
Programmable Shunt Valves for Pediatric Hydrocephalus: 22-Year Experience from a Singapore Children’s Hospital

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Demographics
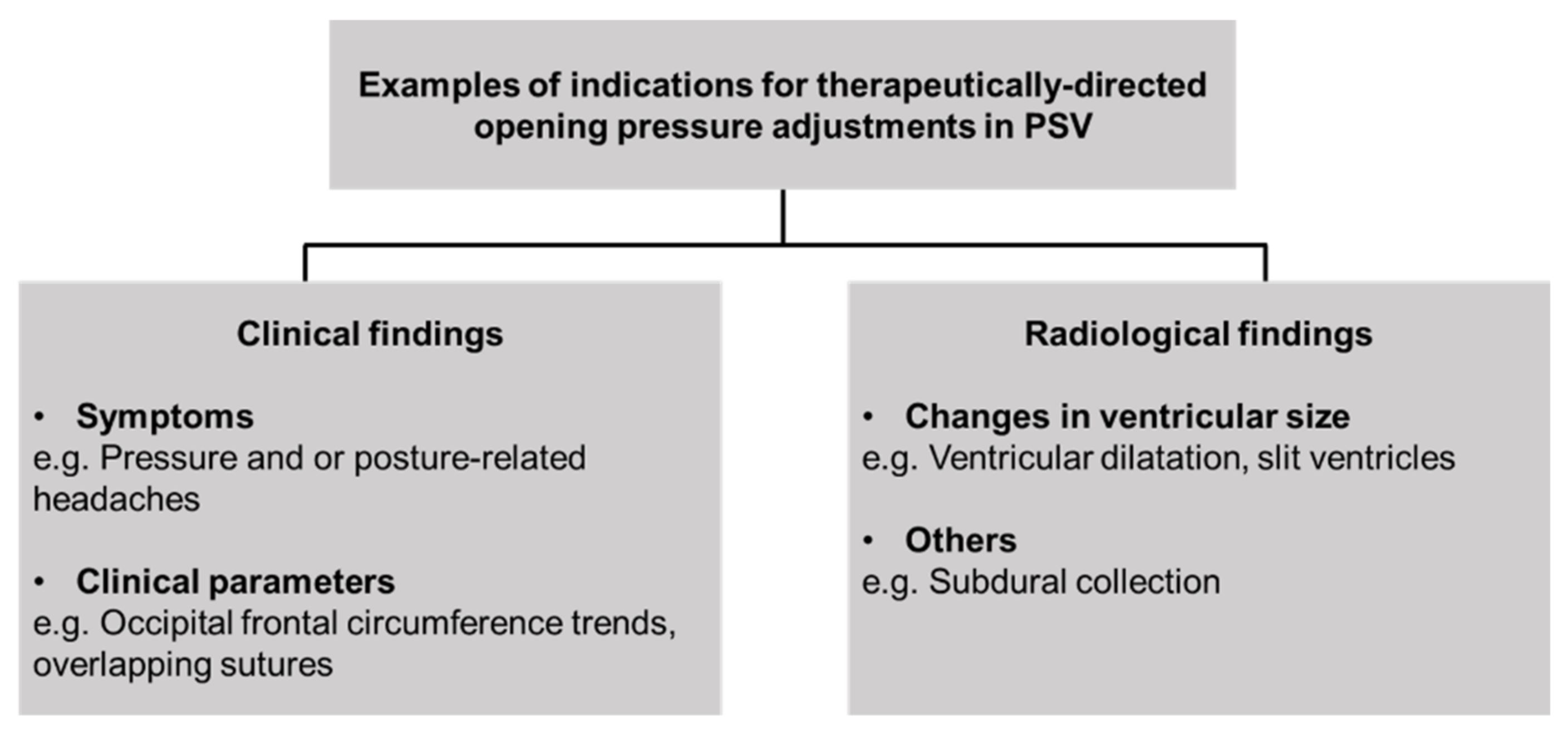
2.2. Incidence of Opening Pressure Adjustments in PSV
2.3. Statistical Methods
3. Results
3.1. Overview of Study Population and its Demographics
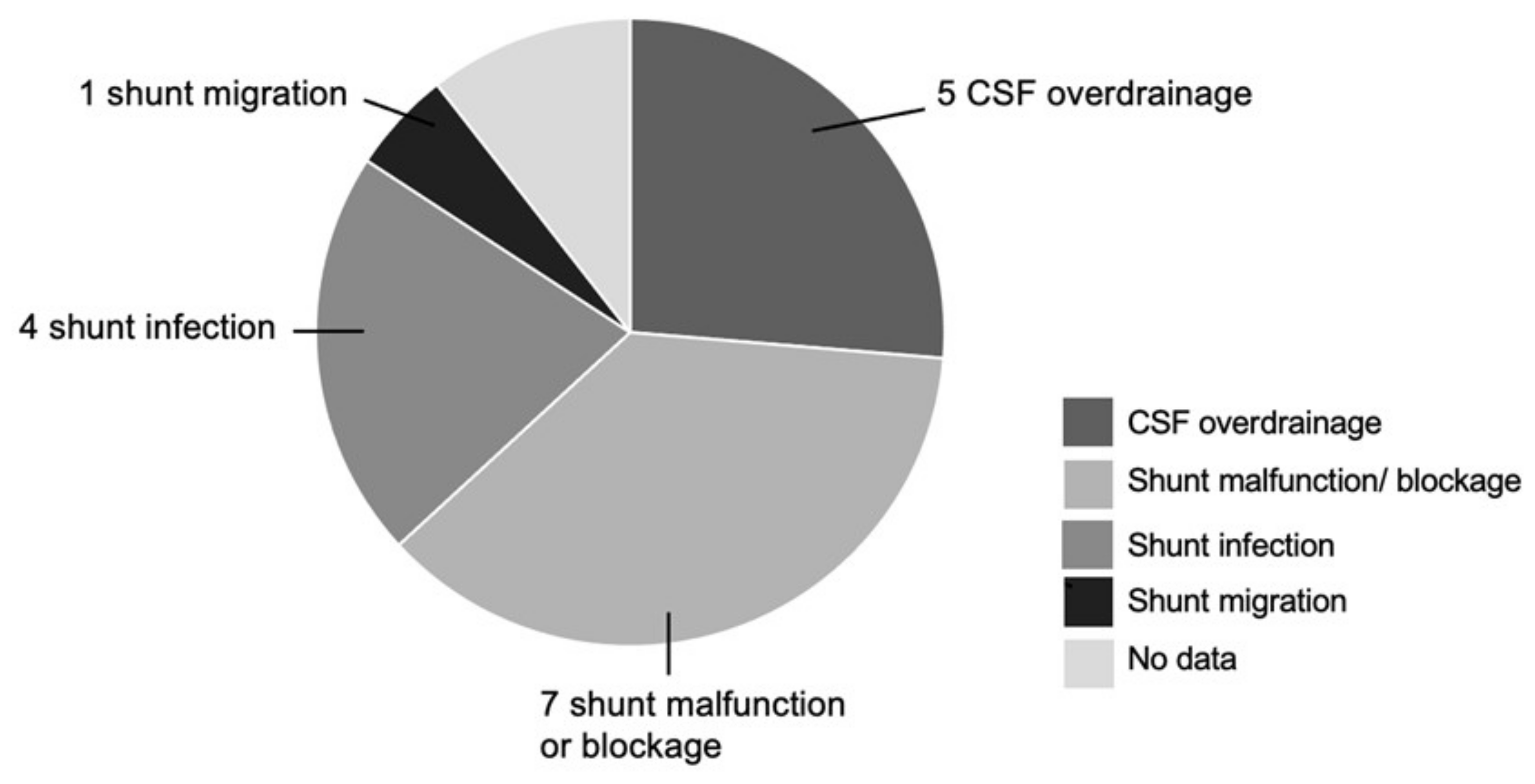
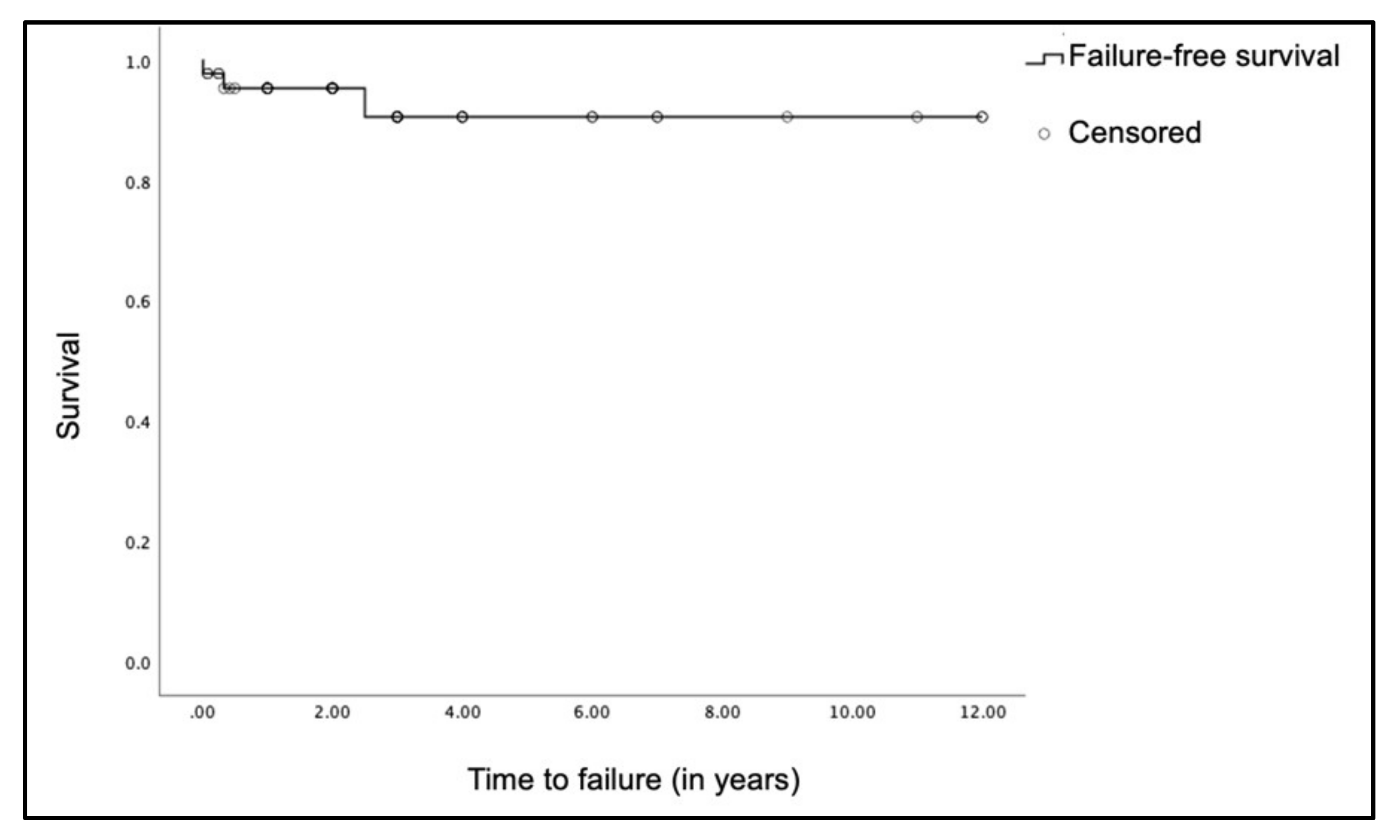
3.2. Types of PSV Encountered and Shunt Failure Rate
3.3. Analysis of Frequency of PSV Adjustments
4. Discussion
4.1. Is There a Therapeutic Role for PSV in Pediatric Hydrocephalus?
4.2. Quantifying Adjustments in PSV—Has Our Use Been Appropriate?
4.3. Limitations of the PSV
4.4. Study Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flannery, A.M.; Mitchell, L. Pediatric hydrocephalus: Systematic literature review and evidence-based guidelines. Part 1: Introduction and methodology. J. Neurosurg. Pediatr. 2014, 14, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Notarianni, C.; Vannemreddy, P.; Caldito, G.; Bollam, P.; Wylen, E.; Willis, B.; Nanda, A. Congenital hydrocephalus and ven-triculoperitoneal shunts: Influence of etiology and programmable shunts on revisions. J. Neurosurg. Pediatr. 2009, 4, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Beuriat, P.-A.; Puget, S.; Cinalli, G.; Blauwblomme, T.; Beccaria, K.; Zerah, M.; Sainte-Rose, C. Hydrocephalus treatment in children: Long-term outcome in 975 consecutive patients. J. Neurosurg. Pediatr. 2017, 20, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, M.K.; Black, N.A.; Lamping, D.L.; McKee, C.M.; Sanderson, C.F.B.; Askham, J.; Marteau, T. Consensus development methods, and their use in clinical guideline development. Health Technol. Assess. 1998, 2, 1–88. [Google Scholar] [CrossRef] [Green Version]
- Mangano, F.T.; Menendez, J.A.; Habrock, T.; Narayan, P.; Leonard, J.R.; Park, T.S.; Smyth, M.D. Early programmable valve mal-functions in pediatric hydrocephalus. J. Neurosurg. 2005, 103 (Suppl. S6), 501–507. [Google Scholar]
- Zemack, G.; Bellner, J.; Siesjö, P.; Strömblad, L.-G.; Romner, B. Clinical experience with the use of a shunt with an adjustable valve in children with hydrocephalus. J. Neurosurg. 2003, 98, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Black, P.M.; Hakim, R.; Bailey, N.O. The use of the Codman-Medos Programmable Hakim valve in the management of pa-tients with hydrocephalus: Illustrative cases. Neurosurgery 1994, 34, 1110–1113. [Google Scholar]
- Lumenta, C.B.; Roosen, N.; Dietrich, U. Clinical experience with a pressure-adjustable valve SOPHY in the management of hydrocephalus. Child Nerv. Syst. 1990, 6, 270–274. [Google Scholar] [CrossRef]
- Drake, J.M.; Kestle, J.R.; Milner, R.; Cinalli, G.; Boop, F.; Piatt, J., Jr.; Haines, S.; Schiff, S.J.; Cochrane, D.D.; Steinbok, P.; et al. Ran-domized trial of cerebrospinal fluid shunt valve design in pediatric hydrocephalus. Neurosurgery 1998, 43, 294–303. [Google Scholar] [CrossRef] [Green Version]
- McGirt, M.J.; Buck, D.W., 2nd; Sciubba, D.; Woodworth, G.F.; Carson, B.; Weingart, J.; Jallo, G. Adjustable vs set-pressure valves decrease the risk of proximal shunt obstruction in the treatment of pediatric hydrocephalus. Childs Nerv. Syst. 2007, 23, 289–295. [Google Scholar] [CrossRef]
- Davis, S.E.; Levy, M.L.; McComb, J.G.; Sposto, R. The Delta Valve: How Does Its Clinical Performance Compare with Two other Pressure Differential Valves without Antisiphon Control? Pediatr. Neurosurg. 2000, 33, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Drake, J.M.; Kestle, J.R.; Tuli, S. CSF shunts 50 years on—past, present and future. Childs Nerv. Syst. 2000, 16, 800–804. [Google Scholar] [CrossRef]
- Kestle, J.; Drake, J.; Milner, R.; Sainte-Rose, C.; Cinalli, G.; Boop, F.; Piatt, J.; Haines, S.; Schiff, S.; Cochrane, D.; et al. Long-term fol-low-up data from the Shunt Design Trial. Pediatr. Neurosurg. 2000, 33, 230–236. [Google Scholar] [CrossRef]
- Kestle, J.; Milner, R.; Drake, J. The shunt design trial: Variation in surgical experience did not influence shunt survival. Pediatr. Neurosurg. 1999, 30, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Xenos, C.; Sgouros, S.; Natarajan, K.; Walsh, A.R.; Hockley, A. Influence of shunt type on ventricular volume changes in children with hydrocephalus. J. Neurosurg. 2003, 98, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Kaufman, B.A.; Park, T. Outcome Analysis of Initial Neonatal Shunts: Does the Valve Make a Difference? Pediatr. Neurosurg. 2002, 37, 287–294. [Google Scholar] [CrossRef]
- Berns, J.; Priddy, B.; Belal, A.; Seibold, R.D.; Zieles, K.; Jea, A. Standardization of cerebrospinal fluid shunt valves in pediatric hydrocephalus: An analysis of cost, operative time, length of stay, and shunt failure. J. Neurosurg. Pediatr. 2021, 27, 400–405. [Google Scholar] [CrossRef]
- Baird, L.C.; Mazzola, C.A.; Auguste, K.I.; Klimo, P., Jr.; Flannery, A.M. Pediatric Hydrocephalus Systematic R, Evidence-Based Guidelines Task F: Pediatric hydrocephalus: Systematic literature review and evidence-based guidelines. Part 5: Effect of valve type on cerebrospinal fluid shunt efficacy. J. Neurosurg. Pediatr. 2014, 14 (Suppl. S1), 35–43. [Google Scholar] [CrossRef] [Green Version]
- Symss, N.P.; Oi, S. Is there an ideal shunt? A panoramic view of 110 years in CSF diversions and shunt systems used for the treatment of hydrocephalus: From historical events to current trends. Childs Nerv. Syst. 2014, 31, 191–202. [Google Scholar] [CrossRef]
- Texakalidis, P.; Tora, M.; Wetzel, J.S.; Chern, J.J. Endoscopic third ventriculostomy versus shunt for pediatric hydrocephalus: A systematic literature review and meta-analysis. Childs Nerv. Syst. 2019, 35, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.A.; McAllister, J.P.; Walker, M.L.; Kranz, D.A.; Bergsneider, M.; Del Bigio, M.R.; Fleming, L.; Frim, D.M.; Gwinn, K.; Kes-tle, J.R.; et al. Priorities for hydrocephalus research: Report from a National Institutes of Health-sponsored workshop. J. Neurosurg. 2007, 107 (Suppl. S5), 345–357. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, D.D.; Kestle, J. Ventricular shunting for hydrocephalus in children: Patients, procedures, surgeons and institu-tions in English Canada, 1989-2001. Eur. J. Pediatr. Surg. 2002, 12 (Suppl. S1), S6–S11. [Google Scholar] [CrossRef] [PubMed]
- Tomei, K.L. The Evolution of Cerebrospinal Fluid Shunts: Advances in Technology and Technique. Pediatr. Neurosurg. 2017, 52, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Pople, I.K. Hydrocephalus and shunts: What the neurologist should know. J. Neurol. Neurosurg. Psychiatry 2002, 73 (Suppl. S1), i17–i22. [Google Scholar] [PubMed]
- Faulhauer, K.; Schmitz, P. Overdrainage phenomena in shunt treated hydrocephalus. Acta Neurochir. 1978, 45, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Rekate, H.L. Shunt-related headaches: The slit ventricle syndromes. Child Nerv. Syst. 2008, 24, 423–430. [Google Scholar] [CrossRef]
- Pudenz, R.H.; Foltz, E.L. Hydrocephalus: Overdrainage by ventricular shunts. A review and recommendations. Surg. Neurol. 1991, 35, 200–212. [Google Scholar] [CrossRef]
- Martínez-Lage, J.F.; Vilar, A.R.-E.; Pérez-Espejo, M.A.; Almagro, M.-J.; Pedro, J.R.D.S.; Murcia, M.F. Shunt-related craniocerebral disproportion: Treatment with cranial vault expanding procedures. Neurosurg. Rev. 2006, 29, 229–235. [Google Scholar] [CrossRef]
- Sinha, A.; Sharma, A.; Gupta, C. Pediatric hydrocephalus: Does the shunt device pressure selection affect the outcome? J. Indian Assoc. Pediatr. Surg. 2012, 17, 54–57. [Google Scholar] [CrossRef]
- Kondageski, C.; Thompson, D.; Reynolds, M.; Hayward, R.D. Experience with the Strata valve in the management of shunt overdrainage. J. Neurosurg. Pediatr. 2007, 106, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, A.V.; Riva-Cambrin, J.; Butler, J.; Browd, S.R.; Drake, J.M.; Holubkov, R.; Kestle, J.R.; Limbrick, D.D.; Simon, T.D.; Tamber, M.S.; et al. Outcomes of CSF shunting in children: Comparison of Hydrocephalus Clinical Research Network cohort with historical controls: Clinical article. J. Neurosurg. Pediatr. 2013, 12, 334–338. [Google Scholar] [CrossRef]
- Pollack, I.F.; Albright, A.L.; Adelson, P.D. A randomized, controlled study of a programmable shunt valve versus a conven-tional valve for patients with hydrocephalus. Hakim-Medos Investigator Group. Neurosurgery 1999, 45, 1399–1408, discussion 1408-1311. [Google Scholar] [CrossRef]
- Bauer, D.F.; Baird, L.C.; Flannery, A.M.; Klimo, P.; Tamber, M.S.; Nikas, D.C.; Mazzola, C.A.; Rehring, P. In Reply: Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on the Treatment of Pediatric Hydrocepha-lus: Update of the 2014 Guidelines. Neurosurgery 2021, 89, E76–E77. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y. Withdrawal of shunt systems—Clinical use of the programmable shunt system and its effect on hydrocephalus in children. Child Nerv. Syst. 2001, 17, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Kushnirsky, M.; Feun, L.G.; Gultekin, S.H.; de la Fuente, M.I. Prolonged Complete Response With Combined Dabrafenib and Trametinib After BRAF Inhibitor Failure in BRAF-Mutant Glioblastoma. JCO Precis. Oncol. 2020, 2020, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Nobre, L.; Zapotocky, M.; Ramaswamy, V.; Ryall, S.; Bennett, J.; Alderete, D.; Guill, J.B.; Baroni, L.; Bartels, U.; Bavle, A.; et al. Outcomes of BRAF V600E Pediatric Gliomas Treated With Targeted BRAF Inhibition. JCO Precis. Oncol. 2020, 2020, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Toma, A.K.; Tarnaris, A.; Grieve, J.P.; Watkins, L.D.; Kitchen, N.D. Adjustable shunt valve-induced magnetic resonance imag-ing artifact: A comparative study. J. Neurosurg. 2010, 113, 74–78. [Google Scholar] [CrossRef]
- Zabramski, J.M.; Debbins, J.; Preul, M.C.; McCusker, D.J. 3T magnetic resonance imaging testing of externally programmable shunt valves. Surg. Neurol. Int. 2012, 3, 81. [Google Scholar] [CrossRef] [Green Version]
- INTEGRA—Certas Plus Programmable Valves. Available online: https://www.integralife.com/file/general/1549983654.pdf (accessed on 28 May 2021).
- MIETHKE proGAV® 2.0. Available online: https://www.bbraun.com/en/products/b0/miethke-progav-20.html (accessed on 28 May 2021).
- Strata NSC Adjustable Pressure Valve—Magenetic Field Influences. Available online: https://www.medtronic.com/us-en/healthcare-professionals/products/neurological/shunts/strata-nsc-adjustable-pressure-valve/magnetic-field-influences.html (accessed on 28 May 2021).
- Uchida, D.; Amano, Y.; Nakatogawa, H.; Masui, T.; Ando, N.; Nakayama, T.; Sato, H.; Sameshima, T.; Tanaka, T. Setting pressure can change the size and shape of MRI artifacts caused by adjustable shunt valves: A study of the 4 newest models. J. Neurosurg. 2019, 130, 1260–1267. [Google Scholar] [CrossRef] [Green Version]
- Singleton, R.H.; Kellermier, H.; Lunsford, L.D. Radiation-induced meningioma concealed by shunt valve artifact: Case report. Neurosurgery 2008, 62, E743–E744. [Google Scholar] [CrossRef] [PubMed]
- Schwarm, F.P.; Nagl, J.; Bender, M.; Stein, M.; Giese, K.; Hahn, A.; Uhl, E.; Kolodziej, M.A. Programmable valve breakage in shunt systems of children with posthemorrhagic hydrocephalus after minor head trauma—A case series. Child Nerv. Syst. 2020, 36, 2027–2031. [Google Scholar] [CrossRef] [PubMed]
- Muir, R.; Wang, S.; Warf, B.C. Global surgery for pediatric hydrocephalus in the developing world: A review of the history, challenges, and future directions. Neurosurg. Focus 2016, 41, E11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, A.V.; Schiff, S.J.; Mbabazi-Kabachelor, E.; Mugamba, J.; Ssenyonga, P.; Donnelly, R.; Levenbach, J.; Monga, V.; Peterson, M.; Macdonald, M.; et al. Endoscopic Treatment versus Shunting for Infant Hydrocephalus in Uganda. N. Engl. J. Med. 2017, 377, 2456–2464. [Google Scholar] [CrossRef] [PubMed]
- The ISPN Guide to Pediatric Neurosurgery—Medtronic PS Medical CSF Flow Control Valves. Available online: https://www.ispn.guide/hydrocephalus-and-other-anomalies-of-csf-circulation-in-children/the-ispn-shunt-guide/medtronic-ps-medical-csf-flow-control-valves/ (accessed on 28 May 2021).
- Medtronic Product Catalog—CSF Management, Critical Care, and Cranial Repair. Available online: http://www.medtronic.me/content/dam/medtronic-com/products/neurological/documents/catalog_csfmgt_criticalcare_cranialrepair_neuroendoscopy_uc201709479EN.pdf (accessed on 28 May 2021).
- INTEGRA—Hakim Programmable Valves. Available online: https://www.integralife.com/file/general/1542301599.pdf (accessed on 28 May 2021).
- Sophysa Hydrocephalus Catalog 1st Edition. Available online: https://www.promedics.de/assets/sophysa_hydrocephalusprodukte_2014.pdf (accessed on 28 May 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medtronic PS Medical® Strata® | Codman Certas Plus | MIETHKE proGAV® 2.0 | Codman Hakim | Sophysa Polaris | |
|---|---|---|---|---|---|
| Pressure range (mmH2O) | 15–220 | 25–400 | 0–200 | 30–200 | 30–200 |
| Number of settings | 5 | 8 | 20 | 18 | 5 |
| ‘Virtual off’ function | No | Yes | No | No | No |
| MRI-safe | Yes | Yes | Yes | Yes | Yes |
| MRI-resistant | No | Yes, up to 3 Tesla | Yes, up to 3 Tesla | No | No |
| MRI artefacts | Yes, worse at higher settings | Yes, worse at higher settings | Yes, worse at lower settings | Yes, based on in vitro findings | Yes, worse at higher settings |
| Verification and adjustment of settings | Portable, handheld adjuster tool | Portable, handheld adjuster tool | Portable, handheld adjuster tool | Requires X-ray verification | Portable, handheld adjuster tool |
| Availability in Singapore | Yes | Yes | Yes | Yes | No |
| Availability in small sizes | Yes | Yes, but not available in Singapore | Yes | Microvalve shunt available by manufacturer, but not available in Singapore | No |
| Before 2016 | From 2016 Onwards | p-Value | |
|---|---|---|---|
| Mean number of adjustments per PSV | 0.8 SD ± 0.9 | 2.1 SD ± 1.7 | p = 0.031 |
| Comparison between Subgroups of PSV Patients | Mean Number of Adjustments per PSV | p-Value |
| Revision shunts versus index shunts | 2.2; SD ± 1.9 1.7; SD ± 1.6 | p = 0.488 |
| Tumor-related versus other etiologies | 2.3; SD ± 1.6 | p = 0.107 |
| 1.1; SD ± 1.5 | ||
| Previous CSF over-drainage shunts versus all other shunt revisions | 3.7; SD ± 2.1 | p = 0.231 |
| 1.7; SD ± 1.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tey, M.L.; Ng, L.P.; Low, D.C.Y.; Seow, W.T.; Low, S.Y.Y. Programmable Shunt Valves for Pediatric Hydrocephalus: 22-Year Experience from a Singapore Children’s Hospital. Brain Sci. 2021, 11, 1548. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111548
Tey ML, Ng LP, Low DCY, Seow WT, Low SYY. Programmable Shunt Valves for Pediatric Hydrocephalus: 22-Year Experience from a Singapore Children’s Hospital. Brain Sciences. 2021; 11(11):1548. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111548
Chicago/Turabian StyleTey, Min Li, Lee Ping Ng, David C. Y. Low, Wan Tew Seow, and Sharon Y. Y. Low. 2021. "Programmable Shunt Valves for Pediatric Hydrocephalus: 22-Year Experience from a Singapore Children’s Hospital" Brain Sciences 11, no. 11: 1548. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111548