Descriptive Psychopathology of the Acute Effects of Intravenous Delta-9-Tetrahydrocannabinol Administration in Humans

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Procedure
2.2. Subjects
2.3. Psychopathological Assessment
2.4. Ethics Approval
3. Results
3.1. Demographic Information
3.2. Prevalence and Severity of Symptoms: Results at a Glance
3.2.1. Following Acute ∆9-THC Administration
3.2.2. Following Placebo Administration
3.3. Symptoms Description
3.3.1. Psychosis-Related Positive Symptoms and Disorganization
3.3.2. Psychosis-Related Negative Symptoms
3.3.3. Psychosis-Related General Psychopathology
3.4. Subjects’ Quotes
3.5. Additional Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tsuang, M.T.; Bar, J.L.; Stone, W.S.; Faraone, S.V. Gene-environment interactions in mental disorders. World Psychiatry 2004, 3, 73–83. [Google Scholar] [PubMed]
- Rapoport, J.L.; Giedd, J.N.; Gogtay, N. Neurodevelopmental model of schizophrenia: Update 2012. Mol. Psychiatry 2012, 17, 1228–1238. [Google Scholar] [CrossRef]
- Gouzoulis-Mayfrank, E.; Hermle, L.; Thelen, B.; Sass, H. History, rationale and potential of human experimental hallucinogenic drug research in psychiatry. Pharmacopsychiatry 1998, 31, 63–68. [Google Scholar] [CrossRef]
- Strakowski, S.M.; Sax, K.W.; Setters, M.J.; Keck, P.E., Jr. Enhanced response to repeated d-amphetamine challenge: Evidence for behavioral sensitization in humans. Biol. Psychiatry 1996, 40, 872–880. [Google Scholar] [CrossRef]
- Vollenweider, F.X.; Vollenweider-Scherpenhuyzen, M.F.; Babler, A.; Vogel, H.; Hell, D. Psilocybin induces schizophrenia-like psychosis in humans via a serotonin-2 agonist action. Neuroreport 1998, 9, 3897–3902. [Google Scholar] [CrossRef]
- Krystal, J.H.; Karper, L.P.; Seibyl, J.P.; Freeman, G.K.; Delaney, R.; Bremner, J.D.; Heninger, G.R.; Bowers, M.B., Jr.; Charney, D.S. Subanesthetic effects of the noncompetitive NMDA antagonist, ketamine, in humans. Psychotomimetic, perceptual, cognitive, and neuroendocrine responses. Arch. Gen. Psychiatry 1994, 51, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Sewell, R.A.; Skosnik, P.D.; Garcia-Sosa, I.; Ranganathan, M.; D’Souza, D.C. Behavioral, cognitive and psychophysiological effects of cannabinoids: Relevance to psychosis and schizophrenia. Rev. Bras. Psiquiatr. 2010, 32, 15–30. [Google Scholar]
- Bhattacharyya, S.; Crippa, J.A.; Martin-Santos, R.; Winton-Brown, T.; Fusar-Poli, P. Imaging the neural effects of cannabinoids: Current status and future opportunities for psychopharmacology. Curr. Pharm. Des. 2009, 15, 2603–2614. [Google Scholar] [CrossRef] [PubMed]
- Nestler, E.J.; Hyman, S.E. Animal models of neuropsychiatric disorders. Nat. Neurosci. 2010, 13, 1161–1169. [Google Scholar] [CrossRef]
- Bhattacharyya, S.; Fusar-Poli, P.; Borgwardt, S.; Martin-Santos, R.; Nosarti, C.; O’Carroll, C.; Allen, P.; Seal, M.L.; Fletcher, P.C.; Crippa, J.A.; et al. Modulation of Mediotemporal and Ventrostriatal Function in Humans by Delta 9-Tetrahydrocannabinol A Neural Basis for the Effects of Cannabis sativa on Learning and Psychosis. Arch. Gen. Psychiatry 2009, 66, 442–451. [Google Scholar] [CrossRef]
- Bhattacharyya, S.; Crippa, J.A.; Allen, P.; Martin-Santos, R.; Borgwardt, S.; Fusar-Poli, P.; Rubia, K.; Kambeitz, J.; O’Carroll, C.; Seal, M.L.; et al. Induction of psychosis by Delta9-tetrahydrocannabinol reflects modulation of prefrontal and striatal function during attentional salience processing. Arch. Gen. Psychiatry 2012, 69, 27–36. [Google Scholar] [CrossRef]
- D’Souza, D.C.; Perry, E.; MacDougall, L.; Ammerman, Y.; Cooper, T.; Wu, Y.T.; Braley, G.; Gueorguieva, R.; Krystal, J.H. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: Implications for psychosis. Neuropsychopharmacology 2004, 29, 1558–1572. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Atakan, Z.; Martin-Santos, R.; Crippa, J.A.; Kambeitz, J.; Prata, D.; Williams, S.; Brammer, M.; Collier, D.A.; McGuire, P.K. Preliminary report of biological basis of sensitivity to the effects of cannabis on psychosis: AKT1 and DAT1 genotype modulates the effects of delta-9-tetrahydrocannabinol on midbrain and striatal function. Mol. Psychiatry 2012, 17, 1152–1155. [Google Scholar] [CrossRef]
- Moore, T.H.; Zammit, S.; Lingford-Hughes, A.; Barnes, T.R.; Jones, P.B.; Burke, M.; Lewis, G. Cannabis use and risk of psychotic or affective mental health outcomes: A systematic review. Lancet 2007, 370, 319–328. [Google Scholar] [CrossRef]
- Morrison, P.D.; Bhattacharyya, S.; Murray, R. Recreational cannabis: The risk of schizophrenia. In Handbook of Cannabis; Pertwee, R.G., Ed.; Oxford University Press: Oxford, UK, 2015; pp. 661–673. [Google Scholar]
- Colizzi, M.; Murray, R. Cannabis and psychosis: What do we know and what should we do? Br. J. Psychiatry 2018, 212, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Colizzi, M.; Iyegbe, C.; Powell, J.; Ursini, G.; Porcelli, A.; Bonvino, A.; Taurisano, P.; Romano, R.; Masellis, R.; Blasi, G.; et al. Interaction Between Functional Genetic Variation of DRD2 and Cannabis Use on Risk of Psychosis. Schizophr. Bull. 2015, 41, 1171–1182. [Google Scholar] [CrossRef] [Green Version]
- Colizzi, M.; Iyegbe, C.; Powell, J.; Blasi, G.; Bertolino, A.; Murray, R.M.; Di Forti, M. Interaction between DRD2 and AKT1 genetic variations on risk of psychosis in cannabis users: A case–control study. Npj Schizophr. 2015, 1, 15025. [Google Scholar] [CrossRef]
- Colizzi, M.; Carra, E.; Fraietta, S.; Lally, J.; Quattrone, D.; Bonaccorso, S.; Mondelli, V.; Ajnakina, O.; Dazzan, P.; Trotta, A.; et al. Substance use, medication adherence and outcome one year following a first episode of psychosis. Schizophr. Res. 2016, 170, 311–317. [Google Scholar] [CrossRef] [Green Version]
- Patel, R.; Wilson, R.; Jackson, R.; Ball, M.; Shetty, H.; Broadbent, M.; Stewart, R.; McGuire, P.; Bhattacharyya, S. Association of cannabis use with hospital admission and antipsychotic treatment failure in first episode psychosis: An observational study. BMJ Open 2016, 6, e009888. [Google Scholar] [CrossRef] [PubMed]
- Schoeler, T.; Petros, N.; Di Forti, M.; Klamerus, E.; Foglia, E.; Ajnakina, O.; Gayer-Anderson, C.; Colizzi, M.; Quattrone, D.; Behlke, I.; et al. Effects of continuation, frequency, and type of cannabis use on relapse in the first 2 years after onset of psychosis: An observational study. Lancet Psychiatry 2016, 3, 947–953. [Google Scholar] [CrossRef]
- Schoeler, T.; Petros, N.; Di Forti, M.; Pingault, J.B.; Klamerus, E.; Foglia, E.; Small, A.; Murray, R.; Bhattacharyya, S. Association Between Continued Cannabis Use and Risk of Relapse in First-Episode Psychosis: A Quasi-Experimental Investigation Within an Observational Study. JAMA Psychiatry 2016, 73, 1173–1179. [Google Scholar] [CrossRef]
- Schoeler, T.; Monk, A.; Sami, M.B.; Klamerus, E.; Foglia, E.; Brown, R.; Camuri, G.; Altamura, A.C.; Murray, R.; Bhattacharyya, S. Continued versus discontinued cannabis use in patients with psychosis: A systematic review and meta-analysis. Lancet Psychiatry 2016, 3, 215–225. [Google Scholar] [CrossRef]
- Appiah-Kusi, E.; Leyden, E.; Parmar, S.; Mondelli, V.; McGuire, P.; Bhattacharyya, S. Abnormalities in neuroendocrine stress response in psychosis: The role of endocannabinoids. Psychol. Med. 2016, 46, 27–45. [Google Scholar] [CrossRef]
- Leweke, F.M.; Giuffrida, A.; Koethe, D.; Schreiber, D.; Nolden, B.M.; Kranaster, L.; Neatby, M.A.; Schneider, M.; Gerth, C.W.; Hellmich, M.; et al. Anandamide levels in cerebrospinal fluid of first-episode schizophrenic patients: Impact of cannabis use. Schizophr. Res. 2007, 94, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Taurisano, P.; Antonucci, L.A.; Fazio, L.; Rampino, A.; Romano, R.; Porcelli, A.; Masellis, R.; Colizzi, M.; Quarto, T.; Torretta, S.; et al. Prefrontal activity during working memory is modulated by the interaction of variation in CB1 and COX2 coding genes and correlates with frequency of cannabis use. Cortex 2016, 81, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Colizzi, M.; Bhattacharyya, S. Does Cannabis Composition Matter? Differential Effects of Delta-9-tetrahydrocannabinol and Cannabidiol on Human Cognition. Curr. Addict. Rep. 2017, 4, 62–74. [Google Scholar] [CrossRef] [Green Version]
- Colizzi, M.; Fazio, L.; Ferranti, L.; Porcelli, A.; Masellis, R.; Marvulli, D.; Bonvino, A.; Ursini, G.; Blasi, G.; Bertolino, A. Functional genetic variation of the cannabinoid receptor 1 and cannabis use interact on prefrontal connectivity and related working memory behavior. Neuropsychopharmacology 2015, 40, 640–649. [Google Scholar] [CrossRef]
- Chopra, G.S.; Smith, J.W. Psychotic Reactions Following Cannabis Use in East Indians. Arch. Gen. Psychiatry 1974, 30, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Talbott, J.A.; Teague, J.W. Marihuana Psychosis—Acute Toxic Psychosis Associated with Use of Cannabis Derivatives. J. Amer. Med. Assoc. 1969, 210, 299–302. [Google Scholar] [CrossRef]
- Keeler, M.H.; Moore, E. Paranoid reactions while using marijuana. Dis. Nerv. Syst. 1974, 35, 535–536. [Google Scholar]
- Morrison, P.D.; Zois, V.; McKeown, D.A.; Lee, T.D.; Holt, D.W.; Powell, J.F.; Kapur, S.; Murray, R.M. The acute effects of synthetic intravenous Delta(9)-tetrahydrocannabinol on psychosis, mood and cognitive functioning. Psychol. Med. 2009, 39, 1607–1616. [Google Scholar] [CrossRef]
- Barkus, E.; Morrison, P.D.; Vuletic, D.; Dickson, J.C.; Ell, P.J.; Pilowsky, L.S.; Brenneisen, R.; Holt, D.W.; Powell, J.; Kapur, S.; et al. Does intravenous Δ9-tetrahydrocannabinol increase dopamine release? A SPET study. J. Psychopharmacol. 2011, 25, 1462–1468. [Google Scholar] [CrossRef]
- Morrison, P.D.; Stone, J.M. Synthetic delta-9-tetrahydrocannabinol elicits schizophrenia-like negative symptoms which are distinct from sedation. Hum. Psychopharmacol. 2011, 26, 77–80. [Google Scholar] [CrossRef]
- Englund, A.; Morrison, P.D.; Nottage, J.; Hague, D.; Kane, F.; Bonaccorso, S.; Stone, J.M.; Reichenberg, A.; Brenneisen, R.; Holt, D.; et al. Cannabidiol inhibits THC-elicited paranoid symptoms and hippocampal-dependent memory impairment. J. Psychopharmacol. 2013, 27, 19–27. [Google Scholar] [CrossRef]
- Martin-Santos, R.; Crippa, J.A.; Batalla, A.; Bhattacharyya, S.; Atakan, Z.; Borgwardt, S.; Allen, P.; Seal, M.; Langohr, K.; Farre, M.; et al. Acute Effects of a Single, Oral dose of d9-tetrahydrocannabinol (THC) and Cannabidiol (CBD) Administration in Healthy Volunteers. Curr. Pharm. Des. 2012, 18, 4966–4979. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, R.M.; Kraft, B.; Frey, R.; Winkler, D.; Weiszenbichler, S.; Backer, C.; Kasper, S.; Kress, H.G. Acute psychotropic effects of oral cannabis extract with a defined content of Delta9-tetrahydrocannabinol (THC) in healthy volunteers. Pharmacopsychiatry 2010, 43, 24–32. [Google Scholar] [CrossRef]
- D’Souza, D.C.; Ranganathan, M.; Braley, G.; Gueorguieva, R.; Zimolo, Z.; Cooper, T.; Perry, E.; Krystal, J. Blunted psychotomimetic and amnestic effects of delta-9-tetrahydrocannabinol in frequent users of cannabis. Neuropsychopharmacology 2008, 33, 2505–2516. [Google Scholar] [CrossRef] [PubMed]
- Colizzi, M.; Bhattacharyya, S. Cannabis use and the development of tolerance: A systematic review of human evidence. Neurosci. Biobehav. Rev. 2018, 93, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Colizzi, M.; Weltens, N.; McGuire, P.; Lythgoe, D.; Williams, S.; Van Oudenhove, L.; Bhattacharyya, S. Delta-9-tetrahydrocannabinol increases striatal glutamate levels in healthy individuals: Implications for psychosis. Mol. Psychiatry 2019. [Google Scholar] [CrossRef] [PubMed]
- Naef, M.; Russmann, S.; Petersen-Felix, S.; Brenneisen, R. Development and pharmacokinetic characterization of pulmonal and intravenous delta-9-tetrahydrocannabinol (THC) in humans. J. Pharm. Sci. 2004, 93, 1176–1184. [Google Scholar] [CrossRef]
- Radhakrishnan, R.; Wilkinson, S.T.; D’Souza, D.C. Gone to pot—A review of the association between cannabis and psychosis. Front. Psychiatry 2014, 5. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5 Disorders, Clinician Version (SCID-5-CV); American Psychiatric Association: Arlington, VA, USA, 2015. [Google Scholar]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Spencer, L.; Ritchie, J.; Lewis, J.; Dillon, L. Quality in Qualitative Evaluation: A Framework for Assessing Research Evidence; Cabinet Office: London, UK, 2003. [Google Scholar]
- Hauser, W.; Sarzi-Puttini, P.; Tolle, T.R.; Wolfe, F. Placebo and nocebo responses in randomised controlled trials of drugs applying for approval for fibromyalgia syndrome treatment: Systematic review and meta-analysis. Clin. Exp. Rheumatol. 2012, 30, S78–S87. [Google Scholar]
- Planes, S.; Villier, C.; Mallaret, M. The nocebo effect of drugs. Pharmacol. Res. Perspect. 2016, 4, e00208. [Google Scholar] [CrossRef]
- Hart, C.L.; van Gorp, W.; Haney, M.; Foltin, R.W.; Fischman, M.W. Effects of acute smoked marijuana on complex cognitive performance. Neuropsychopharmacology 2001, 25, 757–765. [Google Scholar] [CrossRef]
- Curran, H.V.; Brignell, C.; Fletcher, S.; Middleton, P.; Henry, J. Cognitive and subjective dose-response effects of acute oral Delta(9)-tetrahydrocannabinol (THC) in infrequent cannabis users. Psychopharmacology 2002, 164, 61–70. [Google Scholar] [CrossRef]
- Colizzi, M.; McGuire, P.; Giampietro, V.; Williams, S.; Brammer, M.; Bhattacharyya, S. Previous cannabis exposure modulates the acute effects of delta-9-tetrahydrocannabinol on attentional salience and fear processing. Exp. Clin. Psychopharm. 2018, 26, 582–598. [Google Scholar] [CrossRef]
- Colizzi, M.; McGuire, P.; Giampietro, V.; Williams, S.; Brammer, M.; Bhattacharyya, S. Modulation of acute effects of delta-9-tetrahydrocannabinol on psychotomimetic effects, cognition and brain function by previous cannabis exposure. Eur. Neuropsychopharm. 2018, 28, 850–862. [Google Scholar] [CrossRef]
- Kelly, P.; Jones, R.T. Metabolism of Tetrahydrocannabinol in Frequent and Infrequent Marijuana Users. J. Anal. Toxicol. 1992, 16, 228–235. [Google Scholar] [CrossRef]
- Law, B.; Mason, P.A.; Moffat, A.C.; Gleadle, R.I.; King, L.J. Forensic aspects of the metabolism and excretion of cannabinoids following oral ingestion of cannabis resin. J. Pharm. Pharmacol. 1984, 36, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Huestis, M.A.; Gustafson, R.A.; Moolchan, E.T.; Barnes, A.; Bourland, J.A.; Sweeney, S.A.; Hayes, E.F.; Carpenter, P.M.; Smith, M.L. Cannabinoid concentrations in hair from documented cannabis users. Forensic Sci. Int. 2007, 169, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Colizzi, M.; Bhattacharyya, S. Neurocognitive effects of cannabis: Lessons learned from human experimental studies. Prog. Brain. Res. 2018, 242, 179–216. [Google Scholar] [CrossRef] [PubMed]
- Semple, D.M.; McIntosh, A.M.; Lawrie, S.M. Cannabis as a risk factor for psychosis: Systematic review. J. Psychopharmacol. 2005, 19, 187–194. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Participant | Drug | Delusions | Conceptual Disorganization | Hallucinatory Behavior | Excitement | Grandiosity | Suspiciousness/Persecution | Hostility |
|---|---|---|---|---|---|---|---|---|
| male 1 | Δ9-THC | ✕ | ✓ mild | ✕ | ✓ minimal | ✕ | ✓ mild | ✕ |
| male 2 | Δ9-THC | ✕ | ✓ mild | ✕ | ✓ mild | ✓ minimal | ✕ | ✕ |
| male 3 | Δ9-THC | ✕ | ✓ severe | ✓ mild | ✓ moderate | ✓ moderate | ✓ mild | ✕ |
| male 4 | Δ9-THC | ✕ | ✓ minimal | ✕ | ✓ minimal | ✕ | ✕ | ✕ |
| male 5 | Δ9-THC | ✕ | ✓ moderate | ✓ mild | ✕ | ✕ | ✓ minimal | ✕ |
| male 6 | Δ9-THC | ✓ mild | ✓ moderate | ✓ mild | ✓ moderate | ✓ moderate | ✕ | ✕ |
| male 7 | Δ9-THC | ✕ | ✓ moderate | ✓ mild | ✓ mild | ✕ | ✓ minimal | ✕ |
| female 1 | Δ9-THC | ✕ | ✓ mild | ✕ | ✕ | ✕ | ✕ | ✓ mild |
| female 2 | Δ9-THC | ✕ | ✓ mild | ✓ mild | ✕ | ✕ | ✕ | ✕ |
| female 3 | Δ9-THC | ✕ | ✓ mild | ✕ | ✓ mild | ✕ | ✕ | ✕ |
| female 4 | Δ9-THC | ✕ | ✓ moderate | ✓ minimal | ✓ mild | ✕ | ✓ mild | ✓ mild |
| female 5 | Δ9-THC | ✕ | ✓ mild | ✓ mild | ✓ mild | ✕ | ✓ mild | ✕ |
| female 6 | Δ9-THC | ✕ | ✓ moderate | ✓ mild | ✓ minimal | ✕ | ✕ | ✕ |
| female 7 | Δ9-THC | ✕ | ✓ moderate | ✕ | ✕ | ✕ | ✓ minimal | ✕ |
| female 8 | Δ9-THC | ✓ moderate | ✓ moderate/severe | ✓ severe | ✕ | ✓ moderate | ✓ minimal | ✕ |
| female 9 | Δ9-THC | ✓ minimal | ✓ moderate | ✓ moderate | ✕ | ✕ | ✓ moderate | ✓ mild |
| male 1 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 2 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 3 | placebo | ✕ | ✕ | ✕ | ✓ minimal | ✕ | ✕ | ✕ |
| male 4 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 5 | placebo | ✕ | ✓ mild | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 6 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 7 | placebo | ✕ | ✓ mild | ✓ minimal | ✕ | ✕ | ✕ | ✕ |
| female 1 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 2 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 3 | placebo | ✕ | ✕ | ✕ | ✓ minimal | ✕ | ✕ | ✕ |
| female 4 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 5 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 6 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 7 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 8 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 9 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| Study Participant | Drug | Blunted Affect | Emotional Withdrawal | Poor Rapport | Social Withdrawal | Difficulty in Abstract Thinking | Lack of Spontaneity and Flow of Conversation | Stereotyped Thinking |
|---|---|---|---|---|---|---|---|---|
| male 1 | Δ9-THC | ✓ minimal | ✕ | ✕ | ✕ | ✕ | ✓ mild | ✓ minimal |
| male 2 | Δ9-THC | ✓ mild | ✕ | ✕ | ✕ | ✓ mild | ✓ mild | ✓ minimal |
| male 3 | Δ9-THC | ✕ | ✕ | ✓ mild | ✕ | ✓ moderate | ✓ minimal | ✓ mild |
| male 4 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 5 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ moderate | ✓ minimal |
| male 6 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✓ mild | ✕ | ✓ minimal |
| male 7 | Δ9-THC | ✓ mild | ✕ | ✓ moderate | ✕ | ✕ | ✓ moderate | ✓ mild |
| female 1 | Δ9-THC | ✓ minimal | ✓ mild | ✓ mild | ✓ mild | ✓ mild | ✓ mild | ✓ mild |
| female 2 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ mild | ✕ |
| female 3 | Δ9-THC | ✕ | ✓ mild | ✓ minimal | ✕ | ✕ | ✓ mild | ✕ |
| female 4 | Δ9-THC | ✓ mild | ✓ mild | ✓ mild | ✕ | ✓ moderate | ✓ moderate | ✓ mild |
| female 5 | Δ9-THC | ✓ mild | ✕ | ✓ mild | ✓ mild | ✓ moderate | ✓ mild | ✓ mild |
| female 6 | Δ9-THC | ✓ moderate | ✓ mild | ✓ mild | ✓ mild | ✕ | ✓ moderate | ✕ |
| female 7 | Δ9-THC | ✓ mild | ✓ moderate | ✓ mild | ✓ mild | ✓ moderate/ severe | ✓ mild | ✕ |
| female 8 | Δ9-THC | ✓ moderate/severe | ✓ moderate/severe | ✓ severe | ✓ moderate | ✓ moderate | ✓ moderate/severe | ✓ moderate |
| female 9 | Δ9-THC | ✓ mild | ✓ minimal | ✓ mild | ✕ | ✕ | ✕ | ✓ minimal |
| male 1 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 2 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 3 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 4 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 5 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ mild | ✕ |
| male 6 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 7 | placebo | ✕ | ✕ | ✓ mild | ✕ | ✕ | ✓ mild | ✕ |
| female 1 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 2 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 3 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 4 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 5 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 6 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 7 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 8 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 9 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| Study Participant | Drug | Somatic Concern | Anxiety | Guilt Feelings | Tension | Mannerism and Posturing | Depression | Motor Retardation | Uncooperative | Unusual Thought Content | Disorientation | Poor Attention | Lack of Judgment & Insight | Disturbance of Volition | Poor Impulse Control | Preoccupation | Active Social Avoidance |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| male 1 | Δ9-THC | ✓minimal | ✕ | ✕ | ✕ | ✓minimal | ↓ | ✕ | ✕ | ✕ | ✓minimal | ✓mild | ✕ | ✕ | ✓minimal | ✓mild | ✕ |
| male 2 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✓minimal | ✕ | ✓mild | ✕ | ✕ | ✓mild | ✓mild | ✕ | ✓mild | ✕ | ✓mild | ✓mild |
| male 3 | Δ9-THC | ✓mild | ✕ | ✓ mild | ✕ | ✕ | ✓minimal | ✕ | ✕ | ✓mild | ✓mild | ✓moderate | ✕ | ✓moderate | ✓mild | ✓mild | ✓minimal |
| male 4 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓minimal | ✕ | ✕ |
| male 5 | Δ9-THC | ✓mild | ✓mild | ✕ | ✓mild | ✕ | ✓mild | ✕ | ✕ | ✕ | ✓mild | ✓moderate | ✕ | ✓mild | ✓mild | ✓mild | ✕ |
| male 6 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✓moderate | ✕ | ✕ | ✕ | ✓mild | ✓minimal | ✓mild | ✓mild | ✓mild | ✓mild | ✕ | ✕ |
| male 7 | Δ9-THC | ✓mild | ✓minimal | ✕ | ✓minimal | ✕ | ✕ | ✓mild | ✓minimal | ✓minimal | ✓mild | ✓moderate | ✓mild | ✓moderate | ✕ | ✕ | ✕ |
| female 1 | Δ9-THC | ✕ | ✕ | ✓ minimal | ✓minimal | ✕ | ✓minimal | ✓mild | ✓mild | ✓minimal | ✓minimal | ✓mild | ✕ | ✓mild | ✓mild | ✕ | ✓minimal |
| female 2 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓minimal | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓minimal | ✕ | ✕ |
| female 3 | Δ9-THC | ✓mild | ✕ | ✕ | ✓mild | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓mild | ✕ | ✓mild | ✕ | ✓mild | ✕ |
| female 4 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✓minimal | ✕ | ✓mild | ✓minimal | ✓mild | ✓mild | ✓moderate | ✓mild | ✓mild | ✓mild | ✕ | ✓minimal |
| female 5 | Δ9-THC | ✓mild | ✓moderate | ✕ | ✓mild | ✓minimal | ✓minimal | ✕ | ✕ | ✓mild | ✓mild | ✓mild | ✕ | ✓mild | ✕ | ✓moderate | ✕ |
| female 6 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✓mild | ✓mild | ✓moderate | ✕ | ✕ | ✓mild | ✓moderate | ✓minimal | ✓mild | ✕ | ✕ | ✓mild |
| female 7 | Δ9-THC | ✓mild | ✓mild | ✕ | ✓mild | ✕ | ✕ | ✓mild | ✕ | ✕ | ✕ | ✓mild | ✕ | ✓mild | ✓minimal | ✓minimal | ✓mild |
| female 8 | Δ9-THC | ✓mild | ✓mild | ✕ | ✓mild | ✓mild | ✕ | ✓mod./severe | ✓minimal | ✓moderate | ✓mild | ✓moderate | ✓moderate | ✓moderate | ✕ | ✓mod./severe | ✓mild |
| female 9 | Δ9-THC | ✕ | ✕ | ✕ | ✕ | ✓minimal | ✕ | ✕ | ✓mild | ✓mild | ✕ | ✓moderate | ✓mild | ✕ | ✓minimal | ✕ | ✕ |
| male 1 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 2 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 3 | placebo | ✕ | ✓minimal | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓minimal | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 4 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 5 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓mild | ✓mild | ✕ | ✕ | ✓mild | ✕ | ✕ |
| male 6 | placebo | ✕ | ✓minimal | ✕ | ✓minimal | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| male 7 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓mild | ✕ | ✓mild | ✕ | ✕ | ✕ |
| female 1 | placebo | ✓mild | ✓minimal | ✕ | ✓mild | ✓minimal | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓mild | ✕ |
| female 2 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 3 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓minimal | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 4 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 5 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 6 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 7 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 8 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| female 9 | placebo | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ |
| Study Participant | Δ9-THC | Symptom |
| male 1 | ‘I was so stressed, irritable, and prone to anger that I started an argument with my partner the afternoon after the study’ | Hostility, irritability, mood lability |
| male 2 | ‘I feel I am all over the place and can’t stop laughing, thinking you will expose me, I will say something stupid or strange’ | Conceptual disorganization, thought disorder, loosening of associations, excitement |
| male 3 | ‘I can’t follow my thoughts, I am not able to think’ | Conceptual disorganization, racing thoughts |
| male 3 | ‘I can understand things better and look for details, I am superior to others’ | Grandiosity |
| male 3 | ‘I might have done something wrong, not willing to say’ | Feelings of guilt |
| male 3 | ‘I am thinking about death and cemeteries’ | Unusual thought content |
| male 6 | ‘The injection changed me into someone with increased abilities’ | Grandiosity |
| male 7 | ‘I am feeling quite confused and disoriented, like time is passing slower and the space is different, like from a camera zoom’ | Conceptual disorganization, disorientation |
| female 1 | ‘I am not interested and I am not willing to talk, I don’t care, I want just to go... I feel down, under the weather; maybe I am depressed’ | Negative symptoms, depression |
| female 4 | ‘What have you done to me? I understand, you want to make me paranoid with brainwashing questions...’ | Suspiciousness/paranoia with loss of insight |
| female 4 | ‘What an apple and a ball have in common...You can eat the apple, but not the ball’ | Difficulty in abstract thinking |
| female 5 | ‘I thought you were going to attack me, people are entering the room to check on me’ | Suspiciousness/paranoia, ideas of reference |
| female 7 | ‘What an apple and a ball have in common...You can put the apple in the ball’ | Difficulty in abstract thinking |
| female 8 | ‘My mind went blank, empty, with no thoughts’ | Thought blocking |
| female 8 | ‘The ventilator’s noise is louder...This noise is actually rain, it’s raining inside the room, I can see and feel it, there is a black sky with seven blue drops, I can count them, someone has opened the ceiling to let the rain in, and put my bed closer to the ceiling...Maybe someone is projecting a sky in front of me’ | Inability to ‘filter’ out irrelevant background stimuli, hallucinatory behavior, secondary delusions |
| female 9 | ‘Is this real? Is this a fake interview made by a fake doctor, like a Truman show?’ | Depersonalization/derealization |
| female 9 | ‘Colors are brighter, noises louder, and I have something making a noise in the back of my head’ | Hallucinatory behavior |
| male 3, 7; female 5, 7 | ‘I think I am going to chock up...something is wrong with my body...the heart is racing’ | Preoccupation/somatic concern, anxiety/tension |
| Study Participant | Placebo | Symptom |
| male 7 | ‘I felt spaced out, a little bit paranoid and upset after a conversation with someone who had a strange facial expression’ | Suspiciousness/paranoia |
| Study Participant | Δ9-THC |
| physical reactions | |
| female 2 | generalized tremors, vagal reaction |
| female 3 | about to faint |
| female 5 | about to faint, paleness |
| female 6 | about to faint, orthostatic hypotension, sick feeling |
| female 8 | flushing |
| observed symptoms | |
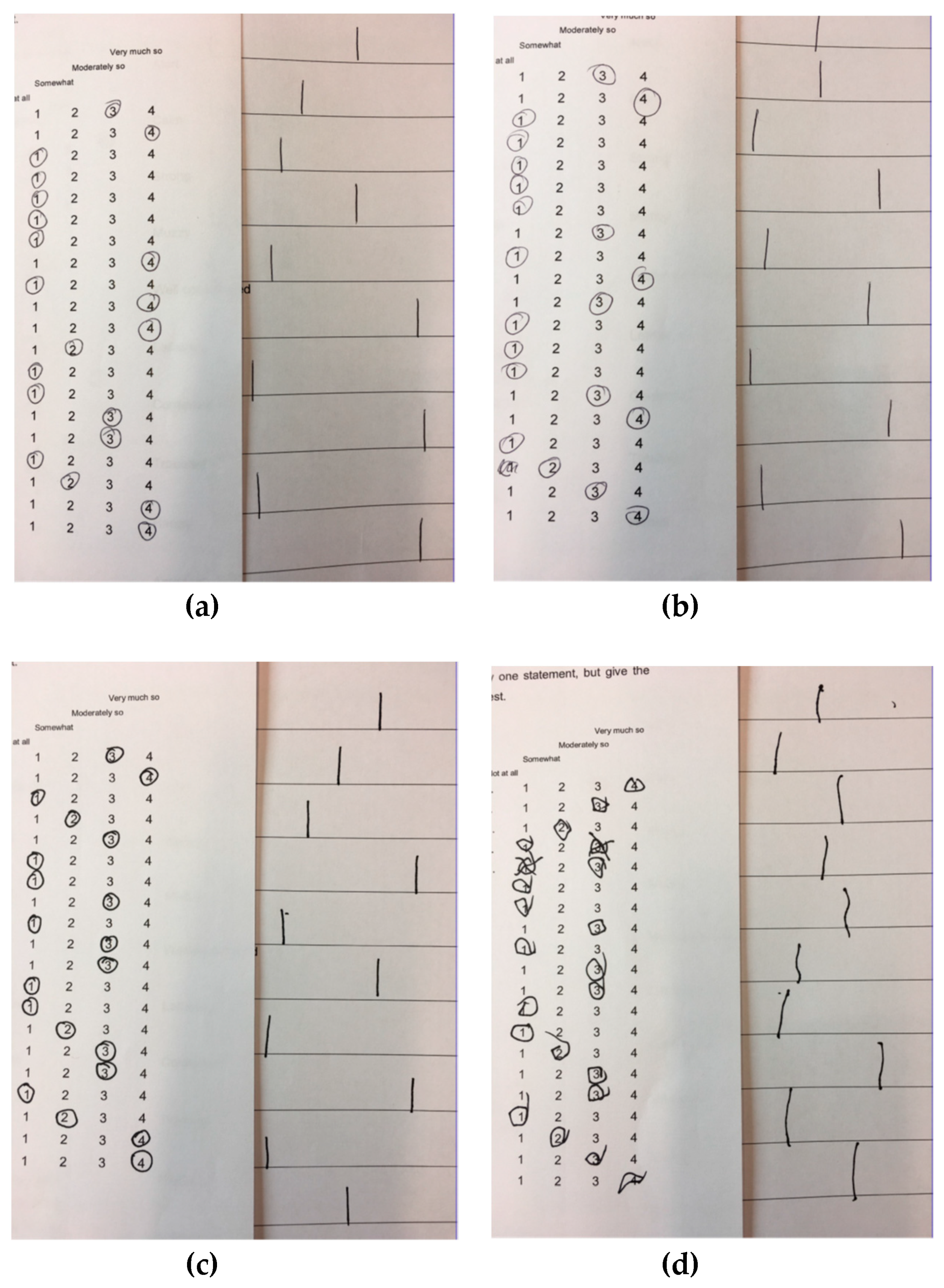
| males 2, 3, 6; females 1, 2, 3, 4, 8 | Different handwriting, errors and corrections in filling out the questionnaires (still present at 2.5 h after the injection for males 3 and 6) |
| male 6 | The participant kept the arm in a distinctively awkward position for 30 min |
| female 4 | The participant committed errors when asked four times to recall words related to a memory task (night instead of black 2/4, vegetable instead of apple 3/4, crisis instead of cries 4/4) |
| female 8 | The participant was internally absorbed and didn’t engage at all with a cognitive task |
| reported long-lasting symptoms (telephone follow-up) | |
| male 1 | suspiciousness, hostility, tension, and poor impulse control until afternoon |
| male 1 | headache, sick and weak feeling, fatigue, exhaustion, physical and mental strain until day after |
| male 2 | tiredness, sleepiness, postprandial somnolence |
| male 6 | disorientation and tiredness until evening |
| female 5 | tiredness and cravings for savory foods until afternoon |
| female 6 | tiredness, sleepiness, and hunger until the end of the day |
| female 9 | sleepiness, thirst, and hungry |
| females 1 and 4 | Symptoms reported during the trial were the same experienced in the past when using recreational cannabis |
| Study participant | Placebo |
| physical reactions | |
| female 1 | flushing, drowsiness, stomach pain |
| female 6 | flushing, increase in heart rate, heavy chest feeling |
| reported long-lasting symptoms (telephone follow-up) | |
| male 7 | suspiciousness until afternoon |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colizzi, M.; Weltens, N.; McGuire, P.; Van Oudenhove, L.; Bhattacharyya, S. Descriptive Psychopathology of the Acute Effects of Intravenous Delta-9-Tetrahydrocannabinol Administration in Humans. Brain Sci. 2019, 9, 93. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9040093
Colizzi M, Weltens N, McGuire P, Van Oudenhove L, Bhattacharyya S. Descriptive Psychopathology of the Acute Effects of Intravenous Delta-9-Tetrahydrocannabinol Administration in Humans. Brain Sciences. 2019; 9(4):93. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9040093
Chicago/Turabian StyleColizzi, Marco, Nathalie Weltens, Philip McGuire, Lukas Van Oudenhove, and Sagnik Bhattacharyya. 2019. "Descriptive Psychopathology of the Acute Effects of Intravenous Delta-9-Tetrahydrocannabinol Administration in Humans" Brain Sciences 9, no. 4: 93. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9040093