
Key Challenges and Future Directions When Running Auditory Brainstem Response (ABR) Research Protocols with Newborns: A Music and Language EEG Feasibility Study

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. The Study Design
2.3. The Feasibility Analysis
3. Results
3.1. Evaluation of Recruitment (Objective 1)
3.1.1. Obstacles to Recruitment
3.1.2. Relevance of the Intervention to the Intended Population
3.2. Evaluation of Data Collection and Outcome Measures (Objective 2)
3.3. Evaluation of Acceptability and Suitability of Intervention and Study Procedures (Objective 3)
3.4. Evaluation of Resources and Ability to Manage and Implement the Study and Intervention (Objective 4)
3.5. Preliminary Evaluation of Participant Responses to Intervention (Objective 5)
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Objectives and Guiding Questions for a Feasibility Study
- How many potential eligible members of the targeted population are accessible in the local community?
- What are the recruitment rates?
- How many participants enter the study at a time?
- How long does it take to recruit enough participants into the study?
- What are the refusal rates for participation?
- How feasible and suitable are eligibility criteria?
- Are criteria clear and sufficient or too inclusive or restrictive?
- What are the obstacles to recruitment?
- Are colleagues and local organizations willing to assist with recruitment?
- What are the reasons for refusal or ineligibility?
- How relevant is the intervention to the intended population?
- Do study participants show evidence of need for the intervention?
- Are the characteristics of the study participants consistent with the range of expected characteristics as informed by the research literature?
- How feasible and suitable are the data collection procedures?
- Do participants understand the questions and other data collection procedures?
- Do they respond with missing or unusable data?
- How feasible and suitable is the amount of data collection?
- Do the participants have the capacity to complete the data collection procedures?
- Does the overall data collection plan involve a reasonable amount of time or does it create a burden for the participants?
- Do the measures appear to be performing in a consistent way with the intended population as compared to measurement information available in the research literature?
- Are internal consistency indicators of measures with the recruited sample congruent with expectations based on prior studies reported in the research literature?
- Do planned outcome measures appear to be sensitive to the effects of the intervention?
- Does a suitable outcome measure need to be developed?
- What are the retention and follow-up rates as the participants move through the study and intervention?
- What are the adherence rates to study procedures, intervention attendance, and engagement?
- Does the intervention fit with the daily life activities of study participants?
- Do the participants have enough time and capacity to complete the intervention?
- Does the intervention involve a reasonable amount of time, or does it create a burden for the participants?
- To what extent is the intervention acceptable and appealing to participants?
- If appropriate, how many participants agree to be randomized to group?
- What is the level of safety of the procedures in the intervention?
- Are there any unexpected adverse events?
- Does the research team have the administrative capacity, expertise, skills, space and time to conduct the study and intervention?
- Can we conduct the study procedures and intervention in an ethical manner?
- To what extent does staff comply with the approved human participants’ protocol?
- How effectively are adverse events during implementation identified, documented, and reported?
- Can the study and intervention be conducted within the designated budget?
- Is the technology and equipment sufficient to conduct the study and intervention, including collection, management, and analysis of data?
- Is equipment available when needed?
- What is involved in training personal and/or participants to use the equipment?
- Are we able to manage data entry and analysis efficiently and effectively?
- Does examination of quantitative data suggest that the intervention is likely to be successful?
- Does examination of the data at the participant level suggest that changes in key outcome variables occurred?
- Are the changes of the outcome variable(s) in the expected direction?
- Do the estimates of effects suggest that the intervention has promise?
- Do participants or relevant others provide qualitative feedback that may be indicative of the likelihood that the intervention will be successful?
- If the quantitative and/or qualitative data suggest that the intervention is not promising:
- Are the data collection procedures and outcome measures appropriate for the population and study?
- Are the outcome measures and intervention theoretically aligned?
- Is there evidence that the intervention does not produce change in the desired outcomes?
- Is there evidence that the intervention was not implemented in the intended manner?
- Have too many adaptations been made in the intervention process to adequately assess the participants’ responses to the intervention?
- Are the findings congruent with the proposed theoretical model for the intervention?
References
- Wang, S.; Agius, M. The neuroscience of music; a review and summary. Psychiatr. Danub. 2018, 30, 588–594. [Google Scholar]
- Jäncke, L. Music, memory and emotion. J. Biol. 2008, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Sihvonen, A.J.; Särkämö, T.; Leo, V.; Tervaniemi, M.; Altenmüller, E.; Soinila, S. Music-based interventions in neurological rehabilitation. Lancet Neurol. 2017, 16, 648–660. [Google Scholar] [CrossRef] [Green Version]
- Thaut, M.H. The future of music in therapy and medicine. Ann. N. Y. Acad. Sci. 2005, 1060, 303–308. [Google Scholar] [CrossRef]
- Chanda, M.L.; Levitin, D.J. The neurochemistry of music. Trends Cogn. Sci. 2013, 17, 179–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zatorre, R.J.; Salimpoor, V.N. From perception to pleasure: Music and its neural substrates. Proc. Natl. Acad. Sci. USA 2013, 110 (Suppl. 2), 10430–10437. [Google Scholar] [CrossRef] [Green Version]
- Warren, J. How does the brain process music? Clin. Med. 2008, 8, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Shanyinde, M.; Pickering, R.M.; Weatherall, M. Questions asked and answered in pilot and feasibility randomized controlled trials. BMC Med Res. Methodol. 2011, 11, 117. [Google Scholar] [CrossRef] [Green Version]
- Tickle-Degnen, L. Nuts and bolts of conducting feasibility studies. Am. J. Occup. Ther. 2013, 67, 171–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cope, D.G. Conducting pilot and feasibility studies. Oncol. Nurs. Forum 2015, 42, 196–197. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N. Introducing a new intervention: An overview of research phases and common challenges. Am. J. Occup. Ther. 2013, 67, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health Research. NIHR Evaluation, Trials and Studies Coordination Centre: Glossary. 2012. Available online: http://www.nets.nihr.ac.uk/glossary?result_1655_result_page=F (accessed on 19 November 2021).
- Orsmond, G.I.; Cohn, E.S. The Distinctive Features of a Feasibility Study. OTJR Occup. Particip. Health 2015, 35, 169–177. [Google Scholar] [CrossRef]
- Cartocci, G.; Attanasio, G.; Fattapposta, F.; Locuratolo, N.; Mannarelli, D.; Filipo, R. An electrophysiological approach to tinnitus interpretation. Int. Tinnitus J. 2012, 17, 152–157. [Google Scholar] [CrossRef]
- Grose, J.H.; Buss, E.; Hall, J.W., 3rd. Loud Music Exposure and Cochlear Synaptopathy in Young Adults: Isolated Auditory Brainstem Response Effects but No Perceptual Consequences. Trends Hear. 2017, 21, 2331216517737417. [Google Scholar] [CrossRef] [PubMed]
- Skoe, E.; Kraus, N. Auditory brain stem response to complex sounds: A tutorial. Ear Hear. 2010, 31, 302–324. [Google Scholar] [CrossRef] [Green Version]
- Cianfrone, F.; Mammarella, F.; Ralli, M.; Evetovic, V.; Pianura, C.M.; Bellocchi, G. Universal newborn hearing screening using A-TEOAE and A-ABR: The experience of a large public hospital. J. Neonatal Perinat. Med. 2018, 11, 87–92. [Google Scholar] [CrossRef]
- Mario, C.; Sofia, H.; Wafaa, S.D. Sensitivity of ABR based newborn screening with the MB11 BERAphone®. Int. J. Pediatric Otorhinolaryngol. 2014, 7, 756–761. [Google Scholar] [CrossRef]
- Ramkumar, V.; Hall, J.W.; Nagarajan, R.; Shankarnarayan, V.C.; Kumaravelu, S. Tele-ABR using a satellite connection in a mobile van for newborn hearing testing. J. Telemed. Telecare 2013, 19, 233–237. [Google Scholar] [CrossRef]
- Croom, A.M. Music practice and participation for psychological well-being: A review of how music influences positive emotion, engagement, relationships, meaning, and accomplishment. Musicae Sci. 2015, 19, 44–64. [Google Scholar] [CrossRef] [Green Version]
- Welch, G.F.; Biasutti, M.; MacRitchie, J.; McPherson, G.E.; Himonides, E. The Impact of Music on Human Development and Well-Being. Front. Psychol. 2020, 11, 1246. [Google Scholar] [CrossRef]
- Hays, T.; Bright, R.; Minichiello, V. The Contribution of Music to Positive Aging: A Review. J. Aging Identity 2002, 7, 165–175. [Google Scholar] [CrossRef]
- Papatzikis, E. The educational neuroscience perspective of ABR and lullabies: Setting up an infants brain development study. Int. J. Cross-Discip. Subj. Educ. 2017, 8, 3179–3185. [Google Scholar] [CrossRef]
- Papatzikis, E. An Infant’s Question on COVID-19 and Music: Should I Attend My Online Classes? Front. Psychol. 2021. [Google Scholar] [CrossRef]
- Lordier, L.; Loukas, S.; Grouiller, F.; Vollenweider, A.; Vasung, L.; Meskaldij, D.E.; Lejeune, F.; Pittet, M.P.; Borradori-Tolsa, C.; Lazeyras, F.; et al. Music processing in preterm and full-term newborns: A psychophysiological interaction (PPI) approach in neonatal fMRI. Neuroimage 2019, 15, 857–864. [Google Scholar] [CrossRef]
- Haslbeck, F.B.; Bucher, H.U.; Bassler, D.; Hagmann, C. Creative music therapy to promote brain structure, function, and neurobehavioral outcomes in preterm infants: A randomized controlled pilot trial protocol. Pilot Feasibility Stud. 2017, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tervaniemi, M.; Putkinen, V.; Nie, P.; Wang, C.; Du, B.; Lu, J.; Li Shuting Cowley BUTammi, T.; Tao, S. Improved Auditory Function Caused by Music Versus Foreign Language Training at School Age: Is There a Difference? Cereb. Cortex 2021, 1–13. [Google Scholar] [CrossRef]
- Lordier, L.; Meskaldji, D.E.; Grouiller, F.; Pittet, M.P.; Vollenweider, A.; Vasung, L.; Borradori-Tolsa, C.; Lazeyras, F.; Grandjean, D.; Ville, D.V.D.; et al. Music in premature infants enhances high-level cognitive brain networks. Proc. Natl. Acad. Sci. USA 2019, 116, 12103–12108. [Google Scholar] [CrossRef] [Green Version]
- Anderson, D.E.; Patel, A.D. Infants born preterm, stress, and neurodevelopment in the neonatal intensive care unit: Might music have an impact? Dev. Med. Child Neurol. 2018, 60, 256–266. [Google Scholar] [CrossRef]
- Cannam, C.; Landone, C.; Sandler, M. Sonic visualiser: An open source application for viewing, analysing, and annotating music audio files. In Proceedings of the 18th ACM international conference on Multimedia, Firenze, Italy, 25–29 October 2010; pp. 1467–1468. [Google Scholar] [CrossRef]
- Feirn, R.; Lightfoot, G.; Meredith, R.; Minchom, S.; Parker, G.; Brennan, S.; Booth, R. Guidelines for the Early Audiological Assessment and Management of Babies Referred from the Newborn Hearing Screening Programme, Version 3.1; Stevens, J., Sutton, G., Sally, W., Eds.; NHSP Group, British Society of Audiology: Seafield, UK, 2013; Available online: https://www.thebsa.org.uk/wp-content/uploads/2014/08/NHSP_NeonateAssess_2014.pdf (accessed on 19 November 2021).
- Kraus, N.L.; White-Schwoch, T. Auditory brainstem development: More than meets the ear. Heart J. 2015, 68, 30–32. [Google Scholar] [CrossRef]
- Dubai Healthcare Authority. Annual Health Statistic Book—Dubai, 2019; Data Analysis, Research and Studies Department—Strategy and Corporate Development Sector; 2019. Available online: https://www.dha.gov.ae/DHAOpenData/Annual%20Statistical%20Books/DHADoc404326583-05-11-2020.pdf (accessed on 19 November 2021).
- Papatzikis, E.; Svec, C.; Tsakmakidou, N. Studying Neural Correlates of Music Features in the Early Years Education and Development Process: A Preliminary Understanding based on a Taxonomical Classification and Logistic Regression Analysis. In Proceedings of the Conference Abstract: 4th International Conference on Educational Neuroscience, Abu Dhabi, United Arab Emirates, 10–11 March 2019. [Google Scholar] [CrossRef]
- Chorna, O.; Filippa, M.; Sa De Almeida, J.; Lordier, L.; Monaci, M.G.; Hüppi, P.; Grandjean, D.; Guzzetta, A. Neuroprocessing Mechanisms of Music during Fetal and Neonatal Development: A Role in Neuroplasticity and Neurodevelopment. Neural Plast. 2019. [Google Scholar] [CrossRef] [Green Version]
- Partanen, E.; Kujala, T.; Tervaniemi, M.; Huotilainen, M. Prenatal music exposure induces long-term neural effects. PLoS ONE 2013, 8, e78946. [Google Scholar] [CrossRef] [Green Version]
- James, W. Development of the ear and hearing. J. Perinatol. 2000, 20. [Google Scholar] [CrossRef] [Green Version]
- Graven, S.N.; Browne, J.V. Auditory development in the fetus and infant. Newborn Infant Nurs. Rev. 2008, 8, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Intartaglia, B.; White-Schwoch, T.; Kraus, N.; Schön, D. Music training enhances the automatic neural processing of foreign speech sounds. Sci. Rep. Nat. Publ. Group 2017, 7. [Google Scholar] [CrossRef]
- Baby-Friendly USA. Ten Steps Success. Breastfeed. 2012. Available online: http://www.babyfriendlyusa.org/about-us/baby-friendly-hospital-initiative/the-ten-steps (accessed on 19 November 2021).
- Taha, Z.; Ali Hassan, A.; Wikkeling-Scott, L.; Eltoum, R.; Papandreou, D. Assessment of Hospital Rooming-in Practice in Abu Dhabi, United Arab Emirates: A Cross-Sectional Multi-Center Study. Nutrients 2020, 12, 2318. [Google Scholar] [CrossRef]
- Smith, J.T.; Wolfe, J. Sound Advice for ABR Analysis. Heart J. 2014, 67, 14–18. [Google Scholar] [CrossRef]
- Picton, T.W. Human Auditory Evoked Potentials; Plural Publishing: San Diego, CA, USA, 2010; ISBN 13: 978-1-59756-362-8. [Google Scholar]
- Beiser, M.; Himelfarb, M.Z.; Gold, S.; Shanon, E. Maturation of auditory brainstem potentials in neonates and infants. Int. J. Pediatric Otorhinolaryngol. 1985, 9, 69–76. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total Amount of Pregnancies per Year | 4000 |
|---|---|
| Per month | 300–350 |
| Per week | 70–80 |
| Per day | 10–11 |
| Left Ear | |||||||
|---|---|---|---|---|---|---|---|
| Peaks | I | III | V | III–I | V–III | V–I | |
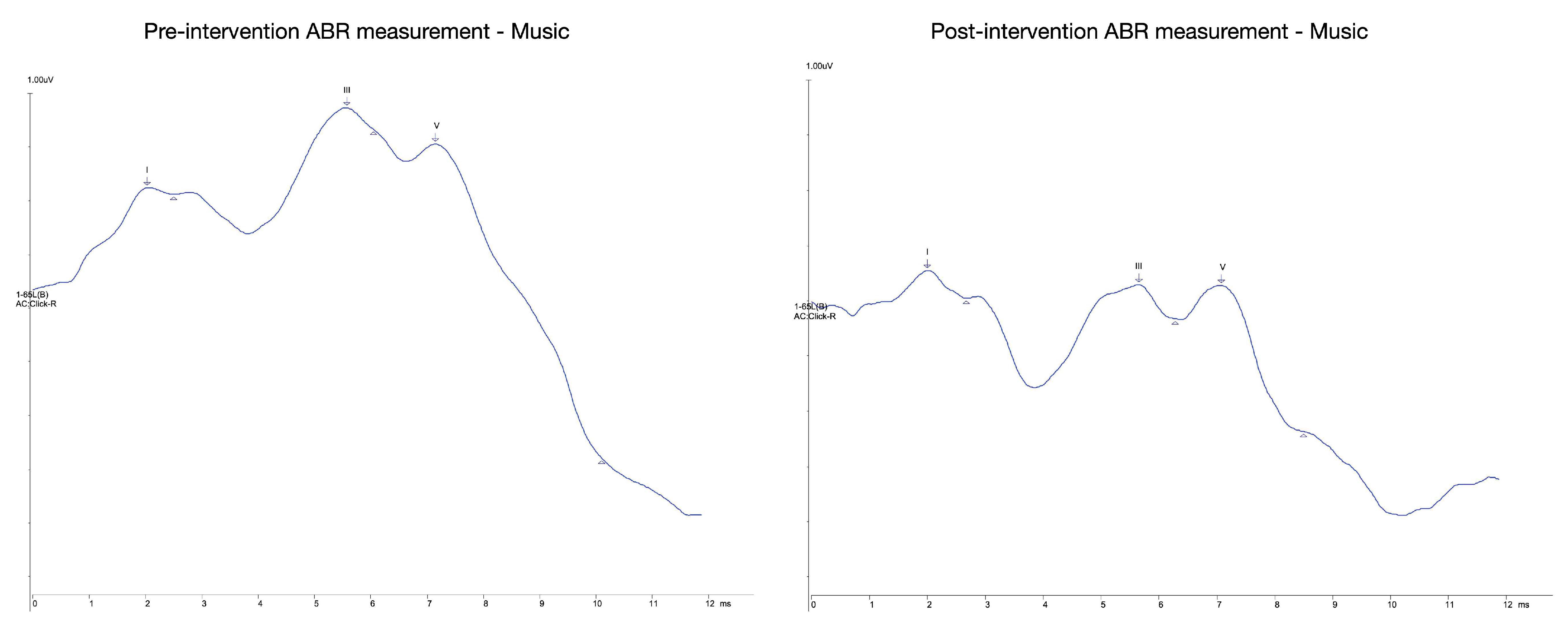
| Music Pre | Latency (ms) | 2.05 | 5.6 | 7.17 | 3.55 | 1.58 | 5.13 |
| Amplitude (uV) | 0.01 | 0.04 | 0.58 | 3.46 AR | 13.73 AR | 47.51 AR | |
| Music Post | Latency (ms) | 2.05 | 5.2 | 7.08 | 9.58 | −4.83 | 5.03 |
| Amplitude (uV) | 0.1 | 0.6 | 0.18 | 1.88 AR | |||
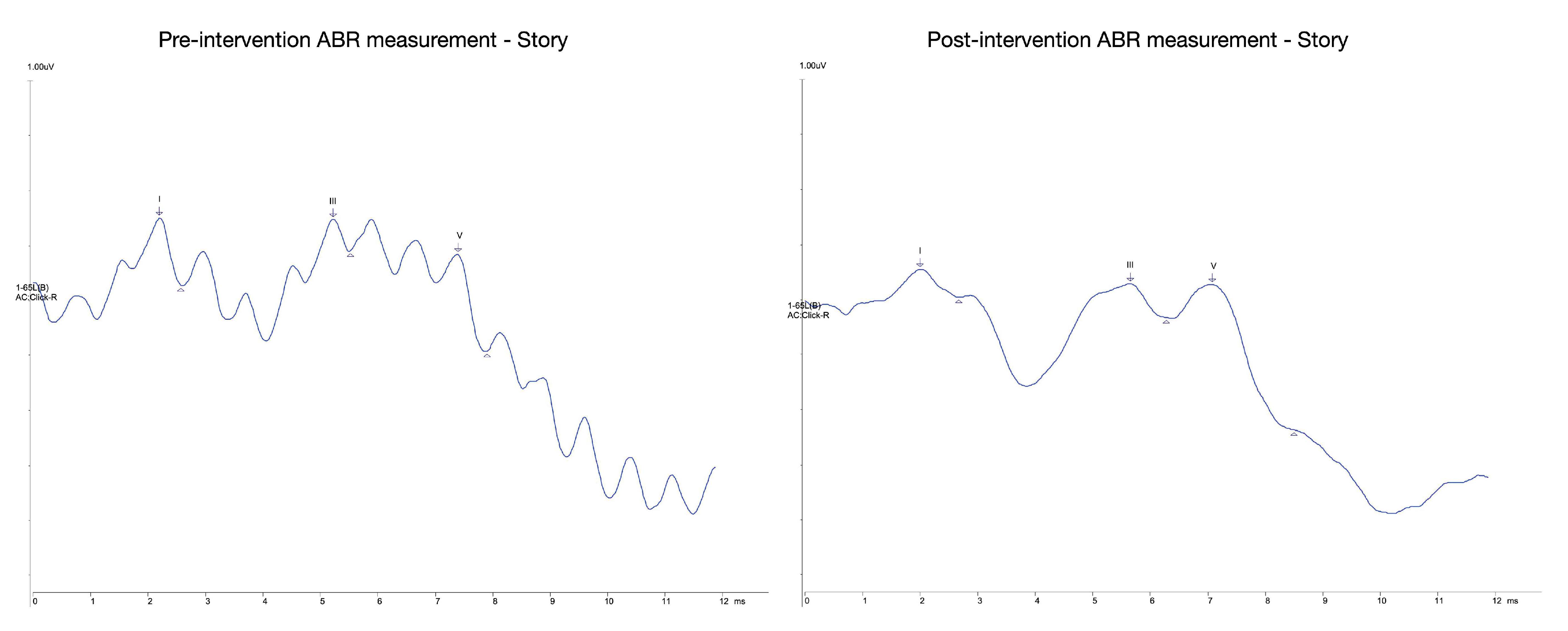
| Story Pre | Latency (ms) | 2.23 | 5.25 | 7.42 | 3.02 | 2.17 | 5.2 |
| Amplitude (uV) | 0.12 | 0.06 | 0.18 | 0.47 AR | 3.05 AR | 1.44 AR | |
| Story Post | Latency (ms) | 2.02 | 5.67 | 7.1 | 3.65 | 1.42 | 5.07 |
| Amplitude (uV) | 0.05 | 0.06 | 0.26 | 1.24 AR | 4.29 AR | 5.33 AR | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papatzikis, E.; Elhalik, M.; Inocencio, S.A.M.; Agapaki, M.; Selvan, R.N.; Muhammed, F.S.; Haroon, N.A.; Dash, S.K.; Sofologi, M.; Bezoni, A. Key Challenges and Future Directions When Running Auditory Brainstem Response (ABR) Research Protocols with Newborns: A Music and Language EEG Feasibility Study. Brain Sci. 2021, 11, 1562. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121562
Papatzikis E, Elhalik M, Inocencio SAM, Agapaki M, Selvan RN, Muhammed FS, Haroon NA, Dash SK, Sofologi M, Bezoni A. Key Challenges and Future Directions When Running Auditory Brainstem Response (ABR) Research Protocols with Newborns: A Music and Language EEG Feasibility Study. Brain Sciences. 2021; 11(12):1562. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121562
Chicago/Turabian StylePapatzikis, Efthymios, Mahmoud Elhalik, Shannaiah Aubrey Mae Inocencio, Maria Agapaki, Rosari Naveena Selvan, Faseela Shejeed Muhammed, Nazreen Abdulla Haroon, Swarup Kumar Dash, Maria Sofologi, and Antonia Bezoni. 2021. "Key Challenges and Future Directions When Running Auditory Brainstem Response (ABR) Research Protocols with Newborns: A Music and Language EEG Feasibility Study" Brain Sciences 11, no. 12: 1562. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121562