
Relationship between Speed of Response Inhibition and Ability to Suppress a Step in Midlife and Older Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Stop Signal Task (SST)
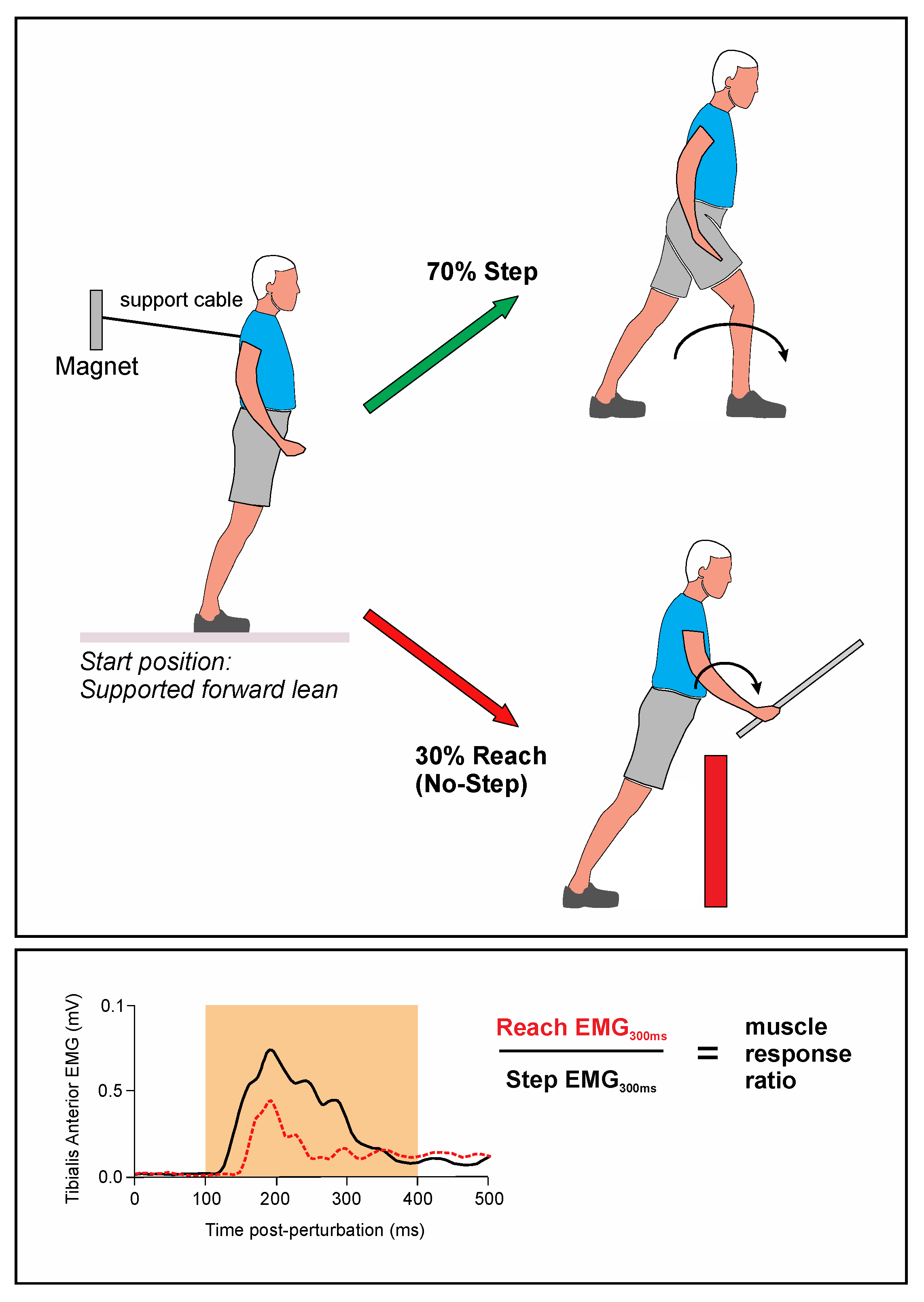
2.2.2. Lean-and-Release Task
2.3. Electromyography and Force Sensors
2.4. Analysis
3. Results
3.1. Stop Signal Task
3.2. Lean-and-Release Task
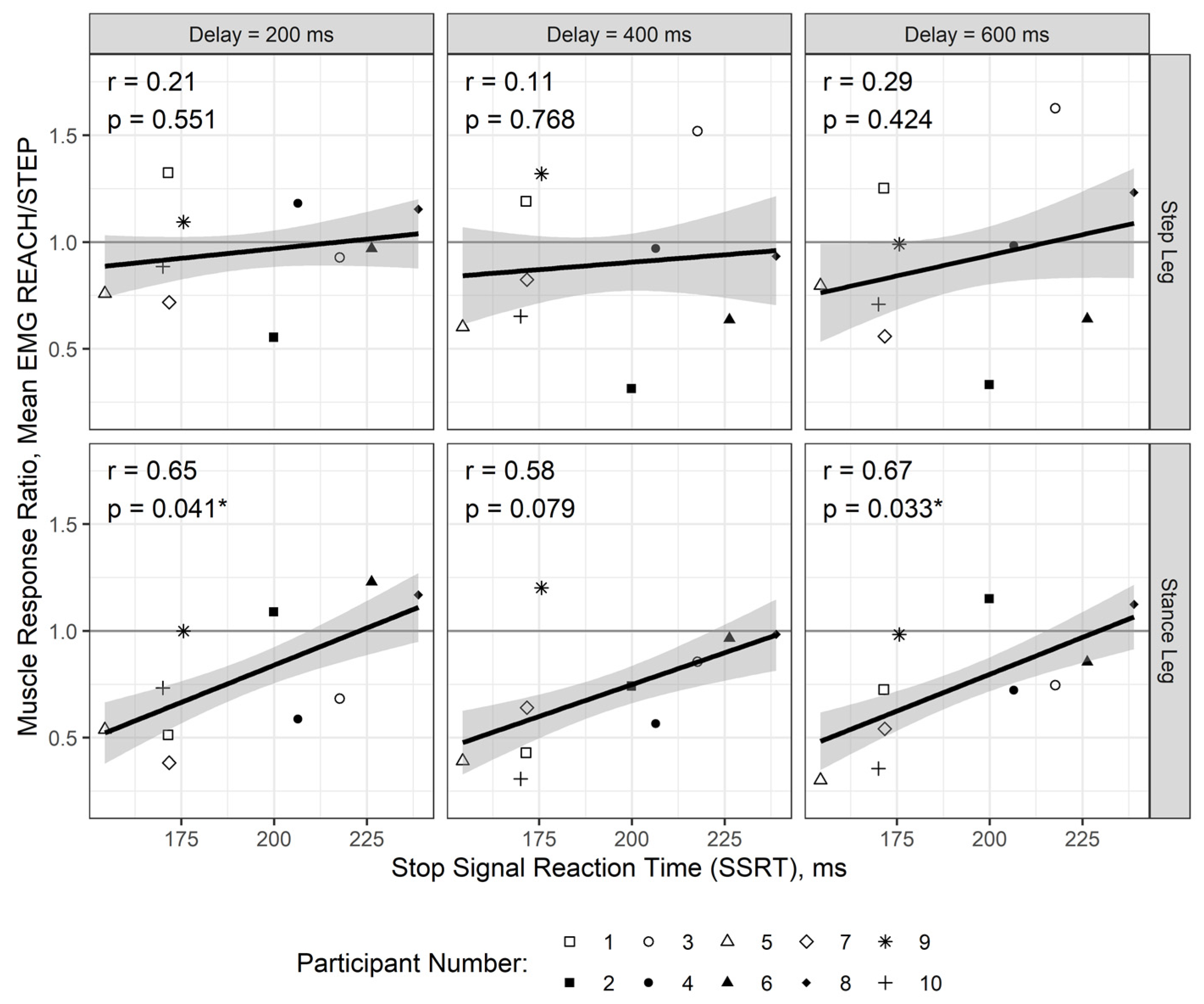
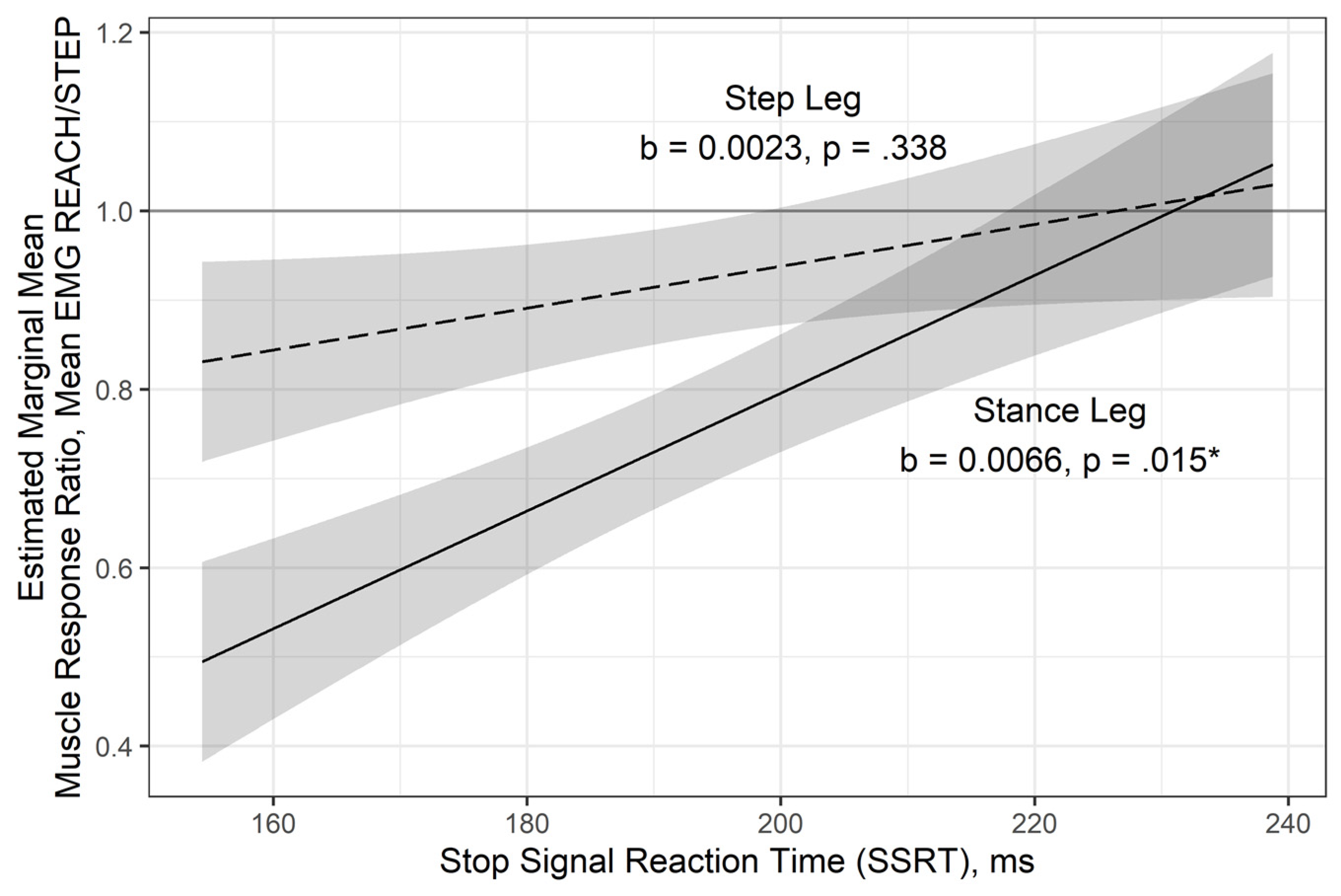
3.3. Relationship Between Muscle Activation in the Legs and Stop Signal Reaction Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fuster, J.M. The Prefrontal Cortex; Academic Press: Camridge, MA, USA, 2008; Volume 4. [Google Scholar]
- Mori, S. Integration of posture and locomotion in acute decerebrate cats and in awake, freely moving cats. Prog. Neurobiol. 1987, 28, 161–195. [Google Scholar] [CrossRef]
- Honeycutt, C.F.; Nichols, T.R. The decerebrate cat generates the essential features of the force constraint strategy. J. Neurophysiol. 2010, 103, 3266–3273. [Google Scholar] [CrossRef] [Green Version]
- Macpherson, J.M.; Horak, F.B. Posture. In Principles of Neural Science; Kandel, E.R., Schwartz, J.H., Jessell, T.M., Siegelbaum, S.A., Hudspeth, A.J., Eds.; McGraw-Hill: New York, NY, USA, 2013; Volume 5, Chapter 41; pp. 935–959. [Google Scholar]
- Mirelman, A.; Herman, T.; Brozgol, M.; Dorfman, M.; Sprecher, E.; Schweiger, A.; Giladi, N.; Hausdorff, J.M. Executive function and falls in older adults: New findings from a five-year prospective study link fall risk to cognition. PLoS ONE 2012, 7, e40297. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Gopaul, K.; Odasso, M.M.M. The role of cognitive impairment in fall risk among older adults: A systematic review and meta-analysis. Age Ageing 2012, 41, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Herman, T.; Mirelman, A.; Giladi, N.; Schweiger, A.; Hausdorff, J.M. Executive control deficits as a prodrome to falls in healthy older adults: A prospective study linking thinking, walking, and falling. J. Gerontol. Biol. Sci. Med. Sci. 2010, 65, 1086–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caetano, M.J.D.; Lord, S.R.; Brodie, M.A.; Schoene, D.; Pelicioni, P.H.S.; Sturnieks, D.L.; Menant, J.C. Executive functioning, concern about falling and quadriceps strength mediate the relationship between impaired gait adaptability and fall risk in older people. Gait Posture 2018, 59, 188–192. [Google Scholar] [CrossRef]
- Amboni, M.; Barone, P.; Hausdorff, J.M. Cognitive contributions to gait and falls: Evidence and implications. Mov. Disord. 2013, 28, 1520–1533. [Google Scholar] [CrossRef] [PubMed]
- Saverino, A.; Waller, D.; Rantell, K.; Parry, R.; Moriarty, A.; Playford, E.D. The role of cognitive factors in predicting balance and fall risk in a neuro-rehabilitation setting. PLoS ONE 2016, 11, e0153469. [Google Scholar] [CrossRef] [Green Version]
- Wardt, V.; Van der Logan, P.; Hood, V.; Booth, V.; Masud, T.; Harwood, R. The association of specific executive functions and falls risk in people with mild cognitive impairment and early-stage dementia. Dement. Geriatr. Cogn. Disord. 2015, 40, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.G.; Nutt, J.G.; Horak, F.B. Errors in postural preparation lead to increased choice reaction times for step initiation in older adults. J. Gerontol. Biol. Sci. Med. Sci. 2011, 66, 705–713. [Google Scholar] [CrossRef] [Green Version]
- Sparto, P.J.; Fuhrman, S.I.; Redfern, M.S.; Jennings, J.R.; Perera, S.; Nebes, R.D.; Furman, J.M. Postural adjustment errors reveal deficits in inhibition during lateral step initiation in older adults. J. Neurophysiol. 2012, 109, 415–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- MacLeod, C.M. Half a century of research on the stroop effect: An integrative review. Psychol. Bull. 1991, 109, 163–203. [Google Scholar] [CrossRef] [PubMed]
- Scarpina, F.; Tagini, S. The stroop color and word test. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoene, D.; Delbaere, K.; Lord, S.R. Impaired response selection during stepping predicts falls in older people—A cohort study. J. Am. Med. Dir. Assoc. 2017, 18, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Aron, A.R.; Poldrack, R.A. Cortical and subcortical contributions to stop signal response inhibition: Role of the subthalamic nucleus. J. Neurosci. Off. J. Soc. Neurosci. 2006, 26, 2424–2433. [Google Scholar] [CrossRef] [Green Version]
- Aron, A.R.; Robbins, T.W.; Poldrack, R.A. Inhibition and the right inferior frontal cortex: One decade on. Trends Cogn. Sci. 2014, 18, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Tabu, H.; Mima, T.; Aso, T.; Takahashi, R.; Fukuyama, H. Common inhibitory prefrontal activation during inhibition of hand and foot responses. NeuroImage 2012, 59, 3373–3378. [Google Scholar] [CrossRef]
- Goode, C.; Cole, D.M.; Bolton, D.A.E. Staying upright by shutting down? Evidence for global suppression of the motor system when recovering balance. Gait Posture 2019, 70, 260–263. [Google Scholar] [CrossRef] [Green Version]
- Badry, R.; Mima, T.; Aso, T.; Nakatsuka, M.; Abe, M.; Fathi, D.; Foly, N.; Nagiub, H.; Nagamine, T.; Fukuyama, H. Suppression of human cortico-motoneuronal excitability during the stop-signal task. Clin. Neurophysiol. 2009, 120, 1717–1723. [Google Scholar] [CrossRef]
- Rydalch, G.; Bell, H.B.; Ruddy, K.L.; Bolton, D.A.E. Stop-signal reaction time correlates with a compensatory balance response. Gait Posture 2019, 71, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Bolton, D.A.E.; Mansour, M. A modified lean and release technique to emphasize response inhibition and action selection in reactive balance. J. Vis. Exp. JoVE 2020, e60688. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.W.; Mille, M.-L. Balance Perturbations. In Handbook of Clinical Neurology; Day, B.L., Lord, S.R., Eds.; Balance, Gait, and Falls; Elsevier: Amsterdam, The Netherlands, 2018; Volume 159, Chapter 5; pp. 85–105. [Google Scholar]
- Rogers, M.W.; Mille, M.-L. Timing paradox of stepping and falls in ageing: Not so quick and quick(Er) on the trigger. J. Physiol. 2016, 594, 4537–4547. [Google Scholar] [CrossRef] [Green Version]
- Mille, M.-L.; Simoneau, M.; Rogers, M.W. Postural dependence of human locomotion during gait initiation. J. Neurophysiol. 2014, 112, 3095–3103. [Google Scholar] [CrossRef] [Green Version]
- Mille, M.-L.; Hilliard, M.J.; Martinez, K.M.; Simuni, T.; Rogers, M.W. Acute effects of a lateral postural assist on voluntary step initiation in patients with parkinson’s disease. Mov. Disord. 2007, 22, 20–27. [Google Scholar] [CrossRef]
- McIlroy, W.E.; Maki, B.E. The control of lateral stability during rapid stepping reactions evoked by antero-posterior perturbation: Does anticipatory control play a role? Gait Posture 1999, 9, 190–198. [Google Scholar] [CrossRef]
- Peeters, G.; Van Schoor, N.M.; Cooper, R.; Tooth, L.; Kenny, R.A. Should prevention of falls start earlier? Co-ordinated analyses of harmonised data on falls in middle-aged adults across four population-based cohort studies. PLoS ONE 2018, 13, e0201989. [Google Scholar] [CrossRef] [Green Version]
- Logan, G.D.; Cowan, W.B. On the ability to inhibit thought and action: A theory of an act of control. Psychol. Rev. 1984, 91, 295–327. [Google Scholar] [CrossRef]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Jaeger, B. R2glmm: Computes R Squared for Mixed (Multilevel) Models. Available online: https://cran.microsoft.com/snapshot/2020-04-01/web/packages/r2glmm/r2glmm.pdf (accessed on 14 May 2021).
- Lüdecke, D.; Makowski, D.; Waggoner, P.; Patil, I. Assessment of Regression Models Performance. Available online: https://easystats.github.io/performance/ (accessed on 2 November 2020).
- Verbruggen, F.; Aron, A.R.; Band, G.P.; Beste, C.; Bissett, P.G.; Brockett, A.T.; Brown, J.W.; Chamberlain, S.R.; Chambers, C.D.; Colonius, H.; et al. A consensus guide to capturing the ability to inhibit actions and impulsive behaviors in the stop-signal task. eLife 2019, 8, e46323. [Google Scholar] [CrossRef]
- Thelen, D.G.; Muriuki, M.; James, J.; Schultz, A.B.; Ashton-Miller, J.A.; Alexander, N.B. Muscle activities used by young and old adults when stepping to regain balance during a forward fall. J. Electromyogr. Kinesiol. 2000, 10, 93–101. [Google Scholar] [CrossRef]
- Manchester, D.; Woollacott, M.; Zederbauer-Hylton, N.; Marin, O. Visual, vestibular and somatosensory contributions to balance control in the older adult. J. Gerontol. 1989, 44, M118–M127. [Google Scholar] [CrossRef]
- Iwamoto, Y.; Takahashi, M.; Shinkoda, K. Muscle co-contraction in elderly people change due to postural stability during single-leg standing. J. Physiol. Anthropol. 2017, 36, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nagai, K.; Yamada, M.; Uemura, K.; Yamada, Y.; Ichihashi, N.; Tsuboyama, T. Differences in muscle coactivation during postural control between healthy older and young adults. Arch. Gerontol. Geriatr. 2011, 53, 338–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, W. Age-related differences in body segmental movement during perturbed stance in humans. Clin. Biomech. Bristol Avon 1998, 13, 300–307. [Google Scholar] [CrossRef]
- Tucker, M.G.; Kavanagh, J.J.; Morrison, S.; Barrett, R.S. Voluntary sway and rapid orthogonal transitions of voluntary sway in young adults, and low and high fall-risk older adults. Clin. Biomech. Bristol Avon 2009, 24, 597–605. [Google Scholar] [CrossRef] [Green Version]
- Louwerens, J.W.K.; Van Linge, B.; Klerk, L.W.L.D.; Mulder, P.G.H.; Snijders, C.J. Peroneus longus and tibialis anterior muscle activity in the stance phase: A quantified electromyographic study of 10 controls and 25 patients with chronic ankle instability. Acta Orthop. Scand. 1995, 66, 517–523. [Google Scholar] [CrossRef]
- Hasher, L.; Zacks, R.T. Working Memory, Comprehension, and Aging: A Review and a New View. In The Psychology of Learning and Motivation: Advances in Research and Theory; Academic Press: San Diego, CA, USA, 1988; Volume 22, pp. 193–225. ISBN 978–0-12–543322–8. [Google Scholar]
- Salthouse, T.A. Aging and measures of processing speed. Biol. Psychol. 2000, 54, 35–54. [Google Scholar] [CrossRef]
- Rey-Mermet, A.; Gade, M. Inhibition in aging: What is preserved? What declines? A meta-analysis. Psychon. Bull. Rev. 2018, 25, 1695–1716. [Google Scholar] [CrossRef] [Green Version]
- Verhaeghen, P. Aging and executive control: Reports of a demise greatly exaggerated. Curr. Dir. Psychol. Sci. 2011, 20, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Sage, M.D.; Beyer, K.B.; Laylor, M.; Liang, C.; Roy, E.A.; McIlroy, W.E. A single session of exercise as a modulator of short-term learning in healthy individuals. Neurosci. Lett. 2016, 629, 92–98. [Google Scholar] [CrossRef]
- Chang, Y.-K.; Tsai, C.-L.; Huang, C.-C.; Wang, C.-C.; Chu, I.-H. Effects of acute resistance exercise on cognition in late middle-aged adults: General or specific cognitive improvement? J. Sci. Med. Sport 2014, 17, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Hochman, S.; Leshem, S.; Henik, A.; Kalanthroff, E. Conditioning automatic inhibition task: Introducing a novel task to associate automatic inhibition with specific cues. J. Neurosci. Methods 2020, 342, 108809. [Google Scholar] [CrossRef] [PubMed]
- Berg, E.A. A simple objective technique for measuring flexibility in thinking. J. Gen. Psychol. 1948, 39, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Monchi, O.; Petrides, M.; Petre, V.; Worsley, K.; Dagher, A. Wisconsin card sorting revisited: Distinct neural circuits participating in different stages of the task identified by event-related functional magnetic resonance imaging. J. Neurosci. 2001, 21, 7733–7741. [Google Scholar] [CrossRef] [Green Version]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Fixed Effects | Estimated Slope b (SE) | Walde Significancee p-Value | Marginal Partiale Pseudo-R2 |
|---|---|---|---|
| Intercept | 0.9220 (0.064) | <0.001 ** | |
| Main Effects | |||
| SSRT, ms | 0.0023 (0.002) | 0.338 | 0.024 |
| Leg, Stance vs. Step | −0.1710 (0.064) | 0.010 * | 0.083 |
| Interaction | |||
| SSRT × Leg | −0.0043 (0.002) | 0.078 † | 0.039 |
| Random Effects | Variance | p-value | |
| Participants Intercepts | 0.0202 | 0.021 * | |
| Residual Error | 0.0627 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
England, D.; Ruddy, K.L.; Dakin, C.J.; Schwartz, S.E.; Butler, B.; Bolton, D.A.E. Relationship between Speed of Response Inhibition and Ability to Suppress a Step in Midlife and Older Adults. Brain Sci. 2021, 11, 643. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050643
England D, Ruddy KL, Dakin CJ, Schwartz SE, Butler B, Bolton DAE. Relationship between Speed of Response Inhibition and Ability to Suppress a Step in Midlife and Older Adults. Brain Sciences. 2021; 11(5):643. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050643
Chicago/Turabian StyleEngland, Derek, Kathy L. Ruddy, Christopher J. Dakin, Sarah E. Schwartz, Blake Butler, and David A. E. Bolton. 2021. "Relationship between Speed of Response Inhibition and Ability to Suppress a Step in Midlife and Older Adults" Brain Sciences 11, no. 5: 643. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050643