
A Lifespan Development Theory of Insecure Attachment and Internalizing Symptoms: Integrating Meta-Analytic Evidence via a Testable Evolutionary Mis/Match Hypothesis


Abstract
:1. Introduction
2. Attachment Assessment across the Lifespan
2.1. Attachment in Infancy and Early Childhood
2.2. Attachment in Adolescence and Adulthood
3. Insecure Attachment and Internalizing Symptoms across the Lifespan: Conceptual Links
3.1. Infancy and Childhood
3.2. Adolescence and Adulthood
4. Insecure Attachment Subtypes and Internalizing Symptoms across the Lifespan: Empirical Findings
4.1. Childhood
4.2. Adolescence and Adulthood
5. An Overview of Results across the Lifespan
6. Methodological Considerations Regarding Assessing Internalizing Symptoms and Attachment across the Lifespan
6.1. Different Informants for Assessments of Internalizing Symptoms
6.2. Different Phenomenology of Internalizing Symptoms
6.3. Assessment of Attachment Patterns
7. Intermediate Summary
8. A Lifespan Development Theory of Insecure Attachment and Internalizing Symptoms
8.1. Developmentally Appropriate Orientation Tendencies toward or away from Caregivers across the Lifespan
8.2. Mis/Match between Attachment Patterns and Developmentally Appropriate Orientation Tendencies in Childhood versus Adolescence/Adulthood
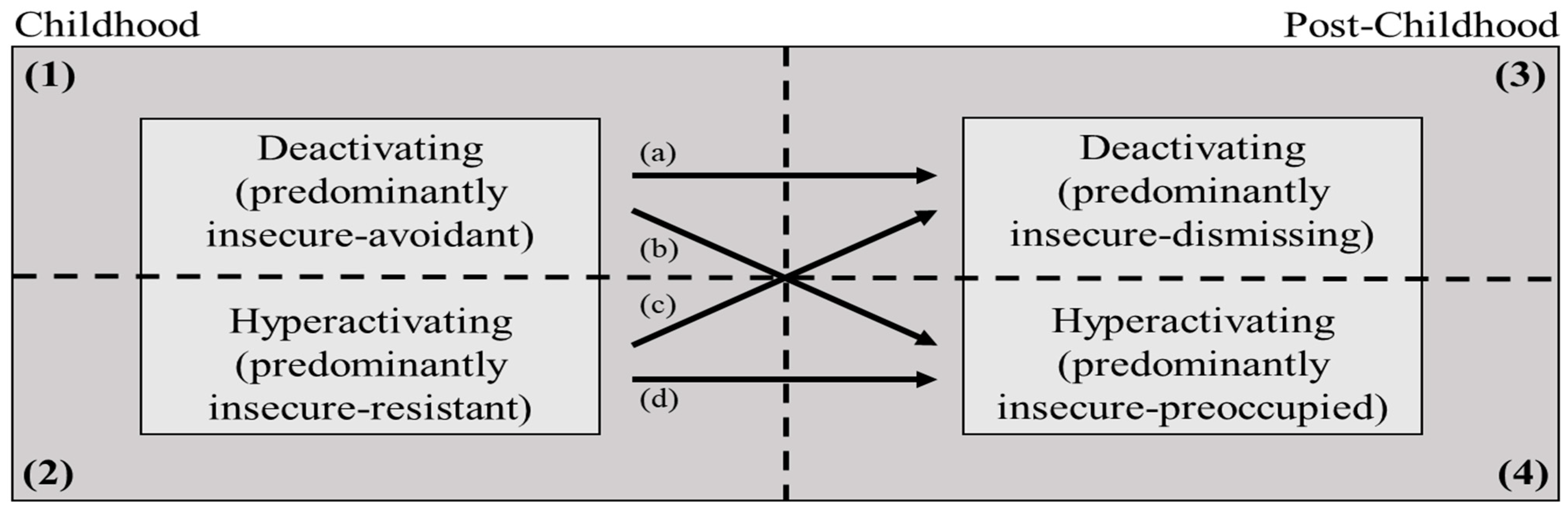
8.2.1. Deactivating Attachment Strategies
8.2.2. Hyperactivating Attachment Strategies
8.3. Testing the Mis/Match Hypothesis in the Context of Insecure Attachment and Internalizing Symptoms across the Lifespan
9. Future Research
10. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Graczyk, P.A.; Hennelly, M.M.; Connolly, S.D. Anxiety disorders in childhood. In Handbook of Childhood Behavioral Issues; Gullotta, H.P., Bla, G.M., Eds.; Routledge: London, UK, 2016; pp. 235–257. [Google Scholar]
- Maughan, B.; Collishaw, S.; Stringaris, A. Depression in childhood and adolescence. J. Can. Acad. Child Adolesc. Psychiatry 2013, 22, 35–40. [Google Scholar] [CrossRef]
- Canals, J.; Voltas, N.; Hernández-Martínez, C.; Cosi, S.; Arija, V. Prevalence of DSM-5 anxiety disorders, comorbidity, and persistence of symptoms in Spanish early adolescents. Eur. Child Adolesc. Psychiatry 2019, 28, 131–143. [Google Scholar] [CrossRef]
- Thapar, A.; Collishaw, S.; Pine, D.S.; Thapar, A.K. Depression in adolescence. Lancet 2012, 379, 1056–1067. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, P.E.; Fournier, A.-A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The global prevalence of common mental disorders: A systematic review and meta-analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef] [Green Version]
- Hidaka, B.H. Depression as a disease of modernity: Explanations for increasing prevalence. J. Affect. Disord. 2012, 140, 205–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mojtabai, R.; Olfson, M.; Han, B. National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics 2016, 138, e20161878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, 2011–2030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehm, J.; Shield, K.D. Global burden of disease and the impact of mental and addictive disorders. Curr. Psychiatry Rep. 2019, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Collins, P.Y.; Patel, V.; Joestl, S.S.; March, D.; Insel, T.R.; Daar, A.S.; Bordin, I.A.; Costello, E.J.; Durkin, M.; Fairburn, C.G.; et al. Grand challenges in global mental health. Nature 2011, 475, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M.; Irwin, M.R. From stress to inflammation and major depressive disorder: A social signal transduction theory of depression. Psychol. Bull. 2014, 140, 774–815. [Google Scholar] [CrossRef]
- Hames, J.L.; Hagan, C.R.; Joiner, T.E. Interpersonal processes in depression. Annu. Rev. Clin. Psychol. 2013, 9, 355–377. [Google Scholar] [CrossRef]
- Rudolph, K.D. Adolescent depression. In Handbook of Depression; Gotlib, H., Hammen, C.L., Eds.; Guilford Press: New York, NY, USA, 2009; pp. 444–466. [Google Scholar]
- LeMoult, J. From stress to depression: Bringing together cognitive and biological science. Curr. Dir. Psychol. Sci. 2020, 29, 592–598. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef]
- Slavich, G.M.; O’Donovan, A.; Epel, E.S.; Kemeny, M.E. Black sheep get the blues: A psychobiological model of social rejection and depression. Neurosci. Biobehav. Rev. 2010, 35, 39–45. [Google Scholar] [CrossRef]
- Dykas, M.J.; Cassidy, J. Attachment and the processing of social information across the life span: Theory and evidence. Psychol. Bull. 2011, 137, 19–46. [Google Scholar] [CrossRef] [Green Version]
- Brumariu, L.E. Parent-child attachment and emotion regulation. New Dir. Child Adolesc. Dev. 2015, 148, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Dozier, M.; Kobak, R.R. Psychophysiology in attachment interviews: Converging evidence for deactivating strategies. Child Dev. 1992, 63, 1473–1480. [Google Scholar] [CrossRef] [PubMed]
- Groh, A.M.; Narayan, A.J. Infant attachment insecurity and baseline physiological activity and physiological reactivity to interpersonal stress: A meta-analytic review. Child Dev. 2019, 90, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Roisman, G.I.; Tsai, J.L.; Chiang, K.-H.S. The emotional integration of childhood experience: Physiological, facial expressive, and self-reported emotional response during the Adult Attachment Interview. Dev. Psychol. 2004, 40, 776–789. [Google Scholar] [CrossRef] [Green Version]
- Hammen, C. Adolescent depression: Stressful interpersonal contexts and risk for recurrence. Curr. Dir. Psychol. Sci. 2009, 18, 200–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapero, B.G.; Abramson, L.Y.; Alloy, L.B. Emotional reactivity and internalizing symptoms: Moderating role of emotion regulation. Cogn. Ther. Res. 2016, 40, 328–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeman, J.; Shipman, K.; Suveg, C. Anger and sadness regulation: Predictions to internalizing and externalizing symptoms in children. J. Clin. Child Adolesc. Psychol. 2002, 31, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Dagan, O.; Bernard, K. It takes a village: A call for engaging attachment with adjunct disciplines to clarify “in-house” clinical conundrums. Attach. Hum. Dev. 2021, 23, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, M.D.S.; Blehar, M.C.; Waters, E.; Wall, S.N. Patterns of Attachment: A Psychological Study of the Strange Situation; Lawrence Erlbaum Associates Publishers: Hillsdale, NJ, USA, 1978; ISBN 9781135016173. [Google Scholar]
- Sroufe, L.A. The coherence of individual development: Early care, attachment, and subsequent developmental issues. Am. Psychol. 1979, 34, 834–841. [Google Scholar] [CrossRef]
- Belsky, J. Attachment, mating, and parenting: An evolutionary interpretation. Hum. Nat. 1997, 8, 361–381. [Google Scholar] [CrossRef]
- Main, M. Avoidance in the service of attachment: A working paper. In Behavioral Development: The Bielfeld Interdisciplinary Project; Immelman, K., Barlow, G., Petrinovich, L., Main, M., Eds.; Cambridge University Press: New York, NY, USA, 1981; pp. 651–693. [Google Scholar]
- Main, M. The organized categories of infant, child, and adult attachment: Flexible vs. inflexible attention under attachment-related stress. J. Am. Psychoanal. Assoc. 2000, 48, 1055–1096; discussion 1175–1187. [Google Scholar] [CrossRef]
- Cassidy, J.; Berlin, L.J. The insecure/ambivalent pattern of attachment: Theory and research. Child Dev. 1994, 65, 971–991. [Google Scholar] [CrossRef]
- Main, M.; Solomon, J. Procedures for identifying disorganized/disoriented infants during the Ainsworth Strange Situation. In Attachment in the Preschool Years; Greenberg, M., Cicchetti, D., Cummings, M., Eds.; University of Chicago Press: Chicago, IL, USA, 1990; pp. 121–160. [Google Scholar]
- Cyr, C.; Euser, E.M.; Bakermans-Kranenburg, M.J.; Van Ijzendoorn, M.H. Attachment security and disorganization in maltreating and high-risk families: A series of meta-analyses. Dev. Psychopathol. 2010, 22, 87–108. [Google Scholar] [CrossRef]
- Hesse, E.; Main, M. Frightened, threatening, and dissociative parental behavior: Theory and associations with parental Adult Attachment Interview status and infant disorganization. Dev. Psychopathol. 2006, 18, 309–343. [Google Scholar] [CrossRef]
- Lyons-Ruth, K.; Jacobvitz, D. Attachment disorganization: Unresolved loss, relational violence, and lapses in behavioral and attentional strategies. In Handbook of Attachment: Theory, Research, and Clinical Applications; The Guilford Press: New York, NY, USA, 1999; pp. 520–554. ISBN 1572300876. [Google Scholar]
- Madigan, S.; Bakermans-Kranenburg, M.J.; Van Ijzendoorn, M.H.; Moran, G.; Pederson, D.R.; Benoit, D. Unresolved states of mind, anomalous parental behavior, and disorganized attachment: A review and meta-analysis of a transmission gap. Attach. Hum. Dev. 2006, 8, 89–111. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Kaplan, N.; Main, M. Adult Attachment Interview; University of California at Berkeley: Berkeley, CA, USA, 1985. [Google Scholar]
- Hesse, E. The Adult Attachment Interview: Protocol, method of analysis, and empirical studies: 1985–2015. In Handbook of Attachment: Theory, Research, and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2016; pp. 553–597. [Google Scholar]
- Roisman, G.I. The psychophysiology of adult attachment relationships: Autonomic reactivity in marital and premarital interactions. Dev. Psychol. 2007, 43, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Bowlby, J. The Making and Breaking of Affectional Bonds; Tavistock Publications: London, UK, 1979. [Google Scholar]
- Bowlby, J. Separation: Anxiety and anger. In Attachment and Loss; Basic Books: New York, NY, USA, 1973; Volume 2. [Google Scholar]
- Bowlby, J. Attachment. In Attachment and Loss; Basic Books: New York, NY, USA, 1969; Volume 1. [Google Scholar]
- Bowlby, J. Loss: Sadness and depression. In Attachment and Loss; Basic Books: New York, NY, USA, 1980; Volume 3. [Google Scholar]
- Egeland, B.; Carlson, E.A. Attachment and psychopathology. In Attachment Issues in Psychopathology and Intervention; Atkinson, L., Goldberg, S., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004; pp. 27–48. [Google Scholar]
- Goldberg, S. Attachment and childhood behavior problems in normal, at-risk and clinical samples. In Attachment and Psychopathology; Atkinson, L., Zucker, K.J., Eds.; Guilford Press: New York, NY, USA, 1997; pp. 171–195. [Google Scholar]
- Carlson, E.A.; Sroufe, L.A. Contribution of attachment theory to developmental psychopathology. In Developmental Psychopathology: Theory and Methods; Cicchetti, D., Cohen, D., Eds.; Wiley: Oxford, UK, 1995; Volume 1, pp. 581–616. [Google Scholar]
- Finnegan, R.A.; Ernest, E.V.E.; Perry, D.G. Preoccupied and aviodant coping during middle childhood. Child Dev. 1996, 67, 1318–1328. [Google Scholar] [CrossRef]
- Manassis, K. Child-parent relations: Attachment and anxiety disorders. In Anxiety Disorders in Children and Adolescents: Research, Assessment, and Intervention; Silverman, W.K., Treffers, P.D.A., Eds.; Cambridge University Press: Cambridge, UK, 2001; pp. 255–272. [Google Scholar]
- Dozier, M.; Stovall-McClough, K.C.; Albus, K.E. Attachment and psychopathology in adulthood. In Handbook of Attachment: Theory, Research, and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; The Guilford Press: New York, NY, USA, 2008; pp. 718–744. ISBN 9781593858742/9781606230282. [Google Scholar]
- Solomon, J.; George, C. The development of attachment in separated and divorced families. Attach. Hum. Dev. 1999, 1, 2–33. [Google Scholar] [CrossRef]
- Moss, E.; Rousseau, D.; Parent, S.; St-Laurent, D.; Saintonge, J. Correlates of attachment at school age: Maternal reported stress, mother-child interaction, and behavior problems. Child Dev. 1998, 69, 1390–1405. [Google Scholar] [CrossRef]
- Madigan, S.; Atkinson, L.; Laurin, K.; Benoit, D. Attachment and internalizing behavior in early childhood: A meta-analysis. Dev. Psychol. 2013, 49, 672–689. [Google Scholar] [CrossRef] [Green Version]
- Fortuna, K.; Roisman, G.I. Insecurity, stress, and symptoms of psychopathology: Contrasting results from self-reports versus interviews of adult attachment. Attach. Hum. Dev. 2008, 10, 11–28. [Google Scholar] [CrossRef]
- Main, M.; Kaplan, N.; Cassidy, J. Security in infancy, childhood, and adulthood: A move to the level of representation. Monogr. Soc. Res. Child Dev. 1985, 50, 66–104. [Google Scholar] [CrossRef]
- Kobak, R.; Cole, H. Attachment and Meta-Monitoring: Implications for Adolescent Autonomy and Psychopathology. In Disorders and Dysfunctions of the Self; Cicchetti, D., Toth, S.L., Eds.; University of Rochester Press: Rochester, NY, USA, 1994; pp. 267–297. ISBN 1878822314. [Google Scholar]
- Kobak, R.R.; Cole, H.E.; Ferenz-Gillies, R.; Fleming, W.S.; Gamble, W. Attachment and emotion regulation during mother-teen problem solving: A control theory analysis. Child Dev. 1993, 64, 231–245. [Google Scholar] [CrossRef]
- Cassidy, J.; Kobak, R. Avoidance and its relation to other defensive processes. In Clinical Implications of Attachment Theory; Belsky, J., Nezworski, T., Eds.; Lawrence Erlbaum Associates Publishers: Hillsdale, NJ, USA, 1988; pp. 300–323. [Google Scholar]
- Bakermans-Kranenburg, M.J.; Van Ijzendoorn, M.H. The first 10,000 Adult Attachment Interviews: Distributions of adult attachment representations in clinical and non-clinical groups. Attach. Hum. Dev. 2009, 11, 223–263. [Google Scholar] [CrossRef]
- Groh, A.M.; Roisman, G.I.; Van Ijzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Fearon, R.P. The significance of insecure and disorganized attachment for children’s internalizing symptoms: A meta-analytic study. Child Dev. 2012, 83, 591–610. [Google Scholar] [CrossRef]
- Dagan, O.; Facompré, C.R.; Bernard, K. Adult attachment representations and depressive symptoms: A meta-analysis. J. Affect. Disord. 2018, 236, 274–290. [Google Scholar] [CrossRef] [PubMed]
- Dagan, O.; Facompré, C.R.; Nivison, M.D.; Roisman, G.I.; Bernard, K. Preoccupied and dismissing attachment representations are differentially associated with anxiety in adolescence and adulthood: A meta-analysis. Clin. Psychol. Sci. 2020, 8, 614–640. [Google Scholar] [CrossRef]
- De Los Reyes, A.; Kazdin, A.E. Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychol. Bull. 2005, 131, 483–509. [Google Scholar] [CrossRef] [PubMed]
- Kaminer, Y.; Feinstein, C.; Seifer, R. Is there a need for observationally based assessment of affective symptomatology in child and adolescent psychiatry? Adolescence 1995, 30, 483–489. [Google Scholar] [PubMed]
- Tandon, M.; Cardeli, E.; Luby, J. Internalizing disorders in early childhood: A review of depressive and anxiety disorders. Child Adolesc. Psychiatr. Clin. 2009, 18, 593–610. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.P.; Moore, C.; Kuperminc, G.; Bell, K. Attachment and adolescent psychosocial functioning. Child Dev. 1998, 69, 1406–1419. [Google Scholar] [CrossRef]
- Madigan, S.; Brumariu, L.E.; Villani, V.; Atkinson, L.; Lyons-Ruth, K. Representational and questionnaire measures of attachment: A meta-analysis of relations to child internalizing and externalizing problems. Psychol. Bull. 2016, 142, 367–399. [Google Scholar] [CrossRef]
- Foland-Ross, L.C.; Gotlib, I.H. Cognitive and neural aspects of information processing in major depressive disorder: An integrative perspective. Front. Psychol. 2012, 3, 489. [Google Scholar] [CrossRef] [Green Version]
- Garber, J.; Kaminski, K.M. Laboratory and performance-based measures of depression in children and adolescents. J. Clin. Child Psychol. 2000, 29, 509–525. [Google Scholar] [CrossRef]
- Carpenter, A.L.; Puliafico, A.C.; Kurtz, S.M.S.; Pincus, D.B.; Comer, J.S. Extending parent-child interaction therapy for early childhood internalizing problems: New advances for an overlooked population. Clin. Child Fam. Psychol. Rev. 2014, 17, 340–356. [Google Scholar] [CrossRef]
- Louters, L.L. Don’t overlook childhood depression. JAAPA 2004, 17, 18–24. [Google Scholar]
- Klein, D.N.; Dougherty, L.R.; Olino, T.M. Toward guidelines for evidence-based assessment of depression in children and adolescents. J. Clin. Child Adolesc. Psychol. 2005, 34, 412–432. [Google Scholar] [CrossRef]
- Cicchetti, D.; Toth, S.L. The development of depression in children and adolescents. Am. Psychol. 1998, 53, 221–241. [Google Scholar] [CrossRef]
- Birmaher, B.; Brent, D. Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 1503–1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caspi, A.; Houts, R.M.; Belsky, D.W.; Goldman-Mellor, S.J. The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clin. Psychol. Sci. 2015, 2, 119–137. [Google Scholar] [CrossRef]
- Eaton, N.R.; Krueger, R.F.; Markon, K.E.; Keyes, K.M.; Skodol, A.E.; Wall, M.; Hasin, D.S.; Grant, B.F. The structure and predictive validity of the internalizing disorders. J. Abnorm. Psychol. 2013, 122, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, B.; Garber, J. Developmental differences in the phenomenology of depression. Dev. Psychopathol. 2003, 15, 403–430. [Google Scholar] [CrossRef] [PubMed]
- Fraley, R.C.; Spieker, S.J. Are infant attachment patterns continuously or categorically distributed? A taxometric analysis of strange situation behavior. Dev. Psychol. 2003, 39, 387–404. [Google Scholar] [CrossRef] [PubMed]
- Haltigan, J.D.; Roisman, G.I.; Haydon, K.C., II. The latent structure of the adult attachment interview: Exploratory and confirmatory evidence. Monogr. Soc. Res. Child Dev. 2014, 79, 15–35. [Google Scholar] [CrossRef]
- Sroufe, L.A. Attachment categories as reflections of multiple dimensions: Comment on Fraley and Spieker (2003). Dev. Psychol. 2003, 39, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Van Ijzendoorn, M.H.; Bakermans-kranenburg, M.J. Confined Quest for Continuity: The Categorical Versus. Monogr. Soc. Res. Child Dev. 2014, 79, 157–167. [Google Scholar] [CrossRef]
- Fraley, R.C.; Roisman, G.I., III. Categories or dimensions? A taxometric analysis of the Adult Attachment Interview. Monogr. Soc. Res. Child Dev. 2014, 79, 36–50. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. The cost of dichotomization. Appl. Psychol. Meas. 1983, 7, 249–253. [Google Scholar] [CrossRef]
- Dagan, O.; Sagi-Schwartz, A. Early attachment network with mother and father: An unsettled issue. Child Dev. Perspect. 2018, 12, 115–121. [Google Scholar] [CrossRef]
- Dagan, O.; Sagi-Schwartz, A. Infant attachment (to mother and father) and its place in human development: Five decades of promising research (and an unsettled issue). In The Cambridge Handbook of Infant Development; Lockman, J.J., Tamis-LeMonda, C., Eds.; Cambridge University Press: Cambridge, UK, 2020; pp. 687–714. [Google Scholar]
- Owens, G.; Crowell, J.; Pan, H.; Treboux, D.; O’Connor, E.; Waters, E. The prototype hypothesis and the origins of attachment working models: Adult relationships with parents and romantic partners. Monogr. Soc. Res. Child Dev. 1995, 60, 216–233. [Google Scholar] [CrossRef]
- Haydon, K.C.; Roisman, G.I.; Burt, K.B. In search of security: The latent structure of the Adult Attachment Interview revisited. Dev. Psychopathol. 2012, 24, 589–606. [Google Scholar] [CrossRef]
- Simpson, J.A.; Belsky, J. Attachment theory within a modern evolutionary framework. In Handbook of Attachment: Theory, Research and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2016; pp. 91–116. [Google Scholar]
- Cassidy, J. The nature of the child’s ties. In Handbook of Attachment: Theory, Research and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 3–22. [Google Scholar]
- Belsky, J.; Steinberg, L.; Draper, P. Childhood experience, interpersonal development, and reproductive strategy: An evolutionary theory of socialization. Child Dev. 1991, 62, 647–670. [Google Scholar] [CrossRef]
- Del Giudice, M. Sex, attachment, and the development of reproductive strategies. Behav. Brain Sci. 2009, 32, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Nesse, R.M. Evolutionary psychology and mental health. In The Handbook of Evolutionary Psychology; Buss, D.M., Ed.; John and Wiley and Sons: Hoboken, NJ, USA, 2005; pp. 903–927. ISBN 9781119125563. [Google Scholar]
- Frankenhuis, W.E.; Del Giudice, M. When do adaptive developmental mechanisms yield maladaptive outcomes? Dev. Psychol. 2012, 48, 628–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nederhof, E.; Schmidt, M.V. Mismatch or cumulative stress: Toward an integrated hypothesis of programming effects. Physiol. Behav. 2012, 106, 691–700. [Google Scholar] [CrossRef]
- Crespi, B.J. Evolutionary and genetic insights for clinical psychology. Clin. Psychol. Rev. 2020, 78, 101857. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Hanson, M.A.; Spencer, H.G.; Bateson, P. Environmental influences during development and their later consequences for health and disease: Implications for the interpretation of empirical studies. Proc. R. Soc. B 2005, 272, 671–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, H.; Hill, K.; Lancaster, J.; Hurtado, A.M. A theory of human life history evolution: Diet, intelligence, and longevity. Evol. Anthropol. 2000, 9, 156–185. [Google Scholar] [CrossRef]
- Waters, E.; Cummings, E.M. A secure base from which to explore close relationships. Child Dev. 2000, 71, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Waters, H.S.; Waters, E. The attachment working models concept: Among other things, we build script-like representations of secure base experiences. Attach. Hum. Dev. 2006, 8, 185–197. [Google Scholar] [CrossRef]
- Dujardin, A.; Santens, T.; Braet, C.; De Raedt, R.; Vos, P.; Maes, B.; Bosmans, G. Middle childhood support-seeking behavior during stress: Links with self-reported attachment and future depressive symptoms. Child Dev. 2016, 87, 326–340. [Google Scholar] [CrossRef]
- Shanahan, L.; Calkins, S.D.; Keane, S.P.; Kelleher, R.; Suffness, R. Trajectories of internalizing symptoms across childhood: The roles of biological self-regulation and maternal psychopathology. Dev. Psychopathol. 2014, 26, 1353–1368. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.P. Attachment in Adolescence. In Handbook of Attachment: Theory, Research and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 319–335. [Google Scholar]
- Goossens, L. Loneliness in adolescence: Insights from Cacioppo’s evolutionary model. Child Dev. Perspect. 2018, 12, 230–234. [Google Scholar] [CrossRef]
- Furman, W.; Simon, V.A. Cognitive Representations of Adolescent Romantic Relationships. In The Development of Romantic Relationships in Adolescence; Cambridge University Press: Cambridge, UK, 1999; pp. 75–98. [Google Scholar]
- Goossens, L. The many faces of adolescent autonomy: Parent-adolescent conflict, behavioral decision-making, and emotional distancing. In Handbook of Adolescent Development; Jackson, S., Goossens, L., Eds.; Psychology Press: New York, NY, USA, 2006; pp. 135–153. ISBN 184169200X/9781841692005. [Google Scholar]
- Hill, J.P.; Holmbeck, G.N. Attachment and autonomy during adolescence. In Annals of Child Development; Whitehurst, G.J., Ed.; JAI Press: Greenwich, CT, USA, 1986; Volume 3. [Google Scholar]
- Allen, J.P.; Miga, E.M. Attachment in adolescence: A move to the level of emotion regulation. J. Soc. Pers. Relationsh. 2010, 27, 181–190. [Google Scholar] [CrossRef] [Green Version]
- Rosenthal, N.L.; Kobak, R. Assessing adolescents’ attachment hierarchies: Differences across developmental periods and associations with individual adaptation. J. Res. Adolesc. 2010, 20, 678–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J.P.; Tan, J.S. The multiple facets of attachment in adolescence. In Handbook of Attachment: Theory, Research, and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2016; pp. 399–415. [Google Scholar]
- Sroufe, A.L. Attachment and development: A prospective, longitudinal study from birth to adulthood. Attach. Hum. Dev. 2005, 7, 349–367. [Google Scholar] [CrossRef] [PubMed]
- Surjadi, F.F.; Lorenz, F.O.; Wickrama, K.A.S.; Conger, R.D. Parental support, partner support, and the trajectories of mastery from adolescence to early adulthood. J. Adolesc. 2011, 34, 619–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J.P.; Hauser, S.T. Autonomy and relatedness in adolescent-family interactions as predictors of young adults’ states of mind regarding attachment. Dev. Psychopathol. 1996, 8, 793–809. [Google Scholar] [CrossRef]
- Amstadter, A. Emotion regulation and anxiety disorders. J. Anxiety Disord. 2008, 22, 211–221. [Google Scholar] [CrossRef] [Green Version]
- Joormann, J.; Gotlib, I.H. Emotion regulation in depression: Relation to cognitive inhibition. Cogn. Emot. 2010, 24, 281–298. [Google Scholar] [CrossRef] [Green Version]
- Laursen, B.; Hartl, A.C. Understanding loneliness during adolescence: Developmental changes that increase the risk of perceived social isolation. J. Adolesc. 2013, 36, 1261–1268. [Google Scholar] [CrossRef]
- Witvliet, M.; Brendgen, M.; Van Lier, P.A.C.; Koot, H.M.; Vitaro, F. Early Adolescent Depressive Symptoms: Prediction from Clique Isolation, Loneliness, and Perceived Social Acceptance. J. Abnorm. Child Psychol. 2010, 38, 1045–1056. [Google Scholar] [CrossRef] [Green Version]
- Romeo, R.D. Adolescence: A central event in shaping stress reactivity. Dev. Psychobiol. 2010, 52, 244–253. [Google Scholar] [CrossRef]
- Steinberg, L.; Morris, A.S. Adolescent devolepmental. Annu. Rev. Psychol. 2001, 52, 83–110. [Google Scholar] [CrossRef]
- Costello, E.; Mustillo, S.; Erkanli, A.; Keeler, G.; Angold, A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch. Gen. Psychiatry 2003, 60, 837–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merikangas, K.R.; He, J.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in US adolescents: Results from the National Comorbidity Study-Adolescent supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, T.; Danese, A.; Wertz, J.; Odgers, C.L.; Ambler, A.; Moffitt, T.E.; Arseneault, L. Social isolation, loneliness and depression in young adulthood: A behavioural genetic analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 339–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Main, M. Cross-cultural studies of attachment organization: Recent studies, changing methodologies, and the concept of conditional strategies. Hum. Dev. 1990, 33, 48–61. [Google Scholar] [CrossRef]
- Borelli, J.L.; Gaskin, G.; Smiley, P.; Chung, D.; Shahar, B.; Bosmans, G. Multisystem physiological reactivity during help-seeking for attachment needs in school-aged children: Differences as a function of attachment. Attach. Hum. Dev. 2021, 1–15. [Google Scholar] [CrossRef]
- Bosmans, G.; Sanchez-Lopez, A.; Finet, C.; De Raedt, R. Attachment-related attention bias plays a causal role in trust in maternal support. J. Exp. Child Psychol. 2019, 185, 176–190. [Google Scholar] [CrossRef]
- Verhees, M.W.F.T.; Ceulemans, E.; Van Ijzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Bosmans, G. State attachment variability across distressing situations in middle childhood. Soc. Dev. 2020, 29, 196–216. [Google Scholar] [CrossRef]
- Boyce, W.T.; Quas, J.; Alkon, A.; Smider, N.A.; Essex, M.J.; Kupfer, D.J. Autonomic reactivity and psychopathology in middle childhood. Br. J. Psychiatry 2001, 179, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Rutter, M. Implications of resilience concepts for scientific understanding. Ann. N. Y. Acad. Sci. 2006, 1094, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraley, R.C.; Garner, J.P.; Shaver, P.R. Adult attachment and the defensive regulation of attention and memory: Examining the role of preemptive and postemptive defensive processes. J. Pers. Soc. Psychol. 2000, 79, 816–826. [Google Scholar] [CrossRef]
- Shaver, P.R.; Mikulincer, M. Adult attachment strategies and the regulation of emotion. In Handbook of Emotion Regulation; Gross, J.J., Ed.; Guilford Press: New York, NY, USA, 2007; pp. 446–465. ISBN 1593851480. [Google Scholar]
- Bakermans-Kranenburg, M.J.; Van Ijzendoorn, M.H. A psychometric study of the Adult Attachment Interview: Reliability and discriminant validity. Dev. Psychol. 1993, 29, 870–879. [Google Scholar] [CrossRef]
- Spangler, G.; Zimmermann, P. Attachment representation and emotion regulation in adolescents: A psychobiological perspective on internal working models. Attach. Hum. Dev. 1999, 1, 270–290. [Google Scholar] [CrossRef]
- Lemche, E.; Giampietro, V.P.; Surguladze, S.A.; Amaro, E.J.; Andrew, C.M.; Williams, S.C.R.; Brammer, M.J.; Lawrence, N.; Maier, M.A.; Russell, T.A.; et al. Human Attachment Security Is Mediated by the Amygdala: Evidence from Combined fMRI and Psychophysiological Measures. Hum. Brain Mapp. 2006, 27, 623–635. [Google Scholar] [CrossRef]
- Main, M. Attachment theory: Eighteen points with suggestions for future studies. In Handbook of Attachment: Theory, Research, and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 1999; pp. 845–887. [Google Scholar]
- Young, K.; Sandman, C.; Craske, M. Positive and negative emotion regulation in adolescence: Links to anxiety and depression. Brain Sci. 2019, 9, 76. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, S.G. Interpersonal emotion regulation model of mood and anxiety disorders. Cogn. Ther. Res. 2014, 38, 483–492. [Google Scholar] [CrossRef]
- Hazan, C.; Shaver, P. Romantic love conceptualized as an attachment process. J. Pers. Soc. Psychol. 1987, 52, 511–524. [Google Scholar] [CrossRef]
- Seiffge-Krenke, I. Coping with relationship stressors: The impact of different working models of attachment and links to adaptation. J. Youth Adolesc. 2006, 35, 25–39. [Google Scholar] [CrossRef]
- Tarabulsy, G.M.; Larose, S.; Bernier, A.; Trottier-Sylvain, K.; Girard, D.; Vargas, M.; Noël, C. Attachment states of mind in late adolescence and the quality and course of romantic relationships in adulthood. Attach. Hum. Dev. 2012, 14, 621–643. [Google Scholar] [CrossRef] [PubMed]
- Hrdy, S.B. Mothers and Others; Harvard University Press: London, UK, 2011; ISBN 0674060326. [Google Scholar]
- Marroquín, B. Interpersonal emotion regulation as a mechanism of social support in depression. Clin. Psychol. Rev. 2011, 31, 1276–1290. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S.; Wisco, B.E.; Lyubomirsky, S. Rethinking rumination. Perspect. Psychol. Sci. 2008, 3, 400–424. [Google Scholar] [CrossRef] [PubMed]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef] [PubMed]
- Clarke, A.T. Coping with interpersonal stress and psychosocial health among children and adolescents: A meta-analysis. J. Youth Adolesc. 2006, 35, 10–23. [Google Scholar] [CrossRef]
- Slavich, G.M.; Way, B.M.; Eisenberger, N.I.; Taylor, S.E. Neural sensitivity to social rejection is associated with inflammatory responses to social stress. Proc. Natl. Acad. Sci. USA 2010, 107, 14817–14822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassidy, J.; Jones, J.D.; Shaver, P.R. Contributions of attachment theory and research: A framework for future research, translation, and policy. Dev. Psychopathol. 2013, 25, 1415–1434. [Google Scholar] [CrossRef]
- Bosmans, G.; Koster, E.H.W.; Vandevivere, E.; Braet, C.; De Raedt, R. Young adolescent’s confidence in maternal support: Attentional bias moderates the link between attachment-related expectations and behavioral problems. Cogn. Ther. Res. 2013, 37, 829–839. [Google Scholar] [CrossRef] [Green Version]
- Bernier, A.; Larose, S.; Whipple, N. Leaving home for college: A potentially stressful event for adolescents with preoccupied attachment patterns. Attach. Hum. Dev. 2005, 7, 171–185. [Google Scholar] [CrossRef]
- Larose, S.; Bernier, A. Social support processes: Mediators of attachment state of mind and adjustment in late adolescence. Attach. Hum. Dev. 2001, 3, 96–120. [Google Scholar] [CrossRef]
- Mcelhaney, K.B.; Allen, J.P.; Stephenson, J.C.; Hare, A.L. Attachment and autonomy during adolescence. In Handbook of Adolescent Psychology; Lerner, R.M., Steinberg, L., Eds.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2009; Volume 1, pp. 358–403. [Google Scholar]
- Creasey, G. Associations between working models of attachment and conflict management behavior in romantic couples. J. Couns. Psychol. 2002, 49, 365–375. [Google Scholar] [CrossRef]
- Kobak, R.R.; Sceery, A. Attachment in late adolescence: Working models, affect regulation, and representations of self and others. Child Dev. 1988, 59, 135–146. [Google Scholar] [CrossRef]
- Zimmermann, P. Attachment representations and characteristics of friendship relations during adolescence. J. Exp. Child Psychol. 2004, 88, 83–101. [Google Scholar] [CrossRef]
- Clark, J.L.; Algoe, S.B.; Green, M.C. Social network sites and well-being: The role of social connection. Curr. Dir. Psychol. Sci. 2017, 27, 32–37. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.P.; Insabella, G.; Porter, M.R.; Smith, F.D.; Land, D.; Phillips, N. A social-interactional model of the development of depressive symptoms in adolescence. J. Consult. Clin. Psychol. 2006, 74, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Barber, B.K.; Olsen, J.E.; Shagle, S.C. Associations between parental psychological and behavioral control and youth internalized and externalized behaviors. Child Dev. 1994, 65, 1120–1136. [Google Scholar] [CrossRef]
- Kuzawa, C.W.; Quinn, E.A. Developmental origins of adult function and health: Evolutionary hypotheses. Annu. Rev. Anthropol. 2009, 38, 131–147. [Google Scholar] [CrossRef] [Green Version]
- Pollak, S.D. Mechanisms linking early experience and the emergence of emotions: Illustrations from the study of maltreated children. Curr. Dir. Psychol. Sci. 2008, 17, 370–375. [Google Scholar] [CrossRef] [Green Version]
- Ellis, B.J.; Del Giudice, M.; Shirtcliff, E.A. The Adaptive Calibration Model of stress responsivity: Concepts, findings, and implications for developmental psychopathology. In Child and Adolescent Psychopathology; Beauchaine, T.P., Hinshaw, S.P., Eds.; John Wiley & Sons: New York, NY, USA, 2017; pp. 237–276. [Google Scholar]
- Champagne, F.A. Epigenetic influence of social experiences across the lifespan. Dev. Psychobiol. 2010, 52, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Oomen, C.A.; Soeters, H.; Audureau, N.; Vermunt, L.; Van Hasselt, F.N.; Manders, E.M.M.; Joëls, M.; Lucassen, P.J.; Krugers, H. Severe early life stress hampers spatial learning and neurogenesis, but improves hippocampal synaptic plasticity and emotional learning under high-stress conditions in adulthood. J. Neurosci. 2010, 30, 6635–6645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santarelli, S.; Lesuis, S.L.; Wang, X.-D.; Wagner, K.V.; Hartmann, J.; Labermaier, C.; Scharf, S.H.; Müller, M.B.; Holsboer, F.; Schmidt, M.V. Evidence supporting the match/mismatch hypothesis of psychiatric disorders. Eur. Neuropsychopharmacol. 2014, 24, 907–918. [Google Scholar] [CrossRef]
- Schmidt, M.V. Animal models for depression and the mismatch hypothesis of disease. Psychoneuroendocrinology 2011, 36, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Raby, K.L.; Verhage, M.L.; Fearon, R.M.P.; Fraley, R.C.; Roisman, G.I.; Van Ijzendoorn, M.H.; Schuengel, C.; Madigan, S.; Oosterman, M.; Bakermans-Kranenburg, M.J.; et al. The latent structure of the adult attachment interview: Large sample evidence from the collaboration on attachment transmission synthesis. Dev. Psychopathol. 2020, 1–13. [Google Scholar] [CrossRef]
- Bosmans, G. Cognitive behaviour therapy for children and adolescents: Can attachment theory contribute to its efficacy? Clin. Child Fam. Psychol. Rev. 2016, 19, 310–328. [Google Scholar] [CrossRef]
- Belsky, J.; Fearon, R.M.P. Infant–mother attachment security, contextual risk, and early development: A moderational analysis. Dev. Psychopathol. 2002, 14, 293–310. [Google Scholar] [CrossRef] [Green Version]
- Ellis, B.J.; Boyce, W.T.; Belsky, J.; Bakermans-Kranenburg, M.J.; Van Ijzendoorn, M.H. Differential susceptibility to the environment: An evolutionary- neurodevelopmental theory. Dev. Psychopathol. 2011, 23, 7–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casey, B.J.; Jones, R.M.; Levita, L.; Libby, V.; Pattwell, S.S.; Ruberry, E.J.; Soliman, F.; Somerville, L.H. The storm and stress of adolescence: Insights from human imaging and mouse genetics. Dev. Psychobiol. 2010, 52, 225–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyrell, F.A.; Yates, T.M.; Widaman, K.F.; Reynolds, C.A.; Fabricius, W.V. Data harmonization: Establishing measurement invariance across different assessments of the same construct across adolescence. J. Clin. Child Adolesc. Psychol. 2019, 48, 555–567. [Google Scholar] [CrossRef] [Green Version]
- Roisman, G.I.; Van Ijzendoorn, M.H. Meta-analysis and idndividual participant data synthesis in child evelopment: Introduction to the special section. Child Dev. 2018, 89, 1939–1942. [Google Scholar] [CrossRef] [PubMed]
- Mayr, E. How to carry out the adaptationist program? Am. Nat. 1983, 121, 324–334. [Google Scholar] [CrossRef]
- Schmitt, D.P.; Pilcher, J.J. Evaluating evidence of psychological adaptation: How do we know one when we see one? Psychol. Sci. 2004, 15, 643–649. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year) | Attachment Measures | Most Prevalent Symptoms Measures | Attachment Group Comparison | k | N | Cohen’s d (95% CI) | Heterogeneity |
|---|---|---|---|---|---|---|---|
| CHILDHOOD | |||||||
| Groh et al. (2012) [60] | SSP | CBCL | A versus B+C+D | 22 | 3119 | 0.17 (0.03, 0.31) | Q(21) = 32.82 * |
| C versus B+A+D | 21 | 3078 | 0.03 (−0.11, 0.17) | Q(20) = 26.05 | |||
| Madigan et al. (2013) [53] | SSP | CBCL, TRF | A versus B | 21 | 1852 | 0.29 (0.12, 0.45) | Q(20) = 33.78 * |
| C versus B | 21 | 1823 | 0.10 (−0.12, 0.32) | Q(20) = 30.11 * | |||
| A versus C | 19 | 664 | −0.17 (−0.41, 0.06) | Q(18) = 48.35 ** | |||
| ADOLESCENCE AND ADULTHOOD | |||||||
| Dagan et al. (2018) [61] | AAI | BDI, CES-D | Ds versus F | 43 | 2881 | 0.09 (−0.03, 0.22) | Q(42) = 90.68 *** |
| E versus F | 38 | 2079 | 0.48 (0.30, 0.65) | Q(37) = 71.90 *** | |||
| E versus Ds | 37 | 1285 | 0.34 (0.19, 0.50) | Q(36) = 47.65 | |||
| Dagan et al. (2020) [62] | AAI | BSI, SCL-90-R | Ds versus F | 50 | 4376 | −0.02 (−0.10, 0.05) | Q(49) = 68.09 * |
| E versus F | 42 | 3271 | 0.35 (0.19, 0.50) | Q(41) = 99.53 *** | |||
| E versus Ds | 41 | 2184 | 0.31 (0.15, 0.47) | Q(40) = 88.99 *** | |||
| Dominant Support Figures | Appropriate Orientation Tendency | Hyperactivating Strategies | Deactivating Strategies | |||
|---|---|---|---|---|---|---|
| Childhood | Parental figures | Toward parental caregivers | Match | (Excessive) orientation tendency toward parental caregivers | Mismatch | Avoiding proximity to parental caregivers |
| Post-Childhood | Non-parental figures | Away (i.e., toward greater independence) from parental caregivers | Mismatch | Enmeshment with parental caregivers | Match | (Excessive) orientation tendency away (i.e., toward greater independence) from parental caregivers |
| Attachment Group | Prediction |
|---|---|
| (a) Continuous deactivation | Decrease in internalizing symptoms from childhood to post-childhood |
| (b) Child deactivation→ Post-childhood hyperactivation | Stable high internalizing symptoms across development |
| (c) Child hyperactivation→ Post-childhood deactivation | Stable low internalizing symptoms across development |
| (d) Continuous hyperactivation | Increase in internalizing symptoms from childhood to post-childhood |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dagan, O.; Groh, A.M.; Madigan, S.; Bernard, K. A Lifespan Development Theory of Insecure Attachment and Internalizing Symptoms: Integrating Meta-Analytic Evidence via a Testable Evolutionary Mis/Match Hypothesis. Brain Sci. 2021, 11, 1226. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091226
Dagan O, Groh AM, Madigan S, Bernard K. A Lifespan Development Theory of Insecure Attachment and Internalizing Symptoms: Integrating Meta-Analytic Evidence via a Testable Evolutionary Mis/Match Hypothesis. Brain Sciences. 2021; 11(9):1226. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091226
Chicago/Turabian StyleDagan, Or, Ashley M. Groh, Sheri Madigan, and Kristin Bernard. 2021. "A Lifespan Development Theory of Insecure Attachment and Internalizing Symptoms: Integrating Meta-Analytic Evidence via a Testable Evolutionary Mis/Match Hypothesis" Brain Sciences 11, no. 9: 1226. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091226