71) | 15(83) | 71(73.2) | 62(72) | 9(75) | 71(72.4) | 68(72) | 3(75) | 71(72.4) | |||||
| CSF Lymphocyte Percent | ||||||||||||||||||||
| >50 | 28(61) | 1(33) | 29(59.2) | 0.559 | 26(68) | 3(27) | 29(59.2) | 0.033 | 26(59) | 2(50) | 28(58.3) | 1 | 27(60) | 2(50) | 29(59.2) | 1 | 28(60) | 1(50) | 29(59.2) | 1 |
| ≤50 | 18(39) | 2(67) | 20(40.8) | 12(32) | 8(73) | 20(40.8) | 18(41) | 2(50) | 20(41.7) | 18(40) | 2(50) | 20(40.8) | 19(40) | 1(50) | 20(40.8) | |||||
| Severity | ||||||||||||||||||||
| Non-Severe | 32(37) | 2(33) | 34(37) | 1 | 32(40) | 2(17) | 34(36.6) | 0.199 | 28(37) | 6(33) | 34(36.6) | 1 | 32(38) | 2(22) | 34(36.6) | 0.478 | 33(37) | 1(33) | 34(36.6) | 1 |
| Severe | 54(63) | 4(67) | 58(63) | 49(60) | 10(83) | 59(63.4) | 47(63) | 12(67) | 59(63.4) | 52(62) | 7(78) | 59(63.4) | 57(63) | 2(67) | 59(63.4) | |||||
| Fatality | ||||||||||||||||||||
| Non-Fatal | 77(82) | 4(80) | 81(81.8) | 1 | 73(83) | 9(75) | 82(82) | 0.448 | 65(82) | 17(85) | 82(82.8) | 1 | 68(80) | 14(93) | 82(82) | 0.295 | 80(82) | 2(67) | 82(82) | 0.452 |
| Fatal | 17(18) | 1(20) | 18(18.2) | 15(17) | 3(25) | 18(18) | 14(18) | 3(15) | 17(17.2) | 17(20) | 1(7) | 18(18) | 17(18) | 1(33) | 18(18) | |||||
| Age | ||||||||||||||||||||
| ≥50 | 69(70) | 5(71) | 74(70.5) | 1 | 68(72) | 7(58) | 75(70.8) | 0.327 | 57(69) | 18(82) | 75(71.4) | 0.293 | 63(69) | 12(80) | 75(70.8) | 0.545 | 74(73) | 1(25) | 75(70.8) | 0.074 |
| <50 | 29(30) | 2(29) | 31(29.5) | 26(28) | 5(42) | 31(29.2) | 26(31) | 4(18) | 30(28.6) | 28(31) | 3(20) | 31(29.2) | 28(27) | 3(75) | 31(29.2) | |||||
| Sex | ||||||||||||||||||||
| Male | 62(66) | 2(50) | 64(65.3) | 0.608 | 53(63) | 11(79) | 64(65.3) | 0.367 | 54(69) | 10(53) | 64(66) | 0.187 | 55(65) | 9(69) | 64(65.3) | 1 | 62(66) | 2(50) | 64(65.3) | 0.608 |
| Female | 32(34) | 2(50) | 34(34.7) | 31(37) | 3(21) | 34(34.7) | 24(31) | 9(47) | 33(34) | 30(35) | 4(31) | 34(34.7) | 32(34) | 2(50) | 34(34.7) | |||||
| Transverse Myelitis | AHNE | ADEM | CLOCC/MERS | ** Others | ||||||||||||||||
| CSF_ Protein | ||||||||||||||||||||
| >45 | 48(55) | 12(75) | 60(57.7) | 0.172 | 51(54) | 9(100) | 60(58.3) | 0.01 | 53(56) | 7(70) | 60(57.7) | 0.512 | 57(60) | 3(33) | 60(57.7) | 0.163 | 46(58) | 13(57) | 59(57.8) | 1 |
| ≤45 | 40(45) | 4(25) | 44(42.3) | 43(46) | 0(0) | 43(41.7) | 41(44) | 3(30) | 44(42.3) | 38(40) | 6(67) | 44(42.3) | 33(42) | 10(43) | 43(42.2) | |||||
| CSF_ Cell Count | ||||||||||||||||||||
| >5 | 18(21) | 9(69) | 27(27.6) | 0.001 | 23(26) | 3(33) | 26(26.8) | 0.698 | 23(26) | 4(40) | 27(27.6) | 0.456 | 27(30) | 0(0) | 27(27.6) | 0.185 | 24(32) | 3(14) | 27(28.1) | 0.108 |
| ≤5 | 67(79) | 4(31) | 71(72.4) | 65(74) | 6(67) | 71(73.2) | 65(74) | 6(60) | 71(72.4) | 64(70) | 7(100) | 71(72.4) | 50(68) | 19(86) | 69(71.9) | |||||
| CSF_lymphocyte Percent | ||||||||||||||||||||
| >50 | 19(51) | 10(83) | 29(59.2) | 0.089 | 25(58) | 4(67) | 29(59.2) | 1 | 25(60) | 4(57) | 29(59.2) | 1 | 29(62) | 0(0) | 29(59.2) | 0.162 | 22(55) | 7(78) | 29(59.2) | 0.277 |
| ≤50 | 18(49) | 2(17) | 20(40.8) | 18(42) | 2(33) | 20(40.8) | 17(40) | 3(43) | 20(40.8) | 18(38) | 2(100) | 20(40.8) | 18(45) | 2(22) | 20(40.8) | |||||
| ♦ Severity | ||||||||||||||||||||
| Non-Severe | 21(28) | 13(76) | 34(36.6) | 0 | 33(40) | 0(0) | 33(35.9) | 0.012 | 30(37) | 4(36) | 34(36.6) | 1 | 31(37) | 3(33) | 34(36.6) | 1 | 27(38) | 7(37) | 34(37.4) | 1 |
| Severe | 55(72) | 4(24) | 59(63.4) | 49(60) | 10(100) | 59(64.1) | 52(63) | 7(64) | 59(63.4) | 53(63) | 6(67) | 59(63.4) | 45(62) | 12(63) | 57(62.6) | |||||
| Fatality | ||||||||||||||||||||
| Non-Fatal | 68(82) | 14(82) | 82(82) | 1 | 76(86) | 5(45) | 81(81.8) | 0.004 | 73(81) | 9(90) | 82(82) | 0.685 | 74(82) | 8(80) | 82(82) | 1 | 65(84) | 17(81) | 82(83.7) | 0.742 |
| Fatal | 15(18) | 3(18) | 18(18) | 12(14) | 6(55) | 18(18.2) | 17(19) | 1(10) | 18(18) | 16(18) | 2(20) | 18(18) | 12(16) | 4(19) | 16(16.3) | |||||
| Age | ||||||||||||||||||||
| ≥50 | 66(74) | 9(53) | 75(70.8) | 0.089 | 65(70) | 9(75) | 74(70.5) | 1 | 69(73) | 6(55) | 75(70.8) | 0.292 | 68(71) | 7(70) | 75(70.8) | 1 | 58(68) | 16(80) | 74(70.5) | 0.416 |
| <50 | 23(26) | 8(47) | 31(29.2) | 28(30) | 3(25) | 31(29.5) | 26(27) | 5(45) | 31(29.2) | 28(29) | 3(30) | 31(29.2) | 27(32) | 4(20) | 31(29.5) | |||||
| Sex | ||||||||||||||||||||
| Male | 55(68) | 9(53) | 64(65.3) | 0.27 | 56(66) | 7(58) | 63(64.9) | 0.748 | 57(66) | 7(64) | 64(65.3) | 1 | 55(62) | 9(90) | 64(65.3) | 0.158 | 53(65) | 9(60) | 62(64.6) | 0.771 |
| Female | 26(32) | 8(47) | 34(34.7) | 29(34) | 5(42) | 34(35.1) | 30(34) | 4(36) | 34(34.7) | 33(38) | 1(10) | 34(34.7) | 28(35) | 6(40) | 34(35.4) | |||||
| Age | ||||
|---|---|---|---|---|
| Variables | 50+ | <50 | Total | Fisher Test |
| n (%) | n (%) | n (%) | p-Value | |
| Stroke | ||||
| 0 | 69(93) | 29(94) | 98(93.3) | 1 |
| 1 | 5(7) | 2(6) | 7(6.7) | |
| Encephalitis | ||||
| 0 | 68(91) | 26(84) | 94(88.7) | 0.327 |
| 1 | 7(9) | 5(16) | 12(11.3) | |
| Encephalopathy | ||||
| 0 | 57(76) | 26(87) | 83(79) | 0.293 |
| 1 | 18(24) | 4(13) | 22(21) | |
| Seizures | ||||
| 0 | 63(84) | 28(90) | 91(85.8) | 0.545 |
| 1 | 12(16) | 3(10) | 15(14.2) | |
| CNS demyelination | ||||
| 0 | 74(99) | 28(90) | 102(96.2) | 0.074 |
| 1 | 1(1) | 3(10) | 4(3.8) | |
| Transverse Myelitis | ||||
| 0 | 66(88) | 23(74) | 89(84) | 0.089 |
| 1 | 9(12) | 8(26) | 17(16) | |
| AHNE | ||||
| 0 | 65(88) | 28(90) | 93(88.6) | 1 |
| 1 | 9(12) | 3(10) | 12(11.4) | |
| ADEM | ||||
| 0 | 69(92) | 26(84) | 95(89.6) | 0.292 |
| 1 | 6(8) | 5(16) | 11(10.4) | |
| CLOCC/MERS | ||||
| 0 | 68(91) | 28(90) | 96(90.6) | 1 |
| 1 | 7(9) | 3(10) | 10(9.4) | |
| CSF Protein | Elevated Cell Count | Lymphocytes | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High | Low | Yes | No | |||||||||
| * Variables | >45 | ≤45 | Total | Fisher Test | >5 | ≤5 | Total | Fisher Test | >50% | ≤50% | Total | Fisher Test |
| n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | |
| Age | ||||||||||||
| 50+ | 41(75) | 29(74) | 70(74.5) | 1.000 | 13(54) | 51(80) | 64(72.7) | 0.030 | 11(48) | 12(63) | 23(54.8) | 0.366 |
| <50 | 14(25) | 10(26) | 24(25.5) | 11(46) | 13(20) | 24(27.3) | 12(52) | 7(37) | 19(45.2) | |||
| Sex | ||||||||||||
| Male | 35(67) | 20(59) | 55(64) | 0.494 | 14(58) | 37(66) | 51(63.8) | 0.613 | 11(50) | 13(65) | 24(57.1) | 0.366 |
| Female | 17(33) | 14(41) | 31(36) | 10(42) | 19(34) | 29(36.2) | 11(50) | 7(35) | 18(42.9) | |||
| ♦ Severity | ||||||||||||
| Non-severe | 17(33) | 13(41) | 30(36.1) | 0.639 | 15(68) | 15(27) | 30(39) | 0.002 | 15(68) | 4(22) | 19(47.5) | 0.005 |
| Severe | 34(67) | 19(59) | 53(63.9) | 7(32) | 40(73) | 47(61) | 7(32) | 14(78) | 21(52.5) | |||
| Fatality | ||||||||||||
| Non-fatal | 41(76) | 33(87) | 74(80.4) | 0.286 | 18(72) | 52(85) | 70(81.4) | 0.221 | 16(73) | 17(85) | 33(78.6) | 0.460 |
| Fatal | 13(24) | 5(13) | 18(19.6) | 7(28) | 9(15) | 16(18.6) | 6(27) | 3(15) | 9(21.4) | |||
| Stroke | ||||||||||||
| 0 | 54(92) | 41(93) | 95(92.2) | 1.000 | 25(93) | 64(91) | 89(91.8) | 1 | 28(97) | 18(90) | 46(93.9) | 0.559 |
| 1 | 5(8) | 3(7) | 8(7.8) | 2(7) | 6(9) | 8(8.2) | 1(3) | 2(10) | 3(6.1) | |||
| Encephalitis | ||||||||||||
| 0 | 50(83) | 40(91) | 90(86.5) | 0.385 | 25(93) | 59(83) | 84(85.7) | 0.338 | 26(90) | 12(60) | 38(77.6) | 0.033 |
| 1 | 10(17) | 4(9) | 14(13.5) | 2(7) | 12(17) | 14(14.3) | 3(10) | 8(40) | 11(22.4) | |||
| Encephalopathy | ||||||||||||
| 0 | 52(88) | 30(68) | 82(79.6) | 0.024 | 23(88) | 56(79) | 79(81.4) | 0.383 | 26(93) | 18(90) | 44(91.7) | 1 |
| 1 | 7(12) | 14(32) | 21(20.4) | 3(12) | 15(21) | 18(18.6) | 2(7) | 2(10) | 4(8.3) | |||
| Seizures | ||||||||||||
| 0 | 53(88) | 36(82) | 89(85.6) | 0.404 | 24(89) | 62(87) | 86(87.8) | 1 | 27(93) | 18(90) | 45(91.8) | 1 |
| 1 | 7(12) | 8(18) | 15(14.4) | 3(11) | 9(13) | 12(12.2) | 2(7) | 2(10) | 4(8.2) | |||
| Vasculopathy/vasculitis | ||||||||||||
| 0 | 58(97) | 43(98) | 101(97.1) | 1.000 | 26(96) | 68(96) | 94(95.9) | 1 | 28(97) | 19(95) | 47(95.9) | 1 |
| 1 | 2(3) | 1(2) | 3(2.9) | 1(4) | 3(4) | 4(4.1) | 1(3) | 1(5) | 2(4.1) | |||
| Transverse Myelitis | ||||||||||||
| 0 | 48(80) | 40(91) | 88(84.6) | 0.172 | 18(67) | 67(94) | 85(86.7) | 0.001 | 19(66) | 18(90) | 37(75.5) | 0.089 |
| 1 | 12(20) | 4(9) | 16(15.4) | 9(33) | 4(6) | 13(13.3) | 10(34) | 2(10) | 12(24.5) | |||
| AHNE | ||||||||||||
| 0 | 51(85) | 43(100) | 94(91.3) | 0.010 | 23(88) | 65(92) | 88(90.7) | 0.698 | 25(86) | 18(90) | 43(87.8) | 1 |
| 1 | 9(15) | 0(0) | 9(8.7) | 3(12) | 6(8) | 9(9.3) | 4(14) | 2(10) | 6(12.2) | |||
| ADEM | ||||||||||||
| 0 | 53(88) | 41(93) | 94(90.4) | 0.512 | 23(85) | 65(92) | 88(89.8) | 0.456 | 25(86) | 17(85) | 42(85.7) | 1 |
| 1 | 7(12) | 3(7) | 10(9.6) | 4(15) | 6(8) | 10(10.2) | 4(14) | 3(15) | 7(14.3) | |||
| CLOCC/MERS | ||||||||||||
| 0 | 57(95) | 38(86) | 95(91.3) | 0.163 | 27(100) | 64(90) | 91(92.9) | 0.185 | 29(100) | 18(90) | 47(95.9) | 0.162 |
| 1 | 3(5) | 6(14) | 9(8.7) | 0(0) | 7(10) | 7(7.1) | 0(0) | 2(10) | 2(4.1) | |||
| ** Others | ||||||||||||
| 0 | 46(78) | 33(77) | 79(77.5) | 1.000 | 24(89) | 50(72) | 74(77.1) | 0.108 | 22(76) | 18(90) | 40(81.6) | 0.277 |
| 1 | 13(22) | 10(23) | 23(22.5) | 3(11) | 19(28) | 22(22.9) | 7(24) | 2(10) | 9(18.4) | |||
| Serum d Dimer | CRP | |||||||
|---|---|---|---|---|---|---|---|---|
| * Variables | Elevated | Normal | Total | Fisher Test | Elevated | Normal | Total | Fisher Test |
| n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | |
| Age | ||||||||
| 50+ | 19(66) | 2(33) | 21(60) | 0.191 | 26(68) | 2(17) | 28(56) | 0.002 |
| <50 | 10(34) | 4(67) | 14(40) | 12(32) | 10(83) | 22(44) | ||
| Sex | ||||||||
| Male | 23(79) | 3(50) | 26(74.3) | 0.162 | 28(74) | 7(58) | 35(70) | 0.471 |
| Female | 6(21) | 3(50) | 9(25.7) | 10(26) | 5(42) | 15(30) | ||
| ♦ Severity | ||||||||
| Non-severe | 9(31) | 2(40) | 11(32.4) | 1 | 9(25) | 8(80) | 17(37) | 0.003 |
| Severe | 20(69) | 3(60) | 23(67.6) | 27(75) | 2(20) | 29(63) | ||
| Fatality | ||||||||
| Non-fatal | 24(80) | 4(67) | 28(77.8) | 0.596 | 29(78) | 9(82) | 38(79.2) | 1 |
| Fatal | 6(20) | 2(33) | 8(22.2) | 8(22) | 2(18) | 10(20.8) | ||
| Stroke | ||||||||
| 0 | 27(90) | 6(100) | 33(91.7) | 1 | 36(95) | 12(100) | 48(96) | 1 |
| 1 | 3(10) | 0(0) | 3(8.3) | 2(5) | 0(0) | 2(4) | ||
| Encephalitis | ||||||||
| 0 | 26(87) | 4(67) | 30(83.3) | 0.256 | 28(74) | 12(100) | 40(80) | 0.092 |
| 1 | 4(13) | 2(33) | 6(16.7) | 10(26) | 0(0) | 10(20) | ||
| Encephalopathy | ||||||||
| 0 | 29(97) | 5(100) | 34(97.1) | 1 | 34(89) | 11(100) | 45(91.8) | 0.562 |
| 1 | 1(3) | 0(0) | 1(2.9) | 4(11) | 0(0) | 4(8.2) | ||
| Seizures | ||||||||
| 0 | 30(100) | 6(100) | 36(100) | 1 | 36(95) | 12(100) | 48(96) | 1 |
| 1 | 0(0) | 0(0) | 0(0) | 2(5) | 0(0) | 2(4) | ||
| Vasculopathy/vasculitis | ||||||||
| 0 | 29(97) | 6(100) | 35(97.2) | 1 | 38(100) | 9(75) | 0.011 | |
| 1 | 1(3) | 0(0) | 1(2.8) | 0(0) | 3(25) | 3(6) | ||
| Transverse Myelitis | ||||||||
| 0 | 25(83) | 4(67) | 29(80.6) | 0.573 | 33(87) | 7(58) | 40(80) | 0.046 |
| 1 | 5(17) | 2(33) | 7(19.4) | 5(13) | 5(42) | 10(20) | ||
| AHNE | ||||||||
| 0 | 22(73) | 5(83) | 27(75) | 1 | 31(82) | 11(92) | 42(84) | 0.661 |
| 1 | 8(27) | 1(17) | 9(25) | 7(18) | 1(8) | 8(16) | ||
| ADEM | ||||||||
| 0 | 28(93) | 6(100) | 34(94.4) | 1 | 36(95) | 9(75) | 45(90) | 0.082 |
| 1 | 2(7) | 0(0) | 2(5.6) | 2(5) | 3(25) | 5(10) | ||
| CLOCC/MERS | ||||||||
| 0 | 24(80) | 6(100) | 30(83.3) | 0.561 | 30(79) | 12(100) | 42(84) | 0.173 |
| 1 | 6(20) | 0(0) | 6(16.7) | 8(21) | 0(0) | 8(16) | ||
| ** Others | ||||||||
| 0 | 27(90) | 4(67) | 31(86.1) | 0.186 | 32(84) | 11(92) | 43(86) | 1 |
| 1 | 3(10) | 2(33) | 5(13.9) | 6(16) | 1(8) | 7(14) | ||
| Variables | N (%) |
|---|---|
| Age | |
| >50 | 73 (77.7) |
| ≤50 | 21 (22.3) |
| * Sex | |
| Male | 59 (64.1) |
| Female | 33 (35.9) |
| PNS manifestation | |
| GBS | 89 (92.7) |
| Facial palsy | 3 (3.1) |
| Polyneuritis cranialis | 2 (2.1) |
| ** COVID-19 Severity | |
| Non-severe | 62 (67.4) |
| Severe | 30 (32.6) |
| ♦ Outcome | |
| Non-fatal | 80 (88.9) |
| Fatal | 10 (11.1) |
| CSF Protein | Elevated Cell Count | Lymphocytes | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High | Low | Yes | No | |||||||||
| * Variables | >45 | ≤45 | Total | Fisher Test | >5 | ≤5 | Total | Fisher Test | >50% | ≤50% | Total | Fisher Test |
| n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | ||
| Age | ||||||||||||
| 50+ | 51(74) | 15(88) | 66(76.7) | 0.338 | 4(67) | 57(78) | 61(77.2) | 0.615 | 4(67) | 15(79) | 19(76) | 0.606 |
| <50 | 18(26) | 2(12) | 20(23.3) | 2(33) | 16(22) | 18(22.8) | 2(33) | 4(21) | 6(24) | |||
| Sex | ||||||||||||
| Male | 41(60) | 11(69) | 52(61.9) | 0.582 | 2(40) | 46(64) | 48(62.3) | 0.359 | 3(75) | 14(74) | 17(73.9) | 1 |
| Female | 27(40) | 5(31) | 32(38.1) | 3(60) | 26(36) | 29(37.7) | 1(25) | 5(26) | 6(26.1) | |||
| ♦ Severity | ||||||||||||
| Non-severe | 42(63) | 13(76) | 55(65.5) | 0.395 | 4(67) | 45(63) | 49(63.6) | 1 | 6(100) | 11(65) | 17(73.9) | 0.144 |
| Severe | 25(37) | 4(24) | 29(34.5) | 2(33) | 26(37) | 28(36.4) | 0(0) | 6(35) | 6(26.1) | |||
| Fatality | ||||||||||||
| Non-fatal | 56(85) | 17(100) | 73(88) | 0.114 | 5(83) | 62(89) | 67(88.2) | 0.544 | 6(100) | 14(82) | 20(87) | 0.539 |
| Fatal | 10(15) | 0(0) | 10(12) | 1(17) | 8(11) | 9(11.8) | 0(0) | 3(18) | 3(13) | |||
| GBS | ||||||||||||
| 0 | 3(4) | 3(17) | 6(6.8) | 0.097 | 1(17) | 5(7) | 6(7.4) | 0.38 | 3(43) | 0(0) | 3(11.5) | 0.013 |
| 1 | 67(96) | 15(83) | 82(93.2) | 5(83) | 70(93) | 75(92.6) | 4(57) | 19(100) | 23(88.5) | |||
| Facial palsy | ||||||||||||
| 0 | 70(100) | 16(89) | 86(97.7) | 0.04 | 6(100) | 73(97) | 79(97.5) | 1 | 6(86) | 19(100) | 25(96.2) | 0.269 |
| 1 | 0(0) | 2(11) | 2(2.3) | 0(0) | 2(3) | 2(2.5) | 1(14) | 0(0) | 1(3.8) | |||
| Polyneuritis Cranialis | ||||||||||||
| 0 | 68(97) | 18(100) | 86(97.7) | 1 | 6(100) | 73(97) | 79(97.5) | 1 | 6(86) | 19(100) | 25(96.2) | 0.269 |
| 1 | 2(3) | 0(0) | 2(2.3) | 0(0) | 2(3) | 2(2.5) | 1(14) | 0(0) | 1(3.8) | |||
| Serum d Dimer | CRP | Serum IL-6 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| * Variables | Elevated | Normal | Total | Fisher Test | Elevated | Normal | Total | Fisher Test | Elevated | Normal | Total | Fisher Test |
| n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | |
| Age | ||||||||||||
| 50+ | 6(86) | 2(100) | 8(88.9) | 1 | 5(100) | 6(67) | 11(78.6) | 0.258 | 5(100) | 0(0) | 5(71.4) | 0.048 |
| <50 | 1(14) | 0(0) | 1(11.1) | 0(0) | 3(33) | 3(21.4) | 0(0) | 2(100) | 2(28.6) | |||
| Sex | ||||||||||||
| Male | 4(57) | 1(50) | 5(55.6) | 1 | 2(40) | 6(67) | 8(57.1) | 0.58 | 4(80) | 2(100) | 6(85.7) | 1 |
| Female | 3(43) | 1(50) | 4(44.4) | 3(60) | 3(33) | 6(42.9) | 1(20) | 0(0) | 1(14.3) | |||
| ♦ Severity | ||||||||||||
| Non-severe | 3(43) | 2(100) | 5(55.6) | 0.444 | 3(60) | 7(78) | 10(71.4) | 0.58 | 4(80) | 2(100) | 6(85.7) | 1 |
| Severe | 4(57) | 0(0) | 4(44.4) | 2(40) | 2(22) | 4(28.6) | 1(20) | 0(0) | 1(14.3) | |||
| Fatality | ||||||||||||
| Non-fatal | 5(71) | 2(100) | 7(77.8) | 1 | 5(100) | 8(89) | 13(92.9) | 1 | 4(80) | 2(100) | 6(85.7) | 1 |
| Fatal | 2(29) | 0(0) | 2(22.2) | 0(0) | 1(11) | 1(7.1) | 1(20) | 0(0) | 1(14.3) | |||
| GBS | ||||||||||||
| 0 | 0(0) | 1(50) | 1(11.1) | 0.222 | 0(0) | 2(22) | 2(14.3) | 0.505 | 0(0) | 0(0) | 0(0) | 1 |
| 1 | 7(100) | 1(50) | 8(88.9) | 5(100) | 7(78) | 12(85.7) | 5(100) | 2(100) | 7(100) | |||
| Facial palsy | ||||||||||||
| 0 | 7(100) | 1(50) | 8(88.9) | 0.222 | 5(100) | 7(78) | 12(85.7) | 0.505 | 5(100) | 2(100) | 7(100) | 1 |
| 1 | 0(0) | 1(50) | 1(11.1) | 0(0) | 2(22) | 2(14.3) | 0(0) | 0(0) | 0(0) | |||
| Polyneuritis_Cranialis | ||||||||||||
| 0 | 7(100) | 2(100) | 9(100) | 1 | 5(100) | 9(100) | 14(100) | 1 | 5(100) | 2(100) | 7(100) | 1 |
| 1 | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | |||
| GBS | Facial Palsy | Polyneuritis Cranialis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| * Variables | 0 | 1 | Total | Fisher Test | 0 | 1 | Total | Fisher Test | 0 | 1 | Total | Fisher Test |
| n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | n (%) | n (%) | n (%) | p-Value | |
| CSF Protein | ||||||||||||
| >45 | 3(50) | 67(82) | 70(79.5) | 0.097 | 70(81) | 0(0) | 70(79.5) | 0.04 | 68(79) | 2(100) | 70(79.5) | 1 |
| ≤45 | 3(50) | 15(18) | 18(20.5) | 16(19) | 2(100) | 18(20.5) | 18(21) | 0(0) | 18(20.5) | |||
| CSF Cell Count | ||||||||||||
| >5 | 1(17) | 5(7) | 6(7.4) | 0.38 | 6(8) | 0(0) | 6(7.4) | 1 | 6(8) | 0(0) | 6(7.4) | 1 |
| ≤5 | 5(83) | 70(93) | 75(92.6) | 73(92) | 2(100) | 75(92.6) | 73(92) | 2(100) | 75(92.6) | |||
| CSF lymphocyte Percent | ||||||||||||
| >50 | 3(100) | 4(17) | 7(26.9) | 0.013 | 6(24) | 1(100) | 7(26.9) | 0.269 | 6(24) | 1(100) | 7(26.9) | 0.269 |
| ≤50 | 0(0) | 19(83) | 19(73.1) | 19(76) | 0(0) | 19(73.1) | 19(76) | 0(0) | 19(73.1) | |||
| ♦ Severity | ||||||||||||
| Non-Severe | 5(100) | 57(66) | 62(67.4) | 0.169 | 60(67) | 2(100) | 62(67.4) | 1 | 60(67) | 2(100) | 62(67.4) | 1 |
| Severe | 0(0) | 30(34) | 30(32.6) | 30(33) | 0(0) | 30(32.6) | 30(33) | 0(0) | 30(32.6) | |||
| Fatality | ||||||||||||
| Non-Fatal | 6(100) | 74(88) | 80(88.9) | 1 | 78(89) | 2(100) | 80(88.9) | 1 | 78(89) | 2(100) | 80(88.9) | 1 |
| Fatal | 0(0) | 10(12) | 10(11.1) | 10(11) | 0(0) | 10(11.1) | 10(11) | 0(0) | 10(11.1) | |||
| Age | ||||||||||||
| ≥50 | 1(20) | 72(81) | 73(77.7) | 0.008 | 72(78) | 1(50) | 73(77.7) | 0.399 | 73(79) | 0(0) | 73(77.7) | 0.048 |
| <50 | 4(80) | 17(19) | 21(22.3) | 20(22) | 1(50) | 21(22.3) | 19(21) | 2(100) | 21(22.3) | |||
| Sex | ||||||||||||
| Male | 3(75) | 56(64) | 59(64.1) | 1 | 58(64) | 1(50) | 59(64.1) | 1 | 58(64) | 1(50) | 59(64.1) | 1 |
| Female | 1(25) | 32(36) | 33(35.9) | 32(36) | 1(50) | 33(35.9) | 32(36) | 1(50) | 33(35.9) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podury, S.; Srivastava, S.; Khan, E.; Kakara, M.; Tandon, M.; Shrestha, A.K.; Freeland, K.; Wen, S.; Sriwastava, S. Relevance of CSF, Serum and Neuroimaging Markers in CNS and PNS Manifestation in COVID-19: A Systematic Review of Case Report and Case Series. Brain Sci. 2021, 11, 1354. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101354
Podury S, Srivastava S, Khan E, Kakara M, Tandon M, Shrestha AK, Freeland K, Wen S, Sriwastava S. Relevance of CSF, Serum and Neuroimaging Markers in CNS and PNS Manifestation in COVID-19: A Systematic Review of Case Report and Case Series. Brain Sciences. 2021; 11(10):1354. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101354
Chicago/Turabian StylePodury, Sanjiti, Samiksha Srivastava, Erum Khan, Mihir Kakara, Medha Tandon, Ashish K. Shrestha, Kerri Freeland, Sijin Wen, and Shitiz Sriwastava. 2021. "Relevance of CSF, Serum and Neuroimaging Markers in CNS and PNS Manifestation in COVID-19: A Systematic Review of Case Report and Case Series" Brain Sciences 11, no. 10: 1354. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101354