Autoimmune Encephalitis and CSF Anti-GluR3 Antibodies in an MS Patient after Alemtuzumab Treatment

 , ,
, , {kind=link}
Abstract
:1. Introduction
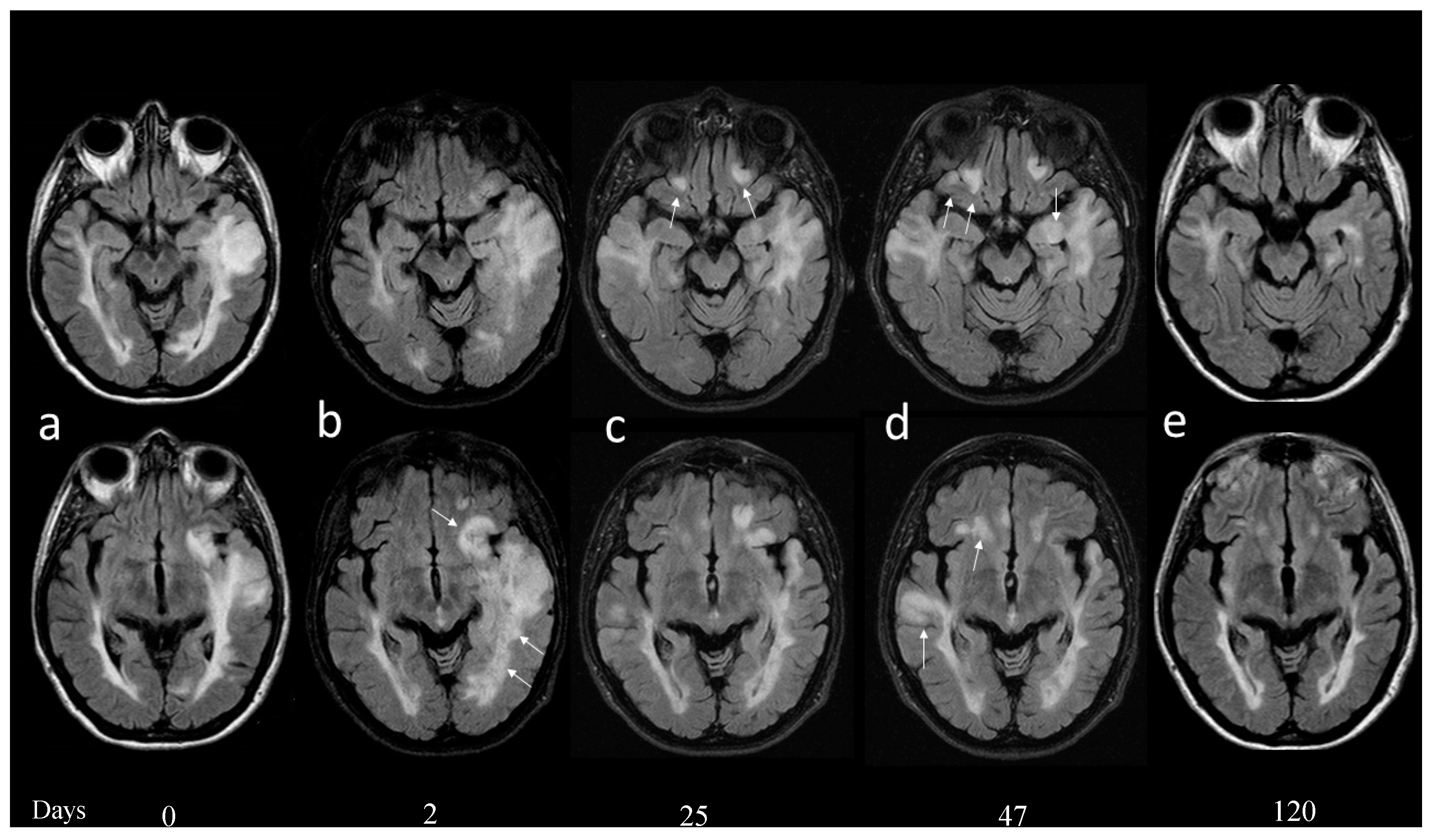
2. Case Report
3. Discussion
Author Contributions
Funding
Conflicts of Interest
Consent
References
- Coles, A.J.; Cohen, J.A.; Fox, E.J.; Giovannoni, G.; Hartung, H.P.; Havrdova, E.; Schippling, S.; Selmaj, K.W.; Traboulsee, A.; Compston, D.A.S.; et al. Alemtuzumab CARE-MS II 5-year follow-up: Efficacy and safety findings. Neurology 2017, 89, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- Nosadini, M.; Mohammad, S.S.; Ramanathan, S.; Brilot, F.; Dale, R.C. Immune therapy in autoimmune encephalitis: A systematic review. Expert Rev. Neurother. 2015, 15, 1391–1419. [Google Scholar] [CrossRef] [PubMed]
- Mantegazza, R.; Bernasconi, P.; Baggi, F.; Spreafico, R.; Ragona, F.; Antozzi, C.; Bernardi, G.; Granata, T.; Italian Rasmussen’s Encephalitis Study Group. Antibodies against GluR3 peptides are nots pecific for Rasmussen’s encephalitis but are also present in epilepsy patients with severe, early onset disease and intractable seizures. J. Neuroimmunol. 2002, 131, 179–185. [Google Scholar] [CrossRef]
- Borroni, B.; Stanic, J.; Verpelli, C.; Mellone, M.; Bonomi, E.; Alberici, A.; Bernasconi, P.; Culotta, L.; Zianni, E.; Archetti, S.; et al. Anti-AMPA GluA3 antibodies in frontotemporal dementia: A new molecular target. Sci. Rep. 2017, 7, 6723. [Google Scholar] [CrossRef] [PubMed]
- Giarola, B.; Massey, J.; Barnett, Y.; Rodrigues, M.; Sutton, I. Autoimmune encephalitis following alemtuzumab treatment of multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 28, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Levite, M. Glutamate receptor antibodies in neurological diseases: Anti-AMPA-GluR3 antibodies, Anti-NMDA-NR1 antibodies, Anti-NMDA-NR2A/B antibodies, Anti-mGluR1 antibodies or Anti-mGluR5 antibodies are present in subpopulations of patients with either: Epilepsy, Encephalitis, Cerebellar Ataxia, Systemic Lupus Erythematosus (SLE) and Neuropsychiatric SLE, Sjogren’ssyndrome, Schizophrenia, Mania or Stroke. These autoimmune anti-glutamate receptor antibodies can bind neurons in few brain regions, activate glutamate receptors, decrease glutamate receptor’s expression, impair glutamate-induced signaling and function, activate Blood Brain Barrier endothelial cells, kill neurons, damage the brain, induce behavioral/psychiatric/cognitive abnormalities and Ataxia in animal models, and can be removed or silenced in some patients by immunotherapy. J. Neural. Transm. 2014, 121, 1029–1075. [Google Scholar] [PubMed]
- Frassoni, C.; Spreafico, R.; Franceschetti, S.; Aurisano, N.; Bernasconi, P.; Garbelli, R.; Antozzi, C.; Taverna, S.; Granata, T.; Mantegazza, R. Labeling of rat neurons by anti-GluR3 IgG from patients with Rasmussen encephalitis. Neurology 2001, 57, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Solaro, C.; Mantegazza, R.; Bacigalupo, A.; Uccelli, A. Intractable myoclonus associated with anti-GluR3 antibodies after allogeneic bone marrow transplantation. Haematologica 2006, 91, ECR62. [Google Scholar] [PubMed]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buscarinu, M.C.; Fornasiero, A.; Pellicciari, G.; Reniè, R.; Landi, A.C.; Bozzao, A.; Cappelletti, C.; Bernasconi, P.; Ristori, G.; Salvetti, M. Autoimmune Encephalitis and CSF Anti-GluR3 Antibodies in an MS Patient after Alemtuzumab Treatment. Brain Sci. 2019, 9, 299. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9110299
Buscarinu MC, Fornasiero A, Pellicciari G, Reniè R, Landi AC, Bozzao A, Cappelletti C, Bernasconi P, Ristori G, Salvetti M. Autoimmune Encephalitis and CSF Anti-GluR3 Antibodies in an MS Patient after Alemtuzumab Treatment. Brain Sciences. 2019; 9(11):299. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9110299
Chicago/Turabian StyleBuscarinu, Maria Chiara, Arianna Fornasiero, Giulia Pellicciari, Roberta Reniè, Anna Chiara Landi, Alessandro Bozzao, Cristina Cappelletti, Pia Bernasconi, Giovanni Ristori, and Marco Salvetti. 2019. "Autoimmune Encephalitis and CSF Anti-GluR3 Antibodies in an MS Patient after Alemtuzumab Treatment" Brain Sciences 9, no. 11: 299. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9110299