
Serum Activin A as Brain Injury Biomarker in the First Three Days of Life. A Prospective Case—Control Longitudinal Study in Human Premature Neonates

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
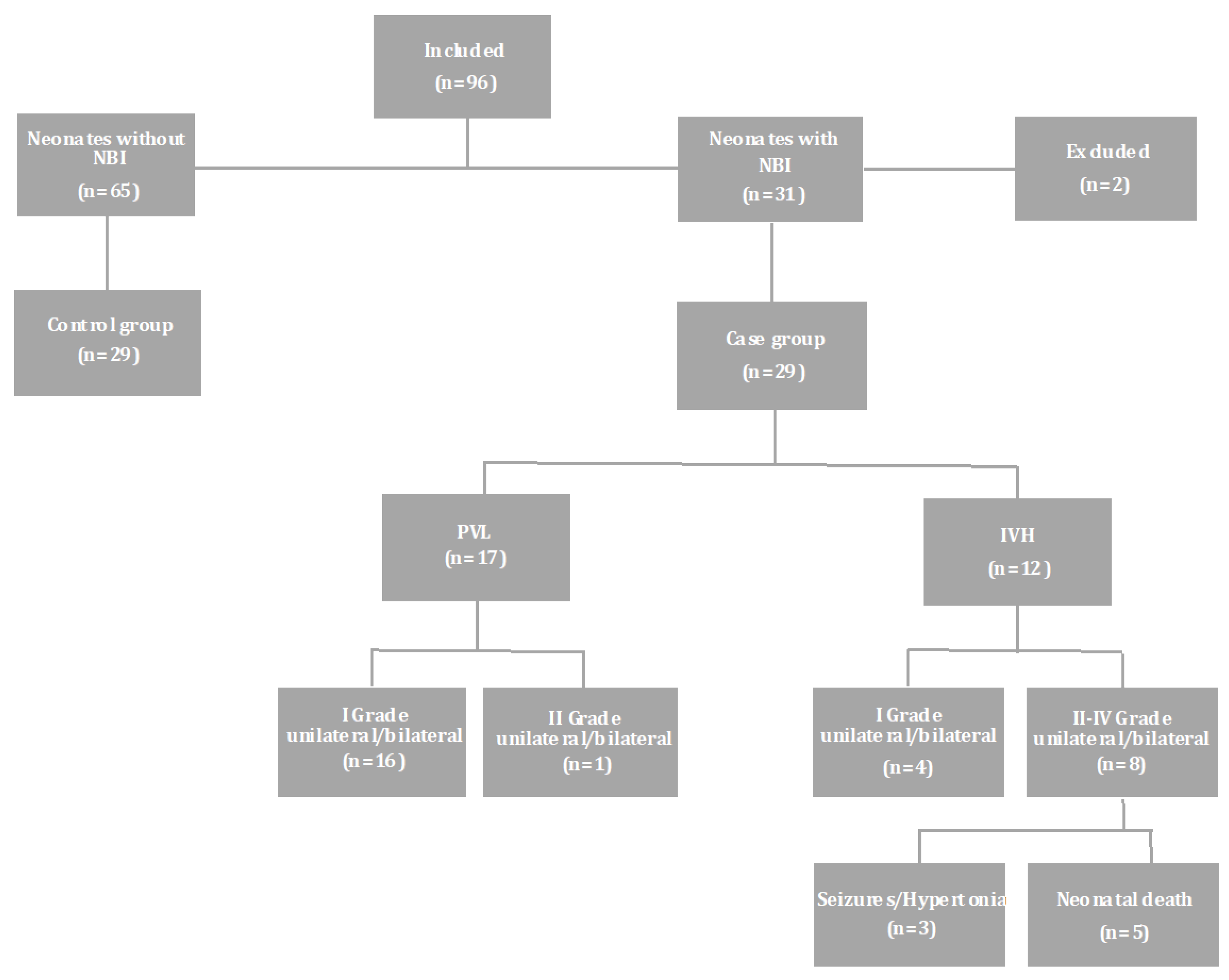
2.1. Study Design
2.2. Clinical Assessment and Laboratory Data
2.3. Definitions and Classifications
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahya, K.P.; Suryawanshi, P. Neonatal periventricular leukomalacia: Current perspectives. Res. Rep. Neonatol. 2018, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Gopagondanahalli, K.R.; Li, J.; Fahey, M.; Hunt, R.W.; Jenkin, G.; Miller, S.; Malhotra, A. Preterm Hypoxic–Ischemic Encephalopathy. Front. Pediatr. 2016, 4, 114. [Google Scholar] [CrossRef] [Green Version]
- Coskun, Y.; Isik, S.; Bayram, T.; Urgun, K.; Sakarya, S.; Akman, I. A clinical scoring system to predict the development of intraventricular hemorrhage (IVH) in premature infants. Child’s Nerv. Syst. 2017, 34, 129–136. [Google Scholar] [CrossRef]
- Larroque, B.; Ancel, P.-Y.; Marret, S.; Marchand, L.; André, M.; Arnaud, C.; Pierrat, V.; Rozé, J.-C.; Messer, J.; Thiriez, G.; et al. Neurodevelopmental disabilities and special care of 5-year-old children born before 33 weeks of gestation (the EPIPAGE study): A longitudinal cohort study. Lancet 2008, 371, 813–820. [Google Scholar] [CrossRef]
- Wang, K.K.; Yang, Z.; Zhu, T.; Shi, Y.; Rubenstein, R.; Tyndall, J.A.; Manley, G.T. An update on diagnostic and prognostic biomarkers for traumatic brain injury. Expert Rev. Mol. Diagn. 2018, 18, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Prout, A.J.; Wolf, M.S.; Fink, E.L. Translating biomarkers from research to clinical use in pediatric neurocritical care. Curr. Opin. Pediatr. 2017, 29, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Chalak, L.F. Inflammatory Biomarkers of Birth Asphyxia. Clin. Perinatol. 2016, 43, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Bersani, I.; Pluchinotta, F.; Dotta, A.; Savarese, I.; Campi, F.; Auriti, C.; Chuklantseva, N.; Piersigilli, F.; Gazzolo, F.; Varrica, A.; et al. Early predictors of perinatal brain damage: The role of neurobiomarkers. Clin. Chem. Lab. Med. 2020, 58, 471–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florio, P.; Gazzolo, D.; Luisi, S.; Petraglia, F. Activin A In Brain Injury. Adv. Appl. Microbiol. 2007, 43, 117–130. [Google Scholar] [CrossRef]
- Sannia, A.; Zimmermann, L.J.; Gavilanes, A.W.; Vles, H.J.; Calevo, M.G.; Florio, P.; Gazzolo, D. Elevated Activin A urine levels are predictors of intraventricular haemorrhage in preterm newborns. Acta Paediatr. 2013, 102, e449–e454. [Google Scholar] [CrossRef]
- Dillenburg, A.; Ireland, G.; Holloway, R.K.; Davies, C.L.; Evans, F.L.; Swire, M.; Bechler, M.E.; Soong, D.; Yuen, T.J.; Su, G.; et al. Activin receptors regulate the oligodendrocyte lineage in health and disease. Acta Neuropathol. 2018, 135, 887–906. [Google Scholar] [CrossRef] [Green Version]
- Goebbels, S.; Wieser, G.L.; Pieper, A.; Spitzer, S.; Weege, B.; Yan, K.; Edgar, J.M.; Yagensky, O.; Wichert, S.P.; Agarwal, A.; et al. A neuronal PI(3,4,5)P3-dependent program of oligodendrocyte precursor recruitment and myelination. Nat. Neurosci. 2016, 20, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Bloise, E.; Ciarmela, P.; Cruz, C.D.; Luisi, S.; Petraglia, F.; Reis, F.M. Activin A in Mammalian Physiology. Physiol. Rev. 2019, 99, 739–780. [Google Scholar] [CrossRef]
- Su, X.; Huang, L.; Xiao, D.; Qu, Y.; Mu, D. Research Progress on the Role and Mechanism of Action of Activin A in Brain Injury. Front. Neurosci. 2018, 12, 697. [Google Scholar] [CrossRef] [PubMed]
- Manickam, M.; Tulsawani, R. Survival Response of Hippocampal Neurons under Low Oxygen Conditions Induced by Hippophae rhamnoides is Associated with JAK/STAT Signaling. PLoS ONE 2014, 9, e87694. [Google Scholar] [CrossRef]
- Shahid, A.D.; Zhu, H.; Lu, H.Y.; Chang, M.; Malik, A.; Sher, M.A.; Adil, W.U. The early prognosis value of activ-in A in premature infants’ brain injury. Int. Res. J. Med. Med. Sc. 2017, 5, 14–18. [Google Scholar] [CrossRef]
- Elfarargy, M.S.; Eltomey, M.A.; Soliman, N.A. Early predictors of neonatal intraventricular hemorrhage. Electron. Physician 2017, 9, 4946–4951. [Google Scholar] [CrossRef] [Green Version]
- Florio, P.; Perrone, S.; Luisi, S.; Vezzosi, P.; Longini, M.; Marzocchi, B.; Petraglia, F.; Buonocore, G. Increased Plasma Concentrations of Activin A Predict Intraventricular Hemorrhage in Preterm Newborns. Clin. Chem. 2006, 52, 1516–1521. [Google Scholar] [CrossRef] [Green Version]
- Florio, P.; Perrone, S.; Luisi, S.; Longini, M.; Tanganelli, D.; Petraglia, F.; Buonocore, G. Activin A Plasma Levels at Birth: An Index of Fetal Hypoxia in Preterm Newborn. Pediatr. Res. 2003, 54, 696–700. [Google Scholar] [CrossRef] [Green Version]
- Fiala, M.; Baumert, M.; Walencka, Z.; Paprotny, M. Umbilical activin A concentration as an early marker of perinatal hypoxia. J. Matern. Neonatal Med. 2012, 25, 2098–2101. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Huang, W.; Chen, X.; Wang, Q.; Zhang, Q.; Chang, M. Relationship between premature brain injury and multiple biomarkers in cord blood and amniotic fluid. J. Matern. Neonatal Med. 2017, 31, 2898–2904. [Google Scholar] [CrossRef]
- Metallinou, D.; Karampas, G.; Nyktari, G.; Iacovidou, N.; Lykeridou, K.; Rizos, D. S100B as a biomarker of brain injury in premature neonates. A prospective case–control longitudinal study. Clin. Chim. Acta 2020, 510, 781–786. [Google Scholar] [CrossRef]
- Metallinou, D.; Karampas, G.; Nyktari, G.; Iacovidou, N.; Lykeridou, K.; Rizos, D. Serum glial fibrillary acidic protein as a biomarker of brain injury in premature neonates. Bosn. J. Basic Med. Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- Portelli, M.; Baron, B. Clinical Presentation of Preeclampsia and the Diagnostic Value of Proteins and Their Methylation Products as Biomarkers in Pregnant Women with Preeclampsia and Their Newborns. J. Pregnancy 2018, 2018, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mushtaq, E.; Parveen, S.; Shaheen, F.; Jan, S.; Abdullah, A.; Lone, Y.A. Perinatal Outcome in Patients with Isolated Oligohydramnios at Term: A Prospective Study. J. Pregnancy Child. Health 2017, 4, 1–5. [Google Scholar] [CrossRef]
- McNeil, A.; Stanford, P. Reporting Thyroid Function Tests in Pregnancy. Clin. Biochem. Rev. 2015, 36, 109–126. [Google Scholar]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.; International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, R.; Chaemsaithong, P.; Korzeniewski, S.; Kusanovic, J.P.; Docheva, N.; Martinez-Varea, A.; Ahmed, A.I.; Yoon, B.H.; Hassan, S.S.; Chaiworapongsa, T.; et al. Clinical chorioamnionitis at term III: How well do clinical criteria perform in the identification of proven intra-amniotic infection? J. Périnat. Med. 2015, 44, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Louis, G.M.B.; Grewal, J.; Albert, P.S.; Sciscione, A.; Wing, D.A.; Grobman, W.A.; Newman, R.B.; Wapner, R.; D’Alton, M.E.; Skupski, D.; et al. Racial/ethnic standards for fetal growth: The NICHD Fetal Growth Studies. Am. J. Obstet. Gynecol. 2015, 213, 449.e1–449.e41. [Google Scholar] [CrossRef]
- Ciobanu, A.; Wright, A.; Syngelaki, A.; Wright, D.; Akolekar, R.; Nicolaides, K.H. Fetal Medicine Foundation reference ranges for umbilical artery and middle cerebral artery pulsatility index and cerebroplacental ratio. Ultrasound Obstet. Gynecol. 2019, 53, 465–472. [Google Scholar] [CrossRef]
- Papile, L.-A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1,500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Romero-Guzman, G.J.; Lopez-Munoz, F. Prevalence and risk factors for periventricular leukomalacia in preterm infants. A systematic review. Rev. Neurol. 2017, 65, 57–62. [Google Scholar]
- Dudink, J.; Hellström-Westas, L.; Zimmermann, L.; Buonocore, G.; Gressens, P.; Pellicer, A.; European Standards of Care for Newborn Health. European Standards of Care for Newborn Health: Neurological Monitoring in the High-Risk Infant: Ultrasound and MRI Scanning. 2018. Available online: https://newborn-health-standards.org/ultrasound-and-mri/ (accessed on 15 July 2021).
- Mukerji, S.S.; Katsman, E.A.; Wilber, C.; Haner, N.A.; Selman, W.R.; Hall, A.K. Activin is a Neuronal Survival Factor that is Rapidly Increased after Transient Cerebral Ischemia and Hypoxia in Mice. Br. J. Pharmacol. 2007, 27, 1161–1172. [Google Scholar] [CrossRef] [Green Version]
- Emoretti, R.; Epansiot, J.; Ebettati, D.; Estrazielle, N.; Ghersi-Egea, J.-F.; Edamante, G.; Fleiss, B.; Etitomanlio, L.; Egressens, P. Blood-brain barrier dysfunction in disorders of the developing brain. Front. Neurosci. 2015, 9, 40. [Google Scholar] [CrossRef] [Green Version]
- Abdel Wahed, M.A.; Khafagy, S.M.; Abdel-Al, H.; El-Sayed, R.F. Serum activin A as a predictor of intraventricular hemorrhage in preterm neonates. JNPM 2012, 4, 241–245. [Google Scholar]
- Florio, P. Biochemical markers of perinatal brain damage. Front. Biosci. 2010, S2, 47–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinojosa-Rodríguez, M.; Harmony, T.; Carrillo-Prado, C.; Van Horn, J.D.; Irimia, A.; Torgerson, C.; Jacokes, Z. Clinical neuroimaging in the preterm infant: Diagnosis and prognosis. NeuroImage Clin. 2017, 16, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Ment, L.R.; Bada, H.S.; Barnes, P.; Grant, P.E.; Hirtz, D.; Papile, L.A.; Pinto–Martin, J.; Rivkin, M.; Slovis, T.L. Practice parameter: Neuroimaging of the neonate. Neurology 2002, 58, 1726–1738. [Google Scholar] [CrossRef] [Green Version]
- Sewell, E.K.; Andescavage, N.N. Neuroimaging for Neurodevelopmental Prognostication in High-Risk Neonates. Clin. Perinatol. 2018, 45, 421–437. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable N | Control 29 | Cases 29 | p-Value |
|---|---|---|---|
| Maternal age (years) | 38.4 ± 5.8 | 37.9 ± 5.7 | 0.764 |
| Gestational age (weeks) | 29.8 ± 2.5 | 29.6 ± 3.0 | 0.817 |
| Parity, n (%) | |||
| Nullipara | 22 (76) | 22 (76) | >0.99 |
| Multipara | 7 (24) | 7 (24) | |
| Race, n (%) | |||
| Caucasian | 29 (100%) | 29 (100%) | >0.99 |
| Conception, n (%) | |||
| Normal | 9 (31) | 11(38) | |
| IVF 1 | 20 (69) | 18 (62) | 0.581 |
| Gestation, n (%) | |||
| Single | 13 (45) | 8 (28) | |
| Multiple | 16 (55) | 21 (72) | 0.172 |
| Caesarean delivery, n (%) | 28 (97) | 25 (86%) | 0.160 |
| Preterm premature rupture of membranes, n (%) | 9 (31) | 9 (31) | >0.99 |
| Preeclampsia, n (%) | 4 (14) | 1 (3.5) | 0.160 |
| Oligohydramnios, n (%) | 2 (7) | 2 (7) | >0.99 |
| Hypothyroidism, n (%) | 15 (52) | 11 (38) | 0.291 |
| Insulin dependent gestational diabetes mellitus, n (%) | 4 (14) | 2 (7) | 0.389 |
| Abnormal Doppler, n (%) | 3 (10) | 6 (20) | 0.277 |
| Antenatal steroid administration, n (%) | 25 (86) | 23 (79) | 0.487 |
| Neonates with PVL 2 | 16/17 | 0.019 * | |
| Neonates with IVH 3 | 7/12 | ||
| Antenatal magnesium sulphate administration, n (%) | 11 (38) | 15 (52) | 0.291 |
| Abruptio placenta, n (%) | 1 (3.5) | 1 (3.5) | >0.99 |
| Clinical chorioamnionitis, n (%) | 7 (24) | 3 (10) | 0.164 |
| Variable N | Control Group 29 | Case Group 29 | p-Value |
|---|---|---|---|
| Sex, n (%) | |||
| Male | 13 (45) | 12 (41) | |
| Female | 16 (55) | 17 (59) | 0.791 |
| Apgar score, median (IQR) 1 | |||
| 1st min | 8 (2) | 8 (3) | 0.089 |
| 5th min | 9 (1) | 9 (1) | 0.665 |
| Apgar score < 7, n (%) | |||
| 1st min | 5 (17) | 9 (31) | 0.220 |
| 5th min | 0 (0) | 1 (3.5) | 0.274 |
| Birthweight (gr) | 1302 ± 429 | 1225 ± 475 | 0.517 |
| Body weight on discharge (gr) | 2837 ± 576 | 2613 ± 385 | 0.134 |
| Head circumference at birth (cm) | 27.5 ± 2.5 | 27.0 ± 3.2 | 0.533 |
| Head circumference on discharge (cm) | 33.5 ± 1.4 | 33.5 ± 1.1 | 0.915 |
| Admission, arterial blood | |||
| pH | 7.37 ± 0.01 | 7.29 ± 0.16 | 0.033 * |
| Base deficit, mmol/L | 4.29 ± 1.92 | 7.22 ± 6.59 | 0.037 * |
| pCO2, mmHg | 38 ± 10 | 40 ± 10 | 0.371 |
| HCO3, mmol/L | 20 ± 2 | 19 ± 5 | 0.087 |
| Lactic acid, mmol/L | 3.1 ± 1.2 | 4.8 ± 4.3 | 0.05 * |
| Hb, g/dL | 16.5 ± 3.0 | 16.9 ± 2.0 | 0.438 |
| WBC 2 count, K/µL | 11456 ± 9550 | 9153 ± 5562 | 0.05 * |
| CRP 3, mg/L | 1.0 ± 0.2 | 1.3 ± 1.5 | 0.998 |
| Positive CRP at admission, n (%) | 14 (48) | 12 (41) | 0.597 |
| CRP 2nd day, mg/L | 6.1 ± 8.7 | 4.9 ± 8.7 | 0.294 |
| CRP 3rd day, mg/L | 7.6 ± 11.1 | 6.0 ± 7.5 | 0.809 |
| Variable N | Control Group 29 | Case Group 29 | p-Value |
|---|---|---|---|
| Surfacant administration n (%) | 21 (72) | 22 (76) | 0.764 |
| Inotrops, n (%) | 14 (48) | 20 (69) | 0.145 |
| Caffeine, n (%) | 26 (90) | 25 (86) | 0.687 |
| Cardiopulmonary resuscitation, n (%) | 3 (10) | 6 (20) | 0.277 |
| Patent ductus arteriosus treatment, n (%) | 8 (28) | 8 (28) | >0.99 |
| 2 | 0 | ||
| Paracetamol | 5 | 7 | |
| Ibuprofen | 1 | 1 | |
| Surgery | |||
| High frequency ventilation, n (%) | 4 (14) | 7 (24) | 0.315 |
| Transfusion, n (%) | 3 (10) | 7 (24) | 0.164 |
| Outcome N | Control Group 29 | Case Group 29 | p-Value |
|---|---|---|---|
| Seizures, n (%) | 0 (0) | 6 (20) | 0.01 * |
| Hypertonia, n (%) | 0 (0) | 2 (7) | 0.15 |
| Death, n (%) | 0 (0) | 5 (17) | 0.019 * |
| Neonates with PVL 1 | 0/17 | ||
| Neonates with IVH 2 | 5/12 | 0.015 * | |
| Positive blood culture, n (%) | 1 (3.5) | 2 (7) | 0.553 |
| Positive cerebrospinal fluid culture, n (%) | 0 (0) | 1 (3.5) | 0.274 |
| Clinical neonatal sepsis, n (%) | 1 (3.5) | 2 (7) | 0.553 |
| Respiratory distress syndrome, n (%) | 21 (72) | 23 (79) | 0.539 |
| Chronic lung disease, n (%) | 6/27 (22) | 5/21 (24) | 0.897 |
| Necrotizing enterocolitis, n (%) | 6 (20) | 1 (3.5) | 0.044 * |
| Otoacoustic Emissions Test negative, n (%) | 7/23 (30) | 9/21 (43) | 0.392 |
| Automated auditory brainstem response test negative, n (%) | 4/11 (36) | 4/10 (40) | 0.864 |
| Length of stay in NICU 3, days | 63 ± 48 | 45 ± 30 | 0.089 |
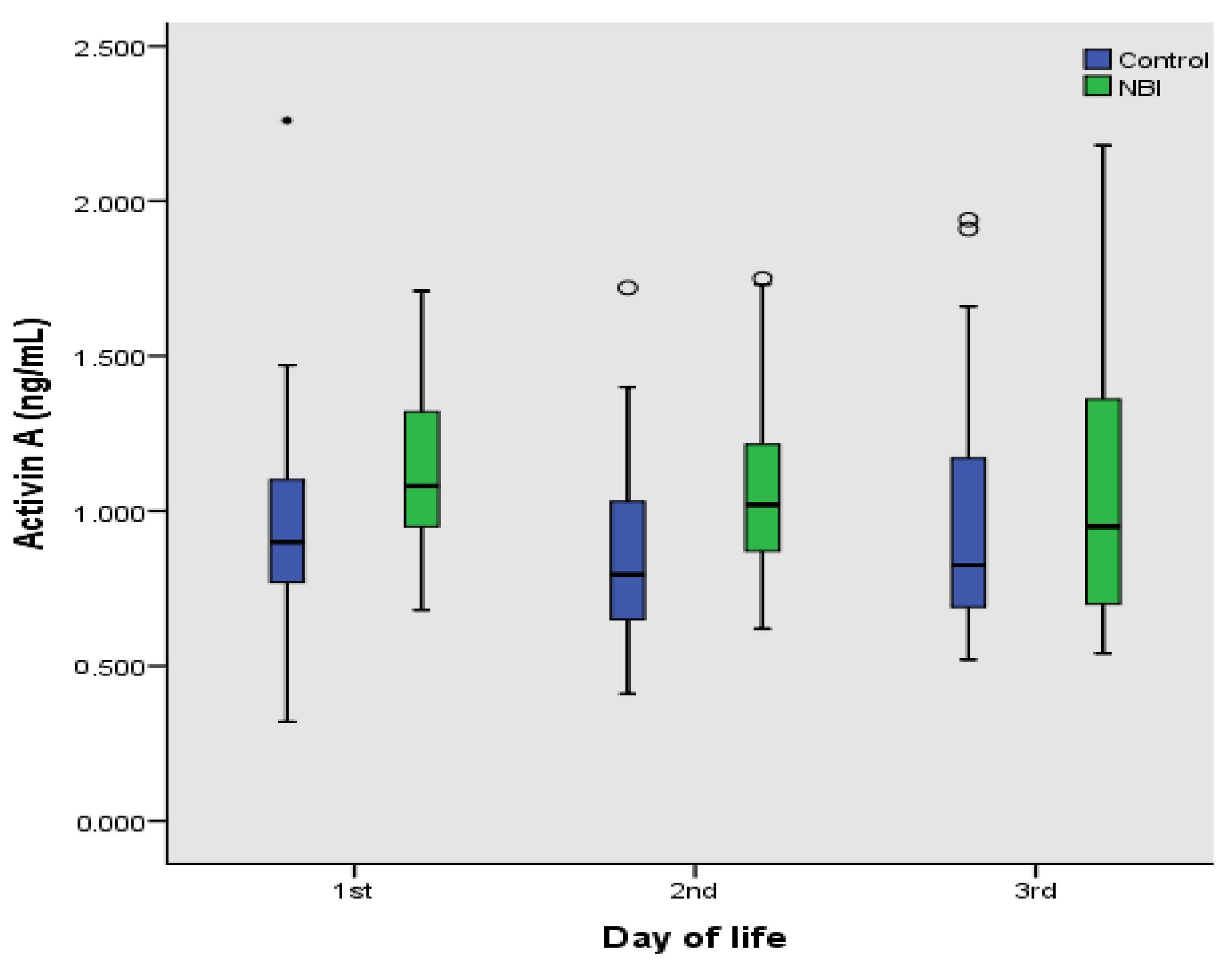
| Control | Cases | |
|---|---|---|
| N | 29 | 29 |
| 1st day | ||
| Mean ± SD | 0.914 ± 0.361 | 1.109 ± 0.287 * |
| 2nd day | ||
| Mean ± SD | 0.873 ± 0.311 | 1.06 ± 0.291 ** |
| 3rd day | ||
| Mean ± SD | 0.987 ± 0.403 | 1.057 ± 0.436 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Metallinou, D.; Karampas, G.; Lazarou, E.; Iacovidou, N.; Pervanidou, P.; Lykeridou, K.; Mastorakos, G.; Rizos, D. Serum Activin A as Brain Injury Biomarker in the First Three Days of Life. A Prospective Case—Control Longitudinal Study in Human Premature Neonates. Brain Sci. 2021, 11, 1243. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091243
Metallinou D, Karampas G, Lazarou E, Iacovidou N, Pervanidou P, Lykeridou K, Mastorakos G, Rizos D. Serum Activin A as Brain Injury Biomarker in the First Three Days of Life. A Prospective Case—Control Longitudinal Study in Human Premature Neonates. Brain Sciences. 2021; 11(9):1243. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091243
Chicago/Turabian StyleMetallinou, Dimitra, Grigorios Karampas, Eleftheria Lazarou, Nikoletta Iacovidou, Panagiota Pervanidou, Katerina Lykeridou, George Mastorakos, and Demetrios Rizos. 2021. "Serum Activin A as Brain Injury Biomarker in the First Three Days of Life. A Prospective Case—Control Longitudinal Study in Human Premature Neonates" Brain Sciences 11, no. 9: 1243. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091243