The Influence of a Conjugated Pneumococcal Vaccination on Plasma Antibody Levels against Oxidized Low-Density Lipoprotein in Metabolic Disease Patients: A Single-Arm Pilot Clinical Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
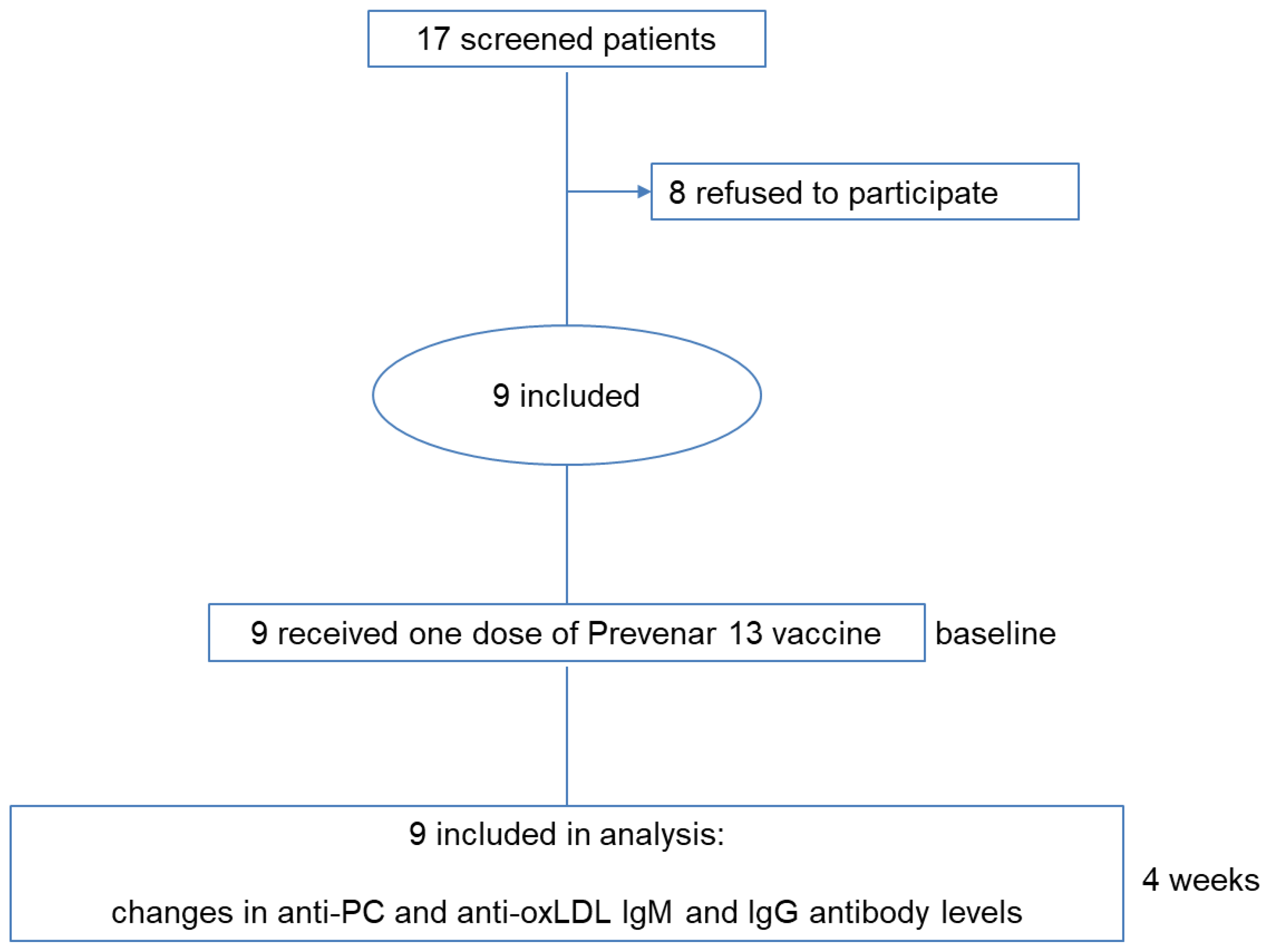
2.1. Patient Recruitment and Inclusion
2.2. Study Procedure and Outcomes
2.3. Antibody Measurements
2.4. Statistical Analysis
3. Results
3.1. Patient Population and Study Outcomes
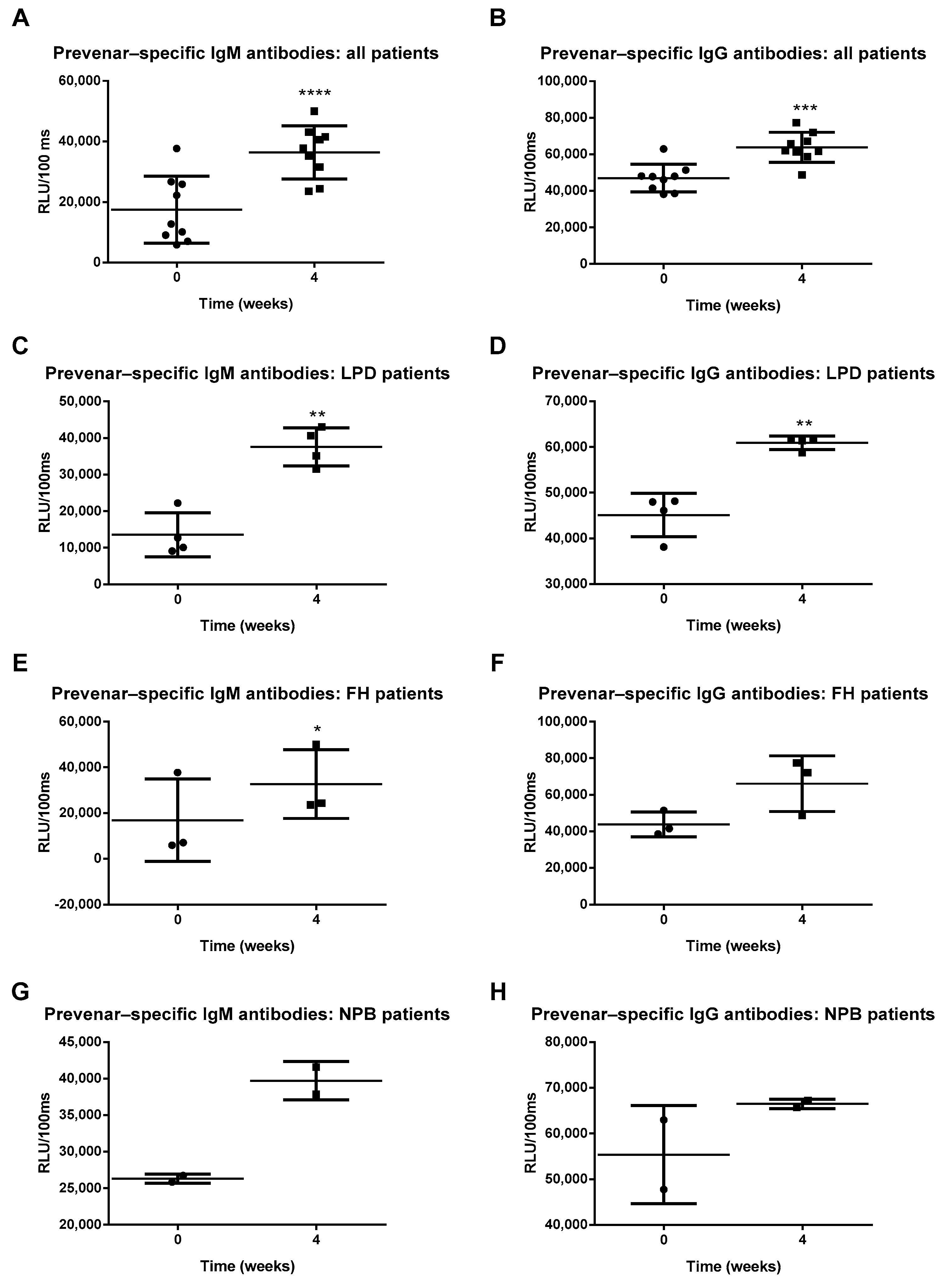
3.2. Prevenar 13 Vaccination Induced an Increase in Prevenar-Specific IgM and IgG Antibodies
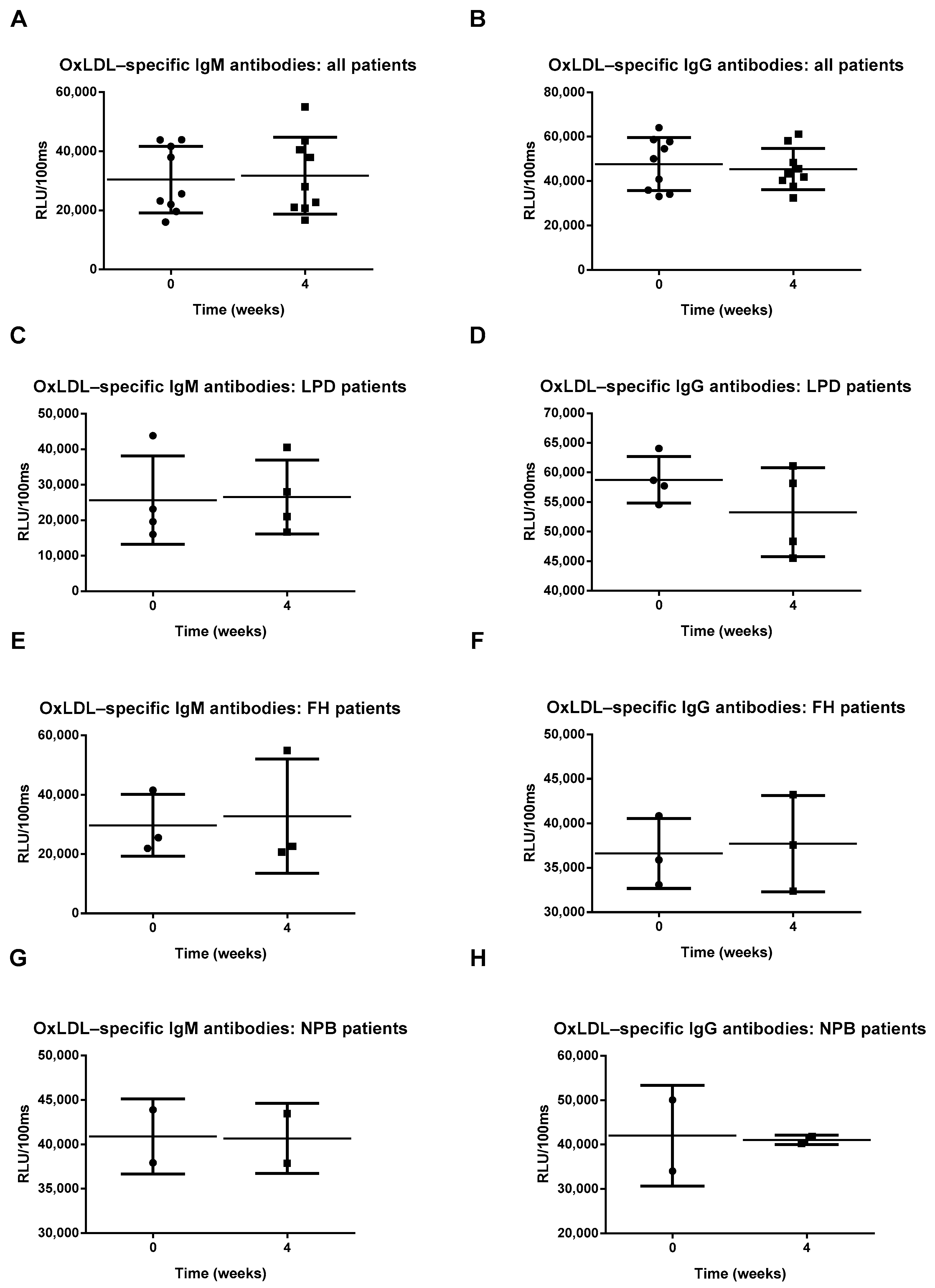
3.3. Prevenar 13 Vaccination Does Not Increase OxLDL or PC-Specific Antibody Titers
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rochlani, Y.; Pothineni, N.V.; Kovelamudi, S.; Mehta, J.L. Metabolic syndrome: Pathophysiology, management, and modulation by natural compounds. Ther. Adv. Cardiovasc. Dis. 2017, 11, 215–225. [Google Scholar] [CrossRef] [PubMed]
- WHO. Noncommunicable Diseases: Key Facts. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 17 July 2020).
- Levitan, I.; Volkov, S.; Subbaiah, P.V. Oxidized LDL: Diversity, Patterns of Recognition, and Pathophysiology. Antioxid. Redox Signal. 2010, 13, 39–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuura, E.; Hughes, G.R.; Khamashta, M.A. Oxidation of LDL and its clinical implication. Autoimmun. Rev. 2008, 7, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Omar, N.N.; El Hefnawy, M.H.; El-Soda, M.; Heider, N.M.; Hamed, H.I. Assessment of oxLDL, anti-oxLDL antibodies and lipoprotein-associated phospholipase A2 as cardiovascular risk markers in obese adolescents with and without T1DM. Bull. Fac. Pharmacy Cairo Univ. 2017, 55, 325–331. [Google Scholar] [CrossRef]
- Holvoet, P.; De Keyzer, D.; Jacobs, D.R., Jr. Oxidized LDL and the metabolic syndrome. Futur. Lipidol. 2008, 3, 637–649. [Google Scholar] [CrossRef]
- Su, J.; Georgiades, A.; Wu, R.; Thulin, T.; de Faire, U.; Frostegård, J. Antibodies of IgM subclass to phosphorylcholine and oxidized LDL are protective factors for atherosclerosis in patients with hypertension. Atherosclerosis 2006, 188, 160–166. [Google Scholar] [CrossRef]
- De Faire, U.; Frostegård, J. Natural Antibodies against Phosphorylcholine in Cardiovascular Disease. Ann. N. Y. Acad. Sci. 2009, 1173, 292–300. [Google Scholar] [CrossRef]
- De Faire, U.; Su, J.; Hua, X.; Frostegård, A.; Halldin, M.; Hellenius, M.-L.; Wikstrom, M.; Dahlbom, I.; Gronlund, H.; Frostegard, J.; et al. Low levels of IgM antibodies to phosphorylcholine predict cardiovascular disease in 60-year old men: Effects on uptake of oxidized LDL in macrophages as a potential mechanism. J. Autoimmun. 2010, 34, 73–79. [Google Scholar] [CrossRef]
- Vas, J.; Grönwall, C.; Silverman, G.J. Fundamental roles of the innate-like repertoire of natural antibodies in immune homeostasis. Front. Immunol. 2013, 4, 4. [Google Scholar] [CrossRef] [Green Version]
- Binder, C.J.; Hörkkö, S.; Dewan, A.T.; Chang, M.-K.; Kieu, E.P.; Goodyear, C.S.; Shaw, P.X.; Palinski, W.; Witztum, J.L.; Silverman, G.J. Pneumococcal vaccination decreases atherosclerotic lesion formation: Molecular mimicry between Streptococcus pneumoniae and oxidized LDL. Nat. Med. 2003, 9, 736–743. [Google Scholar] [CrossRef]
- Houben, T.; Dos Reis, I.M.; Oligschlaeger, Y.; Steinbusch, H.; Gijbels, M.J.J.; Hendrikx, T.; Binder, C.J.; Cassiman, D.; Westerterp, M.; Prickaerts, J.; et al. Pneumococcal Immunization Reduces Neurological and Hepatic Symptoms in a Mouse Model for Niemann-Pick Type C1 Disease. Front. Immunol. 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Bieghs, V.; Van Gorp, P.J.J.; Walenbergh, S.M.; Gijbels, M.J.; Verheyen, F.; Buurman, W.A.; Briles, D.E.; Hofker, M.H.; Binder, C.J.; Shiri-Sverdlov, R. Specific immunization strategies against oxidized low-density lipoprotein: A novel way to reduce nonalcoholic steatohepatitis in mice. Hepatology 2012, 56, 894–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.; Seidman, J.S.; Zhao, P.; Troutman, T.D.; Spann, N.J.; Que, X.; Zhou, F.; Liao, Z.; Pasillas, M.; Yang, X.; et al. Neutralization of Oxidized Phospholipids Ameliorates Non-alcoholic Steatohepatitis. Cell Metab. 2020, 31, 189–206. [Google Scholar] [CrossRef] [PubMed]
- Hendrikx, T.; Watzenböck, M.L.; Walenbergh, S.M.A.; Amir, S.; Gruber, S.; Kozma, M.O.; Grabsch, H.I.; Koek, G.H.; Pierik, M.J.; Staufer, K.; et al. Low levels of IgM antibodies recognizing oxidation-specific epitopes are associated with human non-alcoholic fatty liver disease. BMC Med. 2016, 14, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ylä-Herttuala, S.; Palinski, W.; Butler, S.W.; Picard, S.; Steinberg, D.; Witztum, J.L. Rabbit and human atherosclerotic lesions contain IgG that recognizes epitopes of oxidized LDL. Arter. Thromb. J. Vasc. Biol. 1994, 14, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schenkein, H.A.; Berry, C.R.; Purkall, D.; Burmeister, J.A.; Brooks, C.N.; Tew, J.G. Phosphorylcholine-Dependent Cross-Reactivity between Dental Plaque Bacteria and Oxidized Low-Density Lipoproteins. Infect. Immun. 2001, 69, 6612–6617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, J.T.; Myers, N.; Palaia, J.; Georgopoulos, A.; Rubins, J.B.; Janoff, E.N. Humoral responses to oxidized low-density lipoprotein and related bacterial antigens after pneumococcal vaccine. Transl. Res. 2007, 150, 172–179. [Google Scholar] [CrossRef]
- Even, G.; Kiss, M.; Laschet, J.; Kozma, M.O.; Simon, T.; Wigren, M.; Gaston, A.; Procopio, E.; Le Borgne, M.; Nilsson, J.; et al. Vaccination with Prevenar® boosts the production of anti-phosphorylcholine antibodies and protects APOE knockout mice from atherosclerosis. Atherosclerosis 2018, 275, e6–e7. [Google Scholar] [CrossRef]
- Mestas, J.; Hughes, C.C.W. Of mice and not men: Differences between mouse and human immunology. J. Immunol. 2004, 172, 2731–2738. [Google Scholar] [CrossRef] [Green Version]
- Tao, L.; Reese, T.A. Making Mouse Models That Reflect Human Immune Responses. Trends Immunol. 2017, 38, 181–193. [Google Scholar] [CrossRef] [Green Version]
- Damoiseaux, J.; Rijkers, G.; Tervaert, J.W.C. Pneumococcal vaccination does not increase circulating levels of IgM antibodies to oxidized LDL in humans and therefore precludes an anti-atherogenic effect. Atherosclerosis 2007, 190, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Lafon, D.C.; Nahm, M.H. Measuring immune responses to pneumococcal vaccines. J. Immunol. Methods 2018, 461, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Grievink, H.W.; Gal, P.; Kozma, M.O.; Klaassen, E.S.; Kuiper, J.; Burggraaf, J.; Binder, C.J.; Moerland, M. The Effect of a 13-Valent Conjugate Pneumococcal Vaccine on Circulating Antibodies against Oxidized LDL and Phosphorylcholine in Man, A Randomized Placebo-Controlled Clinical Trial. Biology 2020, 9, 345. [Google Scholar] [CrossRef] [PubMed]
- Carl, E.; Frasch, N.F.C. Specificity of Human Antibodies Reactive with Pneumococcal C Polysaccharide. Infect Immun. 2000. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Sex | Age |
|---|---|---|
| Familial partial lipodystrophy | Female | 28 |
| Female | 38 | |
| Female | 37 | |
| Female | 38 | |
| Familial hypercholesterolemia | Male | 15 |
| Female | 11 | |
| Male | 13 | |
| Niemann–Pick type B | Male | 36 |
| Male | 38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiri-Sverdlov, R.; dos Reis, I.M.; Oligschlaeger, Y.; Hendrikx, T.; Meesters, D.M.; Vanclooster, A.; Vanhoutvin, N.; Koek, G.H.; Westerterp, M.; Binder, C.J.; et al. The Influence of a Conjugated Pneumococcal Vaccination on Plasma Antibody Levels against Oxidized Low-Density Lipoprotein in Metabolic Disease Patients: A Single-Arm Pilot Clinical Trial. Antioxidants 2021, 10, 129. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10010129
Shiri-Sverdlov R, dos Reis IM, Oligschlaeger Y, Hendrikx T, Meesters DM, Vanclooster A, Vanhoutvin N, Koek GH, Westerterp M, Binder CJ, et al. The Influence of a Conjugated Pneumococcal Vaccination on Plasma Antibody Levels against Oxidized Low-Density Lipoprotein in Metabolic Disease Patients: A Single-Arm Pilot Clinical Trial. Antioxidants. 2021; 10(1):129. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10010129
Chicago/Turabian StyleShiri-Sverdlov, Ronit, Inês Magro dos Reis, Yvonne Oligschlaeger, Tim Hendrikx, Dennis M. Meesters, Annick Vanclooster, Nele Vanhoutvin, Ger H. Koek, Marit Westerterp, Christoph J. Binder, and et al. 2021. "The Influence of a Conjugated Pneumococcal Vaccination on Plasma Antibody Levels against Oxidized Low-Density Lipoprotein in Metabolic Disease Patients: A Single-Arm Pilot Clinical Trial" Antioxidants 10, no. 1: 129. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10010129