
Substance Use Outcomes from Two Formats of a Cognitive-Behavioral Intervention for Aggressive Children: Moderating Roles of Inhibitory Control and Intervention Engagement

 ,
,
Abstract
:1. Introduction
1.1. Prevention and Treatment of Substance Use in Aggressive Youth
1.1.1. Coping Power
1.1.2. Moderators of Coping Power Group Intervention for Aggressive Children
Child Inhibitory Control
Child Intervention Engagement
1.2. The Current Study
2. Method
2.1. Sample
2.2. Intervention
2.3. Procedure
2.4. Measures
2.4.1. Inhibitory Control
2.4.2. Substance Use
2.4.3. Group Behavior
2.5. Analytic Strategy
3. Results
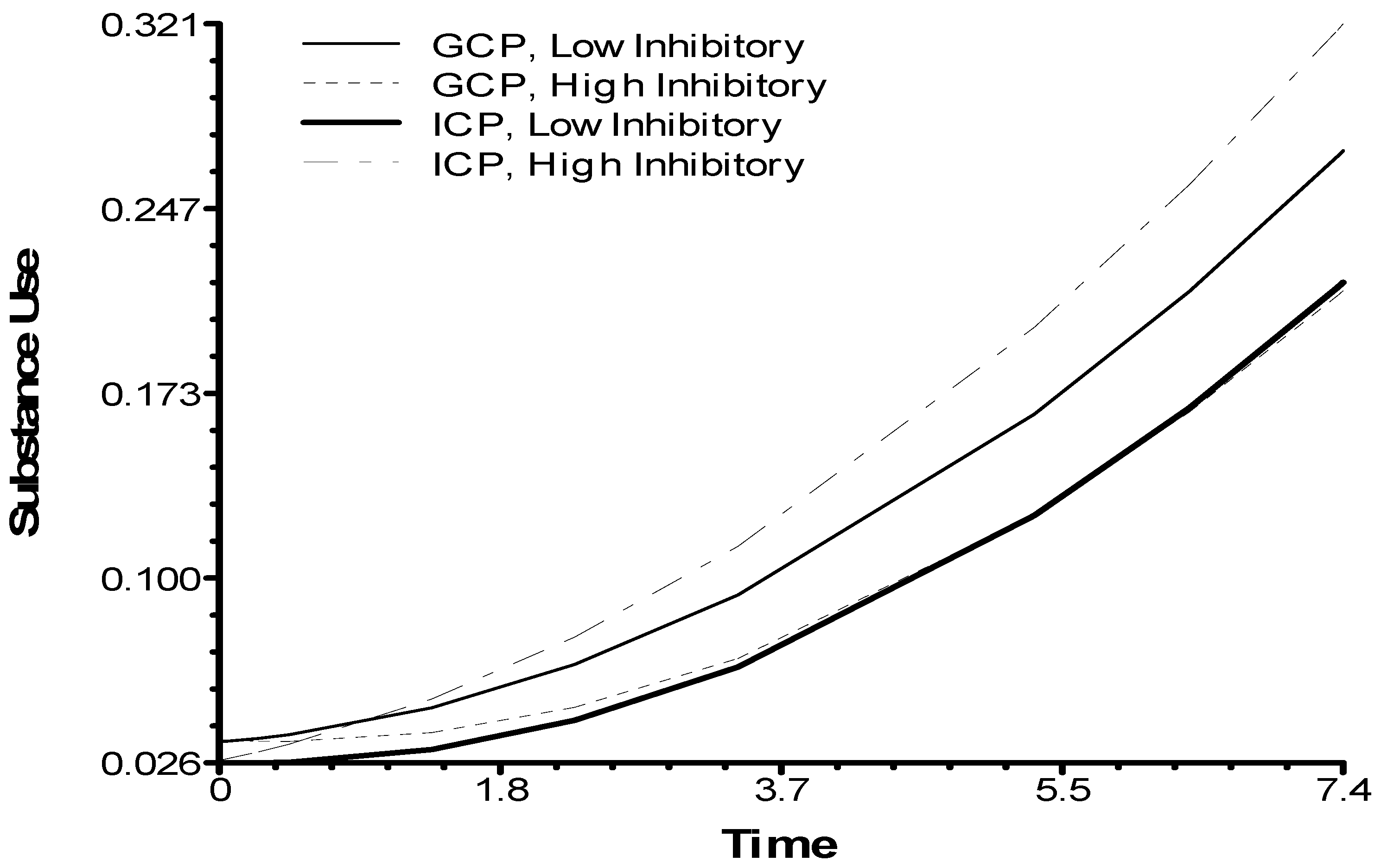
3.1. Hypothesized Moderation Effect of Inhibitory Control on ICP Versus GCP
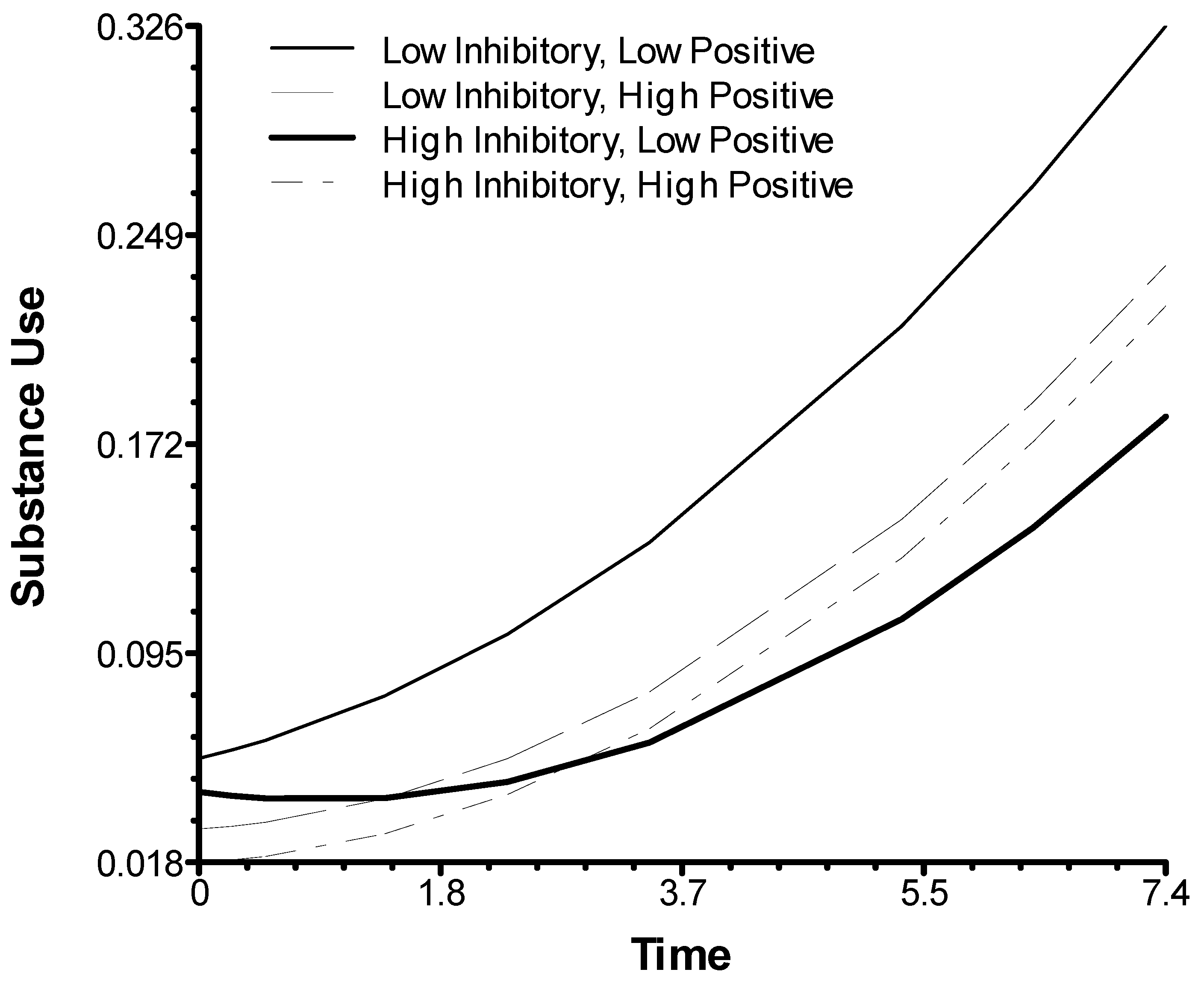
3.2. Child In-Session Behaviors Predicting Substance Use within the GCP Condition
4. Discussion
4.1. Effects of Group Versus Individual Format of Cognitive-Behavioral Intervention
4.2. Interaction of Children’s Inhibitory Control and Their Behavioral Engagement in Groups
4.3. Limitations and Future Directions
4.4. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williams, R.J.; Nowatzki, N.R. Validity of adolescent self report of substance use. Subst. Use Misuse 2005, 40, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conner, B.T.; Lochman, J.E. Comorbid conduct disorder and substance use disorders. Clin. Psychol. Sci. Pract. 2010, 17, 337–349. [Google Scholar] [CrossRef]
- Marmorstein, N.R.; White, H.R. Comorbidity with substance abuse. In The Wiley Handbook of Disruptive and Impulse-Control Disorders; Lochman, J.E., Matthys, W., Eds.; Wiley Blackwell: Hoboken, NJ, USA, 2018; pp. 73–88. [Google Scholar]
- Lansford, J.E.; Godwin, J.; McMahon, R.J.; Crowley, M.; Pettit, G.S.; Bates, J.E.; Coie, J.D.; Dodge, K.A. Early Physical Abuse and Adult Outcomes. Pediatrics 2021, 147, e20200873. [Google Scholar] [CrossRef]
- Groenman, A.P.; Janssen, T.; Oosterlaan, J. Childhood Psychiatric Disorders as Risk Factor for Subsequent Substance Abuse: A Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Trucco, E.M.; Hicks, B.M.; Villafuerte, S.; Nigg, J.T.; Burmeister, M.; Zucker, R.A. Temperament and externalizing behavior as mediators of genetic risk on adolescent substance use. J. Abnorm. Psychol. 2016, 125, 565–575. [Google Scholar] [CrossRef]
- Tanner-Smith, E.E.; Wilson, S.J.; Lipsey, M.W. The comparative effectiveness of outpatient treatment for adolescent substance abuse: A meta-analysis. J. Subst. Abus. Treat. 2013, 44, 145–158. [Google Scholar] [CrossRef] [Green Version]
- Baldwin, S.A.; Christian, S.; Berkeljon, A.; Shadish, W.R. The Effects of Family Therapies for Adolescent Delinquency and Substance Abuse: A Meta-analysis. J. Marital Fam. Ther. 2011, 38, 281–304. [Google Scholar] [CrossRef]
- Henggeler, S.W.; Borduin, C.M.; Melton, G.B.; Mann, B.J. Effects of multisystemic therapy on drug use and abuse in serious juvenile offenders: A progress report from two outcome studies. Fam. Dyn. Addict. Q. 1991, 1, 40–51. [Google Scholar]
- Letourneau, E.J.; Henggeler, S.W.; Borduin, C.M.; Schewe, P.A.; McCart, M.R.; Chapman, J.E.; Saldana, L. Multisystemic therapy for juvenile sexual offenders: 1-year results from a randomized effectiveness trial. J. Fam. Psychol. 2009, 23, 89–102. [Google Scholar] [CrossRef]
- Timmons-Mitchell, J.; Bender, M.B.; Kishna, M.A.; Mitchell, C.C. An Independent Effectiveness Trial of Multisystemic Therapy with Juvenile Justice Youth. J. Clin. Child Adolesc. Psychol. 2006, 35, 227–236. [Google Scholar] [CrossRef]
- Henggeler, S.W.; McCart, M.R.; Cunningham, P.B.; Chapman, J.E. Enhancing the effectiveness of juvenile drug courts by integrating evidence-based practices. J. Consult. Clin. Psychol. 2012, 80, 264–275. [Google Scholar] [CrossRef]
- Godwin, J.W. The Fast Track intervention’s impact on behaviors of despair in adolescence and young adulthood. Proc. Natl. Acad. Sci. USA 2020, 117, 31748–31753. [Google Scholar] [CrossRef] [PubMed]
- Das, J.K.; Salam, R.A.; Arshad, A.; Finkelstein, Y.; Bhutta, Z.A. Interventions for adolescent substance abuse: An overview of systematic reviews. J. Adolesc. Health 2016, 59 (Suppl. 4), S61–S75. [Google Scholar] [CrossRef] [Green Version]
- Griffin, K.W.; Botvin, G.J. Evidence-Based interventions for preventing substance use disorders in adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 2010, 19, 505–526. [Google Scholar] [CrossRef] [Green Version]
- Botvin, G.J.; Baker, E.; Dusenbury, L.; Botvin, E.M.; Diaz, T. Long-term Follow-up Results of a Randomized Drug Abuse Prevention Trial in a White Middle-Class Population. JAMA 1995, 273, 1106–1112. [Google Scholar] [CrossRef]
- Dishion, T.J.; Kavanagh, K.; Schneiger, A.; Nelson, S.; Kaufman, N.K. Preventing Early Adolescent Substance Use: A Family-Centered Strategy for the Public Middle School. Prev. Sci. 2002, 3, 191–201. [Google Scholar] [CrossRef]
- Ialongo, N.; Poduska, J.; Werthamer, L.; Kellam, S. The Distal Impact of Two First-Grade Preventive Interventions on Conduct Problems and Disorder in Early Adolescence. J. Emot. Behav. Disord. 2001, 9, 146–160. [Google Scholar] [CrossRef] [Green Version]
- Lochman, J.E.; Wells, K.C. The Coping Power Program for Preadolescent Aggressive Boys and Their Parents: Outcome Effects at the 1-Year Follow-Up. J. Consult. Clin. Psychol. 2004, 72, 571–578. [Google Scholar] [CrossRef] [Green Version]
- Larson, J.; Lochman, J.E. Helping Schoolchildren Cope with Anger: A Cognitive-Behavioral Intervention; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Lochman, J.E. Cognitive-Behavioral intervention with aggressive boys: Three-year follow-up and preventive effects. J. Consult. Clin. Psychol. 1992, 60, 426–432. [Google Scholar] [CrossRef]
- Lochman, J.E.; Wells, K.C.; Lenhart, L.A. Coping Power: Child Group Program Workbook; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Wells, K.C.; Lochman, J.E.; Lenhart, L.A. Coping Power: Parent Group Program Workbook; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Lochman, J.E.; Wells, K.C. The Coping Power program at the middle-school transition: Universal and indicated prevention effects. Psychol. Addict. Behav. 2002, 16, S40–S54. [Google Scholar] [CrossRef] [PubMed]
- Lochman, J.E.; Wells, K.C. Effectiveness of the coping power program and of classroom intervention with aggressive children: Outcomes at a 1-year follow-up. Behav. Ther. 2003, 34, 493–515. [Google Scholar] [CrossRef]
- Helander, M.; Lochman, J.; Högström, J.; Ljótsson, B.; Hellner, C.; Enebrink, P. The effect of adding Coping Power Program-Sweden to Parent Management Training-effects and moderators in a randomized controlled trial. Behav. Res. Ther. 2018, 103, 43–52. [Google Scholar] [CrossRef]
- Muratori, P.; Milone, A.; Levantini, V.; Ruglioni, L.; Lambruschi, F.; Pisano, S.; Masi, G.; Lochman, J.E. Six-year outcome for children with ODD or CD treated with the coping power program. Psychiatry Res. 2019, 271, 454–458. [Google Scholar] [CrossRef]
- Muratori, P.; Milone, A.; Manfredi, A.; Polidori, L.; Ruglioni, L.; Lambruschi, F.; Masi, G.; Lochman, J.E. Evaluation of Improvement in Externalizing Behaviors and Callous-Unemotional Traits in Children with Disruptive Behavior Disorder: A 1-Year Follow Up Clinic-Based Study. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 44, 452–462. [Google Scholar] [CrossRef]
- Nystrand, C.; Helander, M.; Enebrink, P.; Feldman, I.; Sampaio, F. Adding the Coping Power Programme to parent management training: The cost-effectiveness of stacking interventions for children with disruptive behaviour disorders. Eur. Child Adolesc. Psychiatry 2020, 1–12. [Google Scholar] [CrossRef]
- Pullen, S.J.; Horgan, L.; Romanelli, L.H.; Radin, A.; Gardner, K.; Edwards, C.; Crapo, T.; Bolen, B.; Huck, B.; Wells, K.; et al. The effectiveness of training rural mental health clinicians to treat disruptive behavior disorders. J. Rural. Ment. Health 2021. [Google Scholar] [CrossRef]
- Cowell, K.; Horstmann, S.; Linebarger, J.; Meaker, P.; Aligne, C.A. A “Vaccine” against violence: Coping Power. Pediatr. Rev. 2008, 29, 362–363. [Google Scholar] [CrossRef]
- Eiraldi, R.; Mautone, J.A.; Khanna, M.S.; Power, T.J.; Orapallo, A.; Cacia, J.; Schwartz, B.S.; McCurdy, B.; Keiffer, J.; Paidipati, C.; et al. Group CBT for Externalizing Disorders in Urban Schools: Effect of Training Strategy on Treatment Fidelity and Child Outcomes. Behav. Ther. 2018, 49, 538–550. [Google Scholar] [CrossRef] [PubMed]
- Jurecska, D.E.; Hamilton, E.B.; Peterson, M.A. Effectiveness of the Coping Power Program in middle-school children with disruptive behaviours and hyperactivity difficulties. Support Learn. 2011, 26, 168–172. [Google Scholar] [CrossRef] [Green Version]
- Lochman, J.E.; Boxmeyer, C.; Powell, N.; Qu, L.; Wells, K.; Windle, M. Dissemination of the Coping Power program: Importance of intensity of counselor training. J. Consult. Clin. Psychol. 2009, 77, 397–409. [Google Scholar] [CrossRef] [PubMed]
- McDaniel, S.C.; Lochman, J.E.; Tomek, S.; Powell, N.; Irwin, A.; Kerr, S. Reducing Risk for Emotional and Behavioral Disorders in Late Elementary School: A Comparison of Two Targeted Interventions. Behav. Disord. 2018, 43, 370–382. [Google Scholar] [CrossRef]
- Peterson, M.A.; Hamilton, E.B.; Russell, A.D. Starting well: Facilitating the middle school transition. J. Appl. Sch. Psychol. 2009, 25, 286–304. [Google Scholar] [CrossRef] [Green Version]
- Cabiya, J.J.; Padilla-Cotto, L.; González, K.; Sanchez-Cestero, J.; Martínez-Taboas, A.; Sayers, S. Effectiveness of a cognitive-behavioral intervention for Puerto Rican children. Rev. Interam. Psicol. 2008, 42, 195–202. [Google Scholar]
- Ludmer, J.A.; Sanches, M.; Propp, L.; Andrade, B.F. Comparing the Multicomponent Coping Power Program to Individualized Parent–Child Treatment for Improving the Parenting Efficacy and Satisfaction of Parents of Children with Conduct Problems. Child Psychiatry Hum. Dev. 2017, 49, 100–108. [Google Scholar] [CrossRef]
- Mushtaq, A.; Lochman, J.E.; Tariq, P.N.; Sabih, F. Preliminary Effectiveness Study of Coping Power Program for Aggressive Children in Pakistan. Prev. Sci. 2016, 18, 762–771. [Google Scholar] [CrossRef]
- Zonnevylle-Bender, M.J.S.; Matthys, W.; Van De Wiel, N.M.H.; Lochman, J.E. Preventive Effects of Treatment of Disruptive Behavior Disorder in Middle Childhood on Substance Use and Delinquent Behavior. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 33–39. [Google Scholar] [CrossRef]
- Tremblay, R.E.; Mâsse, L.C.; Vitaro, F.; Dobkin, P.L. The impact of friends’ deviant behavior on early onset of deliquency: Longitudinal data from 6 to 13 years of age. Dev. Psychopathol. 1995, 7, 649–667. [Google Scholar] [CrossRef]
- Price, J.; Drabick, D.A.; Ridenour, T.A. Association with Deviant Peers Across Adolescence: Subtypes, Developmental Patterns, and Long-Term Outcomes. J. Clin. Child Adolesc. Psychol. 2019, 48, 238–249. [Google Scholar] [CrossRef]
- Dishion, T.J.; Andrews, D.W. Preventing escalation in problem behaviors with high-risk young adolescents: Immediate and 1-year outcomes. J. Consult. Clin. Psychol. 1995, 63, 538–548. [Google Scholar] [CrossRef]
- Poulin, F.; Dishion, T.J.; Burraston, B. 3-Year Iatrogenic Effects Associated with Aggregating High-Risk Adolescents in Cognitive-Behavioral Preventive Interventions. Appl. Dev. Sci. 2001, 5, 214–224. [Google Scholar] [CrossRef]
- Dishion, T.J.; Tipsord, J.M. Peer Contagion in Child and Adolescent Social and Emotional Development. Annu. Rev. Psychol. 2011, 62, 189–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lochman, J.E.; Dishion, T.J.; Powell, N.P.; Boxmeyer, C.L.; Qu, L.; Sallee, M. Evidence-Based preventive intervention for preadolescent aggressive children: One-year outcomes following randomization to group versus individual delivery. J. Consult. Clin. Psychol. 2015, 83, 728–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lochman, J.E.; Glenn, A.L.; Powell, N.P.; Boxmeyer, C.L.; Bui, C.; Kassing, F.; Qu, L.; Romerro, D.E.; Dishion, T. Group versus individual format of intervention for aggressive children: Moderators and predictors of outcomes through 4 years after intervention. Dev. Psychopathol. 2019, 31, 1757–1775. [Google Scholar] [CrossRef] [PubMed]
- Glenn, A.L.; Lochman, J.E.; Dishion, T.; Powell, N.P.; Boxmeyer, C.; Qu, L. Oxytocin Receptor Gene Variant Interacts with Intervention Delivery Format in Predicting Intervention Outcomes for Youth with Conduct Problems. Prev. Sci. 2018, 19, 38–48. [Google Scholar] [CrossRef]
- Glenn, A.L.; Lochman, J.E.; Dishion, T.; Powell, N.P.; Boxmeyer, C.; Kassing, F.; Qu, L.; Romero, D. Toward Tailored Interventions: Sympathetic and Parasympathetic Functioning Predicts Responses to an Intervention for Conduct Problems Delivered in Two Formats. Prev. Sci. 2018, 20, 30–40. [Google Scholar] [CrossRef]
- Lochman, J.E.; Dishion, T.J.; Boxmeyer, C.L.; Powell, N.P.; Qu, L. Variation in Response to Evidence-Based Group Preventive Intervention for Disruptive Behavior Problems: A View from 938 Coping Power Sessions. J. Abnorm. Child Psychol. 2017, 45, 1271–1284. [Google Scholar] [CrossRef] [PubMed]
- Enticott, P.; Ogloff, J.; Bradshaw, J.L. Associations between laboratory measures of executive inhibitory control and self-reported impulsivity. Personal. Individ. Differ. 2006, 41, 285–294. [Google Scholar] [CrossRef]
- Rothbart, M.K. Temperament in childhood: A framework. In Temperament in Childhood; Kohnstamm, G.A., Bates, J.E., Rothbart, M.K., Eds.; John Wiley & Sons: Oxford, UK, 1989; pp. 59–73. [Google Scholar]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef] [Green Version]
- Colder, C.R.; Stice, E. A Longitudinal Study of the Interactive Effects of Impulsivity and Anger on Adolescent Problem Behavior. J. Youth Adolesc. 1998, 27, 255–274. [Google Scholar] [CrossRef]
- Sarkisian, K.; Van Hulle, C.; Lemery-Chalfant, K.; Goldsmith, H. Childhood inhibitory control and adolescent impulsivity and novelty seeking as differential predictors of relational and overt aggression. J. Res. Personal. 2017, 67, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Fosco, W.D.; Hawk, L.W.; Colder, C.R.; Meisel, S.N.; Lengua, L.J. The development of inhibitory control in adolescence and prospective relations with delinquency. J. Adolesc. 2019, 76, 37–47. [Google Scholar] [CrossRef]
- Nigg, J.T.; Wong, M.M.; Martel, M.M.; Jester, J.M.; Puttler, L.I.; Glass, J.M.; Adams, K.M.; Fitzgerald, H.E.; Zucker, R.A. Poor Response Inhibition as a Predictor of Problem Drinking and Illicit Drug Use in Adolescents at Risk for Alcoholism and Other Substance Use Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 468–475. [Google Scholar] [CrossRef]
- Tarter, R.E.; Kirisci, L.; Mezzich, A.; Cornelius, J.R.; Pajer, K.; Vanyukov, M.; Gardner, W.; Blackson, T.; Clark, D. Neurobehavioral Disinhibition in Childhood Predicts Early Age at Onset of Substance Use Disorder. Am. J. Psychiatry 2003, 160, 1078–1085. [Google Scholar] [CrossRef] [Green Version]
- Raaijmakers, M.A.J.; Smidts, D.P.; Sergeant, J.A.; Maassen, G.H.; Posthumus, J.A.; Van Engeland, H.; Matthys, W. Executive Functions in Preschool Children with Aggressive Behavior: Impairments in Inhibitory Control. J. Abnorm. Child Psychol. 2008, 36, 1097–1107. [Google Scholar] [CrossRef] [Green Version]
- Utendale, W.T.; Hastings, P.D. Developmental changes in the relations between inhibitory control and externalizing problems during early childhood. Infant Child Dev. 2011, 20, 181–193. [Google Scholar] [CrossRef]
- Oldehinkel, A.J.; Hartman, C.A.; Ferdinand, R.F.; Verhulst, F.C.; Ormel, J. Effortful control as modifier of the association between negative emotionality and adolescents’ mental health problems. Dev. Psychopathol. 2007, 19, 523–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valiente, C.; Eisenberg, N.; Smith, C.L.; Reiser, M.; Fabes, R.A.; Losoya, S.; Guthrie, I.K.; Murphy, B.C. The relations of effortful control and reactive control to children’s externalizing problems: A longitudinal assessment. J. Personal. 2003, 71, 1171–1196. [Google Scholar] [CrossRef] [PubMed]
- Pardini, D.; Lochman, J.; Wells, K. Negative Emotions and Alcohol Use Initiation in High-Risk Boys: The Moderating Effect of Good Inhibitory Control. J. Abnorm. Child Psychol. 2004, 32, 505–518. [Google Scholar] [CrossRef]
- Mitchell, Q.P.; Younginer, S.T.; Lochman, J.E.; Vernberg, E.M.; Powell, N.P.; Qu, L. Examining for the Protective Effects of Therapeutic Engagement on Child Aggression. J. Emot. Behav. Disord. 2020. [Google Scholar] [CrossRef]
- Ellis, M.L.; Lindsey, M.A.; Barker, E.D.; Boxmeyer, C.L.; Lochman, J.E. Predictors of Engagement in a School-Based Family Preventive Intervention for Youth Experiencing Behavioral Difficulties. Prev. Sci. 2013, 14, 457–467. [Google Scholar] [CrossRef]
- Hogue, A.; Henderson, C.E.; Ozechowski, T.J.; Becker, S.J.; Coatsworth, J.D. Can the group harm the individual? Reviewing potential iatrogenic effects of group treatment for adolescent substance use. Clin. Psychol. Sci. Pract. 2019, 28, 40–51. [Google Scholar] [CrossRef]
- Hill, L.G.; The Conduct Problems Prevention Research Group; Coie, J.D.; Lochman, J.E.; Greenberg, M.T. Effectiveness of Early Screening for Externalizing Problems: Issues of Screening Accuracy and Utility. J. Consult. Clin. Psychol. 2004, 72, 809–820. [Google Scholar] [CrossRef] [Green Version]
- Kassing, F.; Conduct Problems Prevention Research Group; Godwin, J.; Lochman, J.E.; Coie, J.D. Using Early Childhood Behavior Problems to Predict Adult Convictions. J. Abnorm. Child Psychol. 2018, 47, 765–778. [Google Scholar] [CrossRef] [PubMed]
- Dodge, K.A.; Lochman, J.E.; Harnish, J.D.; Bates, J.E.; Pettit, G.S. Reactive and proactive aggression in schoolchildren and psychiatrically impaired chronically assaultive youth. J. Abnorm. Psychol. 1997, 106, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, M.A.; Romanelli, M.; Ellis, M.L.; Barker, E.; Boxmeyer, C.L.; Lochman, J.E. The Influence of Treatment Engagement on Positive Outcomes in the Context of a School-Based Intervention for Students with Externalizing Behavior Problems. J. Abnorm. Child Psychol. 2019, 47, 1437–1454. [Google Scholar] [CrossRef]
- Capaldi, D.M.; Rothbart, M.K. Development and Validation of an Early Adolescent Temperament Measure. J. Early Adolesc. 1992, 12, 153–173. [Google Scholar] [CrossRef]
- Reynolds, C.R.; Kamphaus, R.W. Behavior Assessment System for Children (BASC); American Guidance Service: Circle Pines, MN, USA, 1992. [Google Scholar]
- Pentz, M.A.; Trebow, E.A.; Hansen, W.B.; MacKinnon, D.P.; Dwyer, J.H.; Johnson, C.A.; Flay, B.R.; Daniels, S.; Cormack, C. Effects of program implementation on adolescent drug use behavior: The Midwestern Prevention Project (MPP). Eval. Rev. 1990, 14, 264–289. [Google Scholar] [CrossRef]
- Shillington, A.; Clapp, J. Self-Report stability of adolescent substance use: Are there differences for gender, ethnicity and age? Drug Alcohol Depend. 2000, 60, 19–27. [Google Scholar] [CrossRef]
- Fite, P.J.; Colder, C.R.; Lochman, J.E.; Wells, K.C. Pathways from proactive and reactive aggression to substance use. Psychol. Addict. Behav. 2007, 21, 355–364. [Google Scholar] [CrossRef]
- Pentz, M.A.; Johnson, C.A.; Dwyer, J.H.; Mackinnon, D.M.; Hansen, W.B.; Flay, B. A Comprehensive Community Approach to Adolescent Drug Abuse Prevention: Effects on Cardiovascular Disease Risk Behaviors. Ann. Med. 1989, 21, 219–222. [Google Scholar] [CrossRef]
- Boxmeyer, C.; Powell, N.P.; Lochman, J.E.; Dishion, T.J.; Wojnaroski, M.; Winter, C. Cognitive-Behavioral Group Coding System; University of Alabama: Tuscaloosa, AL, USA, 2015. [Google Scholar]
- Raudenbush, S.W.; Bryk, A.S. Hierarchical Linear Models: Applications and Data Analysis Methods; Sage Publications: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Johnston, L.D.; Miech, R.A.; O’Malley, P.M.; Bachman, J.G.; Schulenberg, J.E.; Patrick, M.E. Monitoring the Future Monitoring Survey Results on Drug Use, 1975–2018: 2018 Overview, Key Findings on Adolescent Drug Use; University of Michigan: Ann Arbor, MI, USA, 2019. [Google Scholar]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Pandina, R.J.; Johnson, V.L.; White, H.R. Peer influences on substance use during adolescence and emerging adulthood. In Handbook of Drug Use Etiology; Peeters Publishers: Leuven, Belgium, 2009; pp. 383–401. [Google Scholar]
- Fite, P.J.; Colder, C.R.; Lochman, J.E.; Wells, K.C. The Relation between Childhood Proactive and Reactive Aggression and Substance Use Initiation. J. Abnorm. Child Psychol. 2008, 36, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.; Sherritt, L.; Harris, S.K.; Gates, E.C.; Holder, D.W.; Kulig, J.W.; Knight, J.R. Test-Retest Reliability of Adolescents’ Self-Report of Substance Use. Alcohol. Clin. Exp. Res. 2004, 28, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.L.; Baker, E.L.; Porter, G.; Thayer, S.D.; Burlingame, G.M. Rating group therapist interventions: The validation of the Group Psychotherapy Intervention Rating Scale. Group Dyn. Theory Res. Pract. 2010, 14, 15–31. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Time | Group Format (GCP) | Individual Format (ICP) | ||||
|---|---|---|---|---|---|---|
| Mean | S.D | n | Mean | S.D | n | |
| 1 | 0.05 | 0.26 | 179 | 0.04 | 0.20 | 180 |
| 2 | 0.04 | 0.21 | 179 | 0.03 | 0.13 | 176 |
| 3 | 0.02 | 0.11 | 170 | 0.01 | 0.10 | 163 |
| 4 | 0.04 | 0.14 | 155 | 0.05 | 0.26 | 149 |
| 5 | 0.11 | 0.34 | 140 | 0.12 | 0.42 | 139 |
| 6 | 0.18 | 0.47 | 142 | 0.20 | 0.62 | 137 |
| 7 | 0.17 | 0.54 | 136 | 0.16 | 0.43 | 137 |
| 8 | 0.23 | 0.61 | 141 | 0.29 | 0.66 | 146 |
| Fixed Effect | Random Effect | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Level-3 | Level-2 | Level-1 | ||||||||||||
| Coef. | SE | t-Value | df | p-Value | Var | df | p-Value | Var | df | p-Value | ||||
| Substance use | ||||||||||||||
| Linear growth rate | 0.001 | 0.011 | 0.06 | 58 | 0.951 | 0.000 | 50.85 | 58 | >0.500 | 0.111 | 425.75 | 282 | 0.000 | 0.069 |
| IGCP (1 = I-CP 0 = G-CP) | 0.005 | 0.009 | 0.571 | 58 | 0.570 | |||||||||
| Race (1 = African American, 0 = other) | −0.036 | 0.015 | −2.48 | 175 | 0.014 | |||||||||
| Inhibitory control | −0.008 | 0.008 | −0.93 | 175 | 0.356 | |||||||||
| IGCP × nhibitory control | 0.022 | 0.011 | 1.95 | 175 | 0.053 | |||||||||
| Quadratic curve growth rate | 0.004 | 0.001 | 2.544 | 59 | 0.014 | |||||||||
| Fixed Effect | Random Effect | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Level-3 | Level-2 | Level-1 | ||||||||||||
| Coef. | SE | t-Value | df | p-Value | Var | df | p-Value | Var | df | p-Value | ||||
| Substance use | ||||||||||||||
| Linear growth rate | 0.003 | 0.014 | 0.19 | 27 | 0.851 | 0.000 | 26.31 | 27 | >0.500 | 0.008 | 170.30 | 137 | 0.028 | 0.071 |
| Positive behavior | 0.000 | 0.005 | 0.05 | 27 | 0.964 | |||||||||
| Negative behavior | −0.001 | 0.001 | −0.09 | 27 | 0.930 | |||||||||
| Race | −0.029 | 0.022 | −1.29 | 80 | 0.202 | |||||||||
| Age | 0.004 | 0.011 | 0.34 | 80 | 0.735 | |||||||||
| Gender | −0.009 | 0.014 | −0.66 | 80 | 0.514 | |||||||||
| Inhibit control | −0.007 | 0.009 | −0.79 | 80 | 0.434 | |||||||||
| Positive behav*inhibitory control | 0.013 | 0.006 | 2.24 | 80 | 0.028 | |||||||||
| Negative behav × inhibitory control | 0.007 | 0.007 | 1.11 | 80 | 0.272 | |||||||||
| Quadratic curve growth rate | 0.003 | 0.002 | 1.722 | 29 | 0.096 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lochman, J.E.; Boxmeyer, C.L.; Bui, C.; Hakim, E.; Jones, S.; Kassing, F.; McDonald, K.; Powell, N.; Qu, L.; Dishion, T. Substance Use Outcomes from Two Formats of a Cognitive-Behavioral Intervention for Aggressive Children: Moderating Roles of Inhibitory Control and Intervention Engagement. Brain Sci. 2021, 11, 950. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070950
Lochman JE, Boxmeyer CL, Bui C, Hakim E, Jones S, Kassing F, McDonald K, Powell N, Qu L, Dishion T. Substance Use Outcomes from Two Formats of a Cognitive-Behavioral Intervention for Aggressive Children: Moderating Roles of Inhibitory Control and Intervention Engagement. Brain Sciences. 2021; 11(7):950. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070950
Chicago/Turabian StyleLochman, John E., Caroline L. Boxmeyer, Chuong Bui, Estephan Hakim, Shannon Jones, Francesca Kassing, Kristina McDonald, Nicole Powell, Lixin Qu, and Thomas Dishion. 2021. "Substance Use Outcomes from Two Formats of a Cognitive-Behavioral Intervention for Aggressive Children: Moderating Roles of Inhibitory Control and Intervention Engagement" Brain Sciences 11, no. 7: 950. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070950