Investing in the Early Childhood Mental Health Workforce Development: Enhancing Professionals’ Competencies to Support Emotion and Behavior Regulation in Young Children


Abstract
:1. Introduction
1.1. The Importance of Adult–Child Relationships and Early Childhood Care and Education in Promoting Mental Health
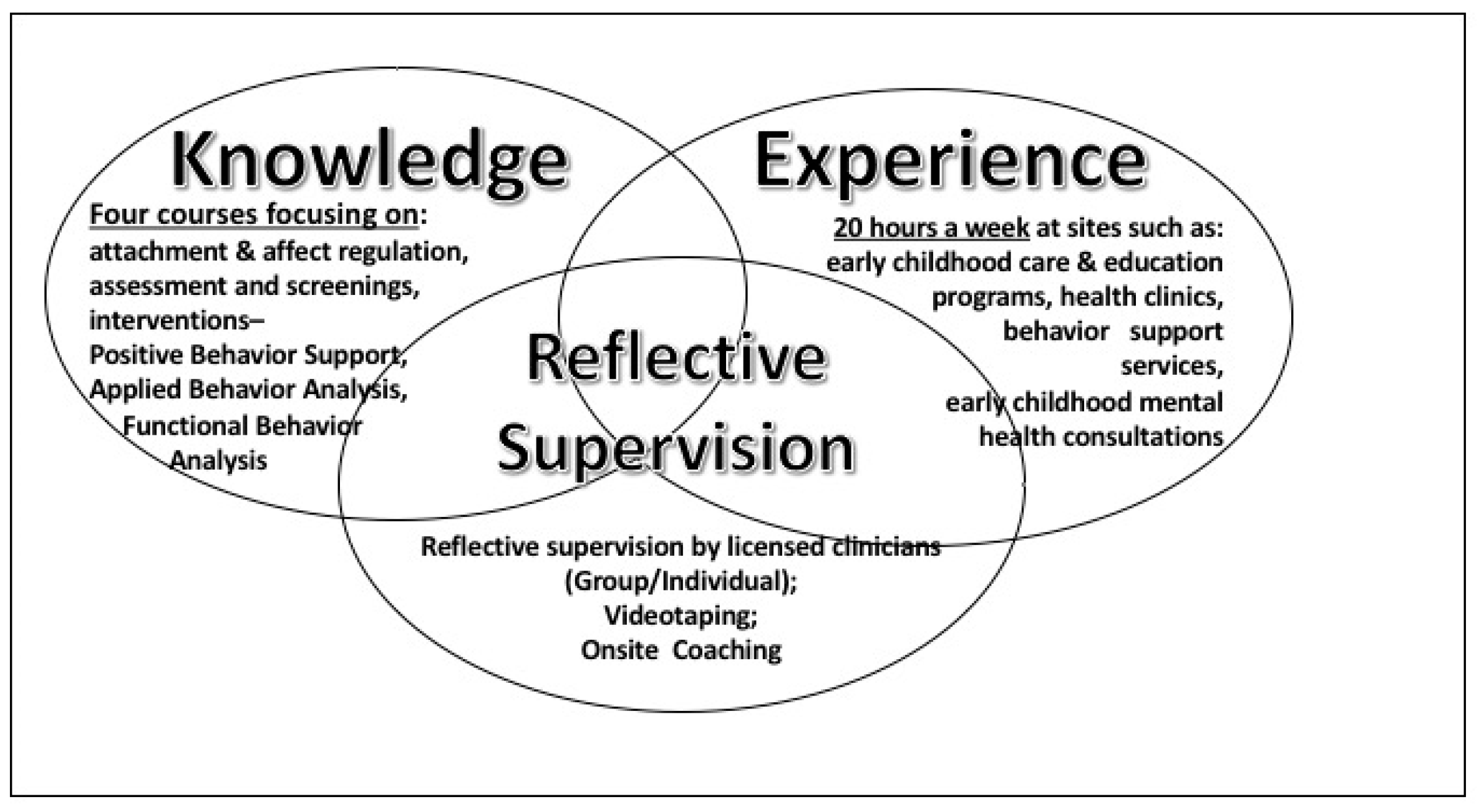
1.2. Training Model: Early Childhood Social Emotional and Behavior Regulation Intervention Specialist (EC-SEBRIS) Program
1.3. Evaluation of EC-SEBRIS Program
2. Materials and Methods
2.1. Participants
2.1.1. Students
2.1.2. Supervisors
2.1.3. Parents
2.2. Measures
2.2.1. The Caregiver Interaction Scale (CIS)
2.2.2. Supervisor Survey
2.2.3. Self-Efficacy (SE) Survey
2.2.4. Parent Survey
2.3. Procedure
3. Results
3.1. Question 1
3.1.1. Effects of Training on Students’ Competencies
3.1.2. Arnett Caregiver Interaction Scale (CIS)
3.1.3. Supervisor and Director Surveys on Student’s Performance
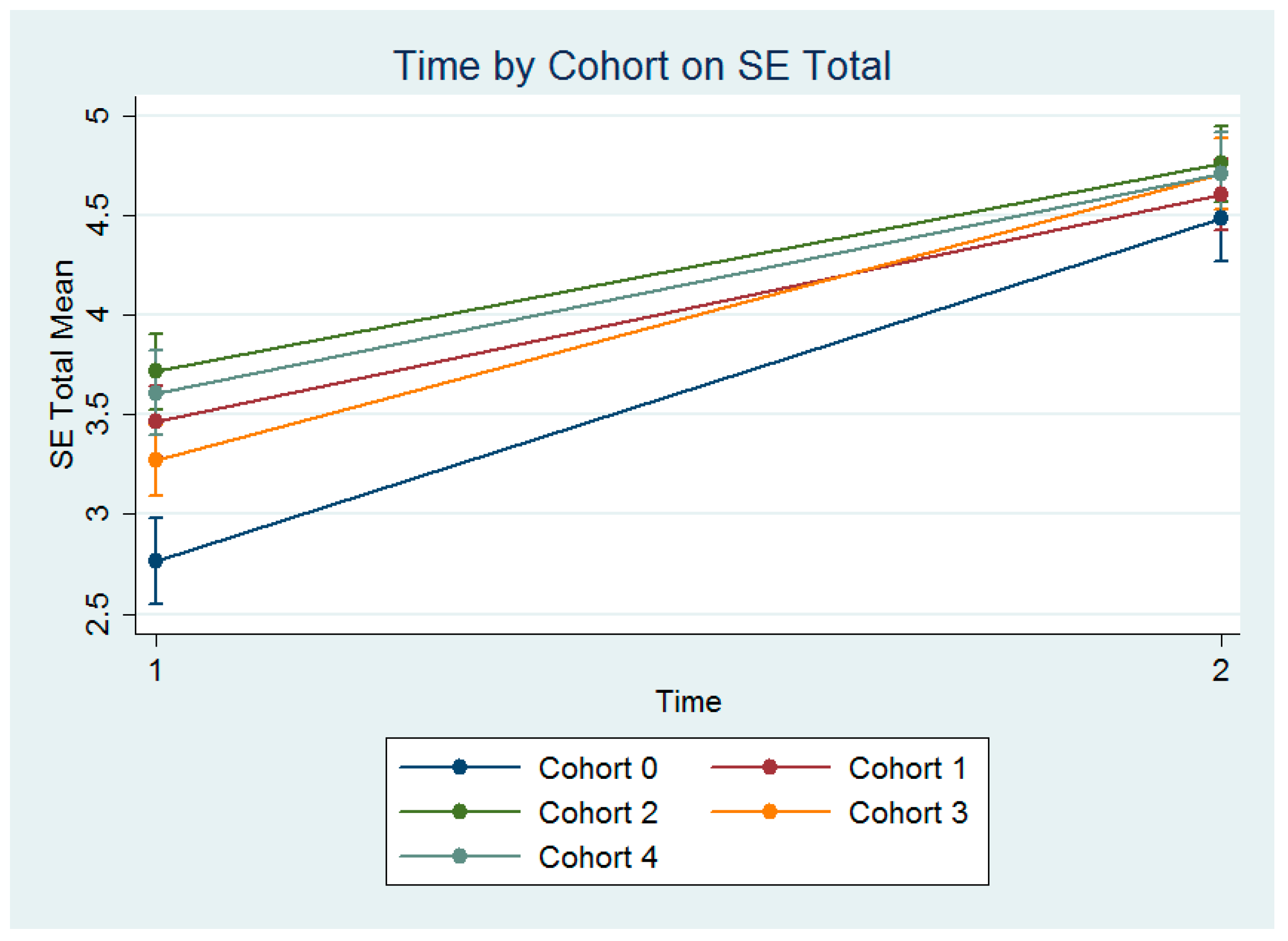
3.1.4. Self-Efficacy (SE)-Student’s Self Report
3.2. Question 2
Parent Surveys on Child’s Social Emotional Skills
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lynda, L. Who’s Minding the Kids? Child. Care Arrangements: Spring 2011; United States Census Bureau: Suitland, MD, USA, 2013.
- Zero to Three. Infants and Toddlers and the California Mental Health Services Act. 2007. Available online: http://ceo.lacounty.gov/ccp/pdf/mhsa_pei/03 Infants and Toddlers and MHSA.pdf (accessed on 20 June 2010).
- Strain, P.S.; Joseph, G.E. Engaged supervision to support recommended practices for young children with challenging behavior. Top. Early Child. Spec. Educ. 2004, 24, 39–50. [Google Scholar] [CrossRef]
- Gilliam, W.S. Prekindergarteners Left Behind: Expulsion Rates in State Kindergarten Programs; Foundation for Child Development (FCD): New York, NY, USA, 2005. [Google Scholar]
- Gilliam, W. Reducing Behavior Problems in Early Care and Education Programs: An Evaluation of Connecticut’s Early Childhood Consultation Partnership; Child Health and Development Institute of Connecticut, Inc.: Farmington, CT, USA, 2007. [Google Scholar]
- Costello, E.J.; Maughan, B. Annual research review: Optimal outcomes of child and adolescent mental illness. J. Child Psychol. Psychiatry 2015, 56, 324–341. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.B. Adult mental health disorders and their age at onset. Br. J. Psychiatry 2013, 202, s5–s10. [Google Scholar] [CrossRef] [PubMed]
- Van Der Ende, J.; Verhulst, C.F.; Tiemeier, H. The bidirectional pathways between internalizing and externalizing problems and academic performance from 6 to 18 years. Dev. Psychopathol. 2016, 28, 855–867. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.; Toth, S.L. Child maltreatment. Ann. Rev. Clin. Psychol. 2005, 1, 409–438. [Google Scholar] [CrossRef] [PubMed]
- DeWall, C.N.; Baumeister, R.F.; Stillman, T.F.; Gailliot, M.T. Violence restrained: Effects of self-regulation and its depletion on aggression. J. Exp. Soc. Psychol. 2007, 43, 62–76. [Google Scholar] [CrossRef]
- Eisenberg, N.; Spinrad, T.L.; Eggum, N.D. Emotion-related self-regulation and its relation to children’s maladjustment. Ann. Rev. Clin. Psychol. 2010, 6, 495–525. [Google Scholar] [CrossRef] [PubMed]
- Quinn, P.D.; Fromme, K. Self-regulation as a protective factor against risky drinking and sexual behavior. Psychol. Addict. Behav. 2010, 24, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Anzman-Frasca, S.; Stifter, C.A.; Birch, L.L. Temperament and childhood obesity risk: A review of the literature. J. Dev. Behav. Pediatr. 2012, 33, 732–745. [Google Scholar] [CrossRef] [PubMed]
- Graziano, P.A.; Calkins, S.D.; Keane, S.P. Toddler self-regulation skills predict risk for pediatric obesity. Int. J. Obes. 2010, 34, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Schwebel, D.C. Temperamental risk factors for children’s unintentional injury: The role of impulsivity and inhibitory control. Personal. Individ. Differ. 2004, 37, 567–578. [Google Scholar] [CrossRef]
- Center for Evidence-Based Practices: Young Children with Challenging Behavior. Prevention and Intervention with Young Children’s Challenging Behavior: A Consensus Based Summary of Current Knowledge; University of South Florida: Tampa, FL, USA, 2005. [Google Scholar]
- Blaze, J.; Roth, T.L. Caregiver maltreatment causes altered neuronal DNA methylation in female rodents. Dev. Psychopathol. 2017, 29, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Turp, M. Why love matters: How affection shapes a baby’s brain: A review. Infant Obs. 2006, 9, 305–309. [Google Scholar]
- Siegel, D.J.; Hartzell, M. Parenting from the Inside Out; Jeremy, P., Ed.; Tarcher/Penguin: New York, NY, USA, 2003. [Google Scholar]
- Anda, R.F.; Felitti, V.; Bremer, D.; Walker, J.; Whitfield, C.; Perry, B.; Dube, S.; Giles, W. The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Fisher, H.; Cohen-Woods, S.; Hosang, G.M.; Korszun, A.; Owen, M.; Craddock, N.; Craig, I.W.; Farmer, A.E.; McGuffin, P.; Uher, R. Interaction between specific forms of childhood maltreatment and the serotonin transporter gene (5-HTT) in recurrent depressive disorder. J. Affect. Disord. 2013, 145, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Shonkoff, J.; Fisher, P. Rethinking evidence-based practice and two-generation programs to create the future of early childhood policy. Dev. Psychopathol. 2013, 25, 1635–1653. [Google Scholar] [CrossRef] [PubMed]
- Meltzoff, A. Roots of social cognition: The like-me framework. In Minnesota Symposia on Child Psychology: Meeting the Challenge of Translational Research in Child Psychology; Cicchetti, D., Gunnar, M.R., Eds.; John Wiley: Hoboken, NJ, USA, 2009; pp. 29–55. [Google Scholar]
- Dalli, C.; White, E.J.; Rockel, J.; Duhn, I.; Buchanan, E.; Davidson, S.; Ganly, S.; Kus, L.; Wang, B. Quality Early Childhood Education for Under-Two-Year-Olds: What Should It Look Like? A literature Review; Report to the Ministry of Education; New Zealand Ministry of Education: Wellington, New Zealand, 2011.
- Herrod, H.G. Do first years really last a lifetime? Clin. Pediatr. 2007, 46, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Shonkoff, J.P. Building a new biodevelopmental framework to guide the future of early childhood policy. Child Dev. 2010, 81, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Center on the Developing Child at Harvard University. The Foundations of Lifelong Health Are Built in Early Childhood; Center on the Developing Child at Harvard University: Cambridge, MA, USA, 2010. [Google Scholar]
- National Scientific Council on the Developing Child Harvard University. Young Children Develop in an Environment of Relationships: Working Paper #1; Harvard University: Cambridge, MA, USA, 2004. [Google Scholar]
- National Scientific Council on the Developing Child. Children’s Emotional Development is Built into the Architecture of Their Brains: Working Paper #2; Harvard University: Cambridge, MA, USA, 2004. [Google Scholar]
- National Scientific Council on the Developing Child. Excessive Stress Disrupts the Architecture of the Developing Brain: Working Paper #3; Harvard University: Cambridge, MA, USA, 2005. [Google Scholar]
- National Scientific Council on the Developing Child. The Science of Early Childhood Development: Closing the Gap between what We Do and What We Know; Harvard University: Cambridge, MA, USA, 2007. [Google Scholar]
- Roisman, G.I.; Barnett-Walker, K.; Owen, M.T.; Bradley, R.H.; Steinberg, L.; Susman, E.; Booth-LaForce, C.; Belsky, J.; Houts, R. Early family and child-care antecedents of awakening cortisol levels in adolescence. Child Dev. 2009, 80, 907–920. [Google Scholar] [CrossRef] [PubMed]
- Watamura, S.; Donzella, B.; Alwin, J.; Gunnar, M.R. Morning-to-afternoon increases in cortisol concentrations for infants and toddlers at child care age differences and behavioral correlates. Child Dev. 2003, 74, 1006–1020. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, S. Why Love Matters: How Affection Shapes a Baby’s Brain; Routledge: London, UK, 2004. [Google Scholar]
- Gunnar, M.R.; Donzella, B. Social regulation of the cortisol levels in early human development. Psychoneuroendocrinology 2002, 27, 199–220. [Google Scholar] [CrossRef]
- Sabol, T.; Pianta, R.C. Recent trends in research on teacher-child relationships. Attach. Hum. Dev. 2012, 14, 213–231. [Google Scholar] [CrossRef] [PubMed]
- Buyse, E.; Verschueren, K.; Verachtert, P.; Van Damme, J. Predicting school adjustment in early elementary school: Impact of teacher-child relationship quality and relational classroom climate. Elem. Sch. J. 2009, 110, 119–141. [Google Scholar] [CrossRef]
- Baker, J.A.; Grant, S.; Morlock, L. The teacher-student relationship as a developmental context for children with internalizing or externalizing behavior problems. Sch. Psychol. Q. 2008, 23, 3–15. [Google Scholar] [CrossRef]
- Birch, S.H.; Ladd, G.W. The teacher-child relationship and children’s early school adjustment. J. Sch. Psychol. 1997, 35, 61–79. [Google Scholar] [CrossRef]
- Colwell, M.J.; Lindsey, E.W. Preschool Children’s Conflict and Social Competence: A Comparative View; Undergraduate Research Community: Okemos, MI, USA, 2000. [Google Scholar]
- Howes, C. 2000 Social-emotional classroom climate in child care, child-teacher relationships and children’s second grade peer relations. Soc. Dev. 2000, 9, 191–204. [Google Scholar] [CrossRef]
- Ladd, G.W.; Birch, S.H.; Buhs, E.S. Children’s social and scholastic lives in kindergarten: Related spheres of influence. Child Dev. 1999, 70, 1373–1400. [Google Scholar] [CrossRef] [PubMed]
- Lisonbee, J.A.; Mize, J.; Payne, A.L.; Granger, D.A. Children’s cortisol and the quality of teacher-child relationships in child care. Child Dev. 2008, 79, 1818–1832. [Google Scholar] [CrossRef] [PubMed]
- Palermo, F.; Hanish, L.D.; Martin, C.L.; Fabes, R.A.; Reiser, M. Preschoolers’ academic readiness: What role does the teacher-child relationship play? Early Child. Res. Q. 2007, 22, 407–422. [Google Scholar] [CrossRef] [PubMed]
- Pianta, R.C.; Stuhlman, M.W. Teacher-child relationships and children’s success in the first years of school. Sch. Psychol. Rev. 2004, 33, 444–458. [Google Scholar]
- Ladd, G.W.; Burgess, K.B. Do relational risks and protective factors moderate the linkages between childhood aggression and early psychological and school adjustment? Child Dev. 2001, 72, 1579–1601. [Google Scholar] [CrossRef] [PubMed]
- Conners-Burrow, N.A.; Whiteside-Mansell, L.; Mckelvey, L.; Virmani, E.A.; Sockwell, L. Improved classroom quality and child behavior in an Arkansas early childhood mental health consultation pilot project. Infant Ment. Health J. 2012, 33, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Fabiano, G.A.; Vujnovic, R.K.; Waschbusch, D.A.; Yu, J.; Mashtare, T.; Pariseau, M.E.; Pelham, W.E.; Parhama, B.R.; Smalls, K.J. Comparison of workshop training versus intensive, experiential training for improving behavior support skills in early educators. Early Child. Res. Q. 2013, 28, 450–460. [Google Scholar] [CrossRef]
- Landry, S.H.; Anthony, J.L.; Swank, P.R.; Pauline Monseque-Bailey, P. Effectiveness of comprehensive professional development for teachers of at-risk preschoolers. J. Educ. Psychol. 2009, 101, 448–465. [Google Scholar] [CrossRef]
- Raver, C.C.; Jones, S.M.; Li-Grining, C.; Zhai, F.; Metzger, M.W.; Solomon, B. Targeting children’s behavior problems in preschool classrooms: A cluster-randomized controlled trial. J. Consult. Clin. Psychol. 2009, 77, 302–316. [Google Scholar] [CrossRef] [PubMed]
- Lambert, R.G.; McCarthy, C.J.; O’Donnell, M.; Wang, C. Measuring elementary teacher stress and coping in the classroom: Validity evidence for the classroom appraisal of resources and demands. Psychol. Sch. 2009, 46, 973–988. [Google Scholar] [CrossRef]
- Li-Grining, C.P.; Votruba-Drzal, E.; Maldonado-Carreño, C.; Haas, K. Children’s early approaches to learning and academic trajectories through fifth grade. Dev. Psychol. 2010, 46, 1062. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M. “They Just Want to be with Us”: Young Children Learning to Live the Culture: A Post-Vygotskian Analysis of Young Children’s Enculturation into a Childcare Setting. Ph.D. Thesis, Victoria University of Wellington, Wellington, New Zealand, 2005. [Google Scholar]
- Perry, D.; Dunne, M.C.; McFadden, L.; Campbell, D. Reducing the risk for preschool expulsion: Mental health consultation for young children with challenging behaviors. J. Child Family Stud. 2008, 17, 44–54. [Google Scholar] [CrossRef]
- Upshur, C.; Wenz-Gross, M.; Reed, G. A pilot study of early childhood mental health consultation for children with behavioral problems in preschool. Early Child. Res. Q. 2009, 24, 29–45. [Google Scholar] [CrossRef]
- Gilliam, W.; Shahar, G. Preschool and child care expulsion and suspension: Rates and predictors in one state. Infants Young Child. 2006, 19, 228–245. [Google Scholar] [CrossRef]
- Alkon, A.; Ramler, M.; MacLennan, K. Evaluation of mental health consultation in child care centers. Early Child. Educ. J. 2003, 31, 91–99. [Google Scholar] [CrossRef]
- Brennan, E.M.; Bradley, J.R.; Allan, D.M.; Perry, D.F. The evidence base for mental health consultation in early childhood settings: Research synthesis addressing staff and program outcomes. J. Early Educ. Dev. 2008, 19, 982–1022. [Google Scholar] [CrossRef]
- Conners-Burrow, N.A.; Kramer, T.L.; Sigel, B.A.; Helpenstill, K.; Sievers, C.; McKelvey, L. Trauma-informed care training in a child welfare system: Moving it to the front line. Child. Youth Serv. Rev. 2013, 35, 1830–1835. [Google Scholar] [CrossRef]
- Green, B.; Simpson, J.; Everhart, M.; Vale, E.; Gettman, M. Understanding integrated mental health services in Head Start: Staff perspectives on mental health consultation. Natl. Head Start Assoc. Dialogue 2004, 7, 35–60. [Google Scholar] [CrossRef]
- Green, B.L.; Everhart, M.; Gordon, L.; Gettman, M.G. Characteristics of effective mental health consultation in early childhood settings: Multilevel analysis of a national survey. Top. Early Child. Spec. Educ. 2006, 26, 142–152. [Google Scholar] [CrossRef]
- Virmani, E.A.; Masyn, K.E.; Thompson, R.A.; Conners-Burrow, N.; Whiteside-Mansell, L. Early childhood mental health consultation: Promoting change in quality of teacher-child interactions. Infant Ment. Health J. 2013, 34, 156–172. [Google Scholar] [CrossRef]
- Virmani, E.; Ontai, L.L. Supervision and training in child care: Does reflective supervision foster caregiver insightfulness? Infant Ment. Health J. 2010, 31, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Fonagy, P.; Target, M.; Steele, H.; Steele, M. Reflective-Functioning Manual Version 5 for Application to Adult Attachment Interviews; University College London: London, UK, 1998. [Google Scholar]
- Gatti, S.N.; Watson, C.L.; Siegel, C.F. Step back and consider: Learning from reflective practice in infant mental health. Young Except. Child. 2011, 14, 32–45. [Google Scholar] [CrossRef]
- Koren-Karie, N.; Oppenheim, D.; Dolve, S.; Sher, E.; Etzion-Carasso, E. Mother’s insightfulness regarding their infant’s internal experience: Relations with maternal sensitivity and infant attachment. Dev. Psychol. 2002, 38, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Slade, A.; Grienenberger, J.; Bernbach, E.; Levy, D.; Locker, A. Maternal reflective functioning and attachment: Considering the transmission gap. Attach. Hum. Dev. 2005, 7, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Fox, L.; Dunlap, G.; Hemmeter, M.L.; Joseph, G.; Strain, P. The teaching pyramid: Model for supporting social competence and preventing challenging behavior in young children. Young Child. 2003, 58, 48–53. [Google Scholar]
- Ritblatt, S.N. Early Childhood Socio-Emotional and Behavior Regulation Intervention Specialist (EC-SEBRIS) training model: A crossroad of mental health and early childhood education. J. Ment. Health Train. Educ. Pract. 2016, 11, 1–13. [Google Scholar] [CrossRef]
- Huhra, R.L. Reviewing videotape in supervision: A developmental approach. J. Couns. Dev. 2008, 86, 412–418. [Google Scholar] [CrossRef]
- Romans, J.C.; Boswell, D.L.; Carlozzi, A.F.; Ferguson, D.B. Training and supervision practices in clinical, counseling, and school psychology programs. Prof. Psychol. Res. Pract. 1995, 26, 407–412. [Google Scholar] [CrossRef]
- Zan, B.; Donegan-Ritter, M. Reflecting, coaching and mentoring to enhance teacher–child interactions in Head Start classroom. Early Child. Educ. J. 2014, 42, 93–104. [Google Scholar] [CrossRef]
- California Infant, Preschool & Family Mental Health Initiative. The Delivery of Infant Family and Early Mental Health Services: Training Guidelines and Recommended Personnel Competencies; WestEd Center for Prevention and Early Intervention: Sacramento, CA, USA, 2010. [Google Scholar]
- Pianta, R.C.; Mashburn, A.J.; Downer, J.T.; Hamre, B.K.; Justice, L. Effects of web-mediated professional development resources on teacher-child interactions in pre-kindergarten classrooms. Early Child. Res. Q. 2008, 23, 431–451. [Google Scholar] [CrossRef] [PubMed]
- Blair, K.S.C.; Fox, L.; Lentini, R. Use of positive behavior support to address the challenging behavior of young children within a community early childhood program. Top. Early Child. Spec. Educ. 2010, 30, 68–79. [Google Scholar] [CrossRef]
- Joyce, B.R.; Showers, B. Student Achievement through Staff Development, 3rd ed.; Association for Supervision & Curriculum Development (ASCD): Alexandria, VA, USA, 2002. [Google Scholar]
- Tout, K.; Isner, T.; Zaslow, M. Coaching for Quality Improvement: Lessons Learned from Quality Rating and Improvement Systems. In Research brief for the Children’s Services Council of Palm Beach County; Child Trends: Washington, DC, USA, 2011. [Google Scholar]
- Arnett, J. Caregivers in day-care centers: Does training matter? J. Appl. Dev. Psychol. 1989, 10, 541–552. [Google Scholar] [CrossRef]
- Colwell, N.; Gordon, R.A.; Ken Fujimoto, K.; Robert Kaestner, R.; Korenmane, S. New evidence on the validity of the Arnett Caregiver Interaction Scale: Results from the Early Childhood Longitudinal Study-Birth Cohort. Early Child. Res. Q. 2013, 28, 218–233. [Google Scholar] [CrossRef] [PubMed]
- Campbell, P.H.; Milbourne, S.A. Improving the quality of infant—Toddler care through professional development. Top. Early Child. Spec. Educ. 2005, 25, 3–14. [Google Scholar] [CrossRef]
- Sutherland, K.S.; Conroy, M.A.; Abrams, L.; Vo, A. Improving interactions between teachers and young children with problem behavior: A strengths-based approach. Exceptionality 2010, 18, 70–81. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Item | Cohort 0 | Cohort 1 | Cohort 2 | Cohort 3 | Cohort 4 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Valid % | N | Valid % | N | Valid % | N | Valid % | N | Valid % | N | |
| Ethnicity | ||||||||||
| White | 44.44 | 12 | 48.6 | 17 | 32.0 | 8 | 57.6 | 19 | 41.7 | 10 |
| Hispanic | 40.74 | 11 | 22.9 | 8 | 48.0 | 12 | 30.3 | 10 | 37.5 | 9 |
| Black | 7.41 | 2 | 11.4 | 4 | - | - | - | - | 4.2 | 1 |
| Other | 7.41 | 2 | 17.2 | 6 | 20.0 | 5 | 12.1 | 4 | 16.7 | 4 |
| Undergraduate Major | ||||||||||
| Child and Family | 40.74 | 11 | 48.3 | 17 | 48.0 | 12 | 48.5 | 16 | 62.5 | 15 |
| Social Science (Other) | 14.81 | 4 | 31.4 | 11 | 36.0 | 9 | 33.3 | 11 | 25.0 | 6 |
| Language | 14.81 | 4 | 5.7 | 2 | - | - | 9.1 | 3 | - | - |
| Communication or Arts | 11.11 | 3 | - | - | - | - | 6.1 | 2 | 4.2 | 1 |
| Other | 18.52 | 5 | 14.3 | 5 | 16.0 | 4 | 3.0 | 1 | 8.3 | 2 |
| Mental Health Experience | ||||||||||
| Yes | 18.52 | 5 | 18.2 | 6 | 20.0 | 5 | 21.2 | 7 | 45.8 | 11 |
| No | 81.48 | 22 | 81.8 | 27 | 80.0 | 20 | 78.8 | 26 | 54.2 | 13 |
| Bilingual | ||||||||||
| Yes | 18.52 | 5 | 37.1 | 13 | 60.0 | 15 | 33.3 | 11 | 27.5 | 9 |
| No | 81.48 | 22 | 62.9 | 22 | 40.0 | 10 | 66.7 | 22 | 62.5 | 15 |
| Primary Language | ||||||||||
| English | 85.19 | 23 | 62.9 | 22 | 56.0 | 14 | 75.8 | 25 | 87.5 | 21 |
| Spanish | 14.81 | 4 | 20.0 | 7 | 32.0 | 8 | 24.2 | 8 | 8.3 | 2 |
| Other | - | - | 17.1 | 6 | 12.0 | 3 | - | - | 4.2 | 1 |
| Second Language | ||||||||||
| English | - | - | 100 | 13 | 66.7 | 10 | 72.7 | 8 | 33.3 | 3 |
| Spanish | 80.0 | 4 | - | - | 13.3 | 2 | 18.2 | 2 | 55.6 | 5 |
| Other | 20.0 | 1 | - | - | 20.0 | 3 | 9.1 | 1 | 11.1 | 1 |
| F (dfd = 113) | p | R2 | M Pre/Post | |
|---|---|---|---|---|
| Quality | ||||
| Time (dfn = 1) | 67.12 | <0.001 | 0.373 | |
| Cohort (dfn = 3) | 6.7.9 | <0.001 | 0.153 | 3.15/3.35 |
| Time × Cohort (dfn = 3) | 0.35 | 0.786 | 0.009 | |
| Sensitivity | ||||
| Time (dfn = 1) | 98.57 | <0.001 | 0.466 | |
| Cohort (dfn = 3) | 75.61 | <0.001 | 0.667 | 2.59/2.95 |
| Time × Cohort (dfn = 3) | 0.25 | 0.863 | 0.023 | |
| Harshness | ||||
| Time (dfn = 1) | 2.34 | 0.128 | 0.005 | |
| Cohort (dfn = 3) | 45.68 | <0.001 | 0.474 | 1.25/1.20 |
| Time × Cohort (dfn = 3) | 2.97 | 0.035 | 0.023 | |
| Detachment | ||||
| Time (dfn = 1) | 30.81 | <0.001 | 0.214 | |
| Cohort (dfn = 3) | 9.49 | <0.001 | 0.201 | 3.51/3.76 |
| Time × Cohort (dfn = 3) | 0.41 | 0.744 | 0.011 | |
| Permissiveness | ||||
| Time (dfn = 1) | 1.48 | 0.226 | 0.013 | |
| Cohort (dfn = 3) | 151.64 | <0.001 | 0.801 | 2.97/3.01 |
| Time × Cohort (dfn = 3) | 9.75 | <0.001 | 0.206 |
| F (dfd = 135) | p | R2 | M Pre/Post | |
|---|---|---|---|---|
| SE NRR | ||||
| Time (dfn = 1) | 413.11 | <0.001 | 0.754 | 3.55/4.67 |
| Cohort (dfn = 4) | 9.10 | <0.001 | 0.212 | |
| Time × Cohort (dfn = 4) | 5.13 | <0.001 | 0.132 | |
| SE HQE | ||||
| Time (dfn = 1) | 398.63 | <0.001 | 0.747 | 3.41/4.67 |
| Cohort (dfn = 4) | 6.84 | <0.001 | 0.169 | |
| Time × Cohort (dfn = 4) | 4.54 | 0.002 | 0.119 | |
| SE SES | ||||
| Time (dfn = 1) | 342.68 | <0.001 | 0.717 | 3.46/4.72 |
| Cohort (dfn = 4) | 6.02 | <0.001 | 0.151 | |
| Time × Cohort (dfn = 4) | 3.81 | 0.006 | 0.101 | |
| SE II | ||||
| Time | 465.97 | <0.001 | 0.775 | 2.75/4.53 |
| Cohort | 3.52 | 0.009 | 0.094 | |
| Time × Cohort | 1.58 | 0.18 | 0.045 | |
| SE Total | ||||
| Time (dfn = 1) | 493.71 | <0.001 | 0.785 | 3.38/4.66 |
| Cohort (dfn = 4) | 8.38 | <0.001 | 0.199 | |
| Time × Cohort (dfn = 4) | 4.44 | 0.002 | 0.116 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ritblatt, S.N.; Hokoda, A.; Van Liew, C. Investing in the Early Childhood Mental Health Workforce Development: Enhancing Professionals’ Competencies to Support Emotion and Behavior Regulation in Young Children. Brain Sci. 2017, 7, 120. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci7090120
Ritblatt SN, Hokoda A, Van Liew C. Investing in the Early Childhood Mental Health Workforce Development: Enhancing Professionals’ Competencies to Support Emotion and Behavior Regulation in Young Children. Brain Sciences. 2017; 7(9):120. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci7090120
Chicago/Turabian StyleRitblatt, Shulamit N., Audrey Hokoda, and Charles Van Liew. 2017. "Investing in the Early Childhood Mental Health Workforce Development: Enhancing Professionals’ Competencies to Support Emotion and Behavior Regulation in Young Children" Brain Sciences 7, no. 9: 120. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci7090120