
Transcranial Direct Current Stimulation (tDCS) for Depression during Pregnancy: Results from an Open-Label Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. tDCS
2.4. Rating Instruments
2.5. Statistics
3. Results
3.1. Clinical and Demographic Characteristics
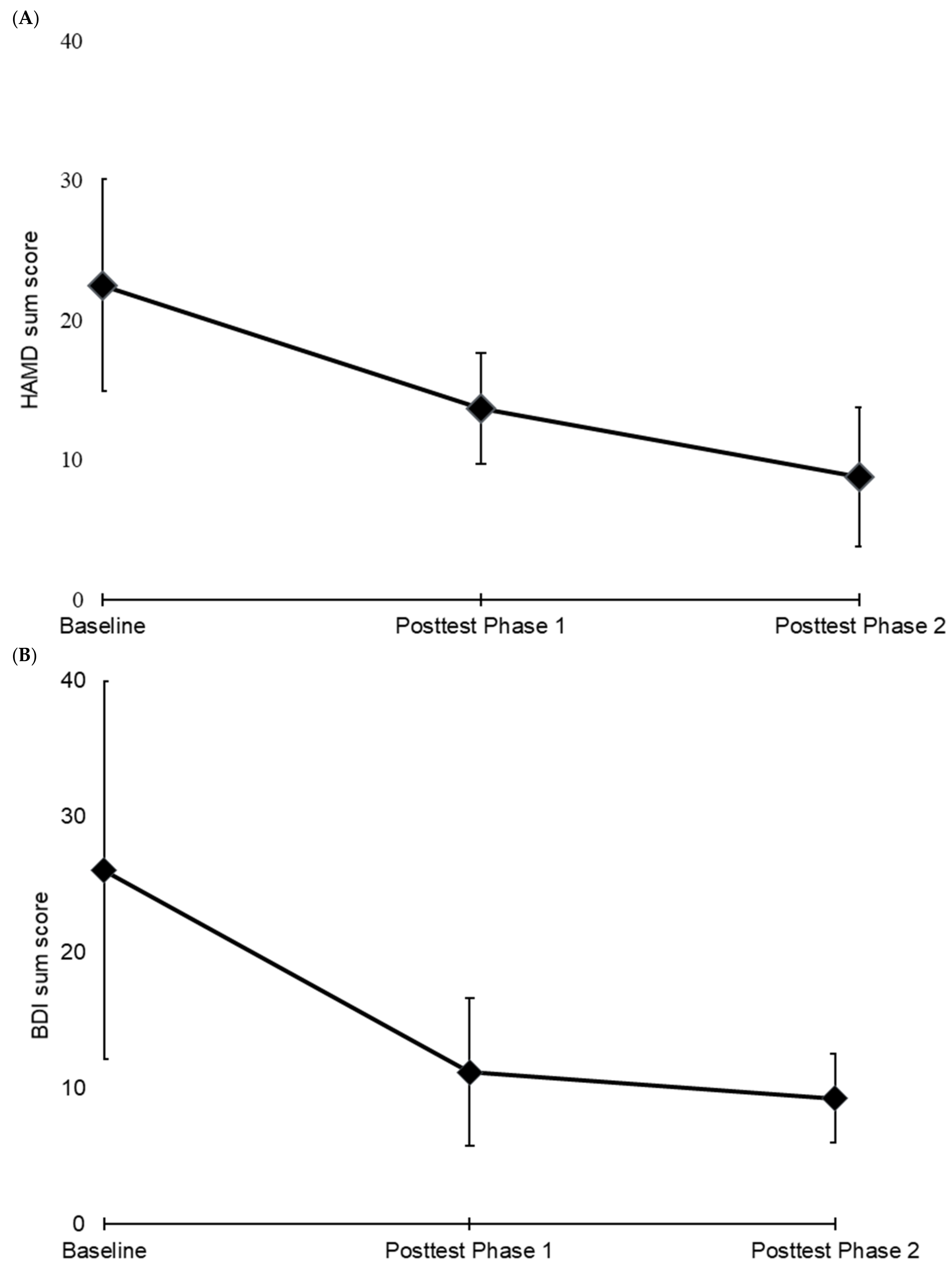
3.2. Primary and Secondary Outcome Measures
3.3. Side Effects and Adverse Events
3.4. Follow-Up
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grigoriadis, S.; VonderPorten, E.H.; Mamisashvili, L.; Tomlinson, G.; Dennis, C.-L.; Koren, G.; Steiner, M.; Mousmanis, P.; Cheung, A.; Radford, K.; et al. The Impact of Maternal Depression during Pregnancy on Perinatal Outcomes. J. Clin. Psychiatry 2013, 74, e321–e341. [Google Scholar] [CrossRef] [PubMed]
- Muzik, M.; Marcus, S.M.; Heringhausen, J.E.; Flynn, H. When Depression Complicates Childbearing: Guidelines for Screening and Treatment During Antenatal and Postpartum Obstetric Care. Obst. Gynecol. Clin. N. Am. 2009, 26, 771–788. [Google Scholar] [CrossRef] [Green Version]
- Robertson, E.; Grace, S.; Wallington, T.; Stewart, D.E. Antenatal risk factors for postpartum depression: A synthesis of recent literature. Gen. Hosp. Psychiatry 2004, 26, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Vigod, S.N.; Wilson, C.A.; Howard, L. Depression in pregnancy. BMJ 2016, 352, i1547. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.; Pearson, R.M.; Goodman, S.H.; Rapa, E.; Rahman, A.; McCallum, M.; Howard, L.M.; Pariante, C.M. Effects of perinatal mental disorders on the fetus and child. Lancet 2014, 384, 1800–1819. [Google Scholar] [CrossRef]
- Paszkiel, S.; Dobrakowski, P.; Łysiak, A. The Impact of Different Sounds on Stress Level in the Context of EEG, Cardiac Measures and Subjective Stress Level: A Pilot Study. Brain Sci. 2020, 10, 728. [Google Scholar] [CrossRef]
- Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance; NICE: Manchester, UK, 2014.
- MacQueen, G.M.; Frey, B.N.; Ismail, Z.; Jaworska, N.; Steiner, M.; Van Lieshout, R.J.; Kennedy, S.; Lam, R.W.; Milev, R.V.; Parikh, S.V.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder. Can. J. Psychiatry 2016, 61, 588–603. [Google Scholar] [CrossRef] [Green Version]
- Ross, L.E.; Grigoriadis, S.; Mamisashvili, L.; VonderPorten, E.H.; Roerecke, M.; Rehm, J.; Dennis, C.-L.; Koren, G.; Steiner, M.; Mousmanis, P.; et al. Selected Pregnancy and Delivery Outcomes after Exposure to Antidepressant Medication. JAMA Psychiatry 2013, 70, 436. [Google Scholar] [CrossRef] [Green Version]
- Casper, R.C.; Fleisher, B.E.; Lee-Ancajas, J.C.; Gilles, A.; Gaylor, E.; DeBattista, A. Follow-up of children of depressed mothers exposed or not exposed to antidepressant drugs during pregnancy. J. Pediatr. 2003, 142, 402–408. [Google Scholar] [CrossRef] [Green Version]
- Alwan, S.; Bandoli, G.; Chambers, C.D. Maternal use of selective serotonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. Clin. Pharmacol. Ther. 2016, 100, 34–41. [Google Scholar] [CrossRef]
- Wen, S.W.; Yang, Q.; Garner, P.; Fraser, W.; Olatunbosun, O.; Nimrod, C.; Walker, M. Selective serotonin reuptake inhibitors and adverse pregnancy outcomes. Am. J. Obstet. Gynecol. 2006, 194, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Hasan, A.; Strube, W.; Padberg, F. tDCS for the treatment of depression: A comprehensive review. Eur. Arch. Psychiatry Clin. Neurosci. 2016, 266, 681–694. [Google Scholar] [CrossRef] [PubMed]
- Grimm, S.; Beck, J.; Schuepbach, D.; Hell, D.; Boesiger, P.; Bermpohl, F.; Niehaus, L.; Boeker, H.; Northoff, G. Imbalance between Left and Right Dorsolateral Prefrontal Cortex in Major Depression Is Linked to Negative Emotional Judgment: An fMRI Study in Severe Major Depressive Disorder. Biol. Psychiatry 2008, 63, 369–376. [Google Scholar] [CrossRef]
- Fales, C.L.; Barch, D.M.; Rundle, M.M.; Mintun, M.A.; Mathews, J.; Snyder, A.Z.; Sheline, Y.I. Antidepressant treatment normalizes hypoactivity in dorsolateral prefrontal cortex during emotional interference processing in major depression. J. Affect Disord. 2009, 112, 206–211. [Google Scholar] [CrossRef] [Green Version]
- Martin, D.M.; Moffa, A.; Nikolin, S.; Bennabi, D.; Brunoni, A.R.; Flannery, W. Cognitive effects of transcranial direct current stimulation treatment in patients with major depressive disorder: An individual patient data meta-analysis of randomised, sham-controlled trials. Neurosci. Biobehav. Rev. 2018, 90, 137–145. [Google Scholar] [CrossRef]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antal, A.; Alekseichuk, I.; Bikson, M.; Brockmöller, J.; Brunoni, A.R.; Chen, R.; Cohen, L.G.; Dowthwaite, G.; Ellrich, J.; Flöel, A.; et al. Low intensity transcranial electric stimulation: Safety, ethical, legal regulatory and application guidelines. Clin. Neurophysiol. 2017, 128, 1774–1809. [Google Scholar] [CrossRef] [Green Version]
- Brunoni, A.R.; Amadera, J.; Berbel, B.; Volz, M.S.; Rizzerio, B.G.; Fregni, F. A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int. J. Neuropsychopharmacol 2011, 14, 1133–1145. [Google Scholar] [CrossRef]
- Sreeraj, V.S.; Bose, A.; Shanbhag, V.; Narayanaswamy, J.C.; Venkatasubramanian, G.; Benegal, V. Monotherapy With tDCS for Treatment of Depressive Episode during Pregnancy: A Case Report. Brain Stimul. 2016, 9, 457–458. [Google Scholar] [CrossRef]
- Vigod, S.N.; Murphy, K.E.; Dennis, C.-L.; Oberlander, T.F.; Ray, J.G.; Daskalakis, Z.J.; Blumberger, D.M. Transcranial direct current stimulation (tDCS) for depression in pregnancy: A pilot randomized controlled trial. Brain Stimul. 2019, 12, 1475–1483. [Google Scholar] [CrossRef]
- Kurzeck, A.K.; Kirsch, B.; Weidinger, E.; Padberg, F.; Palm, U. Transcranial Direct Current Stimulation (tDCS) for Depression during Pregnancy: Scientific Evidence and What Is Being Said in the Media-A Systematic Review. Brain Sci. 2018, 8, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palm, U.; Goerigk, S.; Kirsch, B.; Bäumler, L.; Sarubin, N.; Hasan, A.; Brunoni, A.R.; Padberg, F. Treatment of major depression with a two-step tDCS protocol add-on to SSRI: Results from a naturalistic study. Brain Stimul. 2019, 12, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Feichtner, K.B.; Hasan, A.; Gauglitz, G.; Langguth, B.; Nitsche, M.A.; Keeser, D.; Padberg, F. The role of contact media at the skin-electrode interface during transcranial direct current stimulation (tDCS). Brain Stimul. 2014, 7, 762–764. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Valiengo, L.; Baccaro, A.; Zanão, T.A.; De Oliveira, J.F.; Goulart, A.; Boggio, P.; Lotufo, P.; Benseñor, I.M.; Fregni, F. The Sertraline vs. Electrical Current Therapy for Treating Depression Clinical Study. JAMA Psychiatry 2013, 70, 383. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Moffa, A.H.; Sampaio-Junior, B.; Borrione, L.; Moreno, M.L.; Fernandes, R.A.; Veronezi, B.P.; Nogueira, B.S.; Aparicio, L.V.; Razza, L.B.; et al. Trial of Electrical Direct-Current Therapy versus Escitalopram for Depression. N. Engl. J. Med. 2017, 76, 2523–2533. [Google Scholar] [CrossRef]
- Wilkening, A.; Kurzeck, A.; Dechantsreiter, E.; Padberg, F.; Palm, U. Transcranial alternating current stimulation for the treatment of major depression during pregnancy. Psychiatry Res. 2019, 279, 399–400. [Google Scholar] [CrossRef]
- Bennabi, D.; Haffen, E. Transcranial Direct Current Stimulation (tDCS): A Promising Treatment for Major Depressive Disorder? Brain Sci. 2018, 8, 81. [Google Scholar] [CrossRef] [Green Version]
- Palm, U.; Leitner, B.; Strube, W.; Hasan, A.; Padberg, F. Safety of Repeated Twice-daily 30 Minutes of 2 mA tDCS in Depressed Patients. Int. Neuropsychiatr. Dis. J. 2015, 4, 168–171. [Google Scholar] [CrossRef] [Green Version]
- Moffa, A.H.; Brunoni, A.R.; Fregni, F.; Palm, U.; Padberg, F.; Blumberger, D.M.; Daskalakis, Z.J.; Bennabi, D.; Haffen, E.; Alonzo, A.; et al. Safety and acceptability of transcranial direct current stimulation for the acute treatment of major depressive episodes: Analysis of individual patient data. J. Affect Disord. 2017, 221, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Moffa, A.H.; Fregni, F.; Palm, U.; Padberg, F.; Blumberger, D.M.; Daskalakis, Z.J.; Bennabi, D.; Haffen, E.; Alonzo, A.; et al. Transcranial direct current stimulation for acute major depressive episodes: Meta-analysis of individual patient data. Br. J. Psychiatry 2016, 208, 522–531. [Google Scholar] [CrossRef] [Green Version]
- Konstantinou, G.; Vigod, S.N.; Mehta, S.; Daskalakis, Z.J.; Blumberger, D.M. A systematic review of non-invasive neurostimulation for the treatment of depression during pregnancy. J. Affect Disord. 2020, 272, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Kumpf, U.; Behler, N.; Wulf, L.; Kirsch, B.; Wörsching, J.; Keeser, D.; Hasan, A.; Padberg, F. Home Use, Remotely Supervised, and Remotely Controlled Transcranial Direct Current Stimulation: A Systematic Review of the Available Evidence. Neuromodulation 2018, 21, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Phase 1 (n = 6) | Phase 2 (n =4) | |
|---|---|---|
| Female patients | 6 | 4 |
| Tobacco use | 1 | 0 |
| Handedness (R/L) | 6/0 | 4/0 |
| Years of education (y) | 12.8 ± 3.3 | 13.8 ± 3.4 |
| Mean age (y) | 32.5 ± 6.8 | 30.0 ± 5.6 |
| Age range (y) | 23–43 | 23–35 |
| Age of onset (y) | 26.3 ± 4.7 | 26.0 ± 6.1 |
| Mean gestational week at enrolment | 22.8 ± 7.9 | 18.3 ± 4.3 |
| Range of gestational week at enrolment | 12–33 | 14–21 |
| Course of depression (episodic/continuous) | 3/3 | 2/2 |
| Mean duration of illness (y) | 6.2 ± 6.1 | 4.1 ± 4.8 |
| Number of episodes | 2.0 ± 1.0 | 2.0 ± 1.2 |
| Duration of episodes (months)/range | 7.5 ± 10.5/1–26 | 9.12 ± 11.4/3–26 |
| Total mean duration of hospitalization (months) | 1.8 ± 1.9 | 1.1 ± 1.4 |
| Current mean duration of hospitalization (months) | 0.9 ± 2.0 | 1.1 ± 1.4 |
| HAMD | BDI | TMT-A/B | CGI Item 1 | WHOQOL | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TMT-A | TMT-B | Overall Quality of Life | General Health | Physical Health | Psychological Health | Social Relationships | Environmental Quality of Life | |||||
| PHASE 1 | Mean Baseline Phase 1 (t = pre-tDCS. n = 6) | 22.50 ± 7.56 | 26.00 ± 13.90 | 28.47 ± 5.98 | 77.10 ± 36.22 | 4.66 ± 0.82 | 3.33 ± 1.21 | 3.17 ± 0.98 | 45.24 ± 20.91 | 37.50 ± 19.72 | 52.78 ± 27.22 | 58.34 ± 16.96 |
| Mean score (t = post 2 weeks tDCS. n = 6) | 13.67 ± 3.93 (p = 0.009) ** | 11.17 ± 5.46 (p = 0.038) * | 34.27 ± 23.67 (p = 0.564) | 76.73 ± 40.06 (p = 0.980) | 3.33 ± 0.52 (p = 0.001) ** | 4.17 ± 0.41 (p = 0.141) | 4.33 ± 0.52 (p = 0.058) | 61.90 ± 20.16 (p = 0.105) | 58.33 ± 16.24 (p = 0.040) * | 59.72 ± 20.01 (p = 0.419) | 63.03 ± 18.37 (p = 0.369) | |
| Change Phase 1 (%) | 39.26% | −57.05% | 20.39% | −0.48% | −28.57% | 25.00% | 36.84% | 36.84% | 55.56% | 13.16% | 8.04% | |
| Response/Remission | 2 Responses/0 Remission | 2 Responses/1 Remission | ||||||||||
| PHASE 2 | Mean Baseline Phase 2 (t = post 2 weeks tDCS. n = 4) | 13.50 ± 1.29 | 13.75 ± 2.50 | 34.33 ± 30.56 | 52.29 ± 15.74 | 3.25 ± 0.50 | 4.25 ± 0.50 | 4.50 ± 0.58 | 57.14 ± 21.23 | 57.29 ± 14.18 | 64.58 ± 12.50 | 61.72 ± 17.93 |
| Mean score (t = post 4 weeks tDCS. n = 4) | 8.75 ± 4.99 (p = 0.113) | 9.25 ± 3.30 (p = 0.174) | 19.33 ± 3.20 (p = 0.382) | 49.91 ± 16.54 (p = 0.379) | 3.00 ± 0.82 (p = 0.638) | 3.75 ± 0.50 (p = 0.182) | 4.00 ± 0.82 (p = 0.182) | 71.43 ± 12.37 (p = 0.278) | 68.16 ± 8.27 (p = 0.320) | 66.67 ± 26.35 (p = 0.809) | 67.97 ± 23.44 (p = 0.116) | |
| Change Phase 2 (%) | −35.19% | −32.73% | −43.69% | −4.54% | −7.69% | 11.76% | 81.86% | 25.00% | 18.96% | 3.23% | 10.12% | |
| Response/Remission | 0 Response/1 Remission | 0 Response/1 Remission | ||||||||||
| PHASE 1 + 2 | Mean Baseline Phase 1 + 2 (t = pre-tDCS. n = 4) | 20.75 ± 4.93 | 26.00 ± 10.30 | 25.79 ± 4.91 | 62.90 ± 21.02 | 4.75 ± 0.96 | 3.75 ± 0.50 | 3.25 ± 0.96 | 42.86 ± 23.87 | 36.46 ± 12.44 | 54.17 ± 22.05 | 54.69 ±17.95 |
| Mean score (t = post 4 weeks tDCS. n = 4) | 8.75 ± 4.99 (p = 0.058) | 9.25 ± 3.30 (p = 0.061) | 19.33 ± 3.20 (p = 0.016) * | 49.91 ± 16.54 (p = 0.139) | 3.00 ± 0.82 (p = 0.035) * | 3.75 ± 0.50 (p = 1.000) | 4.00 ± 0.82 (p = 0.391) | 71.43 ± 12.37 (p = 0.165) | 68.16 ± 8.27 (p = 0.043) * | 66.67 ± 26.35 (p = 0.495) | 67.97 ± 23.44 (p = 0.224) | |
| Change Phase 1 + 2 (%) | −57.83% | −64.42% | −25.04% | −20.65% | −36.84% | 0.00% | 23.08% | 66.66% | 86.94% | 23.08% | 24.29% | |
| Response/Remission | 2 Responses/1 Remission | 1 Response/1 Remission | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurzeck, A.K.; Dechantsreiter, E.; Wilkening, A.; Kumpf, U.; Nenov-Matt, T.; Padberg, F.; Palm, U. Transcranial Direct Current Stimulation (tDCS) for Depression during Pregnancy: Results from an Open-Label Pilot Study. Brain Sci. 2021, 11, 947. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070947
Kurzeck AK, Dechantsreiter E, Wilkening A, Kumpf U, Nenov-Matt T, Padberg F, Palm U. Transcranial Direct Current Stimulation (tDCS) for Depression during Pregnancy: Results from an Open-Label Pilot Study. Brain Sciences. 2021; 11(7):947. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070947
Chicago/Turabian StyleKurzeck, Anna Katharina, Esther Dechantsreiter, Anja Wilkening, Ulrike Kumpf, Tabea Nenov-Matt, Frank Padberg, and Ulrich Palm. 2021. "Transcranial Direct Current Stimulation (tDCS) for Depression during Pregnancy: Results from an Open-Label Pilot Study" Brain Sciences 11, no. 7: 947. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070947