
A Pilot Study on Covid and Autism: Prevalence, Clinical Presentation and Vaccine Side Effects

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
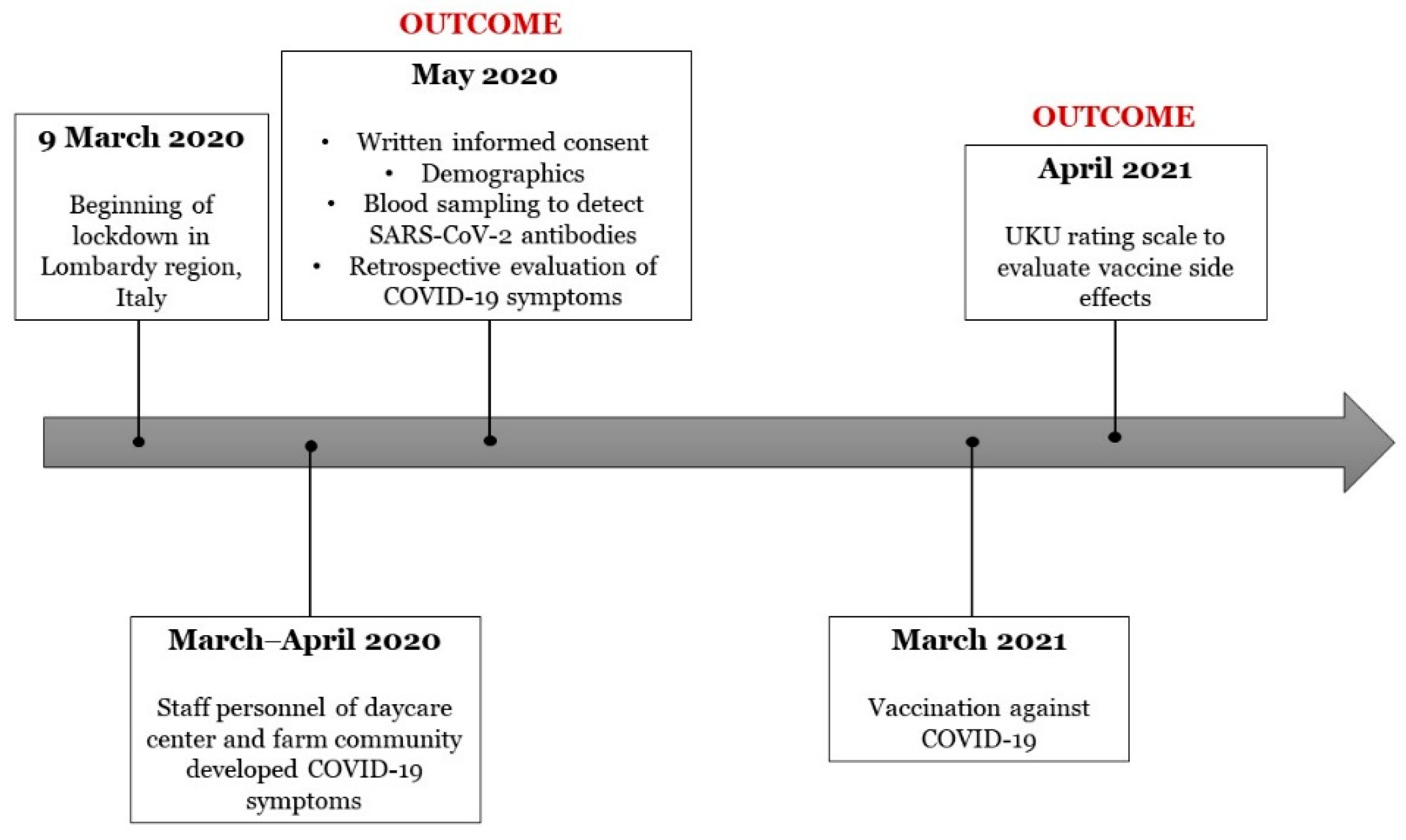
2.1. Setting
2.2. Procedures
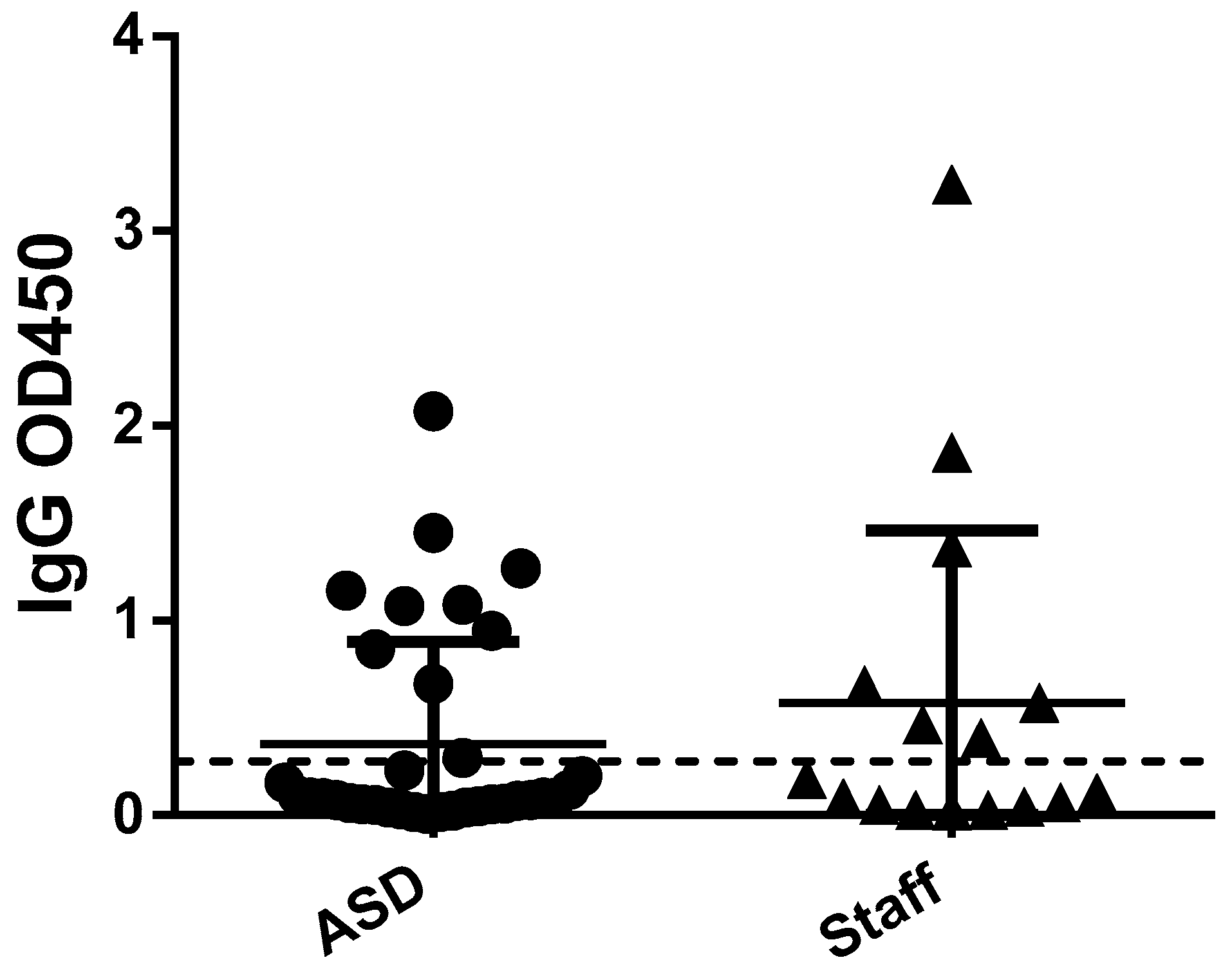
2.3. Blood Sampling and Detection of Antibodies Levels
2.4. Questionnaires
2.5. Statistical Analysis
3. Results
3.1. Susceptibility to SARS-CoV-2 Infection
3.2. Clinical Presentation
3.3. Vaccine Side Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brondino, N.; Damiani, S.; Politi, P. Effective Strategies for Managing COVID-19 Emergency Restrictions for Adults with Severe ASD in a Daycare Center in Italy. Brain Sci. 2020, 10, 436. [Google Scholar] [CrossRef]
- Sabourin, K.R.; Reynolds, A.; Schendel, D.; Rosenberg, S.; Croen, L.A.; Pinto-Martin, J.A.; Schieve, L.A.; Newschaffer, C.; Lee, L.-C.; DiGuiseppi, C. Infections in Children with Autism Spectrum Disorder: Study to Explore Early Development (SEED). Autism Res. 2018, 12, 136–146. [Google Scholar] [CrossRef]
- Lima, M.E.D.S.; Barros, L.C.M.; Aragão, G.F. Could autism spectrum disorders be a risk factor for COVID-19? Med. Hypotheses 2020, 144, 109899. [Google Scholar] [CrossRef]
- Pangrazzi, L.; Balasco, L.; Bozzi, Y. Oxidative Stress and Immune System Dysfunction in Autism Spectrum Disorders. Int. J. Mol. Sci. 2020, 21, 3293. [Google Scholar] [CrossRef]
- Masi, A.; Glozier, N.; Dale, R.; Guastella, A.J. The Immune System, Cytokines, and Biomarkers in Autism Spectrum Disorder. Neurosci. Bull. 2017, 33, 194–204. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, A.; Van De Water, J. The Role of the Immune System in Autism Spectrum Disorder. Neuropsychopharmacology 2017, 42, 284–298. [Google Scholar] [CrossRef] [Green Version]
- Fusar-Poli, L.; Brondino, N.; Rocchetti, M.; Petrosino, B.; Arillotta, D.; Damiani, S.; Provenzani, U.; Petrosino, C.; Aguglia, E.; Politi, P. Prevalence and predictors of psychotropic medication use in adolescents and adults with autism spectrum disorder in Italy: A cross-sectional study. Psychiatry Res. 2019, 276, 203–209. [Google Scholar] [CrossRef]
- May, M.; Slitzky, M.; Rostama, B.; Barlow, D.; Houseknecht, K.L. Antipsychotic-induced immune dysfunction: A consideration for COVID-19 risk. Brain Behav. Immun. Health 2020, 6, 100097. [Google Scholar] [CrossRef]
- Quincozes-Santos, A.; Rosa, R.L.; Tureta, E.F.; Bobermin, L.D.; Berger, M.; Guimarães, J.A.; Santi, L.; Beys-Da-Silva, W.O. COVID-19 impacts the expression of molecular markers associated with neuropsychiatric disorders. Brain Behav. Immun. Health 2021, 11, 100196. [Google Scholar] [CrossRef]
- Brown, G.M.; Karthikeyan, R.; Pandi-Perumal, S.R.; Cardinali, D.P. Autism Spectrum Disorder patients may be susceptible to COVID-19 disease due to deficiency in melatonin. Med. Hypotheses 2021, 149, 110544. [Google Scholar] [CrossRef]
- Grossi, E.; Terruzzi, V. Exceptionally high COVID-19 viral load and very long duration of shedding in a young pauci-symptomatic child with autism resident in an Italian nursing home. J. Infect. 2021, 82, e29–e30. [Google Scholar] [CrossRef] [PubMed]
- Nollace, L.; Cravero, C.; Abbou, A.; Mazda-Walter, B.; Bleibtreu, A.; Pereirra, N.; Sainte-Marie, M.; Cohen, D.; Giannitelli, M. Autism and COVID-19: A Case Series in a Neurodevelopmental Unit. J. Clin. Med. 2020, 9, 2937. [Google Scholar] [CrossRef]
- Faravelli, S.; Campioni, M.; Palamini, M.; Canciani, A.; Chiapparino, A.; Forneris, F. Optimized Recombinant Production of Secreted Proteins Using Human Embryonic Kidney (HEK293) Cells Grown in Suspension. Bio-Protocol 2021, 11, e3998. [Google Scholar] [CrossRef] [PubMed]
- Bruni, M.; Cecatiello, V.; Diaz-Basabe, A.; Lattanzi, G.; Mileti, E.; Monzani, S.; Pirovano, L.; Rizzelli, F.; Visintin, C.; Bonizzi, G.; et al. Persistence of Anti-SARS-CoV-2 Antibodies in Non-Hospitalized COVID-19 Convalescent Health Care Workers. J. Clin. Med. 2020, 9, 3188. [Google Scholar] [CrossRef]
- Bertoglio, F.; Meier, D.; Langreder, N.; Steinke, S.; Rand, U.; Simonelli, L.; Heine, P.A.; Ballmann, R.; Schneider, K.-T.; Roth, K.D.R.; et al. SARS-CoV-2 neutralizing human recombinant antibodies selected from pre-pandemic healthy donors binding at RBD-ACE2 interface. Nat. Commun. 2021, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lingjærde, O.; Ahlfors, U.G.; Bech, P.; Dencker, S.J.; Elgen, K. The UKU side effect rating scale: A new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic-treated patients. Acta Psychiatr. Scand. 1987, 76, 1–100. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, E.; Lipsitch, M.; Cevik, M. On the Effect of Age on the Transmission of SARS-CoV-2 in Households, Schools, and the Community. J. Infect. Dis. 2021, 223, 362–369. [Google Scholar] [CrossRef]
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef] [PubMed]
- Croonenberghs, J.; Bosmans, E.; Deboutte, D.; Kenis, G.; Maes, M. Activation of the Inflammatory Response System in Autism. Neuropsychobiology 2002, 45, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.-J.; Xu, J.; Yin, J.-M.; Li, L.; Hou, W.; Zhang, L.-L.; Zhou, Z.; Yu, Y.-Z.; Li, H.-J.; Feng, Y.-M.; et al. Lower Circulating Interferon-Gamma Is a Risk Factor for Lung Fibrosis in COVID-19 Patients. Front. Immunol. 2020, 11, 585647. [Google Scholar] [CrossRef]
- Brondino, N.; Rocchetti, M.; Fusar-Poli, L.; Damiani, S.; Goggi, A.; Chiodelli, G.; Corti, S.; Visai, L.; Politi, P. Increased CNTF levels in adults with autism spectrum disorders. World J. Biol. Psychiatry 2018, 20, 742–746. [Google Scholar] [CrossRef] [PubMed]
- Emanuele, E.; Orsi, P.; Boso, M.; Broglia, D.; Brondino, N.; Barale, F.; Di Nemi, S.U.; Politi, P. Low-grade endotoxemia in patients with severe autism. Neurosci. Lett. 2010, 471, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, A.; Sapra, L.; Saini, C.; Azam, Z.; Mishra, P.K.; Verma, B.; Mishra, G.C.; Srivastava, R.K. COVID-19: Immunology, Immunopathogenesis and Potential Therapies. Int. Rev. Immunol. 2021, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Vai, B.; Mazza, M.G.; Delli Colli, C.; Foisellee, M.; Allen, B.; Benedetti, F.; Borsini, A.; Casanova Dias, M.; Tamouza, R.; Leboyer, M.; et al. Mental disorders and risk of COVID-19 related mortality, hospitalizationand intensive care unit admission: A systematic review and meta-analysis. Lancet Psychiatry 2021. [Google Scholar] [CrossRef]
- Gerber, J.S.; Offit, P.A. Vaccines and Autism: A Tale of Shifting Hypotheses. Clin. Infect. Dis. 2009, 48, 456–461. [Google Scholar] [CrossRef] [PubMed]
- De Picker, L.J.; Dias, M.C.; Benros, M.; Vai, B.; Branchi, I.; Benedetti, F.; Borsini, A.; Leza, J.C.; Kärkkäinen, H.; Männikkö, M.; et al. Severe mental illness and European COVID-19 vaccination strategies. Lancet Psychiatry 2021, 8, 356–359. [Google Scholar] [CrossRef]
- De Picker, L.J.; Yolken, R.; Benedetti, F.; Borsini, A.; Branchi, I.; Fusar-Poli, P.; Leza, J.C.; Pariante, C.; Pollak, T.; Tamouza, R.; et al. Viewpoint|European COVID-19 exit strategy for people with severe mental disorders: Too little, but not yet too late. Brain Behav. Immun. 2021, 94, 15–17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristic | ASD Participants (n = 36) | Staff Participants (n = 35) | ASD Daycare Center (n = 14) | ASD Farm Community (n = 22) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median or n | IQR or % | Median or n | IQR or % | p-Value | Median or n | IQR or % | Median or n | IQR or % | p-Value | |
| Sex | ||||||||||
| Female | 8 | 22.2 | 25 | 71.4 | <0.001 | 2 | 14.3 | 6 | 27.3 | 0.44 |
| Male | 28 | 77.8 | 10 | 28.6 | 12 | 85.7 | 16 | 72.7 | ||
| Age | 29.5 | 24–40.75 | 38 | 28–48 | 0.01 | 24 | 18.75–27.25 | 38.5 | 29–49 | <0.001 |
| COVID-19 NHS positivity | 10 | 27.8 | 15 | 37.1 | 0.39 | 6 | 42.8 | 4 | 18.1 | 0.14 |
| COVID-19 Ab positivity a | ||||||||||
| IgG | 10 | 27.8 | 9 | 50 | 0.10 | 6 | 42.8 | 4 | 18.1 | 0.14 |
| IgA | 3 | 8.3 | 3 | 16.7 | 0.44 | 1 | 7.1 | 2 | 0.9 | 1 |
| Use of antipsychotics | 21 | 58.3 | - | - | - | 10 | 71.4 | 11 | 50 | 0.20 |
| COVID-19 symptoms | ||||||||||
| Fever | 1 | 9.1 | 12 | 92.9 | <0.001 | 1 | 7.1 | 0 | 0 | 0.39 |
| Cough | 1 | 9.1 | 12 | 92.9 | <0.001 | 1 | 7.1 | 0 | 0 | 0.39 |
| Diarrhea | 0 | 0 | 0 | 0 | - | 0 | 0 | 0 | 0 | - |
| Pneumonia/dyspnea | 0 | 0 | 2 | 15.4 | 0.23 | 0 | 0 | 0 | 0 | - |
| Hospitalization | 0 | 0 | 2 | 15.4 | 0.23 | 0 | 0 | 0 | 0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brondino, N.; Bertoglio, F.; Forneris, F.; Faravelli, S.; Borghesi, A.; Damiani, S.; Provenzani, U.; Nola, M.; Olivola, M.; Caviglia, M.; et al. A Pilot Study on Covid and Autism: Prevalence, Clinical Presentation and Vaccine Side Effects. Brain Sci. 2021, 11, 860. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070860
Brondino N, Bertoglio F, Forneris F, Faravelli S, Borghesi A, Damiani S, Provenzani U, Nola M, Olivola M, Caviglia M, et al. A Pilot Study on Covid and Autism: Prevalence, Clinical Presentation and Vaccine Side Effects. Brain Sciences. 2021; 11(7):860. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070860
Chicago/Turabian StyleBrondino, Natascia, Federico Bertoglio, Federico Forneris, Silvia Faravelli, Alessandro Borghesi, Stefano Damiani, Umberto Provenzani, Marta Nola, Miriam Olivola, Monica Caviglia, and et al. 2021. "A Pilot Study on Covid and Autism: Prevalence, Clinical Presentation and Vaccine Side Effects" Brain Sciences 11, no. 7: 860. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070860