
The Applicability of Acceptance and Commitment Therapy for Obsessive-Compulsive Disorder: A Systematic Review and Meta-Analysis


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Selection of Studies
2.2. Extraction of Data and Assessment of Study Quality
2.3. Statistical Analysis
3. Results
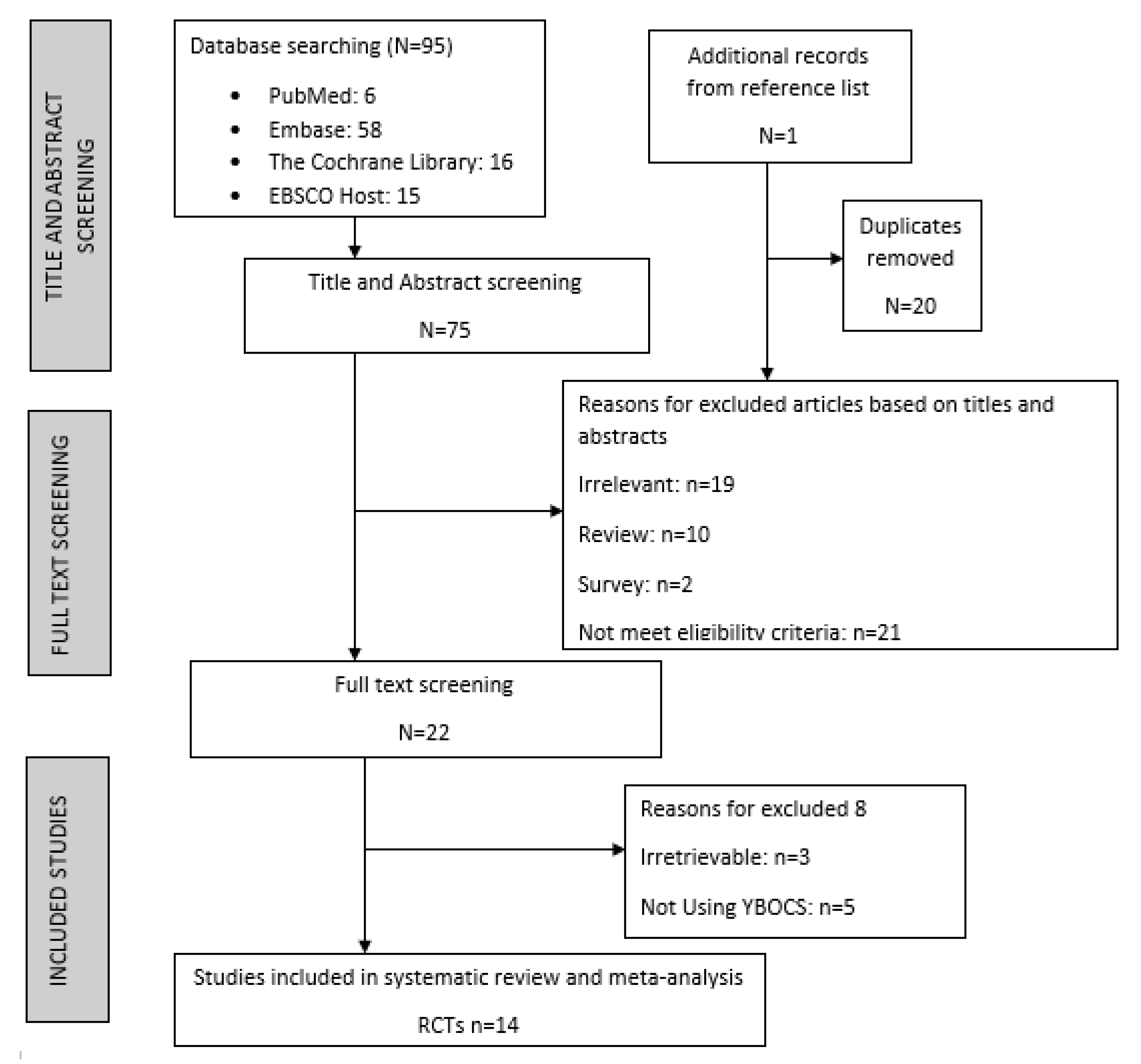
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Research Evidence on ACT for OCD
3.4. Risks of Bias of Included Studies
3.5. Meta-Analysis Results
3.6. Subgroup Analyses
4. Discussion
4.1. Main Findings
4.2. ACT and Waitlist
4.3. ACT and SSRIs
4.4. ACT, ERP, and PRT
4.5. ACT in Case Series and Case Studies
4.6. Clinical Implications
5. Limitations and Further Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Edition, F. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013; Volume 21. [Google Scholar]
- Kessler, R.C.; Aguilar-Gaxiola, S.; Alonso, J.; Chatterji, S.; Lee, S.; Ormel, J.; Üstün, T.B.; Wang, P.S. The global burden of mental disorders: An update from the WHO World Mental Health (WMH) surveys. Epidemiol. E Psichiatr. Soc. 2009, 18, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Biglan, A.; Hayes, S.C. Should the behavioral sciences become more pragmatic? the case for functional contextualism in research on human behavior. Appl. Prev. Psychol. 1996, 5, 47–57. [Google Scholar] [CrossRef]
- Fineberg, N.A.; Reghunandanan, S.; Simpson, H.B.; Phillips, K.A.; Richter, M.A.; Matthews, K.; Stein, D.J.; Sareen, J.; Brown, A.; Sookman, D. Obsessive-compulsive disorder (OCD): Practical strategies for pharmacological and somatic treatment in adults. Psychiatry Res. 2015, 227, 114–125. [Google Scholar] [CrossRef]
- Ruscio, A.M.; Stein, D.J.; Chiu, W.T.; Kessler, R.C. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol. Psychiatry 2010, 15, 53–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couto, J.P.; Moreira, R. Oral N-acetylcysteine in the treatment of obsessive-compulsive disorder: A systematic review of the clinical evidence. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 86, 245–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antony, M.M.; Summerfeldt, L.J.; Skapinakis, P.; Caldwell, D.M.; Hollingworth, W.; Bryden, P.; Fineberg, N.A.; Salkovskis, P.; Welton, N.J.; Baxter, H.; et al. A systematic review and meta-analysis: Memantine augmentation in moderate to severe obsessive-compulsive disorder. Psychiatry Res. 2019, 28, 156–169. [Google Scholar] [CrossRef]
- Abramowitz, J.S.; Deacon, B.J.; Olatunji, B.O.; Wheaton, M.G.; Berman, N.C.; Losardo, D.; Timpano, K.R.; McGrath, P.B.; Riemann, B.C.; Adams, T.; et al. Assessment of Obsessive-Compulsive Symptom Dimensions: Development and Evaluation of the Dimensional Obsessive-Compulsive Scale. Psychol. Assess. 2010, 22, 180–198. [Google Scholar] [CrossRef] [PubMed]
- Law, C.; Boisseau, C.L. Exposure and response prevention in the treatment of obsessive-compulsive disorder: Current perspectives. Psychol. Res. Behav. Manag. 2019, 12, 1167–1174. [Google Scholar] [CrossRef] [Green Version]
- Öst, L.G. Efficacy of the third wave of behavioral therapies: A systematic review and meta-analysis. Behav. Res. Ther. 2008, 46, 296–321. [Google Scholar] [CrossRef]
- Harris, R. The House of ACT: Functional Contextualism, ABA and RFT. Book Chapter. In ACT Made Simple; New Harbinger Publications: Oakland, CA, USA, 2009; pp. 1–23. Available online: https://www.pensierocritico.eu/files/ACT_Made_Simple_Dr._Russ_Harris_preface.pdf (accessed on 10 May 2022).
- Hayes, S.; Barnes-Holmes, D.; Wilson, K. Contextual Behavioral Science: Creating a science more adequate to the challenge of the human condition. J. Contextual Behav. Sci. 2012, 1, 1–16. [Google Scholar] [CrossRef]
- Hayes, S.; Wilson, K.; Gifford, E.; Follette, V.; Strosahl, K. Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. J. Consult. Clin. Psychol. 1996, 64, 1152–1168. [Google Scholar] [CrossRef] [PubMed]
- Bouton, M.E.; Westbrook, R.F.; Corcoran, K.A.; Maren, S. Contextual and Temporal Modulation of Extinction: Behavioral and Biological Mechanisms. Biol. Psychiatry 2006, 60, 352–360. [Google Scholar] [CrossRef] [Green Version]
- Reed, P.; Morgan, T.A. Resurgence of Response Sequences During Extinction in Rats Shows a Primacy Effect. J. Exp. Anal. Behav. 2006, 86, 307–315. [Google Scholar] [CrossRef] [Green Version]
- Twohig, M.P. The Application of Acceptance and Commitment Therapy to Obsessive-Compulsive Disorder. Cogn. Behav. Pract. 2009, 16, 18–28. [Google Scholar] [CrossRef]
- Codd, R.T.; Twohig, M.P.; Crosby, J.M.; Enno, A. Treatment of three anxiety disorder cases with acceptance and commitment therapy in a private practice. J. Cogn. Psychother. 2011, 25, 203–217. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Asmundson, G.J.G. Acceptance and mindfulness-based therapy: New wave or old hat? Clin. Psychol. Rev. 2008, 28, 1–16. [Google Scholar] [CrossRef]
- Levin, M.E.; Hildebrandt, M.J.; Lillis, J.; Hayes, S.C. The Impact of Treatment Components Suggested by the Psychological Flexibility Model: A Meta-Analysis of Laboratory-Based Component Studies. Behav. Ther. 2012, 43, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Marcks, B.A.; Woods, D.W. Role of thought-related beliefs and coping strategies in the escalation of intrusive thoughts: An analog to obsessive-compulsive disorder. Behav. Res. Ther. 2007, 45, 2640–2651. [Google Scholar] [CrossRef] [PubMed]
- Bluett, E.J.; Homan, K.J.; Morrison, K.L.; Levin, M.E.; Twohig, M.P. Acceptance and commitment therapy for anxiety and OCD spectrum disorders: An empirical review. J. Anxiety Disord. 2014, 28, 612–624. [Google Scholar] [CrossRef]
- Philip, J.; Cherian, V. Acceptance and commitment therapy in the treatment of Obsessive-Compulsive Disorder: A systematic review. J. Obs.-Compuls. Relat. Disord. 2021, 28, 100603. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, W.K.; Price, L.H.; Rasmussen, S.A.; Mazure, C.; Fleischmann, R.L.; Hill, C.L.; Heninger, G.R.; Charney, D.S. YBOCS-goodman. Arch. Gen. Psychiatry 1989, 46, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Baer, L.; Brown-Beasley, M.W.; Sorce, J.; Henriques, A.I. Computer-assisted telephone administration of a structured interview for obsessive-compulsive disorder. Am. J. Psychiatry 1993, 150, 1737–1738. [Google Scholar] [PubMed]
- Steketee, G.; Frost, R.; Bogart, K. The Yale-Brown obsessive compulsive scale: Interview versus self-report. Behav. Res. Ther. 1996, 34, 675–684. [Google Scholar] [CrossRef]
- Mitchell, M.; Muftakhidinov, B.; Winchen, T.; Wilms, A.; van Schaik, B.; badshah400; Mo-Gul; Badger, T.G.; Jędrzejewski-Szmek, Z.; kensington; et al. Markummitchell/Engauge-Digitizer; Version 10.4 (10/10/2017) Nonrelease; Zenodo: Geneva, Switzerland, 2020. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Li, P.; Pan, C.; Dai, L.; Wu, Y.; Deng, Y. The Effect of Mind-Body Therapies on Insomnia: A Systematic Review and Meta-Analysis. Evid. -Based Complementary Altern. Med. 2019, 2019, 9359807. [Google Scholar] [CrossRef]
- Twohig, M.P.; Hayes, S.C.; Plumb, J.C.; Pruitt, L.D.; Collins, A.B.; Hazlett-Stevens, H.; Woidneck, M.R. A randomized clinical trial of acceptance and commitment therapy versus progressive relaxation training for obsessive-compulsive disorder. J. Consult. Clin. Psychol. 2010, 78, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Izadi, R.; Asgari, K.; Neshatdust, H.; Abedi, M. The Effect of Acceptance and Commitment Therapy on the Frequency and Severity of Symptoms of Obsessive Compulsive Disorder. Zahedan J. Res. Med. Sci. ZJRMS 2012, 14, 107–112. [Google Scholar]
- Dehlin, J.P.; Morrison, K.L.; Twohig, M.P. Acceptance and Commitment Therapy as a Treatment for Scrupulosity in Obsessive Compulsive Disorder. Behav. Modif. 2013, 37, 409–430. [Google Scholar] [CrossRef] [Green Version]
- Vakili, Y.; Gharraee, B. The effectiveness of acceptance and commitment therapy in treating a case of obsessive compulsive disorder. Iran. J. Psychiatry 2014, 9, 115–117. [Google Scholar]
- Baghooli, H.; Dolatshahi, B.; Mohammadkhani, P.; Moshtagh, N.; Naziri, G. Effectiveness of acceptance and commitment therapy in reduction of severity symptoms of patients with obsessive-compulsive disorder. Adv. Environ. Biol. 2014, 8, 2519–2524. [Google Scholar]
- Soomro, G.M.; Altman, D.G.; Rajagopal, S.; Browne, M.O. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). Cochrane Database Syst. Rev. 2008, 1, CD001765. [Google Scholar] [CrossRef]
- Esfahani, M.; Kjbaf, M.B.; Abedi, M.R. Evaluation and comparison of the effects of time perspective therapy, acceptance and commitment therapy and narrative therapy on severity of symptoms of Obsessive-Compulsive disorder. J. Indian Acad. Appl. Psychol. 2015, 41, 148–155. [Google Scholar]
- Vakili, Y.; Gharaee, B.; Habibi, M. Acceptance and commitment therapy, selective serotonin reuptake inhibitors, and their combination in the improvement of obsessive-compulsive symptoms and experiential avoidance in patients with obsessive-compulsive disorder. Iran. J. Psychiatry Behav. Sci. 2015, 9, 16–20. [Google Scholar] [CrossRef] [Green Version]
- Rohani, F.; Rasouli-Azad, M.; Twohig, M.P.; Ghoreishi, F.S.; Lee, E.B.; Akbari, H. Preliminary test of group acceptance and commitment therapy on obsessive-compulsive disorder for patients on optimal dose of selective serotonin reuptake inhibitors. J. Obs.-Compuls. Relat. Disord. 2018, 16, 8–13. [Google Scholar] [CrossRef]
- Twohig, M.P.; Abramowitz, J.S.; Smith, B.M.; Fabricant, L.E.; Jacoby, R.J.; Morrison, K.L.; Bluett, E.J.; Reuman, L.; Blakey, S.M.; Ledermann, T. Adding acceptance and commitment therapy to exposure and response prevention for obsessive-compulsive disorder: A randomized controlled trial. Behav. Res. Ther. 2018, 108, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ong, C.W.; Lee, E.B.; Krafft, J.; Terry, C.L.; Barrett, T.S.; Levin, M.E.; Twohig, M.P. A randomized controlled trial of acceptance and commitment therapy for clinical perfectionism. J. Obs.-Compuls. Relat. Disord. 2019, 22, 100444. [Google Scholar] [CrossRef] [Green Version]
- Thompson, B.L.; Twohig, M.P.; Luoma, J.B. Psychological Flexibility as Shared Process of Change in Acceptance and Commitment Therapy and Exposure and Response Prevention for Obsessive-Compulsive Disorder: A Single Case Design Study. Behav. Ther. 2021, 52, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Davazdahemami, M.H.; Bayrami, A.; Petersen, J.M.; Twohig, M.P.; Bakhtiyari, M.; Noori, M.; Kheradmand, A. Preliminary evidence of the effectiveness of acceptance and commitment therapy for death anxiety in Iranian clients diagnosed with obsessive-compulsive disorder. Bull. Menn. Clin. 2020, 84, 1–11. [Google Scholar] [CrossRef]
- Zemestani, M.; Ommati, P.; Rezaei, F.; Gallagher, M.W. Changes in neuroticism-related constructs over the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders in patients on an optimal dose of SSRI. Personal. Disord. 2021, 13, 171–181. [Google Scholar] [CrossRef]
- Öst, L.G. The efficacy of Acceptance and Commitment Therapy: An updated systematic review and meta-analysis. Behav. Res. Ther. 2014, 61, 105–121. [Google Scholar] [CrossRef]
- Van Ameringen, M.; Simpson, W.; Patterson, B.; Dell’Osso, B.; Fineberg, N.; Hollander, E.; Hranov, L.; Hranov, G.; Lochner, C.; Karamustafalioglu, O.; et al. Pharmacological treatment strategies in obsessive compulsive disorder: A cross-sectional view in nine international OCD centers. J. Psychopharmacol. 2014, 28, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Skapinakis, P.; Caldwell, D.M.; Hollingworth, W.; Bryden, P.; Fineberg, N.A.; Salkovskis, P.; Welton, N.J.; Baxter, H.; Kessler, D.; Churchill, R.; et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: A systematic review and network meta-analysis. Lancet Psychiatry 2016, 3, 730–739. [Google Scholar] [CrossRef] [Green Version]
- Zemestani, M.; Salavati, M.; Seyedolshohadayi, A.; Petersen, J.M.; Ong, C.W.; Twohig, M.P.; Ghaderi, E. A Preliminary Examination of Acceptance and Commitment Therapy Versus Exposure and Response Prevention for Patients with Obsessive-Compulsive Disorder on an Optimal Dose of SSRIs: A Randomized Controlled Trial in Iran. Behav. Modif. 2020, 46, 553–580. [Google Scholar] [CrossRef]
- Hezel, D.M.; Simpson, H.B. Exposure and response prevention for obsessive-compulsive disorder: A review and new directions. Indian J. Psychiatry 2019, 61 (Suppl 1), S85–S92. [Google Scholar] [CrossRef] [PubMed]
- Tolin, D.F. Alphabet Soup: ERP, CT, and ACT for OCD. Cogn. Behav. Pract. 2009, 16, 40–48. [Google Scholar] [CrossRef]
- Pinto, A.; Liebowitz, M.R.; Foa, E.B.; Simpson, H.B. Behaviour Research and Therapy Obsessive compulsive personality disorder as a predictor of exposure and ritual prevention outcome for obsessive compulsive disorder q. Behav. Res. Ther. 2011, 49, 453–458. [Google Scholar] [CrossRef] [Green Version]
- Twohig, M.P.; Vilardaga, J.C.P.; Levin, M.E.; Hayes, S.C. Changes in psychological flexibility during acceptance and commitment therapy for obsessive compulsive disorder. J. Contextual Behav. Sci. 2015, 4, 196–202. [Google Scholar] [CrossRef]
- Ducasse, D.; Fond, G. La thérapie d’ acceptation et d’ engagement. L’Encephale 2013, 41, 1–9. [Google Scholar] [CrossRef]
- Dindo, L.; Van Liew, J.R.; Arch, J.J. Acceptance and Commitment Therapy: A Transdiagnostic Behavioral Intervention for Mental Health and Medical Conditions. Neurotherapeutics 2017, 14, 546–553. [Google Scholar] [CrossRef] [Green Version]
- Hirschtritt, M.E.; Bloch, M.H.; Mathews, C.A. Obsessive-compulsive disorder advances in diagnosis and treatment. JAMA-J. Am. Med. Assoc. 2017, 317, 1358–1367. [Google Scholar] [CrossRef]
- Gambrill, E. Evidence-Based Practice and Policy: Choices Ahead. Res. Soc. Work. Pract. 2006, 16, 338–357. [Google Scholar] [CrossRef]
- Luoma, J.B.; Hayes, S.C.; Walser, R.D. Learning ACT: An Acceptance & Commitment Therapy Skills-Training Manual for Therapists; New Harbinger Publications: Oakland, CA, USA, 2007. [Google Scholar]
- Gu, B.M.; Park, J.Y.; Kang, D.H.; Lee, S.J.; Yoo, S.Y.; Jo, H.J.; Choi, C.H.; Lee, J.M.; Kwon, J.S. Neural correlates of cognitive inflexibility during task-switching in obsessive-compulsive disorder. Brain 2008, 131, 155–164. [Google Scholar] [CrossRef] [Green Version]
- Gruner, P.; Pittenger, C. Cognitive inflexibility in Obsessive-Compulsive Disorder. Neuroscience 2017, 345, 243–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albertella, L.; Le Pelley, M.E.; Chamberlain, S.R.; Westbrook, F.; Lee, R.S.C.; Fontenelle, L.F.; Grant, J.E.; Segrave, R.A.; McTavish, E.; Yücel, M. Reward-related attentional capture and cognitive inflexibility interact to determine greater severity of compulsivity-related problems. J. Behav. Ther. Exp. Psychiatry 2020, 69, 101580. [Google Scholar] [CrossRef]
- Dupuy, M.; Rouillon, F.; Bungener, C. Place de l’inhibition dans le trouble obsessionnel-compulsif. Encephale 2013, 39, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, S. Motor Inhibition and Cognitive Flexibility in Obsessive-Compulsive Disorder and Trichotillomania. Am. J. Psychiatry 2006, 163, 1282. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Fineberg, N.A.; Menzies, L.A.; Blackwell, A.D.; Bullmore, E.T.; Robbins, T.W.; Sahakian, B.J. Impaired cognitive flexibility and motor inhibition in unaffected first-degree relatives of patients with obsessive-compulsive disorder. Am. J. Psychiatry 2007, 164, 335–338. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study and Year | Design | Intervention and Control (N) | Duration | Outcome Measures | Outcome | Dropout |
|---|---|---|---|---|---|---|
| Twohig 2010 [30] | RCT | ACT—36 OCD patients PRT—33 | 8 sessions weekly ACT or PRT—1 h | YBOCS | ACT posttreatment = 46–56%, PRT posttreatment = 13–18% | 10% |
| Izadi 2012 [31] | Case Series | ACT—5 OCD patients | 10 weekly ACT sessions of 1 h | YBOCS | Scores of all subjects dropped below the previously established cutoff score of 18 on the YBOCS scale | NR |
| Dehlin et al., 2013 [32] | Case Series | ACT—5 Scrupulosity-based OCD patients | 8 sessions | YBOCS | Average daily compulsions reduced pretreatment = 25.0, posttreatment = 5.6, | NR |
| Vakili and Gharraee 2014 [33] | Case Study | ACT—1 OCD patient | 8 sessions of ACT with 1, 3, 6 months follow-up | YBOCS | Scores on YBOCS and BAI reduced by 15 points, i.e., 50% from the baseline | NR |
| Baghooli 2014 [34] | RCT | ACT—25 OCD patients SSRI—25 OCD patients | NR | YBOCS | ACT and combined treatment experienced a greater improvement in obsessive–compulsive symptoms at posttreatment compared to those treated with medication alone, and statistically significant | 5.9% |
| Izadi 2014 [35] | RCT | ACT—25 OCD patients Waitlist—12 patients | 10 sessions weekly for 2 h | YBOCS | ACT made significant changes in OCD symptoms | NR |
| Esfahani 2015 [36] | RCT | ACT—15 OCD patients Waitlist—12 patients | 10 sessions weekly, 1 h | YBOCS | ACT is more effective than TPT, NT | NR |
| Vakili 2015 [37] | RCT | ACT—9 OCD patients SSRI—9 patients | 10 weekly sessions | YBOCS | Unlike SSRI alone, ACT and combined treatment led to greater improvement in obsessive–compulsive symptoms and experiential avoidance | 1 patient |
| Rohani 2017 [38] | RCT | ACT + SSRI—23 OCD patients SSRI—23 patients | 8 weekly sessions | YBOCS | ACT as a successful adjunct to SSRI | |
| Twohig 2018 [39] | RCT | ACT + ERP—30 OCD patients ERP—28 patients | 16 sessions twice weekly ERP or ACT + ERP | YBOCS | Reduction rate in YBOCS: 70% ACT + ERP 68% ERP | 6.9% |
| Ong 2019 [40] | RCT | ACT—28 OCD patients with clinical perfectionism Waitlist—25 patients | 10 sessions of 50 min weekly | Frost Multidimensional Perfectionism Scale | ACT is feasible and efficacious, supporting a shift from symptom-focused to process-based care | 35.7% |
| Thompson 2020 [41] | Case Study | ACT—4 OCD patients | Varied number of sessions of ERP and ACT among patients | YBOCS | Both ACT and ERP can increase psychological flexibility | NR |
| Davazdahemanni 2020 [42] | Case Series | ACT—8 OCD patients with death anxiety | 8 weekly sessions of 45 min | YBOCS | 60–80% decrease in death anxiety, 51–60% decrease in OCD symptoms | NR |
| Zemestani 2021 [43] | RCT | ACT + SSRI—13 OCD patients SSRI—15 OCD | 12 individual weekly sessions of 90 min | YBOCS | Psychological inflexibility decreases in ACT + SSRI group | NR |
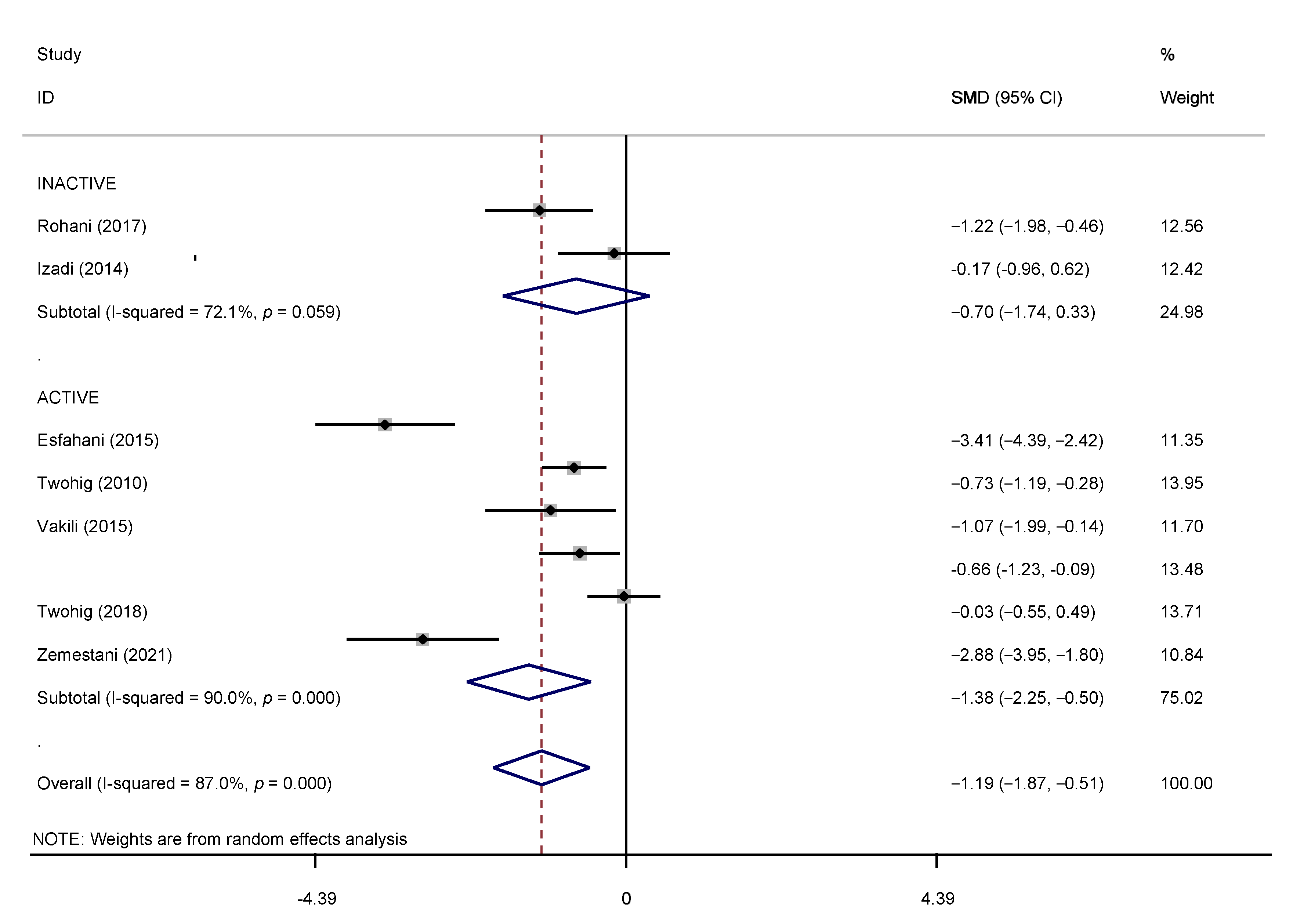
| Control Condition Type | Studies (N) | NO. Of Patients | SMDS (95% CI) | p-Value (Overall Effect) | I2-Value % | p-Value (Heterogeneity) |
|---|---|---|---|---|---|---|
| Overall | 8 | 366 | −1.19 (−1.87, −0.51) | 0.000 | 87% | 0.004 |
| Active | 6 | 279 | −1.38 (−2.248, −0.508) | 0.000 | 90% | 0.011 |
| Inactive | 2 | 87 | −0.702 (−1.735, −0.332) | 0.059 | 72.1% | 0.273 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soondrum, T.; Wang, X.; Gao, F.; Liu, Q.; Fan, J.; Zhu, X. The Applicability of Acceptance and Commitment Therapy for Obsessive-Compulsive Disorder: A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 656. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050656
Soondrum T, Wang X, Gao F, Liu Q, Fan J, Zhu X. The Applicability of Acceptance and Commitment Therapy for Obsessive-Compulsive Disorder: A Systematic Review and Meta-Analysis. Brain Sciences. 2022; 12(5):656. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050656
Chicago/Turabian StyleSoondrum, Tamini, Xiang Wang, Feng Gao, Qian Liu, Jie Fan, and Xiongzhao Zhu. 2022. "The Applicability of Acceptance and Commitment Therapy for Obsessive-Compulsive Disorder: A Systematic Review and Meta-Analysis" Brain Sciences 12, no. 5: 656. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050656