
Gross and Micro-Anatomical Study of the Cavernous Segment of the Abducens Nerve and Its Relationships to Internal Carotid Plexus: Application to Skull Base Surgery

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Gross Anatomical Study and Measurements
2.2. Sihler’s Staining
2.3. Histological Examination
3. Results
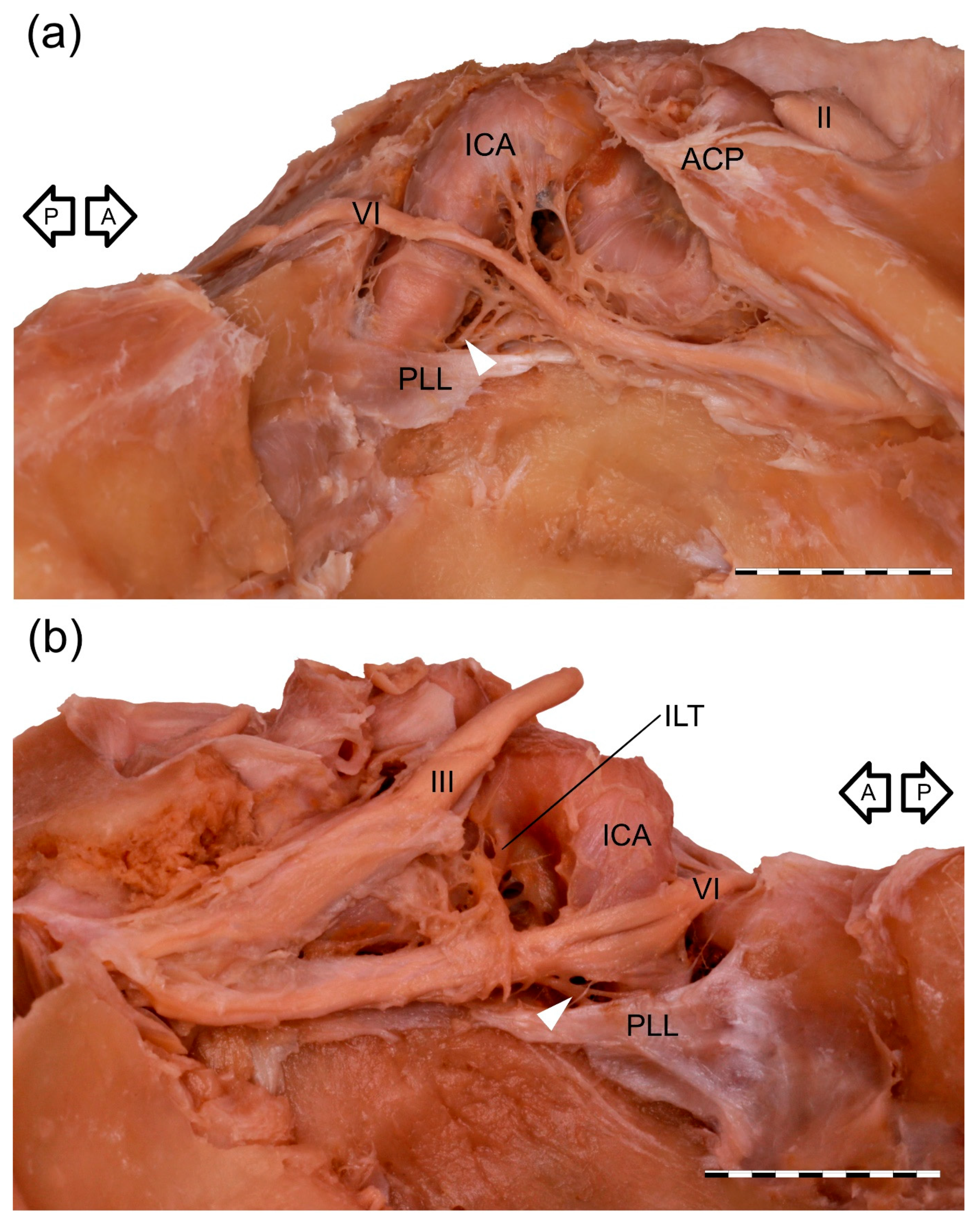
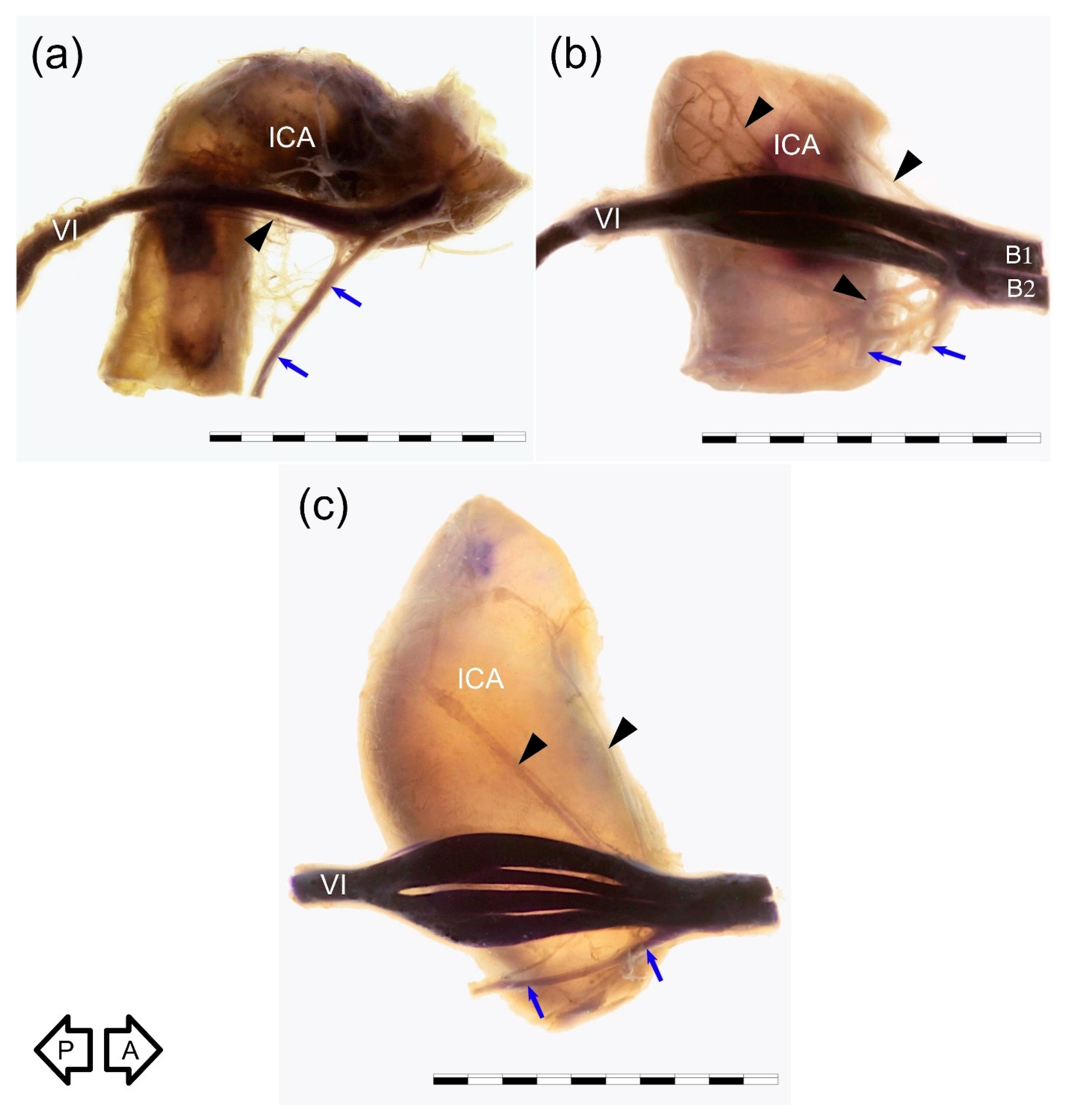
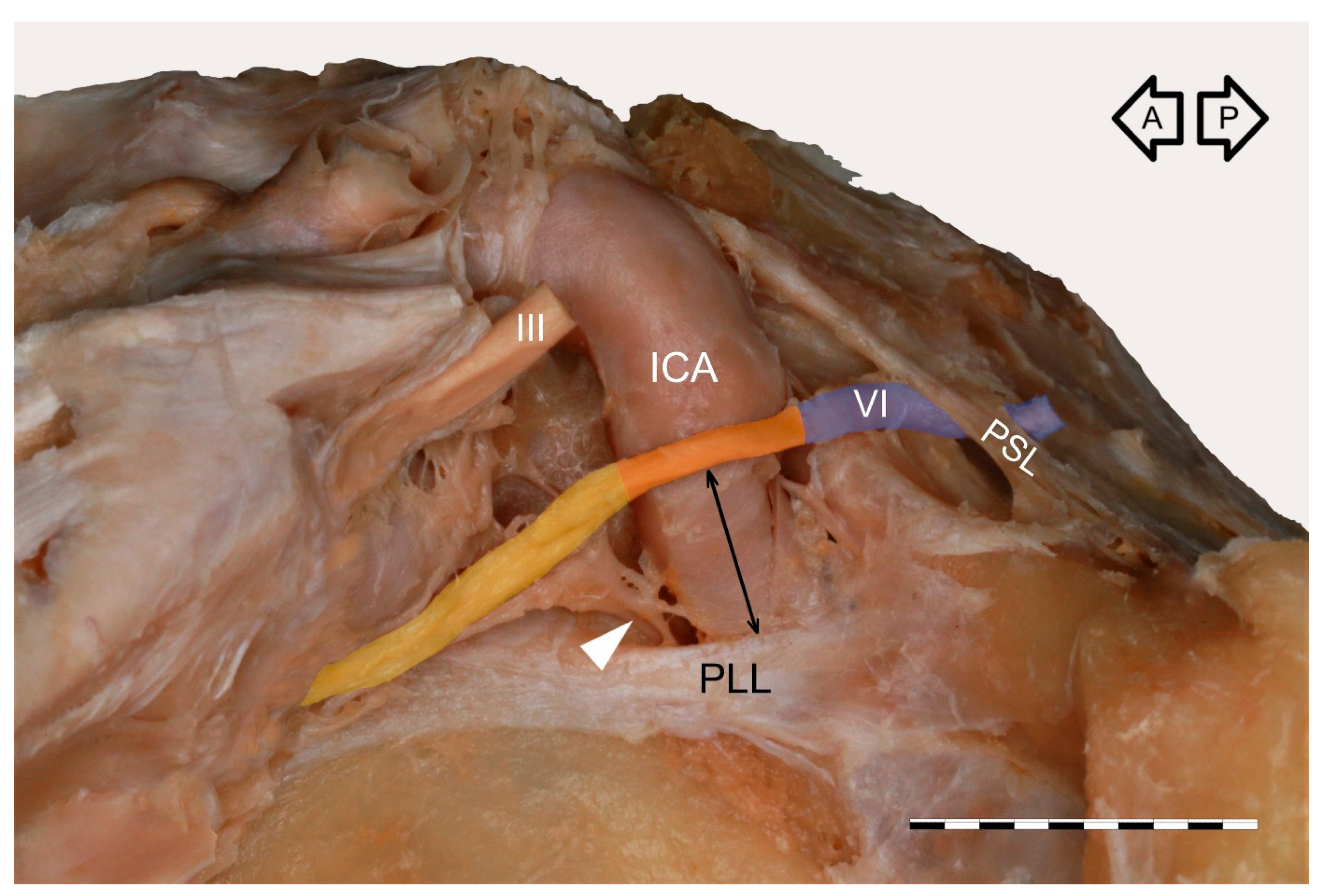
3.1. Gross Anatomical Observations
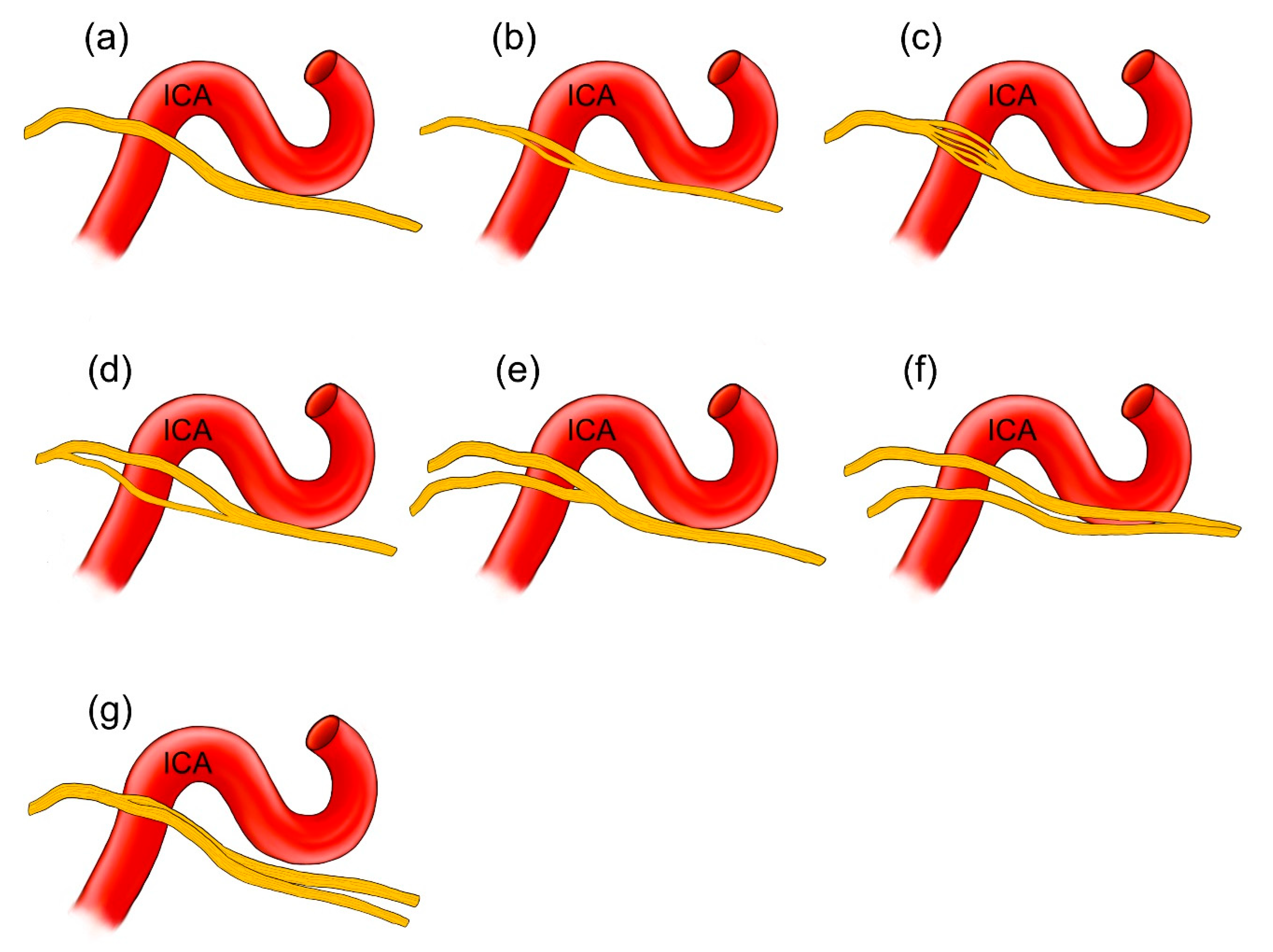
3.2. Anatomical Variations
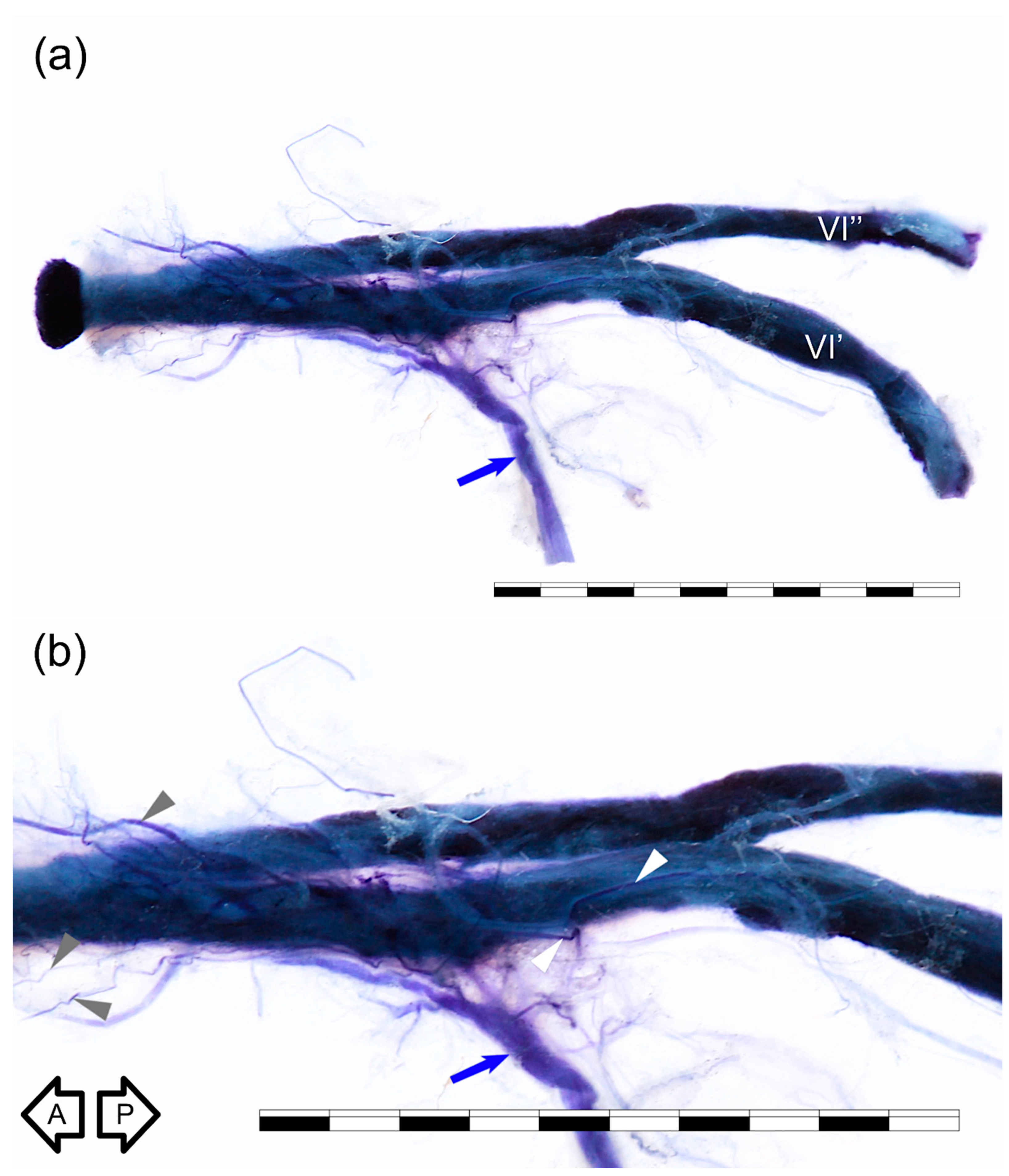
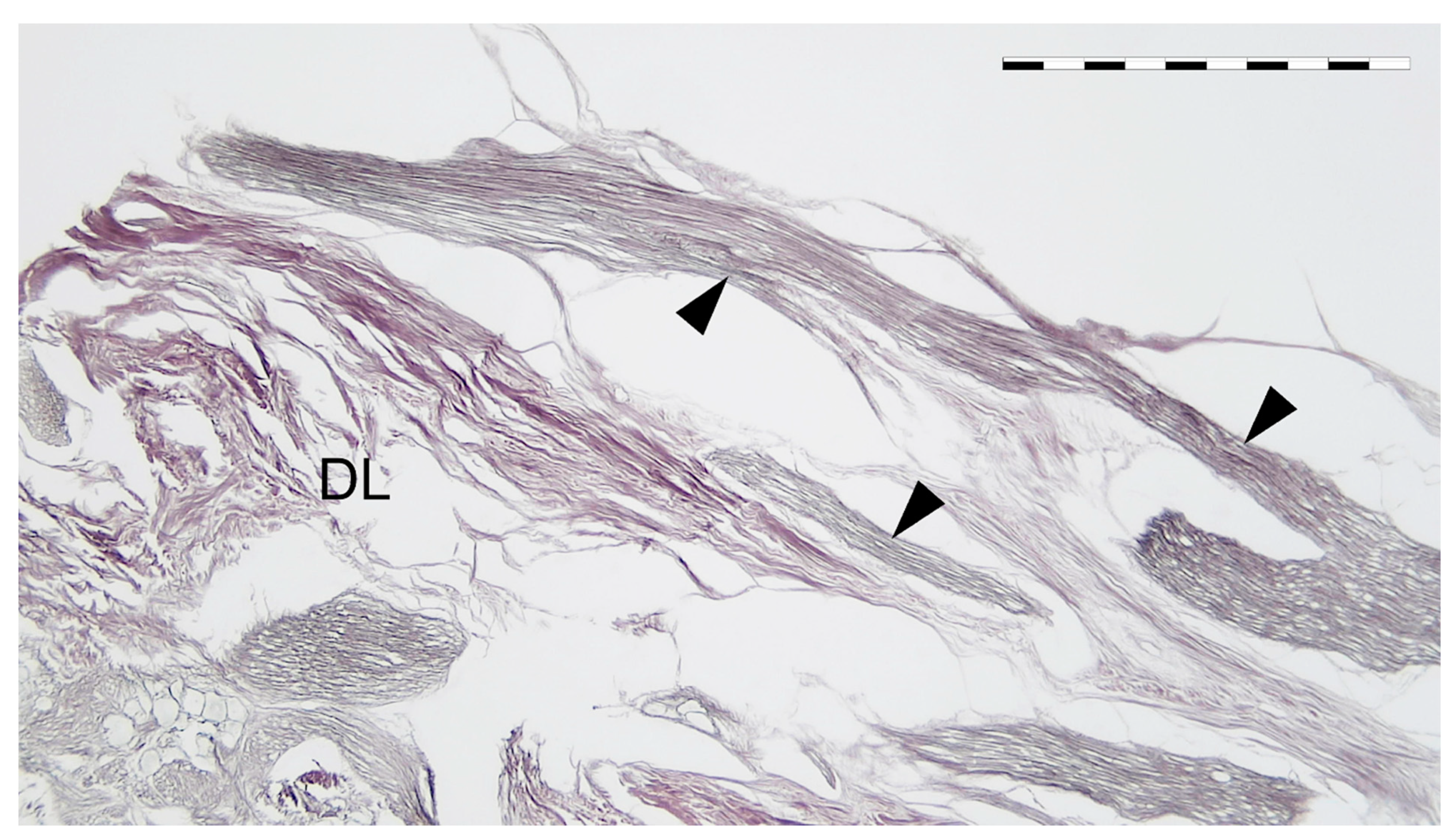
3.3. Sihler’s Staining
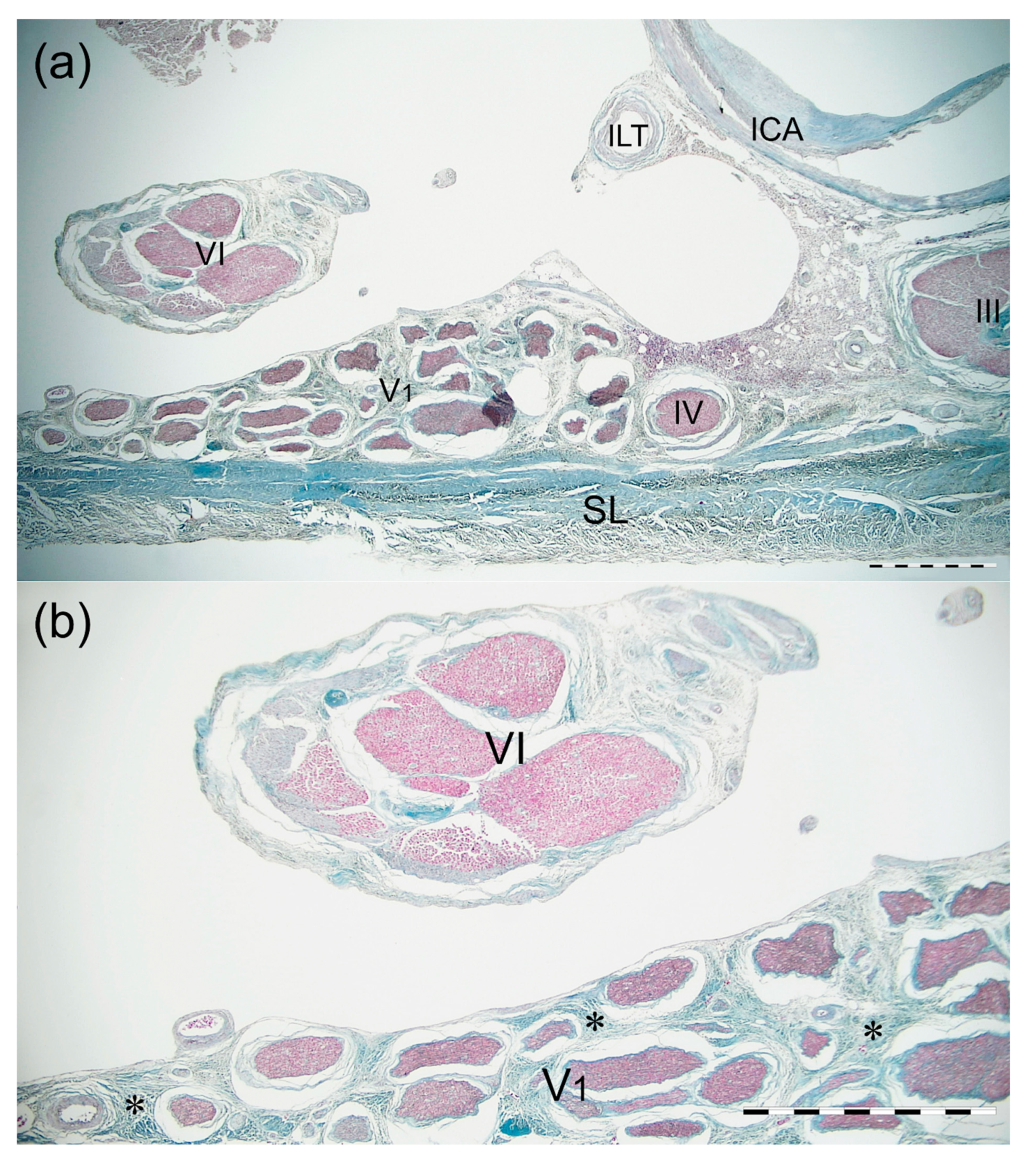
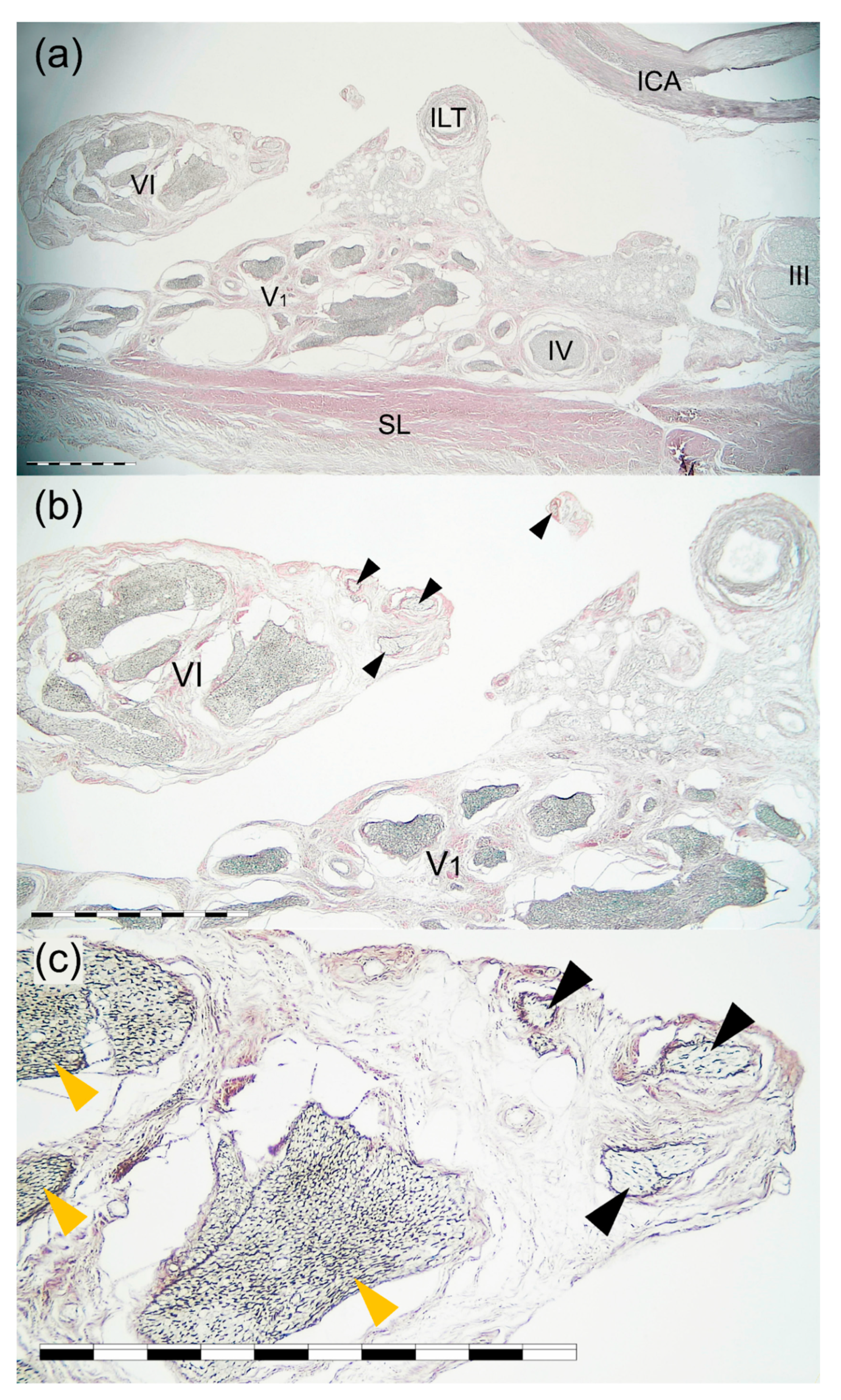
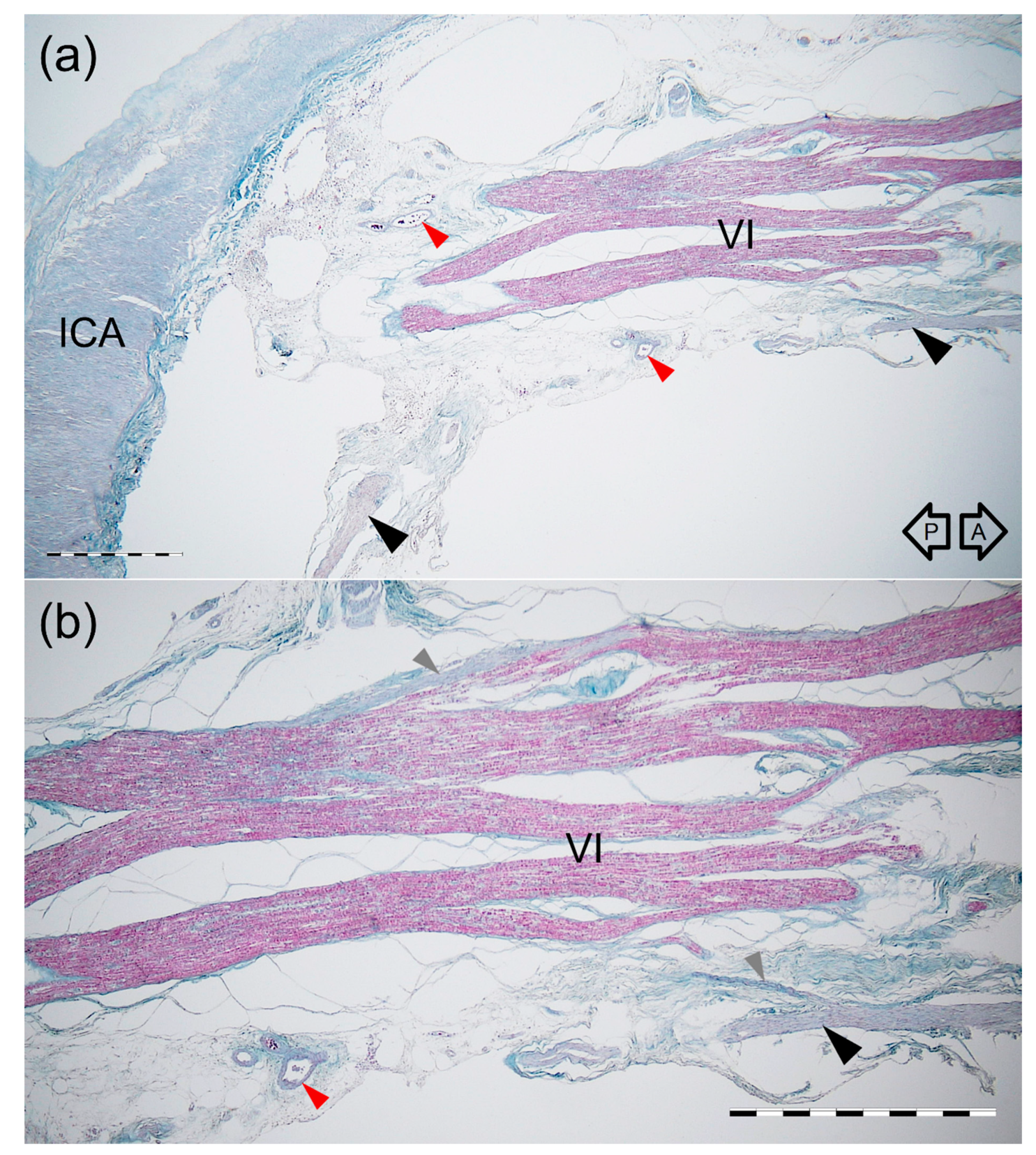
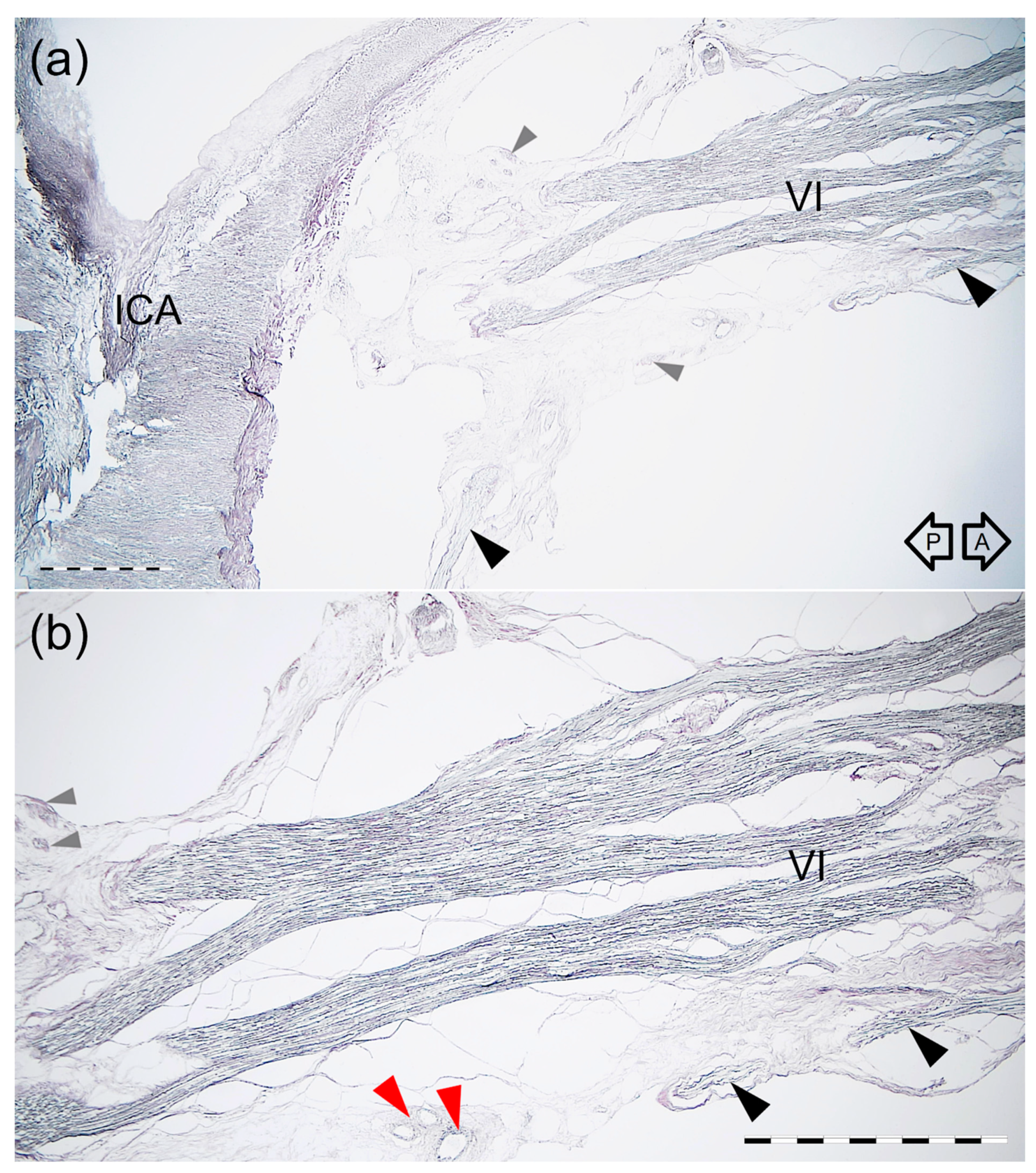
3.4. Histological Examination
3.5. Proposal of AN Cavernous Segment Subdivision
4. Discussion
Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dolenc, V.V. Anatomy and Surgery of the Cavernous Sinus; Springer: Wien, Austria, 1989. [Google Scholar]
- Dolenc, V.V. Microsurgical Anatomy and Surgery of the Central Skull Base; Springer: Wien, Austria, 2003. [Google Scholar]
- Rhoton, A.L., Jr. The Cavernous Sinus, the Cavernous Venous Plexus, and the Carotid Collar. Neurosurgery 2002, 51 (Suppl. 4), S1-375–S1-410. [Google Scholar] [CrossRef]
- Parkinson, D. A surgical approach to the cavernous portion of the carotid artery. Anatomical studies and case report. J. Neurosurg. 1965, 23, 474–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isolan, G.R.; Krayenbühl, N.; de Oliveira, E.; Al-Mefty, O. Microsurgical Anatomy of the Cavernous Sinus: Measurements of the Triangles in and around It. Skull Base 2007, 17, 357–367. [Google Scholar] [CrossRef] [Green Version]
- Isolan, G.R.; Souza Braga, F.L.; Campero, A.; Landeiro, J.A.; de Araújo, R.M.L.; Adjer, P.; Sakaya, G.R.; Rabelo, N.N.; da Silva Brito, J.; Teixeira, M.J.; et al. Microsurgical and Endoscopic Anatomy of the Cavernous Sinus. Bras. Neurocir. Arq. Bras. Neurosurg. 2020, 39, 83–94. [Google Scholar] [CrossRef] [Green Version]
- Bouthillier, A.; van Loveren, H.R.; Keller, J.T. Segments of the internal carotid artery: A new classification. Neurosurgery 1996, 38, 425–432. [Google Scholar] [CrossRef]
- Bleys, R.L.; Janssen, L.M.; Groen, G.J. The lateral sellar nerve plexus and its connections in humans. J. Neurosurg. 2001, 95, 102–110. [Google Scholar] [CrossRef]
- Iwanaga, J.; Anand, M.K.; Camacho, A.; Rodriguez, F.; Watson, C.; Caskey, E.L.; Dumont, A.S.; Tubbs, R.S. Surgical anatomy of the internal carotid plexus branches to the abducens nerve in the cavernous sinus. Clin. Neurol. Neurosurg. 2020, 191, 105690. [Google Scholar] [CrossRef]
- Jittapiromsak, P.; Sabuncuoglu, H.; Deshmukh, P.; McDougall, C.G.; Spetzler, R.F.; Preul, M.C. Anatomical relationships of intracavernous internal carotid artery to intracavernous neural structures. Skull Base 2010, 20, 327–336. [Google Scholar] [CrossRef] [Green Version]
- Iaconetta, G.; Fusco, M.; Cavallo, L.M.; Cappabianca, P.; Samii, M.; Tschabitscher, M. The abducens nerve: Microanatomic and endoscopic study. Neurosurgery 2007, 61 (Suppl. 3), 7–14. [Google Scholar] [CrossRef] [PubMed]
- Umansky, F.; Nathan, H. The lateral wall of the cavernous sinus. With special reference to the nerves related to it. J. Neurosurg. 1982, 56, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Campero, A.; Campero, A.A.; Martins, C.; Yasuda, A.; Rhoton, A.L., Jr. Surgical anatomy of the dural walls of the cavernous sinus. J. Clin. Neurosci. 2010, 17, 746–750. [Google Scholar] [CrossRef]
- Sato, M.; Cho, K.H.; Yamamoto, M.; Hirouchi, H.; Murakami, G.; Abe, H.; Abe, S. Cavernous sinus and abducens nerve in human fetuses near term. Surg. Radiol. Anat. 2020, 42, 761–770. [Google Scholar] [CrossRef]
- van Overbeeke, J.J.; Dujovny, M.; Troost, D. Anatomy of the sympathetic pathways in the cavernous sinus. Neurol. Res. 1995, 17, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Bleys, R.L.; Cowen, T. Innervation of cerebral blood vessels: Morphology, plasticity, age-related, and Alzheimer’s disease-related neurodegeneration. Microsc. Res. Tech. 2001, 53, 106–118. [Google Scholar] [CrossRef]
- Mu, L.; Sanders, I. Sensory nerve supply of the human oro- and laryngopharynx: A preliminary study. Anat. Rec. 2000, 258, 406–420. [Google Scholar] [CrossRef]
- Mu, L.; Sanders, I. Sihler’s whole mount nerve staining technique: A review. Biotech. Histochem. 2010, 85, 19–42. [Google Scholar] [CrossRef]
- Won, S.Y.; Kim, D.H.; Yang, H.M.; Park, J.T.; Kwak, H.H.; Hu, K.S.; Kim, H.J. Clinical and anatomical approach using Sihler’s staining technique (whole mount nerve stain). Anat. Cell. Biol. 2011, 44, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Yu, H.; Shen, B.Y.; Zhong, C.J.; Liu, E.Z.; Lin, Y.Z.; Jing, G.H. Microsurgical anatomy of the abducens nerve. Surg. Radiol. Anat. 2012, 34, 3–14. [Google Scholar] [CrossRef]
- Li, C.; Tang, Y.; Ge, H.; Lin, X.; Sun, B.; Feng, L.; Liu, S.; Liu, C.; Liang, C.; Zhang, Z.; et al. Sectional anatomy of the abducens nerve: According to 3D-SPACE magnetic resonance sequences correlated with cryosectional specimens. Surg. Radiol. Anat. 2015, 37, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Harris, F.S.; Rhoton, A.L. Anatomy of the cavernous sinus. A microsurgical study. J. Neurosurg. 1976, 45, 169–180. [Google Scholar] [CrossRef]
- Ozer, E.; Icke, C.; Arda, N. Microanatomical study of the intracranial abducens nerve: Clinical interest and surgical perspective. Turk. Neurosurg. 2010, 20, 449–456. [Google Scholar] [CrossRef] [Green Version]
- Joo, W.; Yoshioka, F.; Funaki, T.; Rhoton, A.L., Jr. Microsurgical anatomy of the abducens nerve. Clin. Anat. 2012, 25, 1030–1042. [Google Scholar] [CrossRef]
- Wysiadecki, G.; Orkisz, S.; Gałązkiewicz-Stolarczyk, M.; Brzeziński, P.; Polguj, M.; Topol, M. The abducens nerve: Its topography and anatomical variations in intracranial course with clinical commentary. Folia Morphol. 2015, 74, 236–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathan, H.; Ouaknine, G.; Kosary, I.Z. The abducens nerve. Anatomical variations in its course. J. Neurosurg. 1974, 41, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Ozveren, M.F.; Sam, B.; Akdemir, I.; Alkan, A.; Tekdemir, I.; Deda, H. Duplication of the abducens nerve at the petroclival region: An anatomic study. Neurosurgery 2003, 52, 645–652. [Google Scholar] [CrossRef]
- Coquet, T.; Lefranc, M.; Chenin, L.; Foulon, P.; Havet, É.; Peltier, J. Unilateral duplicated abducens nerve coursing through both the sphenopetroclival venous gulf and cavernous sinus: A case report. Surg. Radiol. Anat. 2018, 40, 835–840. [Google Scholar] [CrossRef]
- Wang, J.M.H.; Edwards, B.A.; Loukas, M.; Oskouian, R.J.; Tubbs, R.S. Supernumerary Abducens Nerves: A Comprehensive Review. World Neurosurg. 2018, 112, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.K. Aberrant roots of the abducent nerve. J. Neurosurg. 1964, 21, 349–351. [Google Scholar] [CrossRef] [Green Version]
- Wysiadecki, G.; Polguj, M.; Topol, M. An unusual variant of the abducens nerve duplication with two nerve trunks merging within the orbit: A case report with comments on developmental background. Surg. Radiol. Anat. 2016, 38, 625–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haładaj, R.; Wysiadecki, G.; Tubbs, R.S. Intramuscular innervation of the lateral rectus muscle evaluated using Sihler’s staining technique: Potential application to strabismus surgery. Clin. Anat. 2020, 33, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Yamashiro, T.; Yonahara, M.; Yonaha, A.; Kinoshita, R.; Tsubakimoto, M.; Iraha, R.; Murayama, S. Bilateral duplication of the abducens nerves: An incidental finding on magnetic resonance imaging. Jpn. J. Radiol. 2015, 33, 772–775. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.A.; Parkinson, D. Intracranial sympathetic pathways associated with the sixth cranial nerve. J. Neurosurg. 1974, 40, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Monro, A. The Anatomy of the Human Bones and Nerves; Hamilton & Balfour: Edinburgh, UK, 1746; pp. 362–363. [Google Scholar]
- Meckel, J.F. Manual of Anatomy; Carey & Lea: Philadelphia, PA, USA, 1832; Volume 3, pp. 88–92. [Google Scholar]
- Mariniello, G.; Annecchiarico, H.; Sardo, L.; Buonamassa, S.; de Divitiis, E. Connections of sympathetic fibres inside the cavernous sinus: A microanatomical study. Clin. Neurol. Neurosurg. 2000, 102, 1–5. [Google Scholar] [CrossRef]
- Kim, B.J.; Park, K.M. Isolated abducens nerve palsy due to internal carotid artery aneurysm. Ann. Clin. Neurophysiol. 2020, 22, 46–47. [Google Scholar] [CrossRef]
- Mendez Roberts, A.; Grimes, A.L. Enlargement of internal carotid artery aneurysm presenting with severe visual sequela: A case report and anatomy review. Optometry 2009, 80, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Elder, C.; Hainline, C.; Galetta, S.L.; Balcer, L.J.; Rucker, J.C. Isolated Abducens Nerve Palsy: Update on Evaluation and Diagnosis. Curr. Neurol. Neurosci. Rep. 2016, 16, 69. [Google Scholar] [CrossRef]
- Newman, S. A prospective study of cavernous sinus surgery for meningiomas and resultant common ophthalmic complications (an American Ophthalmological Society thesis). Trans. Am. Ophthalmol. Soc. 2007, 105, 392–447. [Google Scholar] [PubMed]
- Gatto, F.; Perez-Rivas, L.G.; Olarescu, N.C.; Khandeva, P.; Chachlaki, K.; Trivellin, G.; Gahete, M.D.; Cuny, T.; on behalf of the ENEA Young Researchers Committee (EYRC). Diagnosis and Treatment of Parasellar Lesions. Neuroendocrinology 2020, 110, 728–739. [Google Scholar] [CrossRef] [PubMed]
- Wysiadecki, G.; Radek, M.; Tubbs, R.S.; Iwanaga, J.; Walocha, J.; Brzeziński, P.; Polguj, M. Microsurgical Anatomy of the Inferomedial Paraclival Triangle: Contents, Topographical Relationships and Anatomical Variations. Brain Sci. 2021, 11, 596. [Google Scholar] [CrossRef]
- Hamel, E. Perivascular nerves and the regulation of cerebrovascular tone. J. Appl. Physiol. 1985, 100, 1059–1064. [Google Scholar] [CrossRef] [Green Version]
- Iwanaga, J.; Singh, V.; Ohtsuka, A.; Hwang, Y.; Kim, H.J.; Moryś, J.; Ravi, K.S.; Ribatti, D.; Trainor, P.A.; Sañudo, J.R. Acknowledging the use of human cadaveric tissues in research papers: Recommendations from anatomical journal editors. Clin. Anat. 2021, 34, 2–4. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specific Anatomical Variant | Number of Cases | Frequency Observed |
|---|---|---|
| Typical AN with a single trunk | 38/60 | 63.3% |
| Short division of the cavernous portion of the AN into separate rootlets (“pseudobranching”) | 15/60 | 25% |
| Duplication of the AN | 4/60 | 6.7% |
| Early division of the AN (before reaching the orbit) into separate branches | 3/60 | 5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wysiadecki, G.; Radek, M.; Tubbs, R.S.; Iwanaga, J.; Walocha, J.; Brzeziński, P.; Polguj, M. Gross and Micro-Anatomical Study of the Cavernous Segment of the Abducens Nerve and Its Relationships to Internal Carotid Plexus: Application to Skull Base Surgery. Brain Sci. 2021, 11, 649. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050649
Wysiadecki G, Radek M, Tubbs RS, Iwanaga J, Walocha J, Brzeziński P, Polguj M. Gross and Micro-Anatomical Study of the Cavernous Segment of the Abducens Nerve and Its Relationships to Internal Carotid Plexus: Application to Skull Base Surgery. Brain Sciences. 2021; 11(5):649. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050649
Chicago/Turabian StyleWysiadecki, Grzegorz, Maciej Radek, R. Shane Tubbs, Joe Iwanaga, Jerzy Walocha, Piotr Brzeziński, and Michał Polguj. 2021. "Gross and Micro-Anatomical Study of the Cavernous Segment of the Abducens Nerve and Its Relationships to Internal Carotid Plexus: Application to Skull Base Surgery" Brain Sciences 11, no. 5: 649. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050649