
Hot and Cold Cognitive Disturbances in Parkinson Patients Treated with DBS-STN: A Combined PET and Neuropsychological Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Primary Outcomes
2.3.1. Cognitive Measures
2.3.2. Mood State Measures
2.3.3. Brain Imaging with PET [11C]AZ10419369
2.4. Statistical Analyses
3. Results
3.1. Baseline Data
3.1.1. Cold and Hot Cognition
3.1.2. Mood States
3.2. Correlations between Cognition and [11C]AZ10419369 PET
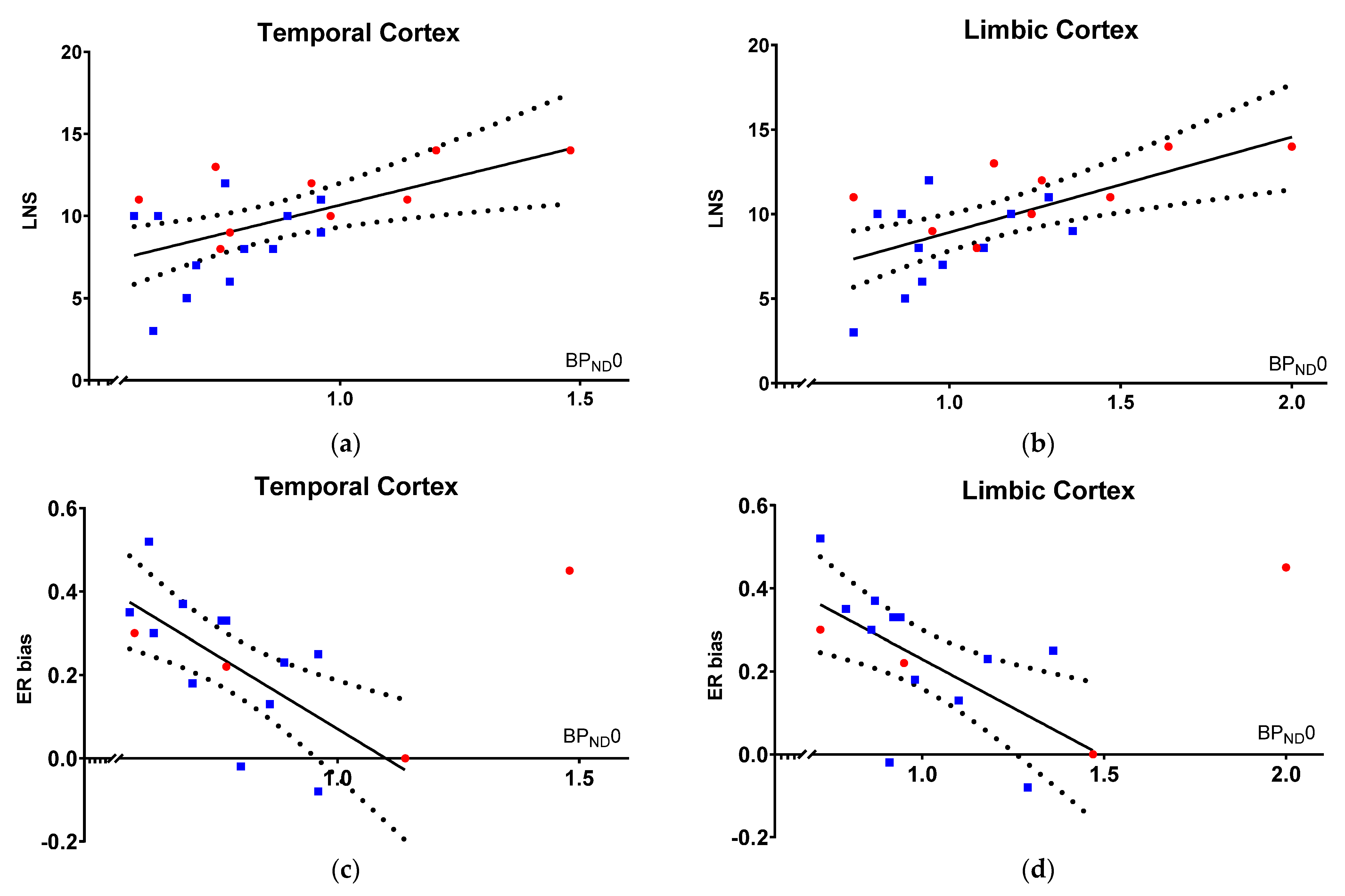
3.2.1. Cold Cognition Correlates with BPND0
3.2.2. Hot Cognition Correlates with BPND0
3.3. Turning DBS-STN Off
3.3.1. Effects on Mood States
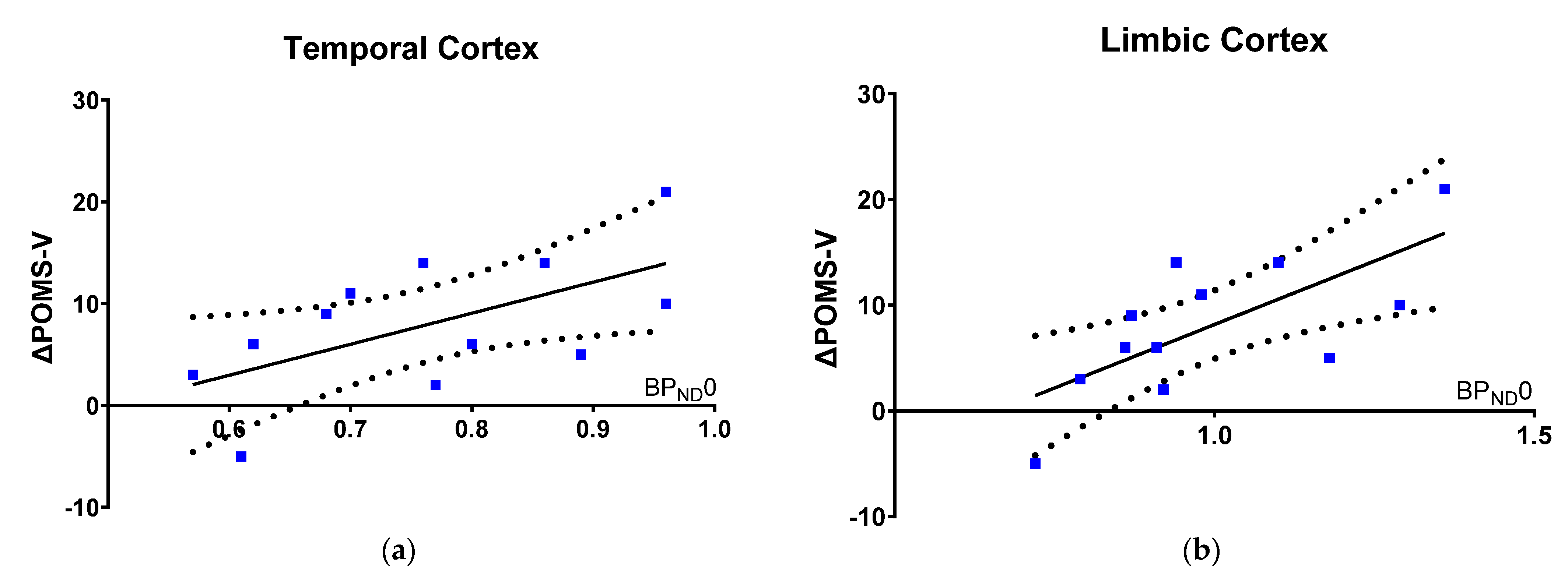
3.3.2. Worsening in Mood State Correlates with [11C]AZ10419369 PET
4. Discussion
4.1. Baseline Cognition
4.2. Association to [11C]AZ10419369 PET
4.3. Turning DBS-STN Off
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goetz, C.G.; Pal, G. Initial Management of Parkinson’s Disease. BMJ 2014, 349, g6258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Politis, M.; Niccolini, F. Serotonin in Parkinson’s Disease. Behav. Brain Res. 2015, 277, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Huot, P.; Fox, S.H.; Brotchie, J.M. The Serotonergic System in Parkinson’s Disease. Prog. Neurobiol. 2011, 95, 163–212. [Google Scholar] [CrossRef] [PubMed]
- Barnes, N.M.; Sharp, T. A Review of Central 5-HT Receptors and Their Function. Neuropharmacology 1999, 38, 1083–1152. [Google Scholar] [CrossRef]
- Goldman, J.G.; Postuma, R. Premotor and Non-Motor Features of Parkinson’s Disease. Curr. Opin. Neurol. 2014, 27, 434. [Google Scholar] [CrossRef] [Green Version]
- Müller, C.P.; Jacobs, B.L. Handbook of the Behavioral Neurobiology of Serotonin, 1st ed.; Elsevier BV: London, UK, 2010; ISBN 978-0-12-374634-4. [Google Scholar]
- Müller, B.; Assmus, J.; Herlofson, K.; Larsen, J.P.; Tysnes, O.-B. Importance of Motor vs. Non-Motor Symptoms for Health-Related Quality of Life in Early Parkinson’s Disease. Parkinsonism Relat. Disord. 2013, 19, 1027–1032. [Google Scholar] [CrossRef]
- Politis, M.; Wu, K.; Molloy, S.; Bain, P.G.; Chaudhuri, K.R.; Piccini, P. Parkinson’s Disease Symptoms: The Patient’s Perspective. Mov. Disord. 2010, 25, 1646–1651. [Google Scholar] [CrossRef]
- Keren, G.; Schul, Y. Two Is Not Always Better Than One: A Critical Evaluation of Two-System Theories. Perspect. Psychol. Sci. 2009, 4, 533–550. [Google Scholar] [CrossRef]
- Evans, J.S.B.T. Dual-Processing Accounts of Reasoning, Judgment, and Social Cognition. Annu. Rev. Psychol. 2008, 59, 255–278. [Google Scholar] [CrossRef] [Green Version]
- Elliott, R.; Zahn, R.; Deakin, J.F.W.; Anderson, I.M. Affective Cognition and Its Disruption in Mood Disorders. Neuropsychopharmacology 2011, 36, 153–182. [Google Scholar] [CrossRef] [Green Version]
- Miskowiak, K.W.; Carvalho, A.F. “Hot” Cognition in Major Depressive Disorder: A Systematic Review. CNS Neurol. Disord. Drug Targets 2014, 13, 1787–1803. [Google Scholar] [CrossRef]
- Calev, A. Affect and Memory in Depression: Evidence of Better Delayed Recall of Positive than Negative Affect Words. PSP 1996, 29, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Bland, A.R.; Roiser, J.P.; Mehta, M.A.; Schei, T.; Boland, H.; Campbell-Meiklejohn, D.K.; Emsley, R.A.; Munafo, M.R.; Penton-Voak, I.S.; Seara-Cardoso, A.; et al. EMOTICOM: A Neuropsychological Test Battery to Evaluate Emotion, Motivation, Impulsivity, and Social Cognition. Front. Behav. Neurosci. 2016, 10, 25. [Google Scholar] [CrossRef] [PubMed]
- Kurtis, M.M.; Rajah, T.; Delgado, L.F.; Dafsari, H.S. The Effect of Deep Brain Stimulation on the Non-Motor Symptoms of Parkinson’s Disease: A Critical Review of the Current Evidence. NPJ Parkinson’s Dis. 2017, 3, 16024. [Google Scholar] [CrossRef] [PubMed]
- Dam, V.H.; Thystrup, C.K.; Jensen, P.S.; Bland, A.R.; Mortensen, E.L.; Elliott, R.; Sahakian, B.J.; Knudsen, G.M.; Frokjaer, V.G.; Stenbæk, D.S. Psychometric Properties and Validation of the EMOTICOM Test Battery in a Healthy Danish Population. Front. Psychol. 2019, 10, 2660. [Google Scholar] [CrossRef] [Green Version]
- Hjordt, L.V.; Ozenne, B.; Armand, S.; Dam, V.H.; Jensen, C.G.; Köhler-Forsberg, K.; Knudsen, G.M.; Stenbæk, D.S. Psychometric Properties of the Verbal Affective Memory Test-26 and Evaluation of Affective Biases in Major Depressive Disorder. Front. Psychol. 2020, 11, 961. [Google Scholar] [CrossRef]
- Jørgensen, L.M.; Henriksen, T.; Mardosiene, S.; Keller, S.H.; Stenbæk, D.S.; Hansen, H.D.; Jespersen, B.; Thomsen, C.; Weikop, P.; Svarer, C.; et al. Parkinson Patients Have a Presynaptic Serotonergic Deficit: A Dynamic Deep Brain Stimulation PET Study. J. Cereb. Blood Flow Metab. 2021, 41, 1954–1963. [Google Scholar] [CrossRef]
- Garcia-Cordero, I.; Migeot, J.; Fittipaldi, S.; Aquino, A.; Campo, C.G.; García, A.; Ibáñez, A. Metacognition of Emotion Recognition across Neurodegenerative Diseases. Cortex 2021, 137, 93–107. [Google Scholar] [CrossRef]
- Voon, V.; Kubu, C.; Krack, P.; Houeto, J.-L.; Tröster, A.I. Deep Brain Stimulation: Neuropsychological and Neuropsychiatric Issues. Mov. Disord. 2006, 21, S305–S327. [Google Scholar] [CrossRef]
- Castrioto, A.; Lhommée, E.; Moro, E.; Krack, P. Mood and Behavioural Effects of Subthalamic Stimulation in Parkinson’s Disease. Lancet Neurol. 2014, 13, 287–305. [Google Scholar] [CrossRef] [Green Version]
- Da Cunha-Bang, S.; Hjordt, L.V.; Dam, V.H.; Stenbæk, D.S.; Sestoft, D.; Knudsen, G.M. Anterior Cingulate Serotonin 1B Receptor Binding Is Associated with Emotional Response Inhibition. J. Psychiatr. Res. 2017, 92, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Deen, M.; Hansen, H.D.; Hougaard, A.; da Cunha-Bang, S.; Nørgaard, M.; Svarer, C.; Keller, S.H.; Thomsen, C.; Ashina, M.; Knudsen, G.M. Low 5-HT1B Receptor Binding in the Migraine Brain: A PET Study. Cephalalgia 2018, 38, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.J.; Lopez, S.J. Wechsler Adult Intelligence Scale-III. In Understanding Psychological Assessment; Dorfman, W.I., Hersen, M., Eds.; Perspectives on Individual Differences; Springer: Boston, MA, USA, 2001; pp. 19–42. ISBN 978-1-4615-1185-4. [Google Scholar]
- McNair, D.M.; Heuchert, P. Profile of Mood States: POMS: Technical Update; Multi-Health Systems: North Tonawanda, NY, USA, 2007. [Google Scholar]
- Da Cunha-Bang, S.; Hjordt, L.V.; Perfalk, E.; Beliveau, V.; Bock, C.; Lehel, S.; Thomsen, C.; Sestoft, D.; Svarer, C.; Knudsen, G.M. Serotonin 1B Receptor Binding Is Associated With Trait Anger and Level of Psychopathy in Violent Offenders. Biol. Psychiatry 2017, 82, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Chen, M.-K.; Endres, C.J.; Ye, W.; Brašić, J.R.; Alexander, M.; Crabb, A.H.; Guilarte, T.R.; Wong, D.F. An Extended Simplified Reference Tissue Model for the Quantification of Dynamic PET with Amphetamine Challenge. NeuroImage 2006, 33, 550–563. [Google Scholar] [CrossRef]
- Jørgensen, L.M.; Weikop, P.; Svarer, C.; Feng, L.; Keller, S.H.; Knudsen, G.M. Cerebral Serotonin Release Correlates with [11C]AZ10419369 PET Measures of 5-HT1B Receptor Binding in the Pig Brain. J. Cereb. Blood Flow Metab. 2018, 38, 1243–1252. [Google Scholar] [CrossRef] [Green Version]
- Maillet, A.; Krack, P.; Lhommée, E.; Météreau, E.; Klinger, H.; Favre, E.; Le Bars, D.; Schmitt, E.; Bichon, A.; Pelissier, P.; et al. The Prominent Role of Serotonergic Degeneration in Apathy, Anxiety and Depression in de Novo Parkinson’s Disease. Brain 2016, 139, 2486–2502. [Google Scholar] [CrossRef] [Green Version]
- Pool, E.; Brosch, T.; Delplanque, S.; Sander, D. Attentional Bias for Positive Emotional Stimuli: A Meta-Analytic Investigation. Psychol. Bull. 2016, 142, 79–106. [Google Scholar] [CrossRef]
- Assogna, F.; Pontieri, F.E.; Caltagirone, C.; Spalletta, G. The Recognition of Facial Emotion Expressions in Parkinson’s Disease. Eur. Neuropsychopharmacol. 2008, 18, 835–848. [Google Scholar] [CrossRef]
- Schroeder, U.; Kuehler, A.; Hennenlotter, A.; Haslinger, B.; Tronnier, V.; Krause, M.; Pfister, R.; Sprengelmeyer, R.; Lange, K.; Ceballos-Baumann, A. Facial Expression Recognition and Subthalamic Nucleus Stimulation. J. Neurol. Neurosurg. Psychiatry 2004, 75, 648–650. [Google Scholar] [CrossRef]
- Dujardin, K.; Blairy, S.; Defebvre, L.; Krystkowiak, P.; Hess, U.; Blond, S.; Destee, A. Subthalamic Nucleus Stimulation Induces Deficits in Decoding Emotional Facial Expressions in Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2004, 75, 202–208. [Google Scholar]
- Fölster, M.; Hess, U.; Werheid, K. Facial Age Affects Emotional Expression Decoding. Front. Psychol. 2014, 5, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaacowitz, D.M.; Stanley, J.T. Bringing an Ecological Perspective to the Study of Aging and Recognition of Emotional Facial Expressions: Past, Current, and Future Methods. J. Nonverbal Behav. 2011, 35, 261–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprengelmeyer, R.; Rausch, M.; Eysel, U.T.; Przuntek, H. Neural Structures Associated with Recognition of Facial Expressions of Basic Emotions. Proc. Biol. Sci. 1998, 265, 1927–1931. [Google Scholar] [CrossRef] [Green Version]
- Dam, V.H.; Stenbæk, D.S.; Köhler-Forsberg, K.; Ip, C.; Ozenne, B.; Sahakian, B.J.; Knudsen, G.M.; Jørgensen, M.B.; Frokjaer, V.G. Hot and Cold Cognitive Disturbances in Antidepressant-Free Patients with Major Depressive Disorder: A NeuroPharm Study. Psychol. Med. 2020, 51, 2347–2356. [Google Scholar] [CrossRef] [PubMed]
- Varrone, A.; Svenningsson, P.; Forsberg, A.; Varnäs, K.; Tiger, M.; Nakao, R.; Halldin, C.; Nilsson, L.-G.; Farde, L. Positron Emission Tomography Imaging of 5-Hydroxytryptamine1B Receptors in Parkinson’s Disease. Neurobiol. Aging 2014, 35, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Lou, J.-S. Fatigue in Parkinson’s Disease and Potential Interventions. NeuroRehabilitation 2015, 37, 25–34. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Healthy Controls | Parkinson’s Disease | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Range | n | Mean | SD | Range | n | |
| Cold Cognition | ||||||||
| Working memory (LNS) | 11.3 | 1.9 | [8–14] | 11 | 8.3 * | 2.6 | [3–12] | 12 |
| Hot Cognition | ||||||||
| Verbal affective memory (VAMT-26 bias) | 0.2 | 1.1 | [−1.9–2.5] | 11 | −0.5 | 1.2 | [−2.6–1.1] | 12 |
| Face recognition (ER bias) | 23.4 | 16.4 | [0–45] | 5 | 24.1 | 16.9 | [−8–52] | 12 |
| Mood state | ||||||||
| Profile of Mood State (POMS-TMD) | −6.5 | 14.6 | [−19–21] | 11 | −6.5 | 15.0 | [−20–24] | 12 |
| [11C]AZ10419369 PET (a) | ||||||||
| Temporal cortex (BPND0) | 0.95 | 0.25 | [0.58–1.48] | 10 | 0.79 | 0.15 | [0.72–1.39] | 13 |
| Limbic cortex (BPND0) | 1.28 | 0.32 | [0.72–2.00] | 10 | 1.02 | 0.21 | [0.57–1.11] | 13 |
| Temporal cortex (ΔBPND (%)) | 3 | 11 | [−19–20] | 10 | −11 | 9 | [−29–1] | 13 |
| Limbic cortex (ΔBPND (%)) | 2 | 7 | [−17–12] | 10 | −9 | 12 | [−27–9] | 13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jørgensen, L.M.; Henriksen, T.; Mardosiene, S.; Wyon, O.; Keller, S.H.; Jespersen, B.; Knudsen, G.M.; Stenbæk, D.S. Hot and Cold Cognitive Disturbances in Parkinson Patients Treated with DBS-STN: A Combined PET and Neuropsychological Study. Brain Sci. 2022, 12, 654. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050654
Jørgensen LM, Henriksen T, Mardosiene S, Wyon O, Keller SH, Jespersen B, Knudsen GM, Stenbæk DS. Hot and Cold Cognitive Disturbances in Parkinson Patients Treated with DBS-STN: A Combined PET and Neuropsychological Study. Brain Sciences. 2022; 12(5):654. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050654
Chicago/Turabian StyleJørgensen, Louise M., Tove Henriksen, Skirmante Mardosiene, Ottilia Wyon, Sune H. Keller, Bo Jespersen, Gitte M. Knudsen, and Dea S. Stenbæk. 2022. "Hot and Cold Cognitive Disturbances in Parkinson Patients Treated with DBS-STN: A Combined PET and Neuropsychological Study" Brain Sciences 12, no. 5: 654. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050654