The Role of the Embodiment Disturbance in the Anorexia Nervosa Psychopathology: A Network Analysis Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Clinical Assessment
2.3. Network Analysis and Statistical Procedures
3. Results
3.1. Sample Characteristics
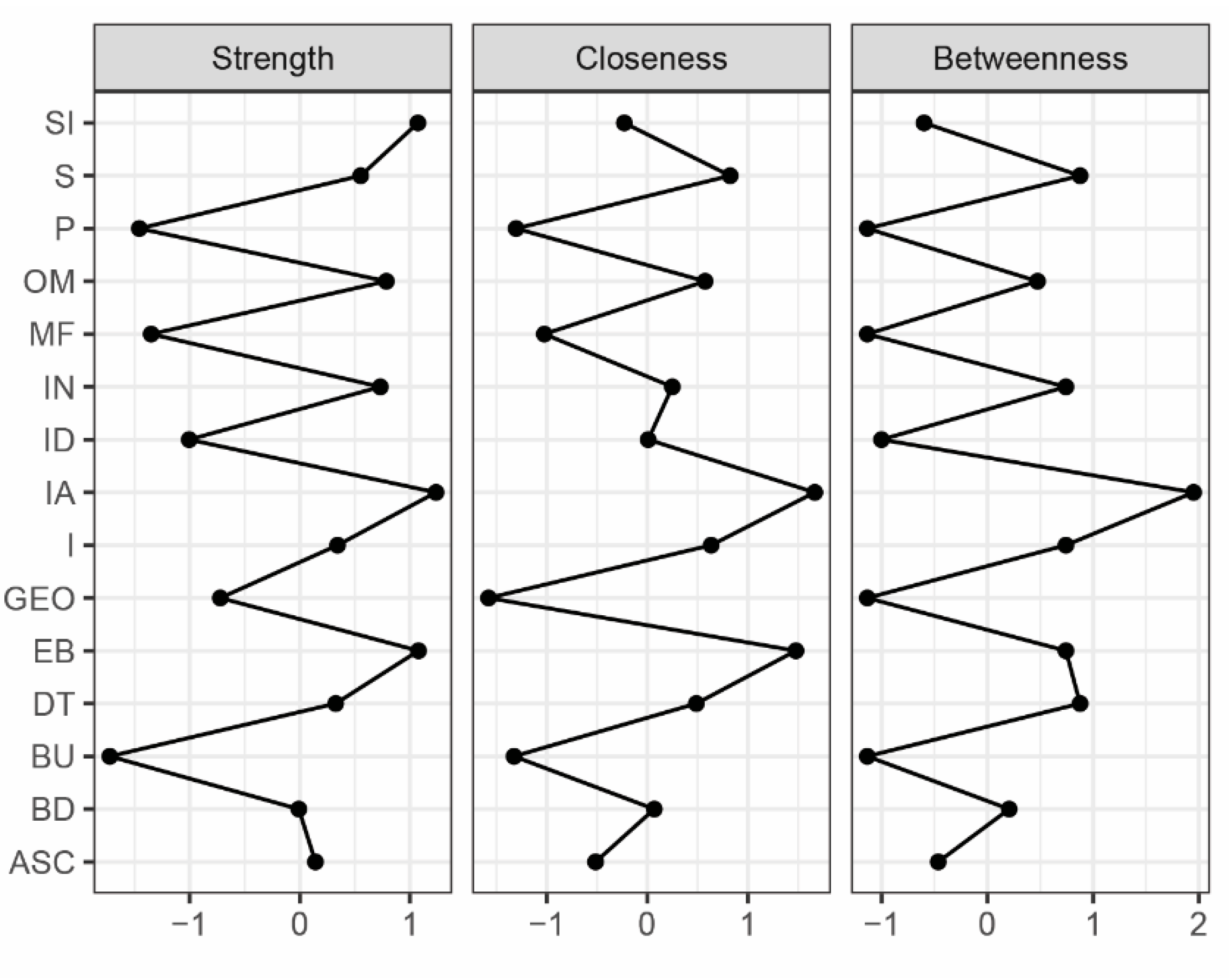
3.2. Network Analysis
4. Discussion
Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Garner, D.M.; Olmstead, M.P.; Polivy, J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int. J. Eat. Disord. 1983, 2, 15–34. [Google Scholar] [CrossRef]
- Gaudio, S.; Brooks, S.J.; Riva, G. Nonvisual Multisensory Impairment of Body Perception in Anorexia Nervosa: A Systematic Review of Neuropsychological Studies. PLoS ONE 2014, 9, e110087. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behav. Res. Ther. 2003, 41, 509–528. [Google Scholar] [CrossRef]
- Dalle Grave, R.; Calugi, S.; Marchesini, G. Compulsive exercise to control shape or weight in eating disorders: Prevalence, associated features, and treatment outcome. Compr. Psychiatry 2008, 49, 346–352. [Google Scholar] [CrossRef]
- Ricca, V.; Castellini, G.; Lo Sauro, C.; Mannucci, E.; Ravaldi, C.; Rotella, F.; Faravelli, C. Cognitive-Behavioral Therapy for Threshold and Subthreshold Anorexia Nervosa: A Three-Year Follow-Up Study. Psychother. Psychosom. 2010, 79, 238–248. [Google Scholar] [CrossRef]
- Stanghellini, G.; Castellini, G.; Brogna, P.; Faravelli, C.; Ricca, V. Identity and eating disorders (IDEA): A questionnaire evaluating identity and embodiment in eating disorder patients. Psychopathology 2012, 45, 147–158. [Google Scholar] [CrossRef]
- Stanghellini, G.; Trisolini, F.; Castellini, G.; Ambrosini, A.; Faravelli, C.; Ricca, V. Is Feeling Extraneous from One’s Own Body a Core Vulnerability Feature in Eating Disorders? Psychopathology 2015, 48, 18–24. [Google Scholar] [CrossRef]
- Monteleone, A.M.; Castellini, G.; Ricca, V.; Volpe, U.; De Riso, F.; Nigro, M.; Zamponi, F.; Mancini, M.; Stanghellini, G.; Monteleone, P.; et al. Embodiment Mediates the Relationship between Avoidant Attachment and Eating Disorder Psychopathology. Eur. Eat. Disord. Rev. 2017, 25, 461–468. [Google Scholar] [CrossRef]
- Eshkevari, E.; Rieger, E.; Longo, M.R.; Haggard, P.; Treasure, J. Increased plasticity of the bodily self in eating disorders. Psychol. Med. 2012, 42, 819–828. [Google Scholar] [CrossRef]
- Eshkevari, E.; Rieger, E.; Longo, M.R.; Haggard, P.; Treasure, J. Persistent body image disturbance following recovery from eating disorders. Int. J. Eat. Disord. 2014, 47, 400–409. [Google Scholar] [CrossRef]
- Tsakiris, M.; Jimenez, A.T.; Costantini, M. Just a heartbeat away from one’s body: Interoceptive sensitivity predicts malleability of body-representations. Proc. R. Soc. B Biol. Sci. 2011, 278, 2470–2476. [Google Scholar] [CrossRef] [PubMed]
- Herbert, B.M.; Pollatos, O. The Body in the Mind: On the Relationship Between Interoception and Embodiment. Top. Cogn. Sci. 2012, 4, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Bruch, H. Anorexia Nervosa: Therapy and theory. Am. J. Psychiatry 1982, 13, 1531–1538. [Google Scholar]
- Treasure, J.; Cardi, V. Anorexia Nervosa, Theory and Treatment: Where Are We 35 Years on from Hilde Bruch’s Foundation Lecture? Eur. Eat. Disord. Rev. 2017, 25, 139–147. [Google Scholar] [CrossRef]
- Fassino, S.; Pierò, A.; Gramaglia, C.; Abbate-Daga, G. Clinical, Psychopathological and Personality Correlates of Interoceptive Awareness in Anorexia nervosa, Bulimia nervosa and Obesity. Psychopathology 2004, 37, 168–174. [Google Scholar] [CrossRef]
- Volpe, U.; Monteleone, A.M.; Monteleone, P. Diagnostic Classification of Eating Disorders: The Role of Body Image. In Body Image, Eating, and Weight; Springer International Publishing: Cham, Switzerland, 2018; pp. 57–66. [Google Scholar]
- Borsboom, D. A network theory of mental disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Borsboom, D.; Cramer, A.O.J. Network analysis: An integrative approach to the structure of psychopathology. Ann. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef]
- Costantini, G.; Epskamp, S.; Borsboom, D.; Perugini, M.; Mõttus, R.; Waldorp, L.J.; Cramer, A.O.J. State of the aRt personality research: A tutorial on network analysis of personality data in R. J. Res. Pers. 2015, 54, 13–29. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Levinson, C.; Calebs, B. A network analysis of eating disorder symptoms and characteristics in an inpatient sample. Psychiatry Res. 2018, 262, 270–281. [Google Scholar] [CrossRef]
- Elliott, H.; Jones, P.J.; Schmidt, U. Central Symptoms Predict Post-Treatment Outcomes and Clinical Impairment in Anorexia Nervosa: A Network Analysis in a Randomized-Controlled Trial. PsyArXiv Preprints 2018. [Google Scholar] [CrossRef] [Green Version]
- Monteleone, A.M.; Cascino, G.; Solmi, M.; Pirozzi, R.; Tolone, S.; Terracciano, G.; Parisi, S.; Cimino, M.; Monteleone, P.; Maj, M.; et al. A network analysis of psychological, personality and eating characteristics of people seeking bariatric surgery: Identification of key variables and their prognostic value. J. Psychosom. Res. 2019, 120, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Castellini, G.; Trisolini, F.; Ricca, V. Psychopathology of eating disorders. J. Psychopathol. 2014, 20, 463–470. [Google Scholar]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. User’s Guide for the Structured Clinical Interview for DSM-5 Disorders, Research Version (SCID-5-RV); American Psychiatric Association: Arlington, VA, USA, 2015. [Google Scholar]
- Garner, D.M. Eating Disorder Inventory—2 Manual; Psychological Assessment Resources: Odessa, FL, USA, 1991. [Google Scholar]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. qgraph: Network Visualizations of Relationships in Psychometric Data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Epskamp, S.; Fried, E.I. A tutorial on regularized partial correlation networks. Psychol. Methods 2018, 23, 617–634. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Glasso: Graphical Lasso-Estimation of Gaussian Graphical Models; R Package Version 1; R Core Team: Vienna, Austria, 2014. [Google Scholar]
- Chen, J.; Chen, Z. Extended Bayesian information criteria for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef] [Green Version]
- Foygel, R.; Drton, M. Extended Bayesian information criteria for Gaussian graphical models. Adv. Neural Inf. Proc. Syst. 2010, 23, 2020–2028. [Google Scholar]
- Opsahl, T.; Agneessens, F.; Skvoretz, J. Node centrality in weighted networks: Generalizing degree and shortest paths. Soc. Netw. 2010, 32, 245–251. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef]
- Fried, E.I.; Cramer, A.O.J. Moving Forward: Challenges and Directions for Psychopathological Network Theory and Methodology. Perspect. Psychol. Sci. 2017, 12, 999–1020. [Google Scholar] [CrossRef]
- Forbes, M.K.; Wright, A.G.C.; Markon, K.E.; Krueger, R.F. The network approach to psychopathology: Promise versus reality. World Psychiatry 2019, 18, 272–273. [Google Scholar] [CrossRef]
- Oldershaw, A.; Startup, H.; Lavender, T. Anorexia Nervosa and a lost emotional self: A psychological formulation of the development, maintenance, and treatment of Anorexia Nervosa. Front. Psychol. 2019, 10, 219. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, A.M.; Mereu, A.; Cascino, G.; Criscuolo, M.; Castiglioni, M.C.; Pellegrino, F.; Patriciello, G.; Ruzzi, V.; Monteleone, P.; Vicari, S.; et al. Re-conceptualization of anorexia nervosa psychopathology: A network analysis study in adolescents with short duration of the illness. Int. J. Eat. Disord. 2019. [Google Scholar] [CrossRef] [PubMed]
- Markus, H.; Smith, J.; Moreland, R.L. Role of the self-concept in the perception of others. J. Pers. Soc. Psychol. 1985, 49, 1494–1512. [Google Scholar] [CrossRef]
- Nordbø, R.H.S.; Espeset, E.M.S.; Gulliksen, K.S.; Skårderud, F.; Holte, A. The meaning of self-starvation: Qualitative study of patients’ perception of anorexia nervosa. Int. J. Eat. Disord. 2006, 39, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Skårderud, F. Eating one’s words, Part II: The embodied mind and reflective function in anorexia nervosa—Theory. Eur. Eat. Disord. Rev. 2007, 15, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, P.M.; Taylor, L.; Laws, K.R. Self-reported interoceptive deficits in eating disorders: A meta-analysis of studies using the eating disorder inventory. J. Psychosom. Res. 2018, 110, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Keizer, A.; Smeets, M.A.M.; Dijkerman, H.C.; van den Hout, M.; Klugkist, I.; van Elburg, A.; Postma, A. Tactile body image disturbance in anorexia nervosa. Psychiatry Res. 2011, 190, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Zucker, N.; Moskovich, A.; Bulik, C.M.; Merwin, R.; Gaddis, K.; Losh, M.; Piven, J.; Wagner, H.R.; LaBar, K.S. Perception of affect in biological motion cues in anorexia nervosa. Int. J. Eat. Disord. 2013, 46, 12–22. [Google Scholar] [CrossRef]
- Keel, P.K.; Dorer, D.J.; Franko, D.L.; Jackson, S.C.; Herzog, D.B. Postremission Predictors of Relapse in Women with Eating Disorders. Am. J. Psychiatry 2005, 162, 2263–2268. [Google Scholar] [CrossRef]
- Calugi, S.; Dalle Grave, R. Body image concern and treatment outcomes in adolescents with anorexia nervosa. Int. J. Eat. Disord. 2019, 52, 582–585. [Google Scholar] [CrossRef]
- Caglar-Nazali, H.P.; Corfield, F.; Cardi, V.; Ambwani, S.; Leppanen, J.; Olabintan, O.; Deriziotis, S.; Hadjimichalis, A.; Scognamiglio, P.; Eshkevari, E.; et al. A systematic review and meta-analysis of ‘Systems for Social Processes’ in eating disorders. Neurosci. Biobehav. Rev. 2014, 42, 55–92. [Google Scholar] [CrossRef] [PubMed]
- Treasure, J.; Schmidt, U. The cognitive-interpersonal maintenance model of anorexia nervosa revisited: A summary of the evidence for cognitive, socio-emotional and interpersonal predisposing and perpetuating factors. J. Eat. Disord. 2013, 1, 13. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, A.M.; Treasure, J.; Kan, C.; Cardi, V. Reactivity to interpersonal stress in patients with eating disorders: A systematic review and meta-analysis of studies using an experimental paradigm. Neurosci Biobehav. Rev. 2018, 87, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Biegel, G.M.; Brown, K.W.; Shapiro, S.L.; Schubert, C.M. Mindfulness-based stress reduction for the treatment of adolescent psychiatric outpatients: A randomized clinical trial. J. Consult. Clin. Psychol. 2009, 77, 855–866. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Whole Sample (n = 84) | Restricting Subtype (n = 57) | Binge-Purging Subtype (n = 27) | |
|---|---|---|---|
| Age (years) | 27.04 ± 8.80 | 26.33 ± 8.19 | 28.76 ± 10.09 |
| BMI (kg/m2) | 16.96 ± 1.87 | 16.77 ± 1.87 | 17.24 ± 1.78 |
| Age at Onset | 17.58 ± 4.93 | 17.48 ± 4.92 | 17.64 ± 4.95 |
| Illness Duration | 8.94 ± 8.85 | 8.22 ± 7.94 | 8.73 ± 8.75 |
| IDEA Total | 2.08 ± 1.07 | 1.98 ± 1.10 | 2.34 ± 0.97 |
| IDEA GEO | 1.83 ± 1.04 | 1.84 ± 1.07 | 1.85 ± 0.99 |
| IDEA OM | 2.38 ± 1.28 | 2.22 ± 1.36 | 2.73 ± 1.05 |
| IDEA EB | 1.91 ± 1.27 | 1.73 ± 1.29 | 2.38 ± 1.07 |
| IDEA S | 2.36 ± 1.25 | 2.23 ± 1.33 | 2.66 ± 1.03 |
| EDI IN | 12.40 ± 8.61 | 11.35 ± 8.65 | 15.00 ± 8.18 |
| EDI MF | 10.19 ± 6.67 | 10.11 ± 6.37 | 10.54 ± 7.47 |
| EDI SI | 8.74 ± 4.49 | 8.60 ± 4.52 | 9.38 ± 4.21 |
| EDI BD | 13.36 ± 7.93 | 12.61 ± 8.1 | 15.27 ± 7.39 |
| EDI P | 7.13 ± 4.82 | 6.93 ± 5.04 | 7.65 ± 4.45 |
| EDI ID | 7.94 ± 4.95 | 8.00 ± 5.11 | 8.04 ± 4.62 |
| EDI IR | 8.05 ± 7.36 | 7.25 ± 6.83 | 9.96 ± 8.35 |
| EDI DT | 12.51 ± 7.69 | 11.61 ± 8.08 | 14.81 ± 6.30 |
| EDI BU | 3.15 ± 4.96 | 1.30 ± 2.38 | 7.35 ± 6.51 * |
| EDI IA | 12.60 ± 8.37 | 11.25 ± 8.09 | 16.00 ± 8.01 |
| EDI ASC | 7.54 ± 5.67 | 6.75 ± 4.92 | 9.38 ± 6.86 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cascino, G.; Castellini, G.; Stanghellini, G.; Ricca, V.; Cassioli, E.; Ruzzi, V.; Monteleone, P.; Monteleone, A.M. The Role of the Embodiment Disturbance in the Anorexia Nervosa Psychopathology: A Network Analysis Study. Brain Sci. 2019, 9, 276. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9100276
Cascino G, Castellini G, Stanghellini G, Ricca V, Cassioli E, Ruzzi V, Monteleone P, Monteleone AM. The Role of the Embodiment Disturbance in the Anorexia Nervosa Psychopathology: A Network Analysis Study. Brain Sciences. 2019; 9(10):276. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9100276
Chicago/Turabian StyleCascino, Giammarco, Giovanni Castellini, Giovanni Stanghellini, Valdo Ricca, Emanuele Cassioli, Valeria Ruzzi, Palmiero Monteleone, and Alessio Maria Monteleone. 2019. "The Role of the Embodiment Disturbance in the Anorexia Nervosa Psychopathology: A Network Analysis Study" Brain Sciences 9, no. 10: 276. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9100276