
Anxiety, Perceived Stress, and Resilience during the COVID-19 Pandemic: Population Estimates of Persons Presenting to a General Practitioner in Romania


Abstract
:1. Introduction
Pandemic Situation in Romania
2. Materials and Methods
2.1. Participants
2.2. Statistical Analysis
3. Results
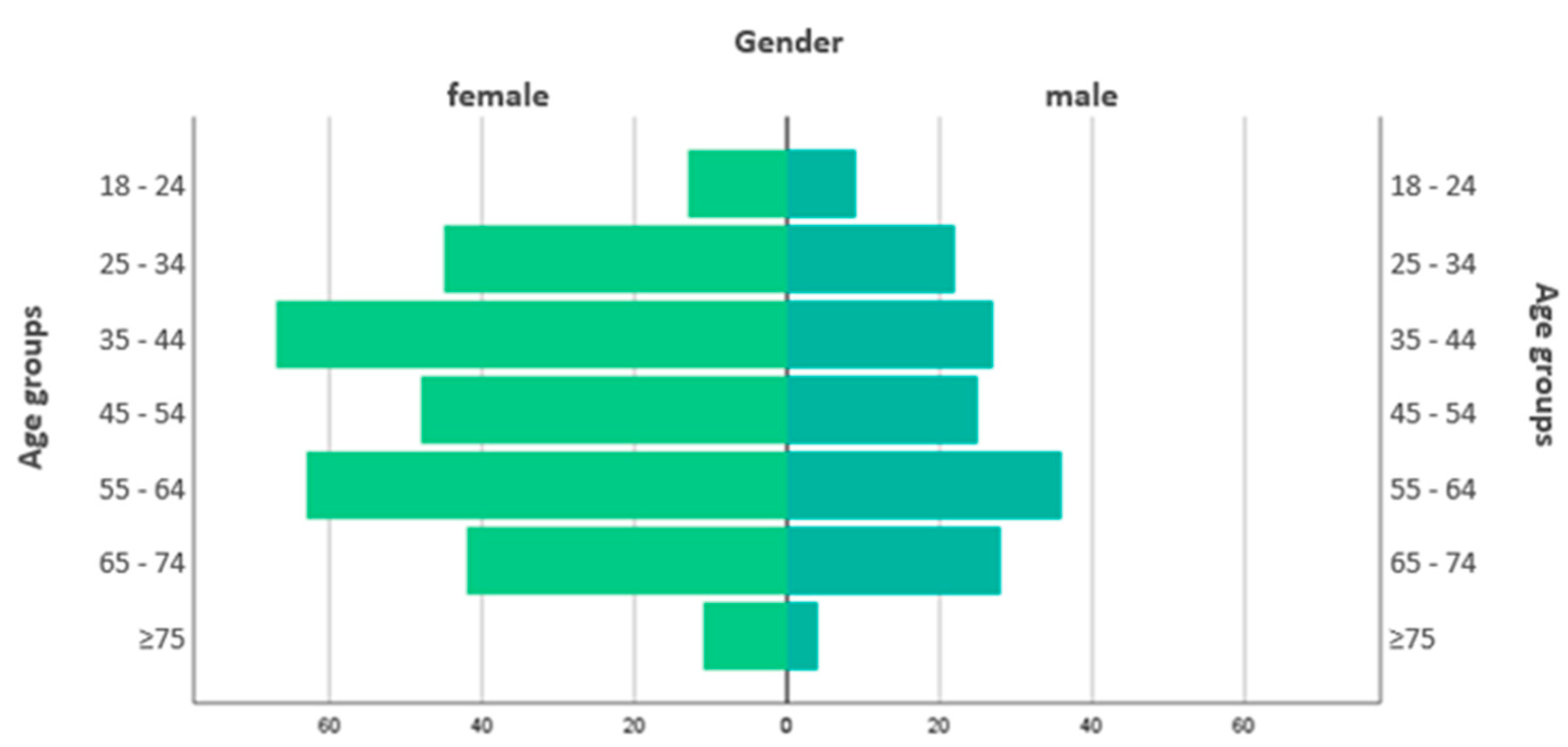
3.1. Sociodemographic Characteristics
3.2. COVID-19 Status
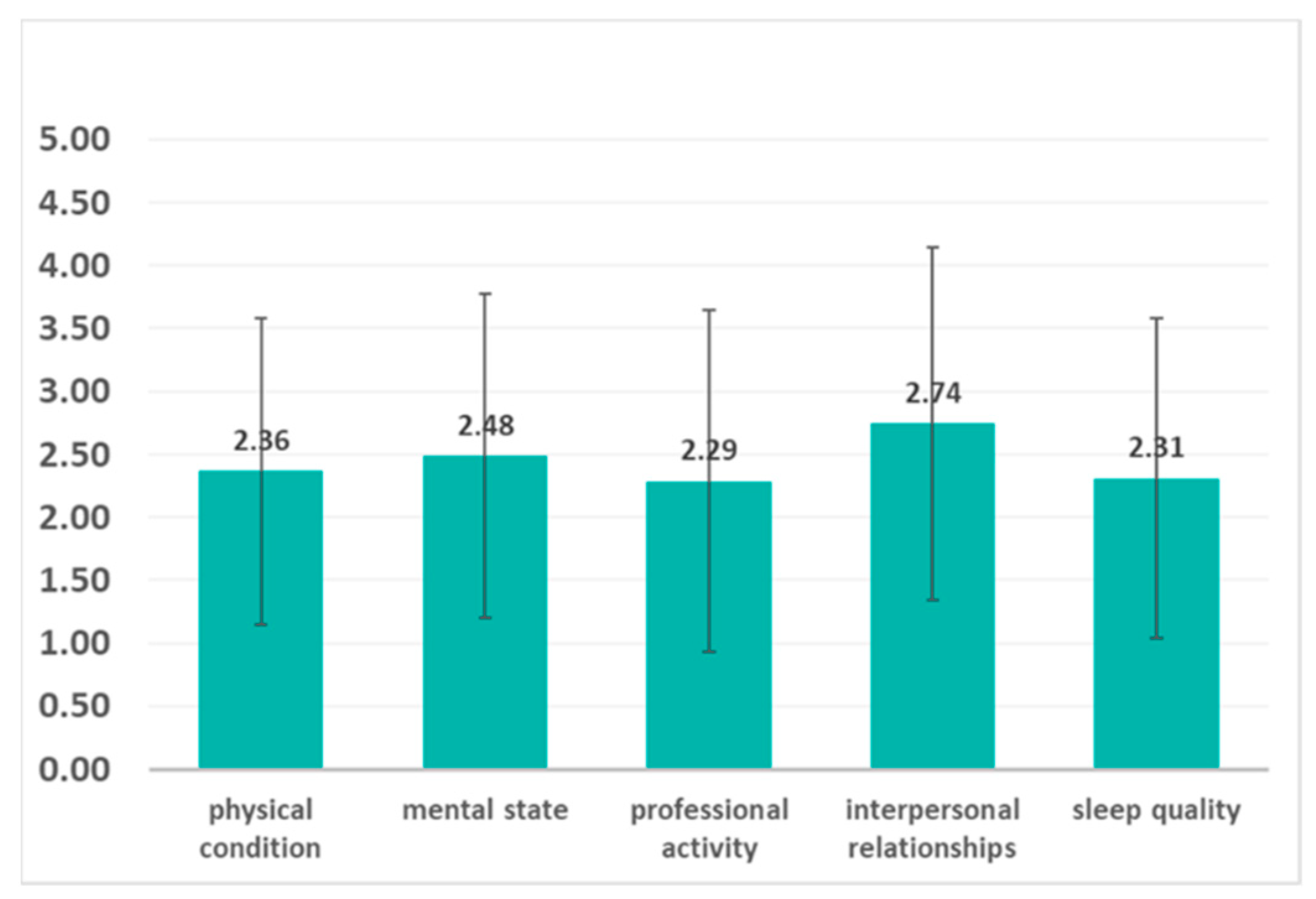
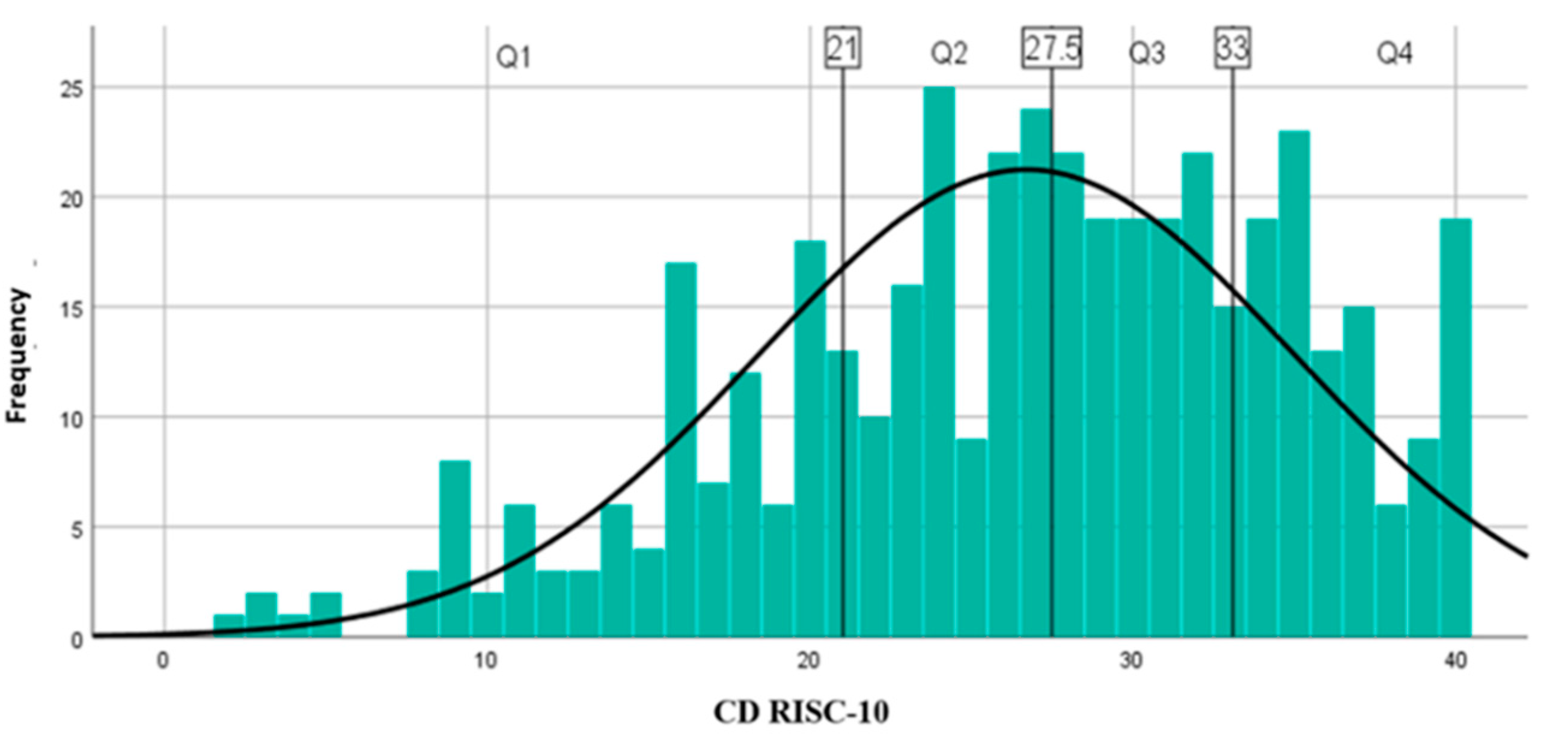
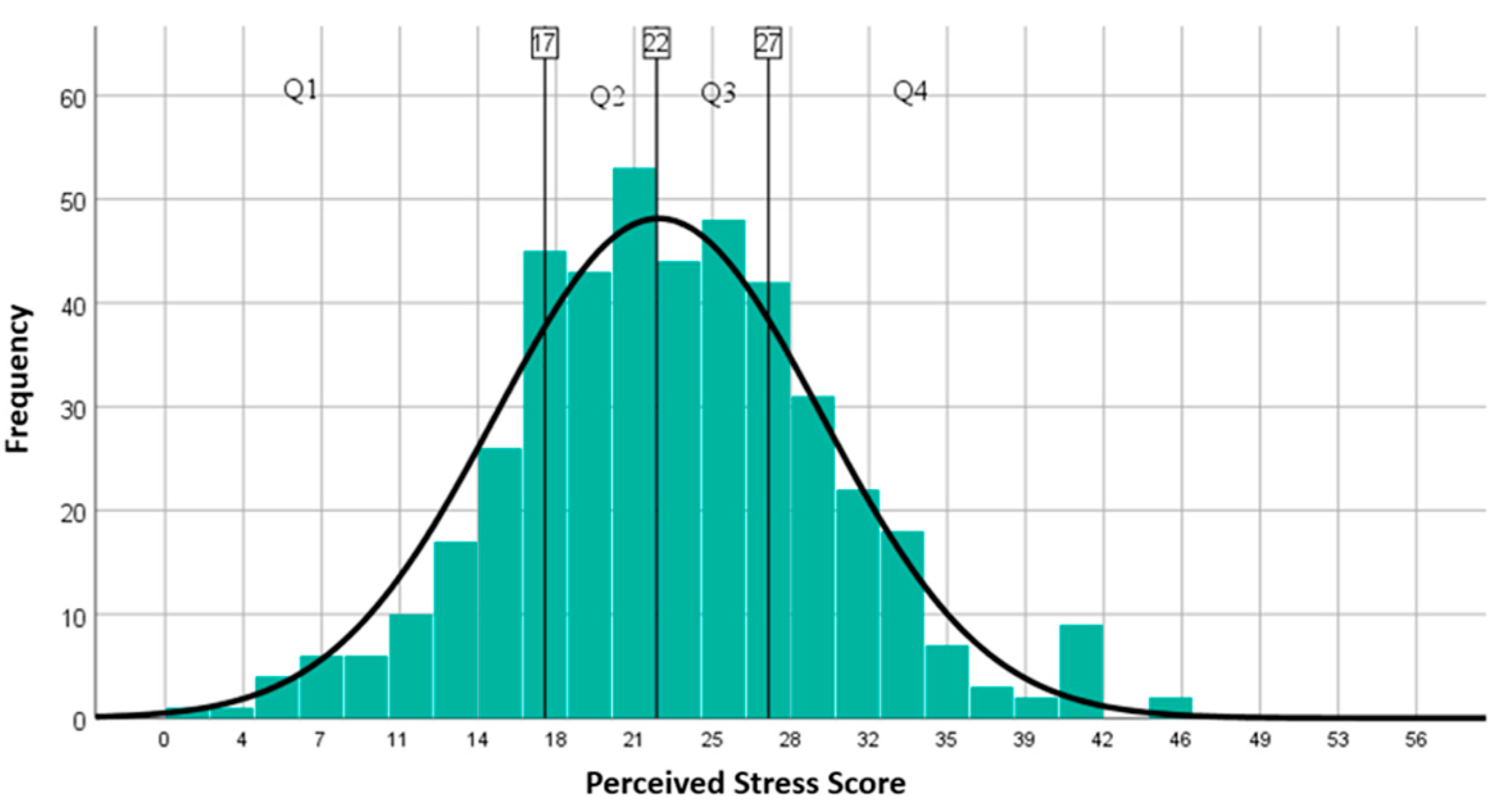
3.3. Clinical Characteristics
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghebreyesus, T. WHO Director-General Opening Remarks at the Member State Briefing on the COVID-19 Pandemic Evaluation. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 24 October 2021).
- Cénat, J.M.; Felix, N.; Blais-Rochette, C.; Rousseau, C.; Bukaka, J.; Derivois, D.; Noorishad, P.G.; Birangui, J.P. Prevalence of mental health problems in populations affected by the Ebola virus disease: A systematic review and meta-analysis. Psychiatry Res. 2020, 289, 113033. [Google Scholar] [CrossRef]
- Keita, M.M.; Taverne, B.; Savané, S.S.; March, L.; Doukoure, M.; Sow, M.S.; Touré, A.; Etard, J.F.; Barry, M.; Delaporte, E. Depressive symptoms among survivors of Ebola virus disease in Conakry (Guinea): Preliminary results of the PostEboGui cohort. BMC Psychiatry 2017, 17, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, A.; Sheikh, T.L.; Gidado, S.; Poggensee, G.; Nguku, P.; Olayinka, A.; Ohuabunwo, C.; Waziri, N.; Shuaib, F.; Adeyemi, J.; et al. An evaluation of psychological distress and social support of survivors and contacts of Ebola virus disease infection and their relatives in Lagos, Nigeria: A cross sectional study—2014. BMC Public Health 2015, 15, 824. [Google Scholar] [CrossRef] [Green Version]
- Xiao, S.; Luo, D.; Xiao, Y. Survivors of COVID-19 are at high risk of posttraumatic stress disorder. Glob. Health Res. Policy 2020, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Jobe, M.C.; Mathis, A.A. Mental health characteristics associated with dysfunctional coronavirus anxiety. Psychol. Med. 2021, 51, 1403–1404. [Google Scholar] [CrossRef] [Green Version]
- Cénat, J.M.; Dalexis, R.D.; Guerrier, M.; Noorishad, P.G.; Derivois, D.; Bukaka, J.; Birangui, J.P.; Adansikou, K.; Clorméus, L.A.; Kokou-Kpolou, C.K.; et al. Frequency and correlates of anxiety symptoms during the COVID-19 pandemic in low-and middle-income countries: A multinational study. J. Psychiatr. Res. 2021, 132, 13–17. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated psychological problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Cénat, J.M.; Blais-Rochette, C.; Kokou-Kpolou, C.K.; Noorishad, P.G.; Mukunzi, J.N.; McIntee, S.E.; Dalexis, R.D.; Goulet, M.A.; Labelle, P. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2020, 295, 113599. [Google Scholar] [CrossRef]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with suspected COVID-19 symptoms were more likely depressed and had lower health-related quality of life: The potential benefit of health literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [Green Version]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Bo, H.X.; Li, W.; Yang, Y.; Wang, Y.; Zhang, Q.; Cheung, T.; Wu, X.; Xiang, Y.T. Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol. Med. 2021, 51, 1052–1053. [Google Scholar] [CrossRef] [Green Version]
- Candini, M.; Battaglia, S.; Benassi, M.; di Pellegrino, G.; Frassinetti, F. The physiological correlates of interpersonal space. Sci Rep. 2021, 11, 2611. [Google Scholar] [CrossRef] [PubMed]
- Ellena, G.; Battaglia, S.; Làdavas, E. The spatial effect of fearful faces in the autonomic response. Exp. Brain Res. 2020, 238, 2009–2018. [Google Scholar] [CrossRef]
- Borgomaneri, S.; Vitale, F.; Battaglia, S.; Avenanti, A. Early Right Motor Cortex Response to Happy and Fearful Facial Expressions: A TMS Motor-Evoked Potential Study. Brain Sci. 2021, 11, 1203. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Scott, K.M.; de Jonge, P.; Kessler, R.C. Epidemiology of anxiety disorders: From surveys to nosology and back. Dialogues Clin. Neurosci. 2017, 19, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Santabárbara, J.; Lasheras, I.; Lipnicki, D.M.; Bueno-Notivol, J.; Pérez-Moreno, M.; López-Antón, R.; De la Cámara, C.; Lobo, A.; Gracia-García, P. Prevalence of anxiety in the COVID-19 pandemic: An updated meta-analysis of community-based studies. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 109, 110207. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Kalisch, R.; Müller, M.B.; Tüscher, O. A conceptual framework for the neurobiological study of resilience. Behav. Brain Sci. 2015, 38, e92. [Google Scholar] [CrossRef]
- American Psychological Association. Building your Resilience. Available online: http://www.apa.org/topics/resilience (accessed on 25 September 2021).
- Mancini, A.D.; Bonanno, G.A. Predictors and parameters of resilience to loss: Toward an individual differences model. J. Pers. 2009, 77, 1805–1832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalisch, R.; Baker, D.G.; Basten, U.; Boks, M.P.; Bonanno, G.A.; Brummelman, E.; Chmitorz, A.; Fernàndez, G.; Fiebach, C.J.; Galatzer-Levy, I.; et al. The resilience framework as a strategy to combat stress-related disorders. Nat. Hum. Behav. 2017, 1, 784–790. [Google Scholar] [CrossRef] [Green Version]
- Gilan, D.; Röthke, N.; Blessin, M.; Kunzler, A.; Stoffers-Winterling, J.; Müssig, M.; Yuen, K.S.; Tüscher, O.; Thrul, J.; Kreuter, F.; et al. Psychomorbidity, Resilience, and Exacerbating and Protective Factors During the SARS-CoV-2 Pandemic: A Systematic Literature Review and Results from the German COSMO-PANEL. Dtsch. Arztebl. Int. 2020, 117, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Sampogna, G.; Del Vecchio, V.; Giallonardo, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; Menculini, G.; et al. What Is the Role of Resilience and Coping Strategies on the Mental Health of the General Population during the COVID-19 Pandemic? Results from the Italian Multicentric COMET Study. Brain Sci. 2021, 11, 1231. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Veer, I.M.; Riepenhausen, A.; Zerban, M.; Wackerhagen, C.; Puhlmann, L.M.C.; Engen, H.; Köber, G.; Bögemann, S.; Weermeijer, J.; Uściłko, A.; et al. Psycho-social factors associated with mental resilience in the Corona lockdown. Transl. Psychiatry 2021, 11, 67. [Google Scholar] [CrossRef]
- Finn, P.; Cinpoes, R.; Ichijo, A.; Ledger, R.; Nancheva, N.; Pettitt, R.; Ranta, R. Covid-19 and Democracy, First Cut Policy Analyses: Country Case Studies; Project Report; Kingston University: London, UK, 2020. [Google Scholar]
- Johns Hopkins University of Medicine. Coronavirus Resource Center. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/region/romania (accessed on 1 October 2021).
- Chiruţă, C.; Bulgariu, E.; Avsec, J.; Ferčec, B.; Mencinger, M. Comparison of the Evolution of the COVID-19 Disease between Romania and Italy. Appl. Syst. Innov. 2020, 3, 44. [Google Scholar] [CrossRef]
- Zung, W.W. A rating instrument for anxiety disorders. Psychosomatics 1971, 12, 371–379. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Deacon, B.J.; Abramowitz, J.S.; Tolin, D.F. Dimensionality of somatic complaints: Factor structure and psychometric properties of the Self-Rating Anxiety Scale. J. Anxiety Disord. 2006, 20, 543–561. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.R.T. Connor-Davidson Resilience Scale (CD-RISC) Manual. Unpublished. 01.01. 2021.
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Lara-Cabrera, M.L.; Betancort, M.; Muñoz-Rubilar, C.A.; Novo, N.R.; De las Cuevas, C. The Mediating Role of Resilience in the Relationship between Perceived Stress and Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 9762. [Google Scholar] [CrossRef] [PubMed]
- Bottino, F.; Tagliente, E.; Pasquini, L.; Napoli, A.D.; Lucignani, M.; Figà-Talamanca, L.; Napolitano, A. COVID Mortality Prediction with Machine Learning Methods: A Systematic Review and Critical Appraisal. J. Pers. Med. 2021, 11, 893. [Google Scholar] [CrossRef]
- Wei, L.; Islam, J.Y.; Mascareno, E.A.; Rivera, A.; Vidot, D.C.; Camacho-Rivera, M. Physical and Mental Health Impacts of the COVID-19 Pandemic among US Adults with Chronic Respiratory Conditions. J. Clin. Med. 2021, 10, 3981. [Google Scholar] [CrossRef]
- Monforte, A.D.; Tavelli, A.; Bai, F.; Tomasoni, D.; Falcinella, C.; Castoldi, R.; Barbanotti, D.; Mulè, G.; Allegrini, M.; Suardi, E.; et al. Declining Mortality Rate of Hospitalised Patients in the Second Wave of the COVID-19 Epidemics in Italy: Risk Factors and the Age-Specific Patterns. Life 2021, 11, 979. [Google Scholar] [CrossRef]
- Pan, K.Y.; Kok, A.A.; Eikelenboom, M.; Horsfall, M.; Jörg, F.; Luteijn, R.A.; Rhebergen, D.; van Oppen, P.; Giltay, E.J.; Penninx, B.W. The mental health impact of the COVID-19 pandemic on people with and without depressive, anxiety, or obsessive-compulsive disorders: A longitudinal study of three Dutch case-control cohorts. Lancet Psychiatry 2021, 8, 121–129. [Google Scholar] [CrossRef]
- Borgomaneri, S.; Serio, G.; Battaglia, S. Please, don’t do it! Ten years of progress of non-invasive brain stimulation in action inhibition. Cortex 2020, 132, 404–422. [Google Scholar] [CrossRef]
- Borgomaneri, S.; Battaglia, S.; Garofalo, S.; Tortora, F.; Avenanti, A.; di Pellegrino, G. State-dependent TMS over prefrontal cortex disrupts fear-memory reconsolidation and prevents the return of fear. Curr. Biol. 2020, 30, 3672–3679. [Google Scholar] [CrossRef]
- Borgomaneri, S.; Battaglia, S.; Avenanti, A.; di Pellegrino, G. Don’t Hurt Me No More: State-dependent Transcranial Magnetic Stimulation for the treatment of specific phobia. J. Affect. Disord. 2021, 286, 78–79. [Google Scholar] [CrossRef]
- Borgomaneri, S.; Battaglia, S.; Sciamanna, G.; Tortora, F.; Laricchiuta, D. Memories are not written in stone: Re-writing fear memories by means of non-invasive brain stimulation and optogenetic manipulations. Neurosci. Biobehav. Rev. 2021, 127, 334–352. [Google Scholar] [CrossRef]
- Battaglia, S.; Serio, G.; Scarpazza, C.; D’Ausilio, A.; Borgomaneri, S. Frozen in (e) motion: How reactive motor inhibition is influenced by the emotional content of stimuli in healthy and psychiatric populations. Behav. Res. Ther. 2021, 146, 103963. [Google Scholar] [CrossRef]
- Hyland, P.; Shevlin, M.; McBride, O.; Murphy, J.; Karatzias, T.; Bentall, R.P.; Martinez, A.; Vallières, F. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr. Scand. 2020, 142, 249–256. [Google Scholar] [CrossRef]
- Petrovič, F.; Murgaš, F.; Králik, R. Happiness in Czechia during the COVID-19 Pandemic. Sustainability 2021, 13, 10826. [Google Scholar] [CrossRef]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; Stocks, T.V.; et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych. Open 2020, 6, E125. [Google Scholar] [CrossRef]
- Georgieva, I.; Lepping, P.; Bozev, V.; Lickiewicz, J.; Pekara, J.; Wikman, S.; Loseviča, M.; Raveesh, B.N.; Mihai, A.; Lantta, T. Prevalence, New Incidence, Course, and Risk Factors of PTSD, Depression, Anxiety, and Panic Disorder during the Covid-19 Pandemic in 11 Countries. Healthcare 2021, 9, 664. [Google Scholar] [CrossRef]
- Varga, T.V.; Bu, F.; Dissing, A.S.; Elsenburg, L.K.; Bustamante, J.J.H.; Matta, J.; Rod, N.H. Loneliness, Worries, Anxiety, and Precautionary Behaviours in Response to the Covid-19 Pandemic: A Longitudinal Analysis of 200,000 Western and Northern Europeans. Lancet Reg. Health Eur. 2021, 2, 100020. [Google Scholar] [CrossRef]
- Ionescu, T.C. Anxiety, perceived stress, and resilience during the COVID-19 pandemic. Mendeley Data 2021, V1. Available online: https://data.mendeley.com/datasets/c9x7gj6c8p/1 (accessed on 19 November 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Place of Residence, % (N) | ||
|---|---|---|
| Urban | 84.5 | (372) |
| Rural | 15.5 | (68) |
| Marital Status, %, (N) | ||
| Married | 297 | (67.5) |
| Widowed | 38 | (8.6) |
| Divorced | 27 | (6.1) |
| In a relationship | 36 | (8.2) |
| Alone | 42 | (9.5) |
| Number of Children, %, (N) | ||
| 0 | 21.4 | (94) |
| 1 | 32.5 | (143) |
| 2 | 38.2 | (168) |
| ≥3 | 8.0 | (35) |
| Living with Someone Else, %, (N) 84.5 (372) | ||
| Education Level, %, (N) | ||
| High school graduation | 54.1 | (238) |
| Bachelor’s Degree Certificate | 30.9 | (136) |
| Master’s Degree Certificate | 12.5 | (55) |
| Doctoral Degree Certificate and Postdoctoral studies | 2.5 | (11) |
| Occupation, %, (N) | ||
| Unemployed | 8.4 | (37) |
| Student | 3.0 | (13) |
| Employed | 53.4 | (235) |
| Retired | 35.2 | 155) |
| Revenues, %, (N) | ||
| Decreased | 44.8 | (197) |
| Stagnated | 38.4 | (169) |
| Increased | 16.8 | (74) |
| Weekly Working Hours *, %, (N) | ||
| <20 | 45.7 | (201) |
| 20–39 | 21.6 | (95) |
| >40 | 32.7 | (144) |
| Any Comorbid Mental Condition(s) %, (N) | ||
|---|---|---|
| Yes | 7.0 | (31) |
| No | 93.0 | (409) |
| Mental Condition(s), %, (N) | ||
| Major depression disorder | 4.8 | (21) |
| Anxiety disorder | 0.7 | (3) |
| Others | 1.4 | (6) |
| Any Comorbid Physical Condition(s) | ||
| Yes | 53.4 | (235) |
| No | 46.6 | (205) |
| Physical Condition(s), %, (N) | ||
| Cardiovascular | 34.1 | (150) |
| Rheumatic or musculoskeletal | 12.5 | (55) |
| Metabolic | 11.8 | (52) |
| Gastrointestinal | 7.0 | (31) |
| Pulmonary | 5.2 | (23) |
| Oncologic | 5.2 | (23) |
| Renal | 4.5 | (20) |
| Other | 4.7 | (21) |
| Physical Activity, %, (N) | |||||
|---|---|---|---|---|---|
| Inactive | 22.0 | (97) | |||
| Mild | 40.7 | (179) | |||
| Moderate | 29.8 | (131) | |||
| Intense | 7.5 | (33) | |||
| Use of Alcohol and Tobacco | |||||
| Smoking Status, %, (N) | Drinking Status, %, (N) | ||||
| Never smoked | 44.3 | (195) | Never drank | 48.6 | (214) |
| Former smoker | 29.8 | (131) | <2 units/day | 50 | (220) |
| <20 cigarettes/day | 24.8 | (109) | >2 units/day | 1.4 | (6) |
| >20 cigarettes/day | 1.1 | (5) | |||
| Smoking Habit in the Pandemic, %, (N) | Drinking Habit in the Pandemic, %, (N) | ||||
| Decreased | 11.4 | (50) | Decreased | 31.8 | (140) |
| Stagnated | 84.3 * | (371) | Stagnated * | 65.2 | (287) |
| Increased | 4.3 | (19) | Increased | 3.0 | (13) |
| Resilience among Different Age Groups | CD RISC-10 a | |||||
|---|---|---|---|---|---|---|
| Mean | Standard Deviation | Median | Percentile 25 | Percentile 75 | ||
| Age Groups | 18–24 | 26.55 | 5.90 | 27 | 24.00 | 30.00 |
| 25–34 | 28.69 | 7.78 | 29 | 23.00 | 34.00 | |
| 35 = 44 | 28.36 | 7.83 | 30 | 25.00 | 34.00 | |
| 45–54 | 28.21 | 7.72 | 29 | 24.00 | 34.00 | |
| 55–64 | 25.82 | 8.31 | 26 | 20.00 | 33.00 | |
| 65–74 | 23.87 | 8.78 | 24 | 18.00 | 31.00 | |
| >75 | 19.33 | 8.62 | 18 | 11.00 | 27.00 | |
| Stress among Different Age Groups | PSS-14 b | |||||
| Mean | Standard Deviation | Median | Percentile 25 | Percentile 75 | ||
| Age Groups | 18–24 | 23.14 | 7.56 | 23.00 | 18.00 | 28.00 |
| 25–34 | 19.40 | 8.25 | 19.00 | 14.00 | 25.00 | |
| 35 = 44 | 20.70 | 6.82 | 21.00 | 16.00 | 25.00 | |
| 45–54 | 21.63 | 6.68 | 20.00 | 17.00 | 24.00 | |
| 55–64 | 22.58 | 7.00 | 22.00 | 17.00 | 27.00 | |
| 65–74 | 24.84 | 6.71 | 25.00 | 20.00 | 29.00 | |
| >75 | 27.40 | 6.15 | 27.00 | 22.00 | 31.00 | |
| Variables | Anxiety SAS a, Mean Score (SD) | p Value | Resilience CD RISC-10 b Mean Score (SD) | p Value | Stress PSS c Mean Score (SD) | p Value |
|---|---|---|---|---|---|---|
| Education Level | ||||||
| High school graduation | 52.31 (+/−10.34) | <0.001 ** | 20.79 (+/−9.42) | <0.001 ** | 26.44 (+/−8.43) | <0.001 ** |
| Bachelor’s Degree Certificate | 44.35 (+/−9.08) | 27.16 (+/−6.80) | 21.95 (+/−6.82) | |||
| Master’s Degree Certificate | 43.85 (+/−11.04) | 29.24 (+/−7.55) | 20.87 (+/−6.50) | |||
| Doctoral Degree Certificate | 37.18 (+/−5.72) | 33.82 (+/−3.74) | 15.64 (+/−6.04) | |||
| Occupation | ||||||
| Unemployed | 49.26 (+/−12.59) | =0.009 ** | 23.29 (+/−9.90) | =0.046 * | 25.94 (+/−8.74) | =0.9 |
| Student | 43.77 (+/−6.88) | 28.46 (+/−5.77) | 21.92 (+/−7.03) | |||
| Employed | 42.47 (+/−9.70) | 28.80 (+/−7.00) | 20.00 (+/−6.64) | |||
| Retired | 48.75 (+/−10.40) | 24.21 (+/−8.87) | 24.15 (+/−6.91) | |||
| Revenues | ||||||
| Decreased | 47.74 (+/−10.51) | <0.001 ** | 25.38 (+/−8.91) | <0.001 ** | 24.69 (+/−7.71) | =0.001** |
| Stagnated | 44.56 (+/−9.98) | 27.11 (+/−7.77) | 21.80 (+/−6.96) | |||
| Increased | 39.47 (+/−8.48) | 29.25 (+/−5.64) | 20.49 (+/−5.81) | |||
| Weekly Working Hours *** | ||||||
| <20 | 48.46 (+/−10.94) | <0.001 ** | 23.79 (+/−9.10) | <0.001 ** | 24.11 (+/−7.80) | <0.001 ** |
| 20–39 | 42.27 (+/−8.18) | 28.15 (+/−7.23) | 20.67 (+/−5.81) | |||
| >40 | 43.78 (+/−9.67) | 29.40 (+/−6.12) | 20.36 (+/− 6.58) | |||
| Resilience Level (CD RISC-10) | Stress Level (PSS) | Anxiety Index (SAS) | ||
|---|---|---|---|---|
| Resilience Level (CD RISC-10) | Pearson Correlation | 1 | −0.676 ** | −0.551 ** |
| Sig. (2-tailed) | 0.000 | 0.000 | ||
| Stress Level (PSS) | Pearson Correlation | −0.676 ** | 1 | 0.622 ** |
| Sig. (2-tailed) | 0.000 | 0.000 | ||
| Anxiety Index (SAS) | Pearson Correlation | −0.551 ** | 0.622 ** | 1 |
| Sig. (2-tailed) | 0.000 | 0.000 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ionescu, T.C.; Fetecau, B.I.; Boscaiu, V.; Tudose, C. Anxiety, Perceived Stress, and Resilience during the COVID-19 Pandemic: Population Estimates of Persons Presenting to a General Practitioner in Romania. Brain Sci. 2021, 11, 1541. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111541
Ionescu TC, Fetecau BI, Boscaiu V, Tudose C. Anxiety, Perceived Stress, and Resilience during the COVID-19 Pandemic: Population Estimates of Persons Presenting to a General Practitioner in Romania. Brain Sciences. 2021; 11(11):1541. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111541
Chicago/Turabian StyleIonescu, Tiberiu Constantin, Bogdana Ioana Fetecau, Voicu Boscaiu, and Catalina Tudose. 2021. "Anxiety, Perceived Stress, and Resilience during the COVID-19 Pandemic: Population Estimates of Persons Presenting to a General Practitioner in Romania" Brain Sciences 11, no. 11: 1541. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111541