
Glutathione as a Molecular Marker of Functional Impairment in Patients with At-Risk Mental State: 7-Tesla 1H-MRS Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
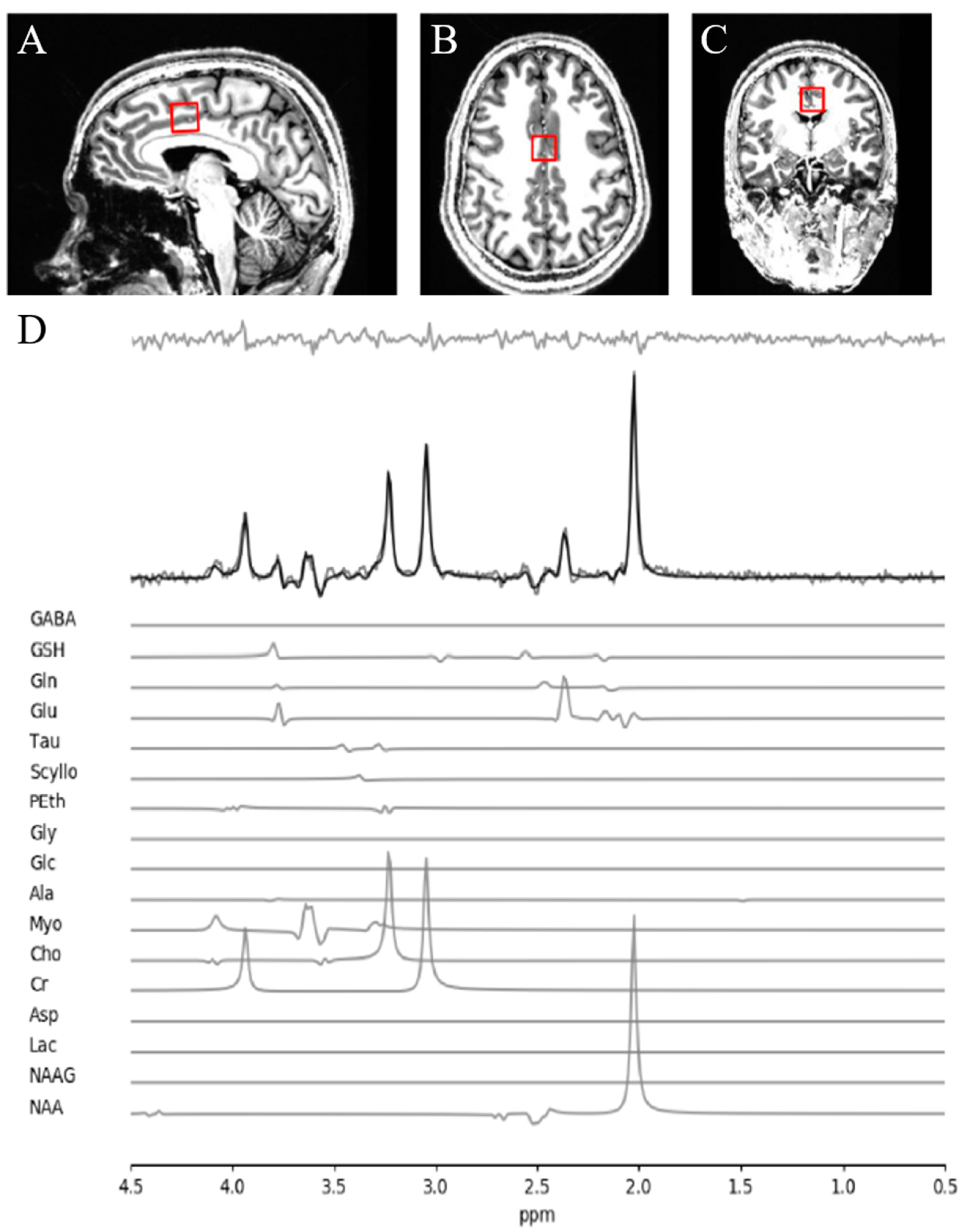
2.2. MRS Acquisition and Analysis
2.3. Clinical Assessments
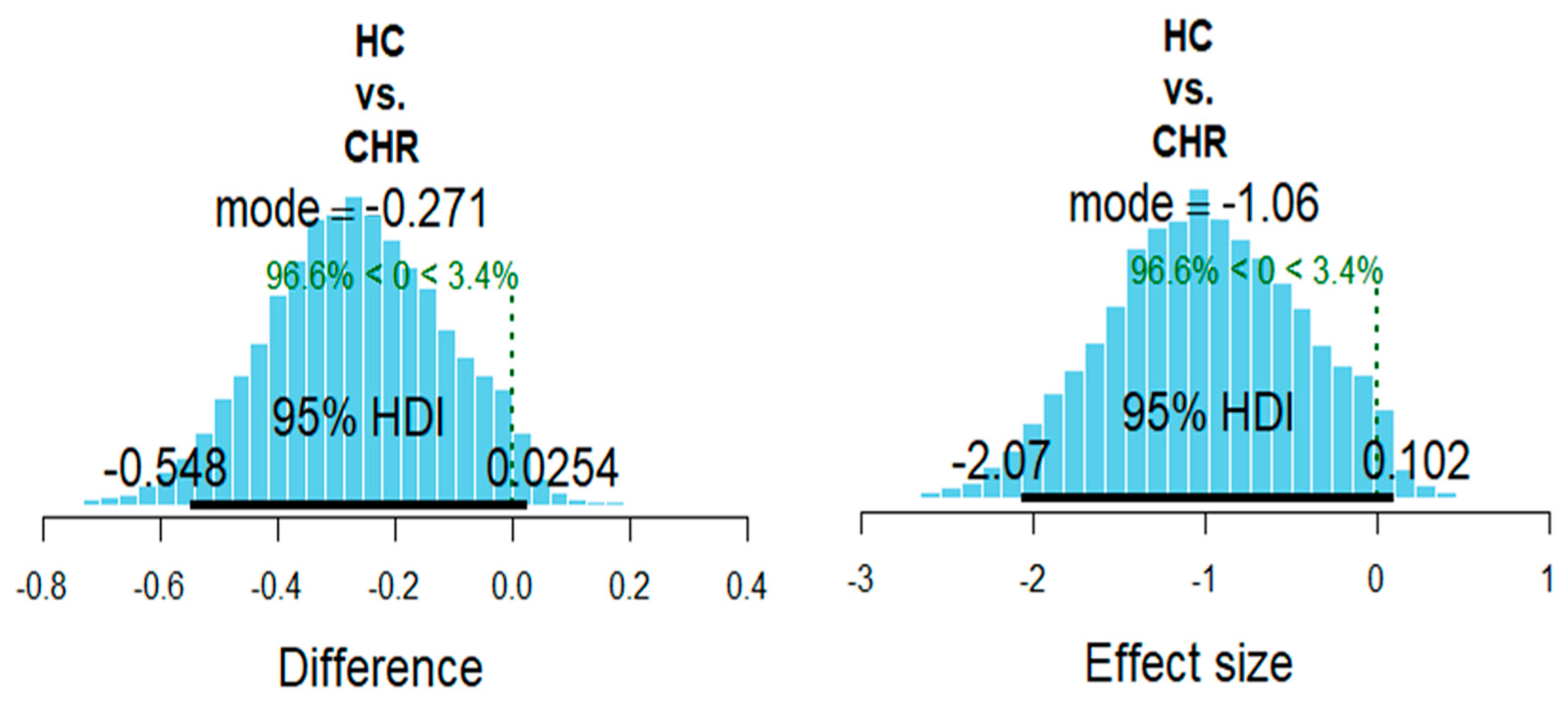
2.4. Bayesian Analysis
2.5. Frequentist Analysis
3. Results
3.1. Demographic Data
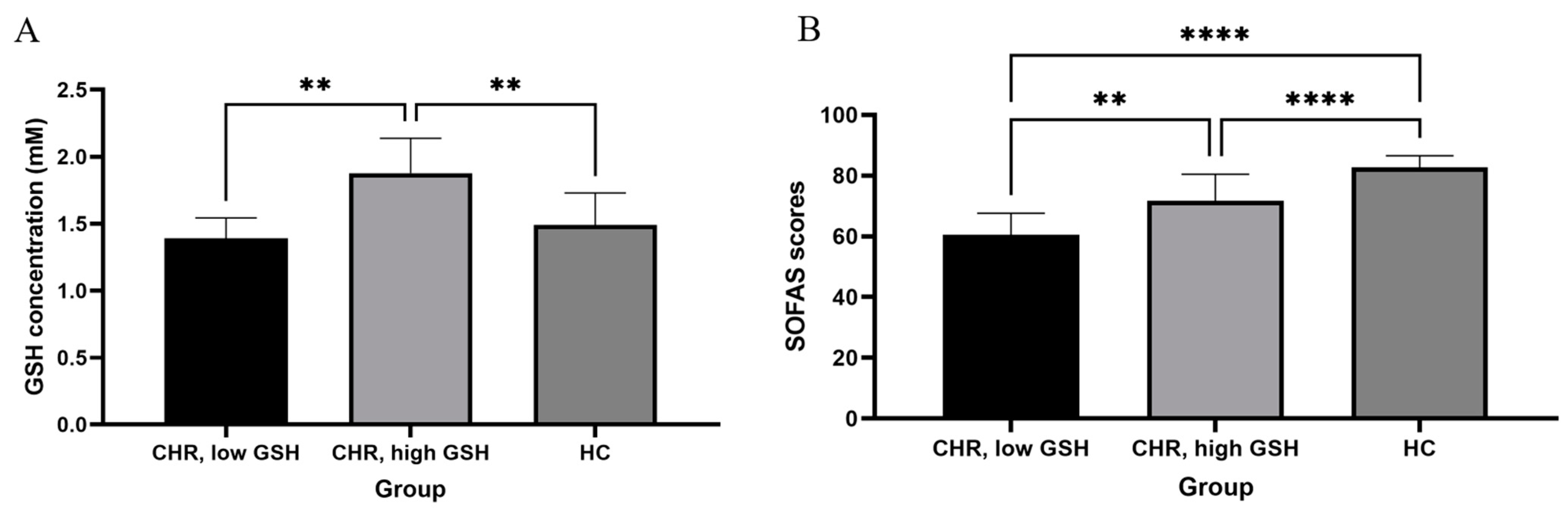
3.2. GSH, CHR Status and Social and Occupational Functioning
3.3. Frequentist Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McGorry, P.D.; Yung, A.R.; Phillips, L.J. The “Close-in” or Ultra High-Risk Model: A Safe and Effective Strategy for Research and Clinical Intervention in Prepsychotic Mental Disorder. Schizophr. Bull. 2003, 29, 771–790. [Google Scholar] [CrossRef] [Green Version]
- Yung, A.R.; McGorry, P.D. The Prodromal Phase of First-episode Psychosis: Past and Current Conceptualizations. Schizophr. Bull. 1996, 22, 353–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, K.; Studerus, E.; Andreou, C.; Egloff, L.; Leanza, L.; Simon, A.E.; Borgwardt, S.; Riecher-Rössler, A. Clinical and functional ultra-long-term outcome of patients with a clinical high risk (CHR) for psychosis. Eur. Psychiatry 2019, 62, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Carrión, R.E.; McLaughlin, D.; Goldberg, T.E.; Auther, A.M.; Olsen, R.H.; Olvet, D.M.; Correll, C.U.; Cornblatt, B.A. Prediction of Functional Outcome in Individuals at Clinical High Risk for Psychosis. JAMA Psychiatry 2013, 70, 1133. [Google Scholar] [CrossRef] [Green Version]
- Simon, A.E.; Velthorst, E.; Nieman, D.H.; Linszen, D.; Umbricht, D.; de Haan, L. Ultra high-risk state for psychosis and non-transition: A systematic review. Schizophr. Res. 2011, 132, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Rutigliano, G.; Valmaggia, L.; Landi, P.; Frascarelli, M.; Cappucciati, M.; Sear, V.; Rocchetti, M.; De Micheli, A.; Jones, C.; Palombini, E.; et al. Persistence or recurrence of non-psychotic comorbid mental disorders associated with 6-year poor functional outcomes in patients at ultra high risk for psychosis. J. Affect. Disord. 2016, 203, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Cannon, T.D. The Current State of the Clinical High Risk for Psychosis Research Paradigm. Biol. Psychiatry 2020, 88, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Flatow, J.; Buckley, P.; Miller, B.J. Meta-analysis of oxidative stress in schizophrenia. Biol. Psychiatry 2013, 74. [Google Scholar] [CrossRef] [Green Version]
- Do, K.Q.; Trabesinger, A.H.; Kirsten-Krüger, M.; Lauer, C.J.; Dydak, U.; Hell, D.; Holsboer, F.; Boesiger, P.; Cuénod, M. Schizophrenia: Glutathione deficit in cerebrospinal fluid and prefrontal cortex in vivo. Eur. J. Neurosci. 2000, 12, 3721–3728. [Google Scholar] [CrossRef]
- Yao, J.K.; Leonard, S.; Reddy, R. Altered Glutathione Redox State in Schizophrenia. Dis. Markers 2006, 22, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Gawryluk, J.W.; Wang, J.-F.; Andreazza, A.C.; Shao, L.; Young, L.T. Decreased levels of glutathione, the major brain antioxidant, in post-mortem prefrontal cortex from patients with psychiatric disorders. Int. J. Neuropsychopharmacol. 2011, 14, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Xin, L.; Mekle, R.; Fournier, M.; Baumann, P.S.; Ferrari, C.; Alameda, L.; Jenni, R.; Lu, H.; Schaller, B.; Cuenod, M.; et al. Genetic Polymorphism Associated Prefrontal Glutathione and Its Coupling With Brain Glutamate and Peripheral Redox Status in Early Psychosis. Schizophr. Bull. 2016, 42, 1185–1196. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kang, S.; Chung, J.-H.; Park, H.; Cho, K.; Park, M.-S. Genetic Polymorphisms of Glutathione-Related Enzymes (GSTM1, GSTT1, and GSTP1) and Schizophrenia Risk: A Meta-Analysis. Int. J. Mol. Sci. 2015, 16, 19602–19611. [Google Scholar] [CrossRef] [Green Version]
- Gysin, R.; Kraftsik, R.; Sandell, J.; Bovet, P.; Chappuis, C.; Conus, P.; Deppen, P.; Preisig, M.; Ruiz, V.; Steullet, P.; et al. Impaired glutathione synthesis in schizophrenia: Convergent genetic and functional evidence. Proc. Natl. Acad. Sci. USA 2007, 104, 16621–16626. [Google Scholar] [CrossRef] [Green Version]
- Tosic, M.; Ott, J.; Barral, S.; Bovet, P.; Deppen, P.; Gheorghita, F.; Matthey, M.-L.; Parnas, J.; Preisig, M.; Saraga, M.; et al. Schizophrenia and Oxidative Stress: Glutamate Cysteine Ligase Modifier as a Susceptibility Gene. Am. J. Hum. Genet. 2006, 79, 586–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matigian, N.; Abrahamsen, G.; Sutharsan, R.; Cook, A.L.; Vitale, A.M.; Nouwens, A.; Bellette, B.; An, J.; Anderson, M.; Beckhouse, A.G.; et al. Disease-specific, neurosphere-derived cells as models for brain disorders. Dis. Model. Mech. 2010, 3, 785–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, D.O.; Jeffries, C.D.; Do, K.Q. Potential Roles of Redox Dysregulation in the Development of Schizophrenia. Biol. Psychiatry 2020, 88, 326–336. [Google Scholar] [CrossRef]
- Dempster, K.; Jeon, P.; MacKinley, M.; Williamson, P.; Théberge, J.; Palaniyappan, L. Early treatment response in first episode psychosis: A 7-T magnetic resonance spectroscopic study of glutathione and glutamate. Mol. Psychiatry 2020, 25, 1640–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, M.; Naber, D.; Schacht, A.; Wagner, T.; Hundemer, H.-P.; Karow, A.; Huber, C.G.; Suarez, D.; Haro, J.M.; Novick, D.; et al. Rates and predictors of remission and recovery during 3 years in 392 never-treated patients with schizophrenia. Acta Psychiatr. Scand. 2008, 118, 220–229. [Google Scholar] [CrossRef]
- Derks, E.M.; Fleischhacker, W.W.; Boter, H.; Peuskens, J.; Kahn, R.S. Antipsychotic Drug Treatment in First-Episode Psychosis should patients be switched to a different antipsychotic drug after 2, 4, or 6 weeks of nonresponse? J. Clin. Psychopharmacol. 2010, 30, 176–180. [Google Scholar] [CrossRef]
- Carbon, M.; Correll, C.U. Clinical predictors of therapeutic response to antipsychotics in schizophrenia. Dialogues Clin. Neurosci. 2014, 16, 505–524. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Liddle, E.B.; Fernandes, C.C.; Palaniyappan, L.; Hall, E.L.; Robson, S.E.; Simmonite, M.; Fiesal, J.; Katshu, M.Z.; Qureshi, A.; et al. Glutathione and glutamate in schizophrenia: A 7T MRS study. Mol. Psychiatry 2020, 25, 873–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuzawa, D.; Obata, T.; Shirayama, Y.; Nonaka, H.; Kanazawa, Y.; Yoshitome, E.; Takanashi, J.; Matsuda, T.; Shimizu, E.; Ikehira, H.; et al. Negative Correlation between Brain Glutathione Level and Negative Symptoms in Schizophrenia: A 3T 1H-MRS Study. PLoS ONE 2008, 3, e1944. [Google Scholar] [CrossRef]
- Wang, A.M.; Pradhan, S.; Coughlin, J.M.; Trivedi, A.; DuBois, S.L.; Crawford, J.L.; Sedlak, T.W.; Nucifora, F.C.; Nestadt, G.; Nucifora, L.G.; et al. Assessing Brain Metabolism With 7-T Proton Magnetic Resonance Spectroscopy in Patients With First-Episode Psychosis. JAMA Psychiatry 2019, 76, 314. [Google Scholar] [CrossRef] [PubMed]
- Steullet, P.; Cabungcal, J.H.; Monin, A.; Dwir, D.; O’Donnell, P.; Cuenod, M.; Do, K.Q. Redox dysregulation, neuroinflammation, and NMDA receptor hypofunction: A “central hub” in schizophrenia pathophysiology? Schizophr. Res. 2016, 176, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Maas, D.A.; Vallès, A.; Martens, G.J.M. Oxidative stress, prefrontal cortex hypomyelination and cognitive symptoms in schizophrenia. Transl. Psychiatry 2017, 7, e1171. [Google Scholar] [CrossRef] [Green Version]
- Worthington, M.A.; Cao, H.; Cannon, T.D. Discovery and Validation of Prediction Algorithms for Psychosis in Youths at Clinical High Risk. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2020, 5, 738–747. [Google Scholar] [CrossRef]
- Fornito, A.; Yung, A.R.; Wood, S.J.; Phillips, L.J.; Nelson, B.; Cotton, S.; Velakoulis, D.; McGorry, P.D.; Pantelis, C.; Yücel, M. Anatomic Abnormalities of the Anterior Cingulate Cortex Before Psychosis Onset: An MRI Study of Ultra-High-Risk Individuals. Biol. Psychiatry 2008, 64, 758–765. [Google Scholar] [CrossRef]
- Takayanagi, Y.; Kulason, S.; Sasabayashi, D.; Takahashi, T.; Katagiri, N.; Sakuma, A.; Obara, C.; Nakamura, M.; Kido, M.; Furuichi, A.; et al. Reduced Thickness of the Anterior Cingulate Cortex in Individuals With an At-Risk Mental State Who Later Develop Psychosis. Schizophr. Bull. 2017, 43, 907–913. [Google Scholar] [CrossRef]
- Pantelis, C.; Velakoulis, D.; McGorry, P.D.; Wood, S.J.; Suckling, J.; Phillips, L.J.; Yung, A.R.; Bullmore, E.T.; Brewer, W.; Soulsby, B.; et al. Neuroanatomical abnormalities before and after onset of psychosis: A cross-sectional and longitudinal MRI comparison. Lancet 2003, 361, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Witthaus, H.; Kaufmann, C.; Bohner, G.; Özgürdal, S.; Gudlowski, Y.; Gallinat, J.; Ruhrmann, S.; Brüne, M.; Heinz, A.; Klingebiel, R.; et al. Gray matter abnormalities in subjects at ultra-high risk for schizophrenia and first-episode schizophrenic patients compared to healthy controls. Psychiatry Res. Neuroimaging 2009, 173, 163–169. [Google Scholar] [CrossRef]
- Whalley, H.C.; Simonotto, E.; Moorhead, W.; McIntosh, A.; Marshall, I.; Ebmeier, K.P.; Owens, D.G.C.; Goddard, N.H.; Johnstone, E.C.; Lawrie, S.M. Functional Imaging as a Predictor of Schizophrenia. Biol. Psychiatry 2006, 60, 454–462. [Google Scholar] [CrossRef]
- Sabb, F.W.; van Erp, T.G.M.; Hardt, M.E.; Dapretto, M.; Caplan, R.; Cannon, T.D.; Bearden, C.E. Language network dysfunction as a predictor of outcome in youth at clinical high risk for psychosis. Schizophr. Res. 2010, 116, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Morey, R.A.; Inan, S.; Mitchell, T.V.; Perkins, D.O.; Lieberman, J.A.; Belger, A. Imaging Frontostriatal Function in Ultra-High-Risk, Early, and Chronic Schizophrenia During Executive Processing. Arch. Gen. Psychiatry 2005, 62, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreou, C.; Borgwardt, S. Structural and functional imaging markers for susceptibility to psychosis. Mol. Psychiatry 2020, 25, 2773–2785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liloia, D.; Brasso, C.; Cauda, F.; Mancuso, L.; Nani, A.; Manuello, J.; Costa, T.; Duca, S.; Rocca, P. Updating and characterizing neuroanatomical markers in high-risk subjects, recently diagnosed and chronic patients with schizophrenia: A revised coordinate-based meta-analysis. Neurosci. Biobehav. Rev. 2021, 123, 83–103. [Google Scholar] [CrossRef] [PubMed]
- Das, T.K.; Javadzadeh, A.; Dey, A.; Sabesan, P.; Théberge, J.; Radua, J.; Palaniyappan, L. Antioxidant defense in schizophrenia and bipolar disorder: A meta-analysis of MRS studies of anterior cingulate glutathione. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 91, 94–102. [Google Scholar] [CrossRef]
- Romeo, B.; Petillion, A.; Martelli, C.; Benyamina, A. Magnetic resonance spectroscopy studies in subjects with high risk for psychosis: A meta-analysis and review. J. Psychiatr. Res. 2020, 125, 52–65. [Google Scholar] [CrossRef]
- Da Silva, T.; Hafizi, S.; Andreazza, A.C.; Kiang, M.; Bagby, R.M.; Navas, E.; Laksono, I.; Truong, P.; Gerritsen, C.; Prce, I.; et al. Glutathione, the Major Redox Regulator, in the Prefrontal Cortex of Individuals at Clinical High Risk for Psychosis. Int. J. Neuropsychopharmacol. 2018, 21, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Miller, T.J.; McGlashan, T.H.; Rosen, J.L.; Cadenhead, K.; Ventura, J.; McFarlane, W.; Perkins, D.O.; Pearlson, G.D.; Woods, S.W. Prodromal Assessment with the Structured Interview for Prodromal Syndromes and the Scale of Prodromal Symptoms: Predictive Validity, Interrater Reliability, and Training to Reliability. Schizophr. Bull. 2003, 29, 703–715. [Google Scholar] [CrossRef] [Green Version]
- Tkáć, I.; Gruetter, R. Methodology of1H NMR spectroscopy of the human brain at very high magnetic fields. Appl. Magn. Reson. 2005, 29, 139–157. [Google Scholar] [CrossRef]
- Near, J.; Edden, R.; Evans, C.J.; Paquin, R.; Harris, A.; Jezzard, P. Frequency and phase drift correction of magnetic resonance spectroscopy data by spectral registration in the time domain. Magn. Reson. Med. 2015, 73, 44–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartha, R.; Drost, D.J.; Menon, R.S.; Williamson, P.C. Spectroscopic lineshape correction by QUECC: Combined QUALITY deconvolution and eddy current correction. Magn. Reson. Med. 2000, 44, 641–645. [Google Scholar] [CrossRef]
- van den Boogaart, A.; Ala-Korpela, M.; Jokisaari, J.; Griffiths, J.R. Time and frequency domain analysis of NMR data compared: An application to 1D1H spectra of lipoproteins. Magn. Reson. Med. 1994, 31, 347–358. [Google Scholar] [CrossRef]
- Bartha, R.; Drost, D.J.; Williamson, P.C. Factors affecting the quantification of short echoin-vivo1H MR spectra: Prior knowledge, peak elimination, and filtering. NMR Biomed. 1999, 12, 205–216. [Google Scholar] [CrossRef]
- Wong, D. MRI Investigations of Metabolic and Structural Brain Changes in Alzheimer’s Disease and Vitamin D Deprivation. Ph.D. Thesis, The University of Western Ontario, London, ON, Canada, 2019. [Google Scholar]
- Rybarczyk, B. Social and Occupational Functioning Assessment Scale (SOFAS). In Encyclopedia of Clinical Neuropsychology; Springer: Cham, Switzerland, 2018; p. 3206. [Google Scholar]
- Stentebjerg-Olesen, M.; Jeppesen, P.; Pagsberg, A.K.; Fink-Jensen, A.; Kapoor, S.; Chekuri, R.; Carbon, M.; Al-Jadiri, A.; Kishimoto, T.; Kane, J.M.; et al. Early Nonresponse Determined by the Clinical Global Impressions Scale Predicts Poorer Outcomes in Youth with Schizophrenia Spectrum Disorders Naturalistically Treated with Second-Generation Antipsychotics. J. Child Adolesc. Psychopharmacol. 2013, 23, 665–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT Alcohol Consumption Questions (AUDIT-C): An Effective Brief Screening Test for Problem Drinking. Arch. Intern. Med. 1998, 158, 1789. [Google Scholar] [CrossRef] [Green Version]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.-O. The Fagerstrom Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Addiction 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Skinner, H.A. The drug abuse screening test. Addict. Behav. 1982, 7, 363–371. [Google Scholar] [CrossRef]
- van Doorn, J.; Ly, A.; Marsman, M.; Wagenmakers, E.-J. Bayesian rank-based hypothesis testing for the rank sum test, the signed rank test, and Spearman’s . J. Appl. Stat. 2020, 47, 2984–3006. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0; IBM: Armonk, NY, USA, 2019. [Google Scholar]
- Limongi, R.; Jeon, P.; Théberge, J.; Palaniyappan, L. Counteracting Effects of Glutathione on the Glutamate-Driven Excitation/Inhibition Imbalance in First-Episode Schizophrenia: A 7T MRS and Dynamic Causal Modeling Study. Antioxidants 2021, 10, 75. [Google Scholar] [CrossRef]
- Limongi, R.; Jeon, P.; Mackinley, M.; Das, T.; Dempster, K.; Théberge, J.; Bartha, R.; Wong, D.; Palaniyappan, L. Glutamate and Dysconnection in the Salience Network: Neurochemical, Effective Connectivity, and Computational Evidence in Schizophrenia. Biol. Psychiatry 2020, 88, 273–281. [Google Scholar] [CrossRef]
- Pan, Y.; Dempster, K.; Jeon, P.; Théberge, J.; Khan, A.R.; Palaniyappan, L. Acute conceptual disorganization in untreated first-episode psychosis: A combined magnetic resonance spectroscopy and diffusion imaging study of the cingulum. J. Psychiatry Neurosci. 2021, 46, E337–E346. [Google Scholar] [CrossRef] [PubMed]
- Perkins, D.O.; Jeffries, C.D.; Cornblatt, B.A.; Woods, S.W.; Addington, J.; Bearden, C.E.; Cadenhead, K.S.; Cannon, T.D.; Heinssen, R.; Mathalon, D.H.; et al. Severity of thought disorder predicts psychosis in persons at clinical high-risk. Schizophr. Res. 2015, 169, 169–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-Madrigal, F.; León-Ortiz, P.; Mao, X.; Mora-Durán, R.; Shungu, D.C.; de la Fuente-Sandoval, C. Striatal Glutathione in First-episode Psychosis Patients Measured In Vivo with Proton Magnetic Resonance Spectroscopy. Arch. Med. Res. 2019, 50, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.; Sousa, C.; Costa, A.; Andrade, P.; Valentão, P. Glutathione and the Antioxidant Potential of Binary Mixtures with Flavonoids: Synergisms and Antagonisms. Molecules 2013, 18, 8858–8872. [Google Scholar] [CrossRef] [Green Version]
- Yagishita, Y.; Gatbonton-Schwager, T.N.; McCallum, M.L.; Kensler, T.W. Current Landscape of NRF2 Biomarkers in Clinical Trials. Antioxidants 2020, 9, 716. [Google Scholar] [CrossRef]
- Zalachoras, I.; Hollis, F.; Ramos-Fernández, E.; Trovo, L.; Sonnay, S.; Geiser, E.; Preitner, N.; Steiner, P.; Sandi, C.; Morató, L. Therapeutic potential of glutathione-enhancers in stress-related psychopathologies. Neurosci. Biobehav. Rev. 2020, 114, 134–155. [Google Scholar] [CrossRef] [PubMed]
- Yolland, C.O.B.; Hanratty, D.; Neill, E.; Rossell, S.L.; Berk, M.; Dean, O.M.; Castle, D.J.; Tan, E.J.; Phillipou, A.; Harris, A.W.F.; et al. Meta-analysis of randomised controlled trials with N -acetylcysteine in the treatment of schizophrenia. Aust. New Zeal. J. Psychiatry 2020, 54, 453–466. [Google Scholar] [CrossRef]
- Kishi, T.; Miyake, N.; Okuya, M.; Sakuma, K.; Iwata, N. N-acetylcysteine as an adjunctive treatment for bipolar depression and major depressive disorder: A systematic review and meta-analysis of double-blind, randomized placebo-controlled trials. Psychopharmacology (Berl) 2020, 237. [Google Scholar] [CrossRef]
- Fernandes, B.S.; Dean, O.M.; Dodd, S.; Malhi, G.S.; Berk, M. N-acetylcysteine in depressive symptoms and functionality: A systematic review and meta-analysis. J. Clin. Psychiatry 2016, 77, e457–e466. [Google Scholar] [CrossRef] [PubMed]
- Conus, P.; Seidman, L.J.; Fournier, M.; Xin, L.; Cleusix, M.; Baumann, P.S.; Ferrari, C.; Cousins, A.; Alameda, L.; Gholam-Rezaee, M.; et al. N-acetylcysteine in a Double-Blind Randomized Placebo-Controlled Trial: Toward Biomarker-Guided Treatment in Early Psychosis. Schizophr. Bull. 2018, 44, 317–327. [Google Scholar] [CrossRef] [Green Version]
- Wong, D.; Schranz, A.L.; Bartha, R. Optimized in vivo brain glutamate measurement using long-echo-time semi-LASER at 7 T. NMR Biomed. 2018, 31, e4002. [Google Scholar] [CrossRef] [PubMed]
- Reid, M.A.; Salibi, N.; White, D.M.; Gawne, T.J.; Denney, T.S.; Lahti, A.C. 7T Proton Magnetic Resonance Spectroscopy of the Anterior Cingulate Cortex in First-Episode Schizophrenia. Schizophr. Bull. 2019, 45, 180–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermens, D.F.; Lagopoulos, J.; Naismith, S.L.; Tobias-Webb, J.; Hickie, I.B. Distinct neurometabolic profiles are evident in the anterior cingulate of young people with major psychiatric disorders. Transl. Psychiatry 2012, 2, e110. [Google Scholar] [CrossRef] [Green Version]
- Fusar-Poli, P.; Bonoldi, I.; Yung, A.R.; Borgwardt, S.; Kempton, M.J.; Valmaggia, L.; Barale, F.; Caverzasi, E.; McGuire, P. Predicting psychosis: Meta-analysis of transition outcomes in individuals at high clinical risk. Arch. Gen. Psychiatry 2012, 69, 220. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Clinical High Risk (N = 13) | Healthy Controls (N = 30) | t/χ2 | p |
|---|---|---|---|---|
| Gender (male/female) | 11/2 | 19/11 | 1.948 | 0.163 |
| Marital status (Mar/S) | 1/12 | 2/28 | 0.009 | 0.926 |
| Age (M/SD) | 22.2/4.0 | 21.8/3.7 | −0.330 | 0.745 |
| Parental NS-SEC (M/SD) | 3.54/0.88 | 3.03/1.38 | −1.444 | 0.158 |
| Cannabis use (Y/N) | 6/7 | 1/29 | 4.926 | 0.026 |
| Antidepressant use (Y/N) | 3/10 | - | ||
| Benzodiazepine use (Y/N) | 2/11 | - | ||
| Antipsychotic use (Y/N) | 1/12 | - | ||
| SOPS, total (M/SD) | 8.4/5.0 | - | ||
| CAST, total (M/SD) | 11.4/7.8 | 6.2/0.8 | −2.20 | 0.052 |
| Audit—C, total (M/SD) | 5.5/3.8 | 5.9/2.5 | 0.281 | 0.783 |
| SOFAS (M/SD) APS/BLIPS Converted (Y/N) | 67.7/9.5 13/0 3/10 | 82.7/3.8 | 6.267 | 0.000 |
| Parameter | Mean | Median | Mode | HDIlow | HDIhigh |
|---|---|---|---|---|---|
| 0.849 | 0.842 | 0.823 | −0.165 | 1.875 | |
| β[CHR] | 0.135 | 0.135 | 0.135 | −0.013 | 0.274 |
| β[HC] | −0.135 | −0.135 | −0.135 | −0.274 | 0.013 |
| βSOFAS | 0.009 | 0.010 | 0.010 | −0.004 | 0.023 |
| σβ | 0.440 | 0.335 | 0.199 | 0.000 | 1.155 |
| σi | 0.270 | 0.267 | 0.264 | 0.212 | 0.332 |
| [HC]SOFAS | 0.154 | 0.143 | 0.114 | −0126 | 0.378 |
| [CHR]SOFAS | 0.478 | 0.509 | 0.586 | 0.045 | 0.769 |
| [CHR]SOPS | −0.073 | −0.076 | −0.171 | −0.335 | 0.196 |
| [CHR]CAST | 0.201 | 0.207 | 0.315 | −0.124 | 0.500 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, P.; Limongi, R.; Ford, S.D.; Branco, C.; Mackinley, M.; Gupta, M.; Powe, L.; Théberge, J.; Palaniyappan, L. Glutathione as a Molecular Marker of Functional Impairment in Patients with At-Risk Mental State: 7-Tesla 1H-MRS Study. Brain Sci. 2021, 11, 941. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070941
Jeon P, Limongi R, Ford SD, Branco C, Mackinley M, Gupta M, Powe L, Théberge J, Palaniyappan L. Glutathione as a Molecular Marker of Functional Impairment in Patients with At-Risk Mental State: 7-Tesla 1H-MRS Study. Brain Sciences. 2021; 11(7):941. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070941
Chicago/Turabian StyleJeon, Peter, Roberto Limongi, Sabrina D. Ford, Cassandra Branco, Michael Mackinley, Maya Gupta, Laura Powe, Jean Théberge, and Lena Palaniyappan. 2021. "Glutathione as a Molecular Marker of Functional Impairment in Patients with At-Risk Mental State: 7-Tesla 1H-MRS Study" Brain Sciences 11, no. 7: 941. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070941