
Emotional Processing and Experience in Amyotrophic Lateral Sclerosis: A Systematic and Critical Review

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
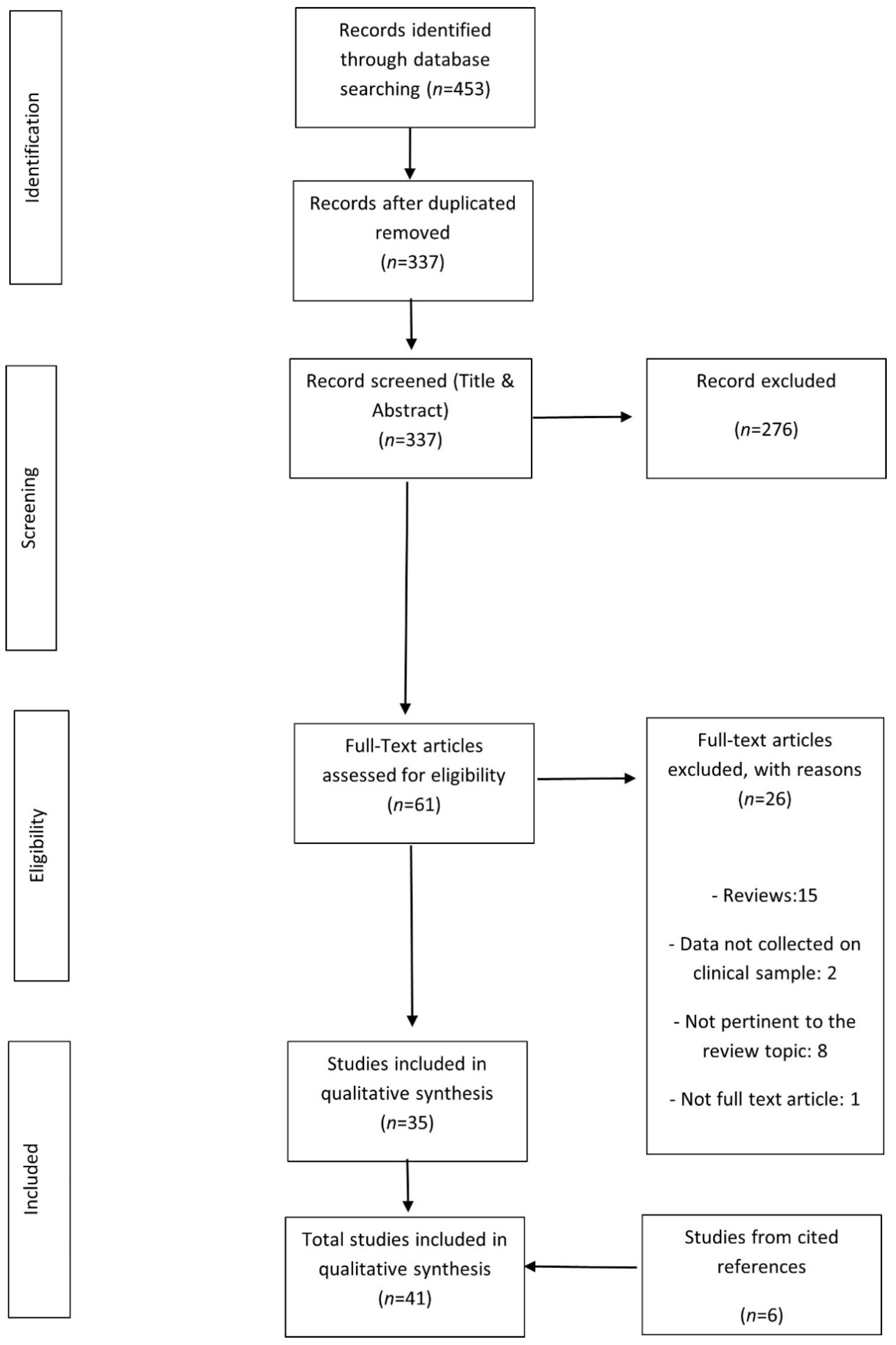
2.4. Study Selection
2.5. Data Collection Process
2.6. Risk of Bias
3. Results
3.1. Emotion Recognition
3.2. Emotional Reactivity
3.3. Emotional Responsiveness—Arousal and Elicited Emotions
3.4. Valence Attribution
3.5. Facial Approachability Rating
3.6. Memory for Emotional Material
3.7. Alexithymia
3.8. Relationship between Emotional and Clinical Aspects
3.9. Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bora, E. Meta-analysis of social cognition in amyotrophic lateral sclerosis. Cortex 2017, 88, 1–7. [Google Scholar] [CrossRef]
- Consonni, M.; Catricalà, E.; Dalla Bella, E.; Gessa, V.C.; Lauria, G.; Cappa, S.F. Beyond the consensus criteria: Multiple cognitive profiles in amyotrophic lateral sclerosis? Cortex 2016, 81, 162–167. [Google Scholar] [CrossRef]
- Strong, M.; Abrahams, S.; Goldstein, L.; Woolley, S.; Mclaughlin, P.; Snowden, J.; Mioshi, E.; Roberts-South, A.; Benatar, M.; Hortobágyi, T.; et al. Amyotrophic lateral sclerosis—Frontotemporal spectrum disorder (ALS-FTSD): Revised diagnostic criteria. Amyotroph. Lateral Scler. Front. Degener. 2017, 18, 153–174. [Google Scholar] [CrossRef]
- Beeldman, E.; Raaphorst, J.; Klein Twennaar, M.; de Visser, M.; Schmand, B.A.; de Haan, R.J. The cognitive profile of ALS: A systematic review and meta-analysis update. J. Neurol. Neurosurg. Psychiatry 2016, 87, 611–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christidi, F.; Migliaccio, R.; Santamaría-García, H.; Santangelo, G.; Trojsi, F. Social Cognition Dysfunctions in Neurodegenerative Diseases: Neuroanatomical Correlates and Clinical Implications. Behav. Neurol. 2018, 1849794. [Google Scholar] [CrossRef] [PubMed]
- Poletti, B.; Carelli, L.; Lunetta, C.; Ticozzi, N.; Silani, V. Advance care planning and mental capacity in ALS: A current challenge for an unsolved matter. Neurol. Sci. 2020, 41, 2997–2998. [Google Scholar] [CrossRef] [PubMed]
- Lulé, D.; Ehlich, B.; Lang, D.; Sorg, S.; Heimrath, J.; Kübler, A.; Birbaumer, N.; Ludolph, A.C. Quality of life in fatal disease: The flawed judgement of the social environment. J. Neurol. 2013, 260, 2836–2843. [Google Scholar] [CrossRef]
- Fortier, J.; Besnard, J.; Allain, P. Theory of mind, empathy and emotion perception in cortical and subcortical neurodegenerative diseases. Rev. Neurol. 2018, 174, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Radakovic, R.; Stephenson, L.; Newton, J.; Crockford, C.; Swingler, R.; Chandran, S.; Abrahams, S. Multidimensional apathy and executive dysfunction in amyotrophic lateral sclerosis. Cortex 2017, 94, 142–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benbrika, S.; Desgranges, B.; Eustache, F.; Viader, F. Cognitive, Emotional and Psychological Manifestations in Amyotrophic Lateral Sclerosis at Baseline and Overtime: A Review. Front. Neurosci. 2019, 13, 951. [Google Scholar] [CrossRef]
- Elamin, M.; Pender, N.; Hardiman, O.; Abrahams, S. Social cognition in neurodegenerative disorders: A systematic review. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1071–1079. [Google Scholar] [CrossRef]
- Marco-Garcia, S.; Ferrer-Quintero, M.; Usall, J.; Ochoa, S.; Del Cacho, N.; Huerta-Ramos, E. Facial emotion recognition in neurological disorders: A narrative review. Rev. Neurol. 2019, 69, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Poletti, M.; Enrici, I.; Adenzato, M. Cognitive and affective Theory of Mind in neurodegenerative diseases: Neuropsychological, neuroanatomical and neurochemical levels. Neurosci. Biobehav. Rev. 2012, 36, 2147–2164. [Google Scholar] [CrossRef]
- Sedda, A. Disorders of emotional processing in amyotrophic lateral sclerosis. Curr. Opin. Neurol. 2014, 27, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Ackley, B.J.; Swan, B.A.; Ladwig, G.; Tucker, S. Evidence-Based Nursing Care Guidelines: Medical-Surgical Interventions; Mosby Elsevier: St. Louis, MO, USA, 2008; p. 7. [Google Scholar]
- Ahmed, R.M.; Devenney, E.M.; Strikwerda-Brown, C.; Hodges, J.R.; Piguet, O.; Kiernan, M.C. Phenotypic variability in ALS-FTD and effect on survival. Neurology 2020, 94, e2005–e2013. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Werner, K.; Roy, S.; Trojanowski, J.Q.; Morgan-Kane, U.; Miller, B.L.; Rankin, K.P. A case study of an emerging visual artist with frontotemporal lobar degeneration and amyotrophic lateral sclerosis. Neurocase 2009, 15, 235–247. [Google Scholar] [CrossRef]
- Woolley, J.D.; Strobl, E.V.; Sturm, V.E.; Shany-Ur, T.; Poorzand, P.; Grossman, S.; Nguyen, L.; Eckart, J.A.; Levenson, R.W.; Seeley, W.W.; et al. Impaired Recognition and Regulation of Disgust Is Associated with Distinct but Partially Overlapping Patterns of Decreased Gray Matter Volume in the Ventroanterior Insula. Biol. Psychiatry 2015, 78, 505–514. [Google Scholar] [CrossRef] [Green Version]
- Savage, S.A.; Lillo, P.; Kumfor, F.; Kiernan, M.C.; Piguet, O.; Hodges, J.R. Emotion processing deficits distinguish pure amyotrophic lateral sclerosis from frontotemporal dementia. Amyotroph. Lateral Scler. Front. Degener. 2014, 15, 39–46. [Google Scholar] [CrossRef]
- Vonk, J.M.J.; Borghesani, V.; Battistella, G.; Younes, K.; DeLeon, J.; Welch, A.; Hubbard, H.I.; Miller, Z.A.; Miller, B.L.; Gorno-Tempini, M.L. Verbal Semantics and the Left Dorsolateral Anterior Temporal Lobe: A Longitudinal Case of Bilateral Temporal Degeneration. Aphasiology 2020, 34, 865–885. [Google Scholar] [CrossRef]
- Lulé, D.; Kurt, A.; Jürgens, R.; Kassubek, J.; Diekmann, V.; Kraft, E.; Neumann, N.; Ludolph, A.C.; Birbaumer, N.; Anders, S. Emotional responding in amyotrophic lateral sclerosis. J. Neurol. 2005, 252, 1517–1524. [Google Scholar] [CrossRef]
- Lulé, D.; Diekmann, V.; Anders, S.; Kassubek, J.; Kübler, A.; Ludolph, A.C.; Birbaumer, N. Brain responses to emotional stimuli in patients with amyotrophic lateral sclerosis (ALS). J. Neurol. 2007, 254, 519–527. [Google Scholar] [CrossRef]
- Zimmerman, E.K.; Eslinger, P.J.; Simmons, Z.; Barrett, A.M. Emotional perception deficits in amyotrophic lateral sclerosis. Cogn. Behav. Neurol. 2007, 20, 79–82. [Google Scholar] [CrossRef]
- de Alcântara, C.; Cruzeiro, M.M.; França, M.C., Jr.; Camargos, S.T.; de Souza, L.C. Amyotrophic lateral sclerosis type 8 is not a pure motor disease: Evidence from a neuropsychological and behavioural study. J. Neurol. 2019, 266, 1980–1987. [Google Scholar] [CrossRef]
- Burke, T.; Pinto-Grau, M.; Lonergan, K.; Elamin, M.; Bede, P.; Costello, E.; Hardiman, O.; Pender, N. Measurement of Social Cognition in Amyotrophic Lateral Sclerosis: A Population Based Study. PLoS ONE 2016, 11, e0160850. [Google Scholar] [CrossRef] [Green Version]
- Schulz, P.E.; York, M.K. Overview of Cognitive Function in ALS, with Special Attention to the Temporal Lobe: Semantic Fluency and Rating the Approachability of Faces. In Amyotrophic Lateral Sclerosis; IntechOpen: London, UK, 2012. [Google Scholar] [CrossRef] [Green Version]
- Watermeyer, T.J.; Brown, R.G.; Sidle, K.C.; Oliver, D.J.; Allen, C.; Karlsson, J.; Ellis, C.M.; Shaw, C.E.; Al-Chalabi, A.; Goldstein, L.H. Executive dysfunction predicts social cognition impairment in amyotrophic lateral sclerosis. J. Neurol. 2015, 262, 1681–1690. [Google Scholar] [CrossRef] [Green Version]
- Aho-Özhan, H.E.; Keller, J.; Heimrath, J.; Uttner, I.; Kassubek, J.; Birbaumer, N.; Ludolph, A.C.; Lulé, D. Perception of Emotional Facial Expressions in Amyotrophic Lateral Sclerosis (ALS) at Behavioural and Brain Metabolic Level. PLoS ONE 2016, 11, e0164655. [Google Scholar] [CrossRef] [PubMed]
- Benbrika, S.; Doidy, F.; Carluer, L.; Mondou, A.; Buhour, M.S.; Eustache, F.; Viader, F.; Desgranges, B. Alexithymia in Amyotrophic Lateral Sclerosis and Its Neural Correlates. Front. Neurol. 2018, 24, 566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerami, C.; Dodich, A.; Canessa, N.; Crespi, C.; Iannaccone, S.; Corbo, M.; Lunetta, C.; Consonni, M.; Scola, E.; Falini, A.; et al. Emotional empathy in amyotrophic lateral sclerosis: A behavioural and voxel-based morphometry study. Amyotroph. Lateral Scler. Front. Degener. 2014, 15, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Crespi, C.; Cerami, C.; Dodich, A.; Canessa, N.; Iannaccone, S.; Corbo, M.; Lunetta, C.; Falini, A.; Cappa, S.F. Microstructural Correlates of Emotional Attribution Impairment in Non-Demented Patients with Amyotrophic Lateral Sclerosis. PLoS ONE 2016, 11, e0161034. [Google Scholar] [CrossRef] [Green Version]
- Crespi, C.; Santi, G.C.; Dodich, A.; Lupo, F.; Greco, L.C.; Piccoli, T.; Lunetta, C.; Cerami, C. Unraveling Moral Reasoning in Amyotrophic Lateral Sclerosis: How Emotional Detachment Modifies Moral Judgment. Front. Psychol. 2020, 11, 2083. [Google Scholar] [CrossRef]
- Gillingham, S.M.; Yunusova, Y.; Ganda, A.; Rogaeva, E.; Black, S.E.; Stuss, D.T.; Zinman, L. Assessing cognitive functioning in ALS: A focus on frontal lobe processes. Amyotroph. Lateral Scler. Front. Degener. 2017, 18, 182–192. [Google Scholar] [CrossRef]
- Lillo, P.; Savage, S.; Mioshi, E.; Kiernan, M.C.; Hodges, J.R. Amyotrophic lateral sclerosis and frontotemporal dementia: A behavioural and cognitive continuum. Amyotroph. Lateral Scler. 2012, 13, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Lillo, P.; Caramelli, P.; Musa, G.; Parrao, T.; Hughes, R.; Aragon, A.; Valenzuela, D.; Cea, G.; Aranguiz, R.; Guimarães, H.C.; et al. Inside minds, beneath diseases: Social cognition in amyotrophic lateral sclerosis-frontotemporal spectrum disorder. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1279–1282. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.P.; Prado, L.G.R.; Lillo, P.; Mioshi, E.; Teixeira, A.L.; de Souza, L.C. Deficits in Emotion Recognition as Markers of Frontal Behavioral Dysfunction in Amyotrophic Lateral Sclerosis. J. Neuropsychiatry Clin. Neurosci. 2019, 31, 165–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.I.; Oh, K.W.; Kim, H.J.; Park, J.S.; Kim, S.H. Impaired Perception of Emotional Expression in Amyotrophic Lateral Sclerosis. J. Clin. Neurol. 2016, 12, 295–300. [Google Scholar] [CrossRef]
- Staios, M.; Fisher, F.; Lindell, A.K.; Ong, B.; Howe, J.; Reardon, K. Exploring sarcasm detection in amyotrophic lateral sclerosis using ecologically valid measures. Front. Hum. Neurosci. 2013, 7, 178. [Google Scholar] [CrossRef] [Green Version]
- Schmolck, H.; Mosnik, D.; Schulz, P. Rating the approachability of faces in ALS. Neurology 2007, 69, 2232–2235. [Google Scholar] [CrossRef]
- Trojsi, F.; Siciliano, M.; Russo, A.; Passaniti, C.; Femiano, C.; Ferrantino, T.; De Liguoro, S.; Lavorgna, L.; Monsurrò, M.R.; Tedeschi, G.; et al. Theory of Mind and Its Neuropsychological and Quality of Life Correlates in the Early Stages of Amyotrophic Lateral Sclerosis. Front. Psychol. 2016, 7, 1934. [Google Scholar] [CrossRef] [Green Version]
- Trojsi, F.; Di Nardo, F.; Santangelo, G.; Siciliano, M.; Femiano, C.; Passaniti, C.; Caiazzo, G.; Fratello, M.; Cirillo, M.; Monsurrò, M.R.; et al. Resting state fMRI correlates of Theory of Mind impairment in amyotrophic lateral sclerosis. Cortex 2017, 97, 1–16. [Google Scholar] [CrossRef]
- Kilani, M.; Micallef, J.; Soubrouillard, C.; Rey-Lardiller, D.; Dematteï, C.; Philippot, P.; Ceccaldi, M.; Pouget, J.; Blin, O. A longitudinal study of the evolution of cognitive function and affective state in patients with amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Other Mot. Neuron Disord. 2004, 5, 46–54. [Google Scholar] [CrossRef]
- Cavallo, M.; Adenzato, M.; Macpherson, S.E.; Karwig, G.; Enrici, I.; Abrahams, S. Evidence of social understanding impairment in patients with amyotrophic lateral sclerosis. PLoS ONE 2011, 6, e25948. [Google Scholar] [CrossRef] [Green Version]
- Crespi, C.; Cerami, C.; Dodich, A.; Canessa, N.; Arpone, M.; Iannaccone, S.; Corbo, M.; Lunetta, C.; Scola, E.; Falini, A.; et al. Microstructural white matter correlates of emotion recognition impairment in Amyotrophic Lateral Sclerosis. Cortex 2014, 53, 1–8. [Google Scholar] [CrossRef]
- Cuddy, M.; Papps, B.J.; Thambisetty, M.; Leigh, P.N.; Goldstein, L.H. Processing and memory for emotional and neutral material in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 2012, 13, 592–598. [Google Scholar] [CrossRef]
- Girardi, A.; MacPherson, S.E.; Abrahams, S. Deficits in emotional and social cognition in amyotrophic lateral sclerosis. Neuropsychology 2011, 25, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Jelsone-Swain, L.; Persad, C.; Burkard, D.; Welsh, R.C. Action processing and mirror neuron function in patients with amyotrophic lateral sclerosis: An fMRI study. PLoS ONE 2015, 10, e0119862. [Google Scholar] [CrossRef]
- Meier, S.L.; Charleston, A.J.; Tippett, L.J. Cognitive and behavioural deficits associated with the orbitomedial prefrontal cortex in amyotrophic lateral sclerosis. Brain 2010, 133, 3444–3457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papps, B.; Abrahams, S.; Wicks, P.; Leigh, P.N.; Goldstein, L.H. Changes in memory for emotional material in amyotrophic lateral sclerosis (ALS). Neuropsychologia 2005, 43, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Passamonti, L.; Fera, F.; Tessitore, A.; Russo, A.; Cerasa, A.; Gioia, C.M.; Monsurrò, M.R.; Migliaccio, R.; Tedeschi, G.; Quattrone, A. Dysfunctions within limbic-motor networks in amyotrophic lateral sclerosis. Neurobiol. Aging 2013, 34, 2499–2509. [Google Scholar] [CrossRef] [PubMed]
- Yunusova, Y.; Ansari, J.; Ramirez, J.; Shellikeri, S.; Stanisz, G.J.; Black, S.E.; Gillingham, S.M.; Kiss, A.; Stuss, D.T.; Zinman, L. Frontal Anatomical Correlates of Cognitive and Speech Motor Deficits in Amyotrophic Lateral Sclerosis. Behav. Neurol. 2019, 13, 9518309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotchoubey, B.; Kaiser, J.; Bostanov, V.; Lutzenberger, W.; Birbaumer, N. Recognition of affective prosody in brain-damaged patients and healthy controls: A neurophysiological study using EEG and whole-head MEG. Cogn. Affect. Behav. Neurosci. 2009, 9, 153–167. [Google Scholar] [CrossRef] [Green Version]
- Palmieri, A.; Naccarato, M.; Abrahams, S.; Bonato, M.; D’Ascenzo, C.; Balestreri, S.; Cima, V.; Querin, G.; Dal Borgo, R.; Barachino, L.; et al. Right hemisphere dysfunction and emotional processing in ALS: An fMRI study. J. Neurol. 2010, 257, 1970–1978. [Google Scholar] [CrossRef] [PubMed]
- Andrews, S.C.; Staios, M.; Howe, J.; Reardon, K.; Fisher, F. Multimodal emotion processing deficits are present in amyotrophic lateral sclerosis. Neuropsychology 2017, 31, 304–310. [Google Scholar] [CrossRef]
- Young, A.W.; Perrett, D.; Calder, A.; Sprengelmeyer, R.; Ekman, P. Facial Expressions of Emotion: Stimuli and Tests (FEEST); Thames Valley Test Company (TVTC): Suffolk, UK, 2002. [Google Scholar]
- Passarelli, M.; Masini, M.; Bracco, F.; Petrosino, M.; Chiorri, C. Development and Validation of the Facial Expression Recognition Test (FERT). Psychol. Assess. 2018, 30, 1479–1490. [Google Scholar] [CrossRef] [PubMed]
- Froming, K.B.; Gregory, A.; Levy, C.M.; Ekman, P. The Comprehensive Affective Testing System. User’s Manual; Psychology Software Tools, Inc.: Gainesville, FL, USA, 2006. [Google Scholar]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The “Reading the Mind in the Eyes” Test revised version: A study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 2001, 42, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Oakley, B.F.M.; Brewer, R.; Bird, G.; Catmur, C. Theory of mind is not theory of emotion: A cautionary note on the Reading the Mind in the Eyes Test. J. Abnorm. Psychol. 2016, 125, 818–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, S.; Bornhofen, C.; Shum, D.; Long, E.; Saunders, C.; Neulinger, K. Reliability and validity of The Awareness of Social Inference Test (TASIT): A clinical test of social perception. Disabil. Rehabil. 2006, 28, 1529–1542. [Google Scholar] [CrossRef]
- Lane, R.D.; Sechrest, L.; Riedel, R. Sociodemographic correlates of alexithymia. Compr. Psychiatry 1998, 39, 377–385. [Google Scholar] [CrossRef]
- Kang, C.; Wang, Z. Emotionally enhanced memory relied on arousal and valence: Automatic and controlled processes. Acta Psychol. Sin. 2013, 45, 970–980. [Google Scholar] [CrossRef]
- Frith, C.D.; Frith, U. Implicit and Explicit Processes in Social Cognition. Neuron 2008, 60, 503–510. [Google Scholar] [CrossRef] [Green Version]
- de Gelder, B.; Van den Stock, J. The Bodily Expressive Action Stimulus Test (BEAST). Construction and Validation of a Stimulus Basis for Measuring Perception of Whole Body Expression of Emotions. Front. Psychol. 2011, 2, 181. [Google Scholar] [CrossRef] [Green Version]
- Van den Stock, J.; De Winter, F.L.; de Gelder, B.; Rangarajan, J.R.; Cypers, G.; Maes, F.; Sunaert, S.; Goffin, K.; Vandenberghe, R.; Vandenbulcke, M. Impaired recognition of body expressions in the behavioral variant of frontotemporal dementia. Neuropsychologia 2015, 75, 496–504. [Google Scholar] [CrossRef]
- Kret, M.E.; Stekelenburg, J.J.; Roelofs, K.; de Gelder, B. Perception of face and body expressions using electromyography, pupillometry and gaze measures. Front. Psychol. 2013, 4, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trinkler, I.; Devignevielle, S.; Achaibou, A.; Ligneul, R.V.; Brugières, P.; Cleret de Langavant, L.; De Gelder, B.; Scahill, R.; Schwartz, S.; Bachoud-Lévi, A.C. Embodied emotion impairment in Huntington’s Disease. Cortex 2017, 92, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Fisher, P.; Dodd, R.; Barrow, E.; Makin, S.; Cherry, M.G.; Rodriguez-Blazquez, C. Predictors of distress in amyotrophic lateral sclerosis: A systematic review. Cogent Psychol. 2019, 6, 1608031. [Google Scholar] [CrossRef]
- Poletti, B.; Carelli, L.; Solca, F.; Pezzati, R.; Faini, A.; Ticozzi, N.; Mitsumoto, H.; Silani, V. Sexuality and intimacy in ALS: Systematic literature review and future perspectives. J. Neurol. Neurosurg. Psychiatry 2019, 90, 712–719. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Emotion Variable | Emotional Test or Stimuli | References |
|---|---|---|
| Emotion recognition (ER): Identification of emotional states with attribution of labels (e.g., joy, sadness, disgust) | ||
| Static facial expressions (SF) | FEEST (Ekman 60 Faces test, Ekman Caricatures task and Morphing); FERT; CATS; RME | [2,9,16,19,20,23,24,27,28,32,33,34,35,36,37,38,40,43,44,46,47,49,50,51,54] |
| Static scenes (SS) | SET | [2,21,33,45] |
| Written stories (WS) | EAT | [40,41] |
| Dynamic social vignettes (DS) | TASIT (emotion evaluation subtest); emotional film clips | [17,18,19,20,27,38] |
| Emotional prosody (PR) | CATS; aprosodia battery | [20,23,48,54] |
| Cross-modal integration (CI) | CATS | [54] |
| Emotional reactivity: Physiological, muscular and brain activity correlates of emotional stimulations | ||
| Coded facial expressions (CF) | variety of subjective/objective emotional stimuli | [17] |
| Physiological data-PA (SC, EMG, GSR, HR, EM) | IAPS; variety of subjective/objective emotional stimuli | [17,21] |
| Brain activation data-BR (fMRI, EEG) | POFA; FEEST; unpleasant/neutral words; IAPS; emotional vocalizations | [22,28,50,52,53] |
| Emotional responsiveness (ER): Subjective reporting of emotional activation | IAPS; emotional film clips, variety of subjective/objective emotional stimuli; moral dilemmas. | [17,21,22,32,42] |
| Approachability attribution (AA): Subjective rating of friendliness of presented emotional faces. | 60 images of faces (from Adolphs and colleagues, 1998) | [26,39,49] |
| Valence attribution (VA): Subjective rating of the affective quality related to the attractiveness/averseness of presented stimuli | IAPS; moral dilemmas; Brierley–Medford sentences; Phelps words | [21,32,45] |
| Alexithymia (AX): Difficulty in identifying and describing emotions and feelings | TAS-20 | [29] |
| Memory for emotional material (ME): Encoding and retention of information related to emotional stimuli/experiences | Brierley–Medford sentences; Phelps words; emotional/neutral sentences; unpleasant/neutral words; autobiographical material | [17,45,49,53] |
| Research Issues |
|---|
|
|
|
|
| Clinical Issues |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carelli, L.; Solca, F.; Tagini, S.; Torre, S.; Verde, F.; Ticozzi, N.; Consonni, M.; Ferrucci, R.; Pravettoni, G.; Poletti, B.; et al. Emotional Processing and Experience in Amyotrophic Lateral Sclerosis: A Systematic and Critical Review. Brain Sci. 2021, 11, 1356. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101356
Carelli L, Solca F, Tagini S, Torre S, Verde F, Ticozzi N, Consonni M, Ferrucci R, Pravettoni G, Poletti B, et al. Emotional Processing and Experience in Amyotrophic Lateral Sclerosis: A Systematic and Critical Review. Brain Sciences. 2021; 11(10):1356. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101356
Chicago/Turabian StyleCarelli, Laura, Federica Solca, Sofia Tagini, Silvia Torre, Federico Verde, Nicola Ticozzi, Monica Consonni, Roberta Ferrucci, Gabriella Pravettoni, Barbara Poletti, and et al. 2021. "Emotional Processing and Experience in Amyotrophic Lateral Sclerosis: A Systematic and Critical Review" Brain Sciences 11, no. 10: 1356. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101356