
Serotonin Levels and Cognitive Recovery in Patients with Subacute Stroke after Rehabilitation Treatment

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. General Assessment
2.3. Cognitive Assessment
2.4. Rehabilitation Treatment
2.5. Serotonin Analyses
2.6. Statistical Analysis
3. Results
3.1. Participants and Baseline Characteristics
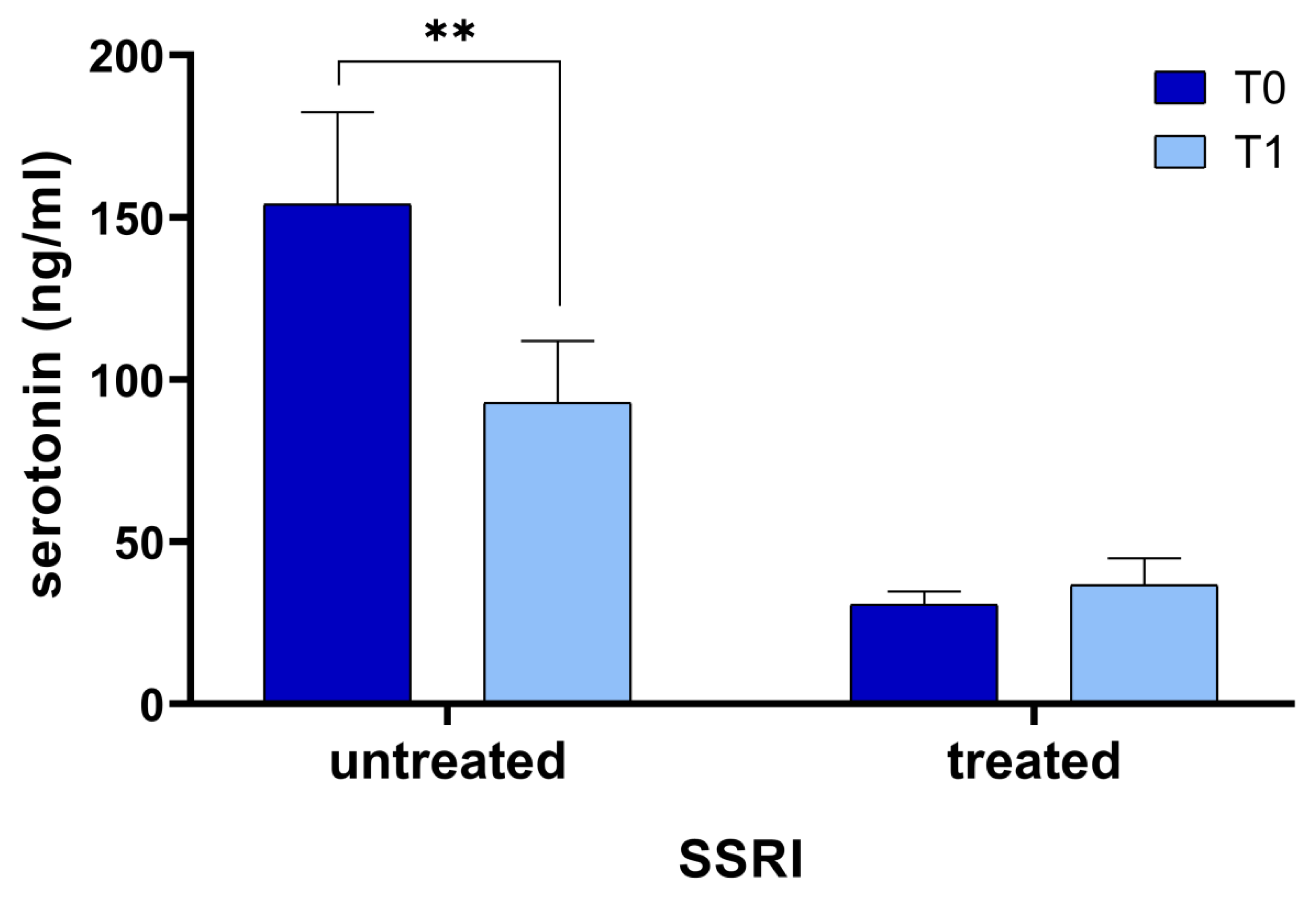
3.2. Serotonin Changes after Rehabilitation Programs
3.3. Correlation Between Serotonin Levels and Rehabilitation and Cognitive Performance Assessment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Executive Summary: Heart Disease and Stroke Statistics—2014 Update: A Report from the American Heart Association. Circulation 2014, 129, 399–410. [Google Scholar] [CrossRef]
- Hay, S.I.; Jayaraman, S.P.; Truelsen, T.; Sorensen, R.J.; Millear, A.; Giussani, G.; Beghi, E. GBD 2015 Disease and Injury Incidence and Prevalence Collaborators Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 310 Diseases and Injuries, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet Lond. Engl. 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Almeida, O.P.; Flicker, L.; Norman, P.; Hankey, G.J.; Vasikaran, S.; van Bockxmeer, F.M.; Jamrozik, K. Association of Cardiovascular Risk Factors and Disease with Depression in Later Life. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2007, 15, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Tatemichi, T.K.; Paik, M.; Bagiella, E.; Desmond, D.W.; Stern, Y.; Sano, M.; Hauser, W.A.; Mayeux, R. Risk of Dementia after Stroke in a Hospitalized Cohort: Results of a Longitudinal Study. Neurology 1994, 44, 1885–1891. [Google Scholar] [CrossRef] [PubMed]
- Kauhanen, M.; Korpelainen, J.T.; Hiltunen, P.; Brusin, E.; Mononen, H.; Määttä, R.; Nieminen, P.; Sotaniemi, K.A.; Myllylä, V.V. Poststroke Depression Correlates with Cognitive Impairment and Neurological Deficits. Stroke 1999, 30, 1875–1880. [Google Scholar] [CrossRef] [PubMed]
- Hackett, M.L.; Pickles, K. Part I: Frequency of Depression after Stroke: An Updated Systematic Review and Meta-Analysis of Observational Studies. Int. J. Stroke 2014, 9, 1017–1025. [Google Scholar] [CrossRef]
- Robinson, R.G.; Jorge, R.E. Post-Stroke Depression: A Review. Am. J. Psychiatry 2016, 173, 221–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villa, R.F.; Ferrari, F.; Moretti, A. Post-Stroke Depression: Mechanisms and Pharmacological Treatment. Pharmacol. Ther. 2018, 184, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Feng, C.; Fang, M.; Liu, X.-Y. The Neurobiological Pathogenesis of Poststroke Depression. Sci. World J. 2014, 2014, 521349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachdev, P.S.; Brodaty, H.; Valenzuela, M.J.; Lorentz, L.; Looi, J.C.L.; Berman, K.; Ross, A.; Wen, W.; Zagami, A.S. Clinical Determinants of Dementia and Mild Cognitive Impairment Following Ischaemic Stroke: The Sydney Stroke Study. Dement. Geriatr. Cogn. Disord. 2006, 21, 275–283. [Google Scholar] [CrossRef]
- Ihle-Hansen, H.; Thommessen, B.; Wyller, T.B.; Engedal, K.; Øksengård, A.R.; Stenset, V.; Løken, K.; Aaberg, M.; Fure, B. Incidence and Subtypes of MCI and Dementia 1 Year after First-Ever Stroke in Patients without Pre-Existing Cognitive Impairment. Dement. Geriatr. Cogn. Disord. 2011, 32, 401–407. [Google Scholar] [CrossRef]
- Nys, G.M.S.; van Zandvoort, M.J.E.; de Kort, P.L.M.; van der Worp, H.B.; Jansen, B.P.W.; Algra, A.; de Haan, E.H.F.; Kappelle, L.J. The Prognostic Value of Domain-Specific Cognitive Abilities in Acute First-Ever Stroke. Neurology 2005, 64, 821–827. [Google Scholar] [CrossRef]
- Leśniak, M.; Bak, T.; Czepiel, W.; Seniów, J.; Członkowska, A. Frequency and Prognostic Value of Cognitive Disorders in Stroke Patients. Dement. Geriatr. Cogn. Disord. 2008, 26, 356–363. [Google Scholar] [CrossRef]
- Narasimhalu, K.; Ang, S.; De Silva, D.A.; Wong, M.-C.; Chang, H.-M.; Chia, K.-S.; Auchus, A.P.; Chen, C.P. The Prognostic Effects of Poststroke Cognitive Impairment No Dementia and Domain-Specific Cognitive Impairments in Nondisabled Ischemic Stroke Patients. Stroke 2011, 42, 883–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oksala, N.K.J.; Jokinen, H.; Melkas, S.; Oksala, A.; Pohjasvaara, T.; Hietanen, M.; Vataja, R.; Kaste, M.; Karhunen, P.J.; Erkinjuntti, T. Cognitive Impairment Predicts Poststroke Death in Long-Term Follow-Up. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1230–1235. [Google Scholar] [CrossRef]
- Chen, C.; Leys, D.; Esquenazi, A. The Interaction between Neuropsychological and Motor Deficits in Patients after Stroke. Neurology 2013, 80, S27–S34. [Google Scholar] [CrossRef]
- Leem, M.J.; Kim, G.S.; Kim, K.H.; Yi, T.I.; Moon, H.I. Predictors of Functional and Motor Outcomes Following Upper Limb Robot-Assisted Therapy after Stroke. Int. J. Rehabil. Res. 2019, 42, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Aprile, I.; Guardati, G.; Cipollini, V.; Papadopoulou, D.; Mastrorosa, A.; Castelli, L.; Monteleone, S.; Redolfi, A.; Galeri, S.; Germanotta, M. Robotic Rehabilitation: An Opportunity to Improve Cognitive Functions in Subjects With Stroke. An Explorative Study. Front. Neurol. 2020, 11, 588285. [Google Scholar] [CrossRef] [PubMed]
- Aprile, I.; Guardati, G.; Cipollini, V.; Papadopoulou, D.; Monteleone, S.; Redolfi, A.; Garattini, R.; Sacella, G.; Noro, F.; Galeri, S.; et al. Influence of Cognitive Impairment on the Recovery of Subjects with Subacute Stroke Undergoing Upper Limb Robotic Rehabilitation. Brain Sci. 2021, 11, 587. [Google Scholar] [CrossRef] [PubMed]
- Riedel, W.J.; Klaassen, T.; Schmitt, J.A.J. Tryptophan, Mood, and Cognitive Function. Brain Behav. Immun. 2002, 16, 581–589. [Google Scholar] [CrossRef]
- Schmitt, J.A.J.; Wingen, M.; Ramaekers, J.G.; Evers, E.A.T.; Riedel, W.J. Serotonin and Human Cognitive Performance. Curr. Pharm. Des. 2006, 12, 2473–2486. [Google Scholar] [CrossRef]
- Gao, H.; Zhu, H.; Zhang, Y.; Wang, L. Reduction of Cerebrospinal Fluid and Plasma Serotonin in Patients with Post-Stroke Depression: A Preliminary Report. Clin. Investig. Med. 2008, 31, 351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowen, P.; Sherwood, A.C. The Role of Serotonin in Cognitive Function: Evidence from Recent Studies and Implications for Understanding Depression. J. Psychopharmacol. Oxf. Engl. 2013, 27, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Smith, A. A Symbol Digit Modalities Test; Western Psychological Services Los Angeles: Torrance, CA, USA, 1973. [Google Scholar]
- Nocentini, U.; Giordano, A.; Di Vincenzo, S.; Panella, M.; Pasqualetti, P. The Symbol Digit Modalities Test-Oral Version: Italian Normative Data. Funct. Neurol. 2006, 21, 93–96. [Google Scholar]
- Hebb, D. Distinctive features of learning in the higher animal. In Brain Mech Learn A Symp; Oxford: Blackwell, UK, 1961; pp. 37–46. [Google Scholar]
- Monaco, M.; Costa, A.; Caltagirone, C.; Carlesimo, G.A. Forward and Backward Span for Verbal and Visuo-Spatial Data: Standardization and Normative Data from an Italian Adult Population. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2013, 34, 749–754. [Google Scholar] [CrossRef]
- Osterrieth, P. Le Test de Copie d’une Figure Complexe; Contribution à l’étude de La Perception et de La Mémoire. Arch. Psychol. Geneve 1944, 30, 206–356. [Google Scholar]
- Rey, A. L’examen Psychologique Dans Les Cas d’encéphalopathie Traumatique. Arch Psychol. 1941, 28, 215–285. [Google Scholar]
- Shin, M.-S.; Park, S.-Y.; Park, S.-R.; Seol, S.-H.; Kwon, J.S. Clinical and Empirical Applications of the Rey-Osterrieth Complex Figure Test. Nat. Protoc. 2006, 1, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Meyers, J.E.; Bayless, J.D.; Meyers, K.R. Rey Complex Figure: Memory Error Patterns and Functional Abilities. Appl. Neuropsychol. 1996, 3, 89–92. [Google Scholar] [CrossRef]
- Shallice, T.; Broadbent, D.E.; Weiskrantz, L. Specific Impairments of Planning. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1982, 298, 199–209. [Google Scholar] [CrossRef]
- Keith Berg, W.; Byrd, D. The Tower of London Spatial Problem-Solving Task: Enhancing Clinical and Research Implementation. J. Clin. Exp. Neuropsychol. 2002, 24, 586–604. [Google Scholar] [CrossRef] [PubMed]
- Boccia, M.; Marin, D.; D’Antuono, G.; Ciurli, P.; Incoccia, C.; Antonucci, G.; Guariglia, C.; Piccardi, L. The Tower of London (ToL) in Italy: Standardization of the ToL Test in an Italian Population. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2017, 38, 1263–1270. [Google Scholar] [CrossRef]
- Caffarra, P.; Vezzadini, G.; Dieci, F.; Zonato, F.; Venneri, A. Una versione abbreviata del test di Stroop: Dati normativi nella popolazione Italiana. Nuova Riv. Neurol. 2002, 12, 111–115. [Google Scholar]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The Post-Stroke Hemiplegic Patient. 1. a Method for Evaluation of Physical Performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Bohannon, R.W. Motricity Index Scores Are Valid Indicators of Paretic Upper Extremity Strength Following Stroke. J. Phys. Ther. Sci. 1999, 11, 59–61. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the Sensitivity of the Barthel Index for Stroke Rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Réus, G.Z.; Jansen, K.; Titus, S.; Carvalho, A.F.; Gabbay, V.; Quevedo, J. Kynurenine Pathway Dysfunction in the Pathophysiology and Treatment of Depression: Evidences from Animal and Human Studies. J. Psychiatr. Res. 2015, 68, 316–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackett Maree, L.; Anderson Craig, S. Predictors of Depression after Stroke. Stroke 2005, 36, 2296–2301. [Google Scholar] [CrossRef]
- Fedoroff, J.P.; Starkstein, S.E.; Parikh, R.M.; Price, T.R.; Robinson, R.G. Are Depressive Symptoms Nonspecific in Patients with Acute Stroke? Am. J. Psychiatry 1991, 148, 1172–1176. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, T.A.; Nguyen, J.C.D.; Polglaze, K.E.; Bertrand, P.P. Influence of Tryptophan and Serotonin on Mood and Cognition with a Possible Role of the Gut-Brain Axis. Nutrients 2016, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Strasser, B.; Gostner, J.M.; Fuchs, D. Mood, Food, and Cognition: Role of Tryptophan and Serotonin. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 55–61. [Google Scholar] [CrossRef]
- Gariballa, S.E.; Parker, S.G.; Taub, N.; Castleden, C.M. Influence of Nutritional Status on Clinical Outcome after Acute Stroke. Am. J. Clin. Nutr. 1998, 68, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Rabadi, M.H.; Coar, P.L.; Lukin, M.; Lesser, M.; Blass, J.P. Intensive Nutritional Supplements Can Improve Outcomes in Stroke Rehabilitation. Neurology 2008, 71, 1856–1861. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, D.K.; Dutta, T.; Kannan, V.; Chandramouleeswaran, V. Amino Acids in Post-Stroke Rehabilitation. Nutr. Neurosci. 2019, 24, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Siotto, M.; Germanotta, M.; Santoro, M.; Di Blasi, C.; Loreti, C.; Mastropaolo, S.; Aprile, I. Total Serum Calcium and Recovery after Rehabilitation in Patients with Stroke. Appl. Sci. 2020, 10, 7893. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D and the Omega-3 Fatty Acids Control Serotonin Synthesis and Action, Part 2: Relevance for ADHD, Bipolar Disorder, Schizophrenia, and Impulsive Behavior. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2015, 29, 2207–2222. [Google Scholar] [CrossRef] [Green Version]
- Young, S.N. How to Increase Serotonin in the Human Brain without Drugs. J. Psychiatry Neurosci. JPN 2007, 32, 394–399. [Google Scholar]


{kind=link}
| Baseline Characteristics | Mean (±SD) or Number (%) |
|---|---|
| Age (years) | 68 ± 15 |
| Sex | |
| Men | 13 (44.8%) |
| Women | 16 (55.2%) |
| Education | 10.7 (4.6) |
| Index stroke type | |
| Ischemic | 23 (79.3%) |
| Hemorrhagic | 6 (20.7%) |
| Affected side | |
| Right | 11 (37.9%) |
| Left | 18 (62.1%) |
| Comorbidities | |
| Hypertension | 20 (69.0%) |
| Type 2 Diabetes | 9 (31.0%) |
| Dislipidemia | 5 (17.2%) |
| Hearth disease | 12 (41.4%) |
| Days from index stroke to enrollment | 92 ± 33 |
| Depression | |
| Minimal to moderate (BDI up to 29) | 18 (62.1%) |
| Severe (BDI equal to or higher than 30) | 11 (37.9%) |
| Antidepressive drugs (Selective Serotonin Reuptake Inhibitors, SSRI) | 16 (55.2%) |
| Cognitive assessment | |
| SDMT | 21.8 ± 13.5 |
| ROCF | 20.1 ± 12.1 |
| DS | 3.6 ± 2.0 |
| Stroop_error | 4.8 ± 5.1 |
| Stroop_time | 41.0 ± 37.2 |
| ToL_point | 29.5 ± 3.5 |
| ToL_Time | 526.9 ± 263.0 |
| ToL_errors | 8.0 ± 12.4 |
| Motor Assessment | |
| Modified Barthel Index (0–100) | 40.7 ± 17.7 |
| Motricity Index | 30.8 ± 24.4 |
| Fugl Meyer | 16.7 ± 15.7 |
| Serum Serotonin (ng/mL) | 85.9 ± 92.4 |
| Serotonin T0 | ||
|---|---|---|
| Spearman Rho | p-Value | |
| SDMT T0 | −0.129 | 0.576 |
| ROCF T0 | 0.100 | 0.666 |
| DS T0 | −0.086 | 0.712 |
| Stroop_error T0 | −0.133 | 0.565 |
| Stroop_time T0 | −0.189 | 0.413 |
| ToL_point T0 | 0.583 * | 0.006 |
| ToL_time T0 | −0.239 | 0.297 |
| ToL_errors T0 | −0.118 | 0.610 |
| Barthel Index | 0.278 | 0.144 |
| Motricity Index | 0.237 | 0.302 |
| Fugl Meyer | 0.124 | 0.592 |
| Serotonin T0 | ΔSerotonin | |||
|---|---|---|---|---|
| Spearman Rho | p-Value | Spearman Rho | p-Value | |
| ΔSDMT | 0.016 | 0.938 | 0.156 | 0.499 |
| ΔROCF | −0.257 | 0.196 | 0.535 * | 0.013 |
| ΔDS | 0.090 | 0.656 | −0.157 | 0.496 |
| ΔStroop_error | 0.034 | 0.865 | −0.165 | 0.476 |
| ΔStroop_time | −0.130 | 0.516 | 0.019 | 0.935 |
| ΔTol_points | −0.173 | 0.387 | 0.621 ** | 0.003 |
| ΔTol_time | 0.321 | 0.102 | −0.619 ** | 0.003 |
| ΔTol_error | 0.378 | 0.052 | −0.375 | 0.094 |
| DeltaBI | −0.206 | 0.221 | 0.248 | 0.194 |
| DeltaMI | −0.065 | 0.748 | 0.007 | 0.975 |
| DeltaFM | −0.028 | 0.890 | 0.157 | 0.497 |
| ΔSerotonin Treated with SSRIs (n = 16) | ΔSerotonin Untreated with SSRIs (n = 13) | |||
|---|---|---|---|---|
| Spearman Rho | p-Value | Spearman Rho | p-Value | |
| ΔSDMT | 0.219 | 0.495 | 0.322 | 0.398 |
| ΔROCF | 0.473 | 0.121 | 0.700 * | 0.036 |
| ΔDS | 0.099 | 0.761 | 0.121 | 0.765 |
| ΔStroop_error | −0.564 | 0.056 | 0.322 | 0.383 |
| ΔStroop_time | −0.525 | 0.079 | 0.750 * | 0.020 |
| ΔTol_points | 0.587 * | 0.045 | 0.740 * | 0.023 |
| ΔTol_time | −0.503 | 0.095 | −0.833 ** | 0.005 |
| ΔTol_error | −0.214 | 0.503 | −0.328 | 0.389 |
| DeltaBI | 0.325 | 0.219 | −0.328 | 0.273 |
| DeltaMI | 0.049 | 0.879 | 0.150 | 0.700 |
| DeltaFM | 0.316 | 0.316 | 0.267 | 0.488 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siotto, M.; Germanotta, M.; Santoro, M.; Cipollini, V.; Guardati, G.; Papadopoulou, D.; Bray, E.; Mastrorosa, A.; Aprile, I. Serotonin Levels and Cognitive Recovery in Patients with Subacute Stroke after Rehabilitation Treatment. Brain Sci. 2021, 11, 642. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050642
Siotto M, Germanotta M, Santoro M, Cipollini V, Guardati G, Papadopoulou D, Bray E, Mastrorosa A, Aprile I. Serotonin Levels and Cognitive Recovery in Patients with Subacute Stroke after Rehabilitation Treatment. Brain Sciences. 2021; 11(5):642. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050642
Chicago/Turabian StyleSiotto, Mariacristina, Marco Germanotta, Massimo Santoro, Valeria Cipollini, Giulia Guardati, Dionysia Papadopoulou, Elisa Bray, Alessia Mastrorosa, and Irene Aprile. 2021. "Serotonin Levels and Cognitive Recovery in Patients with Subacute Stroke after Rehabilitation Treatment" Brain Sciences 11, no. 5: 642. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050642