
Two Faces of a Coin? A Systematic Review of Source Monitoring and Its Relationship with Memory in Autism

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
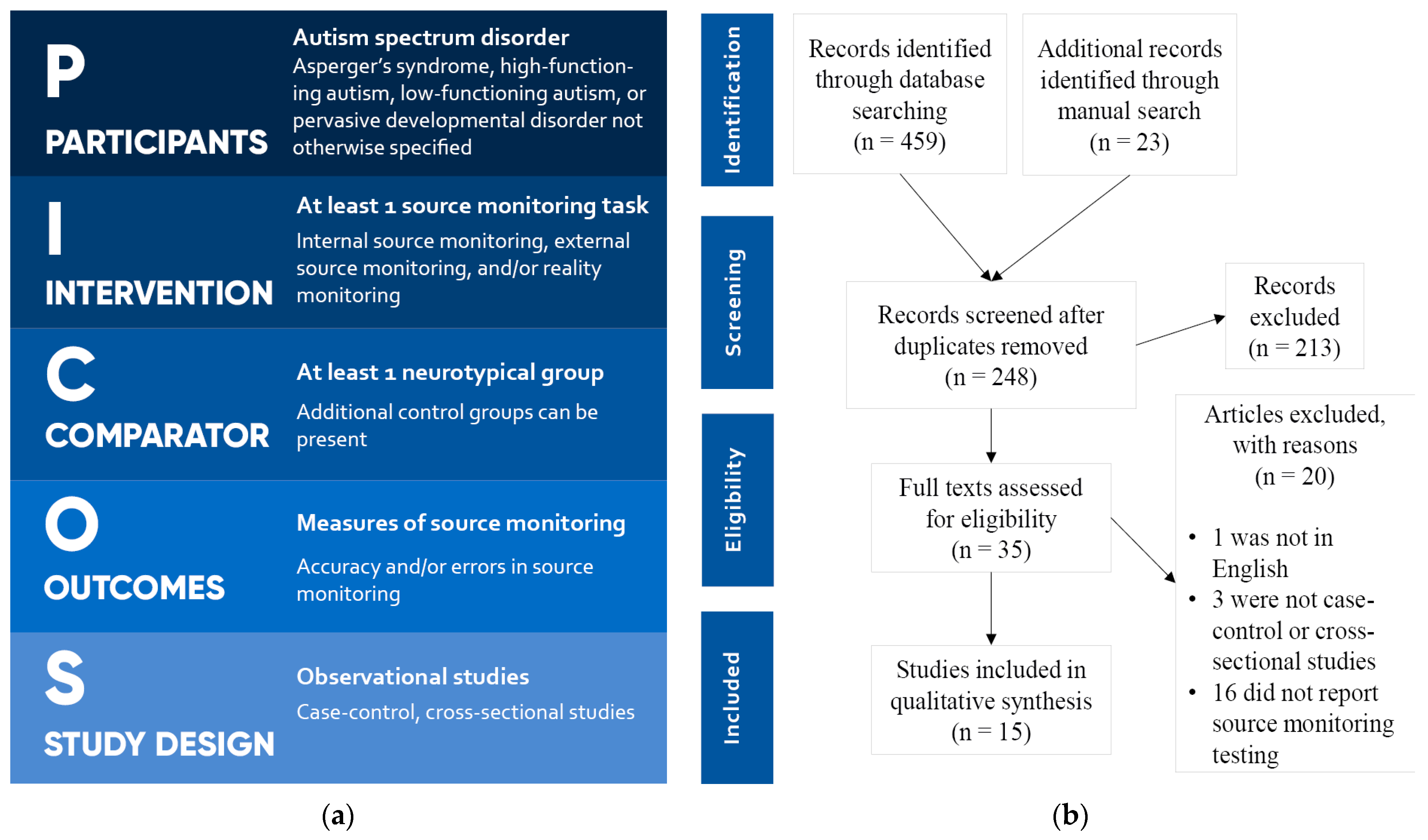
2.1. Search Criteria
2.2. Quality Assessment
2.3. Classification of Task Designs
2.4. Data Extraction and Outcome Measures
3. Results
3.1. Primary Aim—Source Monitoring Scores
3.2. Memory—Old/New Recognition Scores
3.3. Memory—Recall Scores
3.4. Encoding Effects
3.5. Social Cognition
3.6. General Intelligence and Clinical Factors
4. Discussion
4.1. Source Monitoring Performance and Errors
4.2. The Role of Memory in Source Monitoring Tasks
4.3. Encoding Effects
4.4. Social Cognition
4.5. Effects of General Intelligence
4.6. Limitations
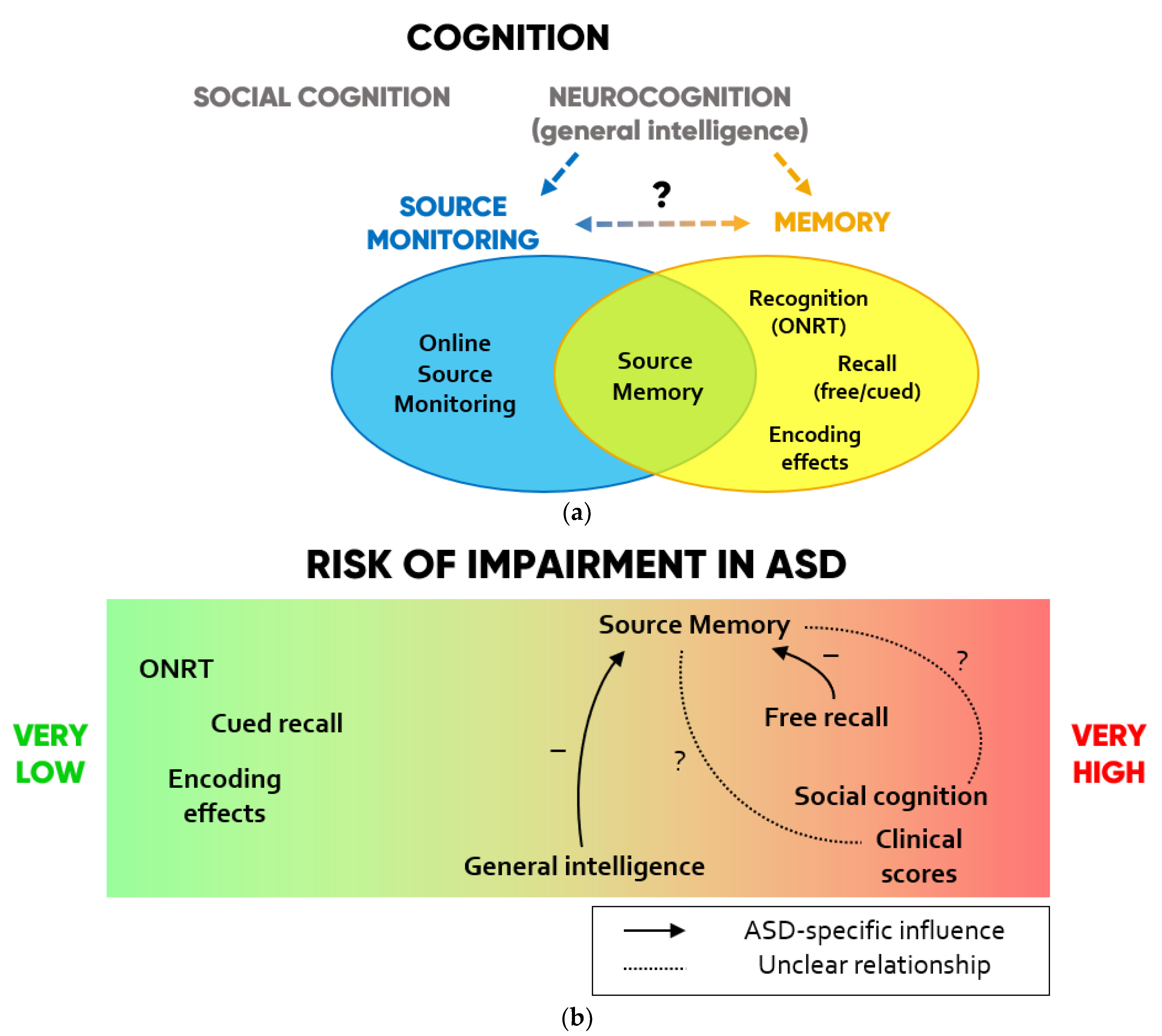
4.7. Toward a Framework for Source Monitoring in Autism
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Study | Selection (★★★★) | Comparability (★★) | Exposure (★★★) | Total Score (9) |
|---|---|---|---|---|
| Farrant et al. (1998) [30] | ★ ★ | ★ ★ | ★ ★ ★ | 7 |
| Russell and Jarrold (1999) [13] | ★ ★ | ★ | ★ ★ ★ | 6 |
| Russell and Hill (2001) [32] | ★ ★ ★ | ★ | ★ ★ ★ | 7 |
| Hill and Russell (2002) [24] | ★ ★ ★ ★ | ★ | ★ ★ ★ | 8 |
| Bowler et al. (2004) [27] | ★ ★ ★ | ★ ★ | ★ ★ ★ | 8 |
| Hala et al. (2005) [26] | ★ ★ ★ | ★ | ★ ★ | 6 |
| O’Shea et al. (2005) [28] | ★ ★ ★ ★ | ★ ★ | ★ ★ ★ | 9 |
| Lind and Bowler (2009) [22] | ★ ★ ★ | ★ ★ | ★ ★ ★ | 8 |
| Williams and Happé (2009) [31] | ★ ★ | ★ ★ ★ | 5 | |
| Zalla et al. (2010) [23] | ★ ★ ★ | ★ ★ | ★ ★ ★ | 8 |
| Maras et al. (2013) [25] | ★ ★ ★ ★ | ★ | ★ ★ ★ | 8 |
| Grainger et al. (2014) [14] | ★ ★ ★ ★ | ★ ★ | ★ ★ ★ | 9 |
| Cooper et al. (2016) [3] | ★ ★ ★ ★ | ★ ★ | ★ ★ ★ | 9 |
| Grainger et al. (2017) [15] | ★ ★ | ★ ★ | ★ ★ ★ | 7 |
| Yamamoto and Masumoto (2018) [29] | ★ ★ ★ ★ | ★ ★ ★ | 7 | |
| Mean values | 7.5 |
| Outcome Measure | Score | Definition |
|---|---|---|
| Source Monitoring | ||
| Errors (SM-E) | External Internal | Incorrectly identified external item sources Incorrectly identified internal item sources |
| Reality internalizing (RMint) | External item sources incorrectly identified as internal | |
| Reality externalizing (RMext) | Internal item sources incorrectly identified as external | |
| Accuracy (SM-A) | Source score | Correctly identified sources/N° old items correctly recognized as old |
| Source proportion | Correctly identified sources/total N° of items presented | |
| Source number | Correctly identified sources | |
| Memory—Old/New Recognition (ONRT) | ||
| Errors (ONRT-E) | False alarm rate (FA) | Proportion of new items incorrectly recognized as old |
| Miss rate (MISS) | Proportion of old items incorrectly recognized as new | |
| FA+MISS | FA errors + MISS errors | |
| Accuracy (ONRT-A) | Hit rate (H) | Proportion of old items correctly recognized as old |
| Recognition number | N° of old items correctly recognized as old | |
| Signal detection (ONRT-SD) | Corrected hit rate | H–FA |
| Recognition performance | z(H)–z(FA) 1 | |
| Item discrimination | 1/2 + [(H − FA)(1 + H − FA)]/[(4H)(1 − FA)] | |
| Memory—Free or cued recall | ||
| Errors (REC-E) | Omission errors | N° of items incorrectly not recalled |
| Commission errors | N° of items incorrectly recalled | |
| Accuracy (REC-A) | Recall number | N° of items correctly recalled |
| Recall proportion | Proportion of items correctly recalled | |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Lombardo, M.V.; Chakrabarti, B.; Bullmore, E.T.; Sadek, S.A.; Pasco, G.; Wheelwright, S.J.; Suckling, J.; Consortium, M.A.; Baron-Cohen, S. Atypical neural self-representation in autism. Brain 2010, 133, 611–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, R.A.; Plaisted-Grant, K.C.; Baron-Cohen, S.; Simons, J.S. Reality monitoring and metamemory in adults with autism spectrum conditions. J. Autism Dev. Disord. 2016, 46, 2186–2198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noel, J.-P.; Cascio, C.J.; Wallace, M.T.; Park, S. The spatial self in schizophrenia and autism spectrum disorder. Schizophr. Res. 2017, 179, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobson, R.P.; Meyer, J.A. Foundations for self and other: A study in autism. Dev. Sci. 2005, 8, 481–491. [Google Scholar] [CrossRef]
- Hobson, R.P. Explaining autism: Ten reasons to focus on the developing self. Autism 2010, 14, 391–407. [Google Scholar] [CrossRef]
- Mitchell, K.J. Definition: Source monitoring. Cortex J. Devoted Study Nerv. Syst. Behav. 2017, 96, 129. [Google Scholar] [CrossRef]
- Johnson, M.K.; Hashtroudi, S.; Lindsay, D.S. Source monitoring. Psychol. Bull. 1993, 114, 3. [Google Scholar] [CrossRef]
- El Haj, M.; Fasotti, L.; Allain, P. Source monitoring in Alzheimer’s disease. Brain Cogn. 2012, 80, 185–191. [Google Scholar] [CrossRef]
- Brookwell, M.; Bentall, R.; Varese, F. Externalizing biases and hallucinations in source-monitoring, self-monitoring and signal detection studies: A meta-analytic review. Psychol. Med. 2013, 43, 2465. [Google Scholar] [CrossRef] [PubMed]
- Boucher, J.; Mayes, A.; Bigham, S. Memory in autistic spectrum disorder. Psychol. Bull. 2012, 138, 458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lind, S.E. Memory and the self in autism: A review and theoretical framework. Autism 2010, 14, 430–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, J.; Jarrold, C. Memory for actions in children with autism: Self versus other. Cogn. Neuropsychiatry 1999, 4, 303–331. [Google Scholar] [CrossRef] [PubMed]
- Grainger, C.; Williams, D.M.; Lind, S.E. Online action monitoring and memory for self-performed actions in autism spectrum disorder. J. Autism Dev. Disord. 2014, 44, 1193–1206. [Google Scholar] [CrossRef]
- Grainger, C.; Williams, D.M.; Lind, S.E. Recognition memory and source memory in autism spectrum disorder: A study of the intention superiority and enactment effects. Autism 2017, 21, 812–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, S.; Franklin, N.; Naka, M.; Yoshimura, H. Higher social intelligence can impair source memory. Journal Exp. Psychol. Learn. Mem. Cogn. 2010, 36, 545–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvares, G.A.; Bebbington, K.; Cleary, D.; Evans, K.; Glasson, E.J.; Maybery, M.T.; Pillar, S.; Uljarević, M.; Varcin, K.; Wray, J. The misnomer of ‘high functioning autism’: Intelligence is an imprecise predictor of functional abilities at diagnosis. Autism 2020, 24, 221–232. [Google Scholar] [CrossRef]
- Uljarević, M.; Baranek, G.; Vivanti, G.; Hedley, D.; Hudry, K.; Lane, A. Heterogeneity of sensory features in autism spectrum disorder: Challenges and perspectives for future research. Autism Res. 2017, 10, 703–710. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.a.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 13 May 2021).
- Lind, S.E.; Bowler, D.M. Recognition memory, self-other source memory, and theory-of-mind in children with autism spectrum disorder. J. Autism Dev. Disord. 2009, 39, 1231–1239. [Google Scholar] [CrossRef] [Green Version]
- Zalla, T.; Daprati, E.; Sav, A.-M.; Chaste, P.; Nico, D.; Leboyer, M. Memory for self-performed actions in individuals with Asperger syndrome. PLoS ONE 2010, 5, e13370. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.L.; Russell, J. Action memory and self-monitoring in children with autism: Self versus other. Infant Child Dev. Int. J. Res. Pract. 2002, 11, 159–170. [Google Scholar] [CrossRef]
- Maras, K.L.; Memon, A.; Lambrechts, A.; Bowler, D.M. Recall of a live and personally experienced eyewitness event by adults with autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 1798–1810. [Google Scholar] [CrossRef] [PubMed]
- Hala, S.; Rasmussen, C.; Henderson, A.M. Three types of source monitoring by children with and without autism: The role of executive function. J. Autism Dev. Disord. 2005, 35, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.M.; Gardiner, J.M.; Berthollier, N. Source memory in adolescents and adults with Asperger’s syndrome. J. Autism Dev. Disord. 2004, 34, 533–542. [Google Scholar] [CrossRef]
- O’Shea, A.G.; Fein, D.A.; Cillessen, A.H.; Klin, A.; Schultz, R.T. Source memory in children with autism spectrum disorders. Dev. Neuropsychol. 2005, 27, 337–360. [Google Scholar] [CrossRef]
- Yamamoto, K.; Masumoto, K. Brief report: Memory for self-performed actions in adults with autism spectrum disorder: Why does memory of self decline in ASD? J. Autism Dev. Disord. 2018, 48, 3216–3222. [Google Scholar] [CrossRef]
- Farrant, A.; Blades, M.; Boucher, J. Source monitoring by children with autism. J. Autism Dev. Disord. 1998, 28, 43–50. [Google Scholar] [CrossRef]
- Williams, D.; Happé, F. Pre-conceptual aspects of self-awareness in autism spectrum disorder: The case of action-monitoring. J. Autism Dev. Disord. 2009, 39, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, J.; Hill, E.L. Action-monitoring and intention reporting in children with autism. J. Child Psychol. Psychiatry 2001, 42, 317–328. [Google Scholar] [CrossRef]
- Baron-Cohen, S. The autistic child’s theory of mind: A case of specific developmental delay. J. Child Psychol. Psychiatry 1989, 30, 285–297. [Google Scholar] [CrossRef] [PubMed]
- Sivaratnam, C.S.; Newman, L.K.; Tonge, B.J.; Rinehart, N.J. Attachment and emotion processing in children with autism spectrum disorders: Neurobiological, neuroendocrine, and neurocognitive considerations. Rev. J. Autism Dev. Disord. 2015, 2, 222–242. [Google Scholar] [CrossRef] [Green Version]
- Bowler, D.M.; Matthews, N.J.; Gardiner, J.M. Asperger’s syndrome and memory: Similarity to autism but not amnesia. Neuropsychologia 1997, 35, 65–70. [Google Scholar] [CrossRef]
- Nelson, B.; Whitford, T.; Lavoie, S.; Sass, L. What are the neurocognitive correlates of basic self-disturbance in schizophrenia?: Integrating phenomenology and neurocognition. Part 1 (Source monitoring deficits). Schizophr. Res. 2014, 152, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Damiani, S.; Fusar-Poli, L.; Brondino, N.; Provenzani, U.; Baldwin, H.; Fusar-Poli, P.; Politi, P. World/self ambivalence: A shared mechanism in different subsets of psychotic experiences? Linking symptoms with resting-state fmri. Psychiatry Res. Neuroimaging 2020, 299, 111068. [Google Scholar] [CrossRef]
- Lombardo, M.V.; Baron-Cohen, S. The role of the self in mindblindness in autism. Conscious. Cogn. 2011, 20, 130–140. [Google Scholar] [CrossRef]
- Lind, S.E.; Williams, D.M.; Nicholson, T.; Grainger, C.; Carruthers, P. The self-reference effect on memory is not diminished in autism: Three studies of incidental and explicit self-referential recognition memory in autistic and neurotypical adults and adolescents. J. Abnorm. Psychol. 2020, 129, 224. [Google Scholar] [CrossRef]
- Freeman, J.E.; Ellis, J.A. The representation of delayed intentions: A prospective subject-performed task? J. Exp. Psychol. Learn. Mem. Cogn. 2003, 29, 976. [Google Scholar] [CrossRef]
- Klin, A.; Jones, W.; Schultz, R.; Volkmar, F.; Cohen, D. Visual fixation patterns during viewing of naturalistic social situations as predictors of social competence in individuals with autism. Arch. Gen. Psychiatry 2002, 59, 809–816. [Google Scholar] [CrossRef] [Green Version]
- Moriuchi, J.M.; Klin, A.; Jones, W. Mechanisms of diminished attention to eyes in autism. Am. J. Psychiatry 2017, 174, 26–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suri, K.; Lewis, M.; Minar, N.; Willson, E.; Ace, J. Face Memory Deficits in Children and Adolescents with Autism Spectrum Disorder. J. Psychopathol. Behav. Assess. 2021, 43, 1–11. [Google Scholar] [CrossRef]
- Provenzani, U.; Fusar-Poli, L.; Brondino, N.; Damiani, S.; Vercesi, M.; Meyer, N.; Rocchetti, M.; Politi, P. What are we targeting when we treat autism spectrum disorder? A systematic review of 406 clinical trials. Autism 2020, 24, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, L.; Brondino, N.; Rocchetti, M.; Panisi, C.; Provenzani, U.; Damiani, S.; Politi, P. Diagnosing ASD in adults without ID: Accuracy of the ADOS-2 and the ADI-R. J. Autism Dev. Disord. 2017, 47, 3370–3379. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T. Pathologies of intersubjectivity in autism and schizophrenia. J. Conscious. Stud. 2015, 22, 191–214. [Google Scholar] [CrossRef] [Green Version]


| Table 2009 | Task Description | Studies |
|---|---|---|
| Reality Monitoring | ||
| Card naming | Picture cards are presented with the instruction to be named by either the participant or the experimenter. Participants must then recall who named each item. | Lind and Bowler (2009) [22] |
| Observe or perform | Actions are shown in a video clip for the participant to either observe or perform the action simultaneously. Participants must then recall whether they had observed or performed them. | Grainger et al. (2014) [14]; Zalla et al. (2010) [23] |
| Object pairs | Pairs of objects are presented for the participant or the experimenter to perform a certain action. Participants must then recall who performed each action. | Hill and Russell (2002) [24] |
| First aid scenario | The participant and the experimenter perform some actions in a first aid scenario. Participants must then recall who performed each action. | Maras et al. (2013) [25] |
| Internal Source Monitoring | ||
| Say or think | Words are presented for the participant to either think or say them out loud. Participants must then recall whether they had thought or said them. | Hala et al. (2005) [26]; |
| Plan or perform | Action phrases are presented for the participant to either read out loud, plan to perform later, or perform now. Participants must then recall whether they had read, planned, or performed them. | Grainger et al. (2017) [15] |
| Word thinking | Words are presented for participants to either think of a word of similar meaning, rhyming, or longer, or to think of a related action. Participants must then recall what they had done with each word. | Bowler et al. (2004) [27] |
| External Source Monitoring | ||
| Word presentation | Words are presented either at the top or bottom of a screen, or in a male or female voice. Participants must then recall how they were presented. | Bowler et al. (2004) [27] |
| Human vs. computer players | Picture cards are placed in cardholders of different colors. The participant, experimenter or computer moves the cards to the central board. Participants must then place each card in the original cardholder | Russell and Jarrold 1999 [13] |
| Short stories | Short stories read by different actors are shown to participants on video tape. The tapes are characterized by different details. Participants must then recognize the correct details for each video tape. | O’Shea et al. (2005) [28] |
| Reality and External Source Monitoring | ||
| Listen, observe or perform | Action phrases are presented for the participant to either listen only, to observe the experimenter perform the action, or to perform it. Participants must then recall whether they had listened, observed or performed each action. | Yamamoto and Masumoto (2018) [29] |
| Red and blue blocks | Either the participant and the experimenter, or two experimenters, hold a red and a blue block. Each presented word is said out loud either by the person holding the red or by the one holding the blue block. Participants must then recall who said each word. | Farrant et al. (1998) [30]; Hala et al. (2005) [26] |
| Moving shapes | When the mouse is moved, a target shape moves in accordance on a screen, while additional distractor shapes move randomly over increasing levels of difficulty. Either the participant or the experimenter moves the mouse. Participants must then identify which is the shape controlled by the mouse. Therefore, they must try to correctly attribute the source of movement to: (i) either themselves or the computer (ii) either the experimenter or the computer. | Grainger et al. (2014) [14] Williams and Happé (2009) [31]; Russell and Hill (2001) [32] |
| All Types of Source Monitoring | ||
| Read or imagine | Word pairs are presented to be read by either the participant or the experimenter. Word pairs are either written in full or with the second word being only suggested. Participants must then recall who read each word pair and how were they written. | Cooper et al. (2016) [3] |
| Human vs. doll players | Picture cards are distributed between participant, experimenter, and two dolls, each controlled by either the participant or the experimenter. In turns, each player lays a card for themselves or their doll partner. Participants must then return each card to the original owner. | Russell and Jarrold (1999) [13]; Williams and Happé (2009) [31] |
| Study | Primary Aim (ASD vs. CTRL) | Secondary Aims (ASD vs. CTRL) | Stimulus Modality | SM Type | Social Cog. | Performance (ASD vs. CTRL) | |||
|---|---|---|---|---|---|---|---|---|---|
| SM Scores | ONRT Scores | Recall Scores | Encoding Effects | ||||||
| Farrant et al. (1998) [30] | SM < | P, A | RM | yes | SM-A = | ONRT-A = ONRT-E = | No enactment = | ||
| Russell and Jarrold (1999) [13] | SM < in human vs. doll | SM = in human vs. computer | P, V | all | yes | SM-A < | Enactment < | ||
| SM-A ESM = | Observer > | ||||||||
| Russell and Hill (2001) [32] | SM < | P, V | RM | no | SM-A = | ||||
| Hill and Russell (2002) [24] | SM < | ONRT and recall = | P, V | RM | yes | SM-A = | ONRT-A = | REC-A cued = | |
| RMint < NT, = MLD | |||||||||
| Bowler et al. (2004) [27] | SM free < SM cued = | Enactment = | I, V, A | ISM, ESM | no | SM-A free < | ONRT-SD < | Enactment = | |
| SM-A cued = | |||||||||
| Hala et al. (2005) [26] | RM < but ONRT = | SM < when self is agent (RM, ISM) | P, I, V | all | yes | SM-A < | ONRT-A = ONRT-E = | No enactment = I > P = | |
| O’Shea et al. (2005) [28] | SM < | Source variables recognition ≠ | V | ESM | yes | SM-A < | ONRT-E = | REC-A free < | |
| SM-E = | REC-A cued = | ||||||||
| Lind and Bowler (2009) [22] | SM < but ONRT = | Enactment = | P, A | RM | yes | SM-A < | ONRT-SD = | Enactment = | |
| Williams and Happé (2009) [31] | Self-reference < | Observer > self-reference | P, V | all | yes | SM-A = | Enactment = | ||
| Zalla et al. (2010) [23] | Enactment = | P, V | RM | no | SM-A = | ONRT-SD = | REC-A free = | Enactment < recall | |
| Enactment = SM, ONRT | |||||||||
| Maras et al. (2013) [25] | Enactment < in free SM = in cued SM | SM-E < in free SM, = in cued SM | P, V | RM | yes | RMint = | REC-A = | Enactment = | |
| RMext free < | REC-E free < | ||||||||
| RMext cued = | REC-E cued < | ||||||||
| Grainger et al. (2014) [14] | Action monitoring = | Enactment = | P, V | RM | yes | SM-A = | ONRT-SD = | REC-A free = | Enactment = |
| Cooper et al. (2016) [3] | Enactment < | SM < for self-other sources | P, I, A | all | yes | SM-A< | ONRT-SD = | Enactment = Generation = | |
| Grainger et al. (2017) [15] | Intention superiority < | Action monitoring = | P, I | ISM | no | SM-A = | ONRT-SD = | Enactment = Intention = | |
| Yamamoto and Masumoto (2018) [29] | Self-reference < | P, V, A | RM, ESM | yes | SM-A< | ONRT-A= ONRT-E= | REC-A free< | Enactment= | |
| Study | ASD Type | CTRL | N Subjects | % Males | Age Mean | Intelligence Measure | Intelligence Mean | Clinical Scores | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ASD | CTRL | ASD | CTRL | ASD | CTRL | ASD | CTRL | |||||
| Farrant et al. (1998) [30] | AUT | NT MMR | 15 | 15 15 | 93.3 | 86.7 86.7 | 12.7 | 7.6 12.9 | BPVS (VMA) | 7.8 | 7.7 7.6 | |
| Russell and Jarrold (1999) [13] | BPVS (IQ) | DSM III-R | ||||||||||
| - Task 1 | AS, AUT | NT MLD | 22 | 22 22 | 13.2 | 6.8 11.3 | 85.6 | 85.4 86.6 | ||||
| - Task 2 | AS, AUT | NT | 19 | 19 | 13.8 | 7.3 | 88 | 87.9 | ||||
| MLD | 19 | 11.9 | 87.5 | |||||||||
| Russell and Hill (2001) [32] | AS, AUT | NT MLD | 28 | 28 28 | 75 | 57.1 32.1 | 10.1 | 6.09 10.06 | BPVS (VMA) | 6.1 | 6.1 6 | |
| Hill and Russell (2002) [24] | AUT | NT MLD | 20 | 20 20 | 75 | 60 50 | 9.8 | 6 9.6 | BPVS (VMA) | 5.9 | 5.9 6 | |
| Bowler et al. (2004) [27] | AS AS | NT NT | 16 16 | 16 16 | 93.8 100 | 13.5 34.5 | 13.4 33.4 | BPVS (IQ) WAIS-R (IQ) | 100.8 100.2 | 94.6 97 | ||
| Hala et al. (2005) [26] | AUT | NT | 13 | 13 | 84.6 | 84.6 | 8 | 6 | PPVT (VMA) | 6 | 6 | |
| O’Shea et al. (2005) [28] | AUT, PDD-NOS | NT | 21 | 21 | 81 | 42.9 | 10.9 | 10.6 | WISC-III (IQ) | 94.7 | 101.8 | ADOS |
| Lind and Bowler (2009) [22] | BPVS (VMA) | |||||||||||
| - Task 1 | AS, AUT | NT, ID | 53 | 50 | 84.9 | 70 | 9.3 | 9.09 | 6.7 | 6.5 | ||
| - Task 2 | AS, AUT | NT, ID | 73 | 55 | 82.2 | 67.3 | 10.1 | 8.6 | 6.6 | 6.1 | ||
| Williams and Happé (2009) [31] | WISC-III, BPVS (IQ) | |||||||||||
| - Task 1 | AS, AUT, PDD-NOS | ID | 16 | 16 | 13.4 | 13 | 72 | 69.9 | ||||
| - Task 2 | ASD | ID | 16 | 16 | 12.4 | 12.2 | 73.5 | 67.4 | ||||
| Zalla et al. (2010) [23] | AS | NT | 18 | 18 | 83.3 | 77.8 | 26.2 | 27.7 | WAIS-III (IQ) | 107.4 | 106.7 | ADI-R |
| Maras et al. (2013) [25] | AS, AUT | NT | 18 | 18 | 88.9 | 83.3 | 41.1 | 45.5 | WAIS-R (IQ) | 109.8 | 110.7 | ADOS, AQ |
| Grainger et al. (2014) [14] | AS, AUT | NT | 17 | 17 | 29.1 | 29.4 | WASI (IQ) | 114.5 | 113.6 | |||
| Cooper et al. (2016) [3] | AS, HFA | NT | 24 | 24 | 45.8 | 45.8 | 31.4 | 30.5 | RM-sf (IQ) | 75.4 | 70.8 | AQ |
| Grainger et al. (2017) [15] | AS, AUT | NT | 22 | 20 | 86.4 | 100 | 13.4 | 13.2 | WASI (IQ) | 106.7 | 109.5 | SRS |
| Yamamoto and Masumoto (2018) [29] | ASD | NT | 14 | 16 | 57.1 | 43.8 | 30.5 | 27.9 | WISC-III (IQ) | 103.6 | 106.4 | AQ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damiani, S.; Guiot, C.; Nola, M.; Donadeo, A.; Bassetti, N.; Brondino, N.; Politi, P. Two Faces of a Coin? A Systematic Review of Source Monitoring and Its Relationship with Memory in Autism. Brain Sci. 2021, 11, 640. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050640
Damiani S, Guiot C, Nola M, Donadeo A, Bassetti N, Brondino N, Politi P. Two Faces of a Coin? A Systematic Review of Source Monitoring and Its Relationship with Memory in Autism. Brain Sciences. 2021; 11(5):640. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050640
Chicago/Turabian StyleDamiani, Stefano, Cecilia Guiot, Marta Nola, Alberto Donadeo, Nicola Bassetti, Natascia Brondino, and Pierluigi Politi. 2021. "Two Faces of a Coin? A Systematic Review of Source Monitoring and Its Relationship with Memory in Autism" Brain Sciences 11, no. 5: 640. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050640