
Mediterranean Diet and Physical Activity Decrease the Initiation of Cardiovascular Drug Use in High Cardiovascular Risk Individuals: A Cohort Study

 , ,
, ,  , , , , , , , , , , and
, , , , , , , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
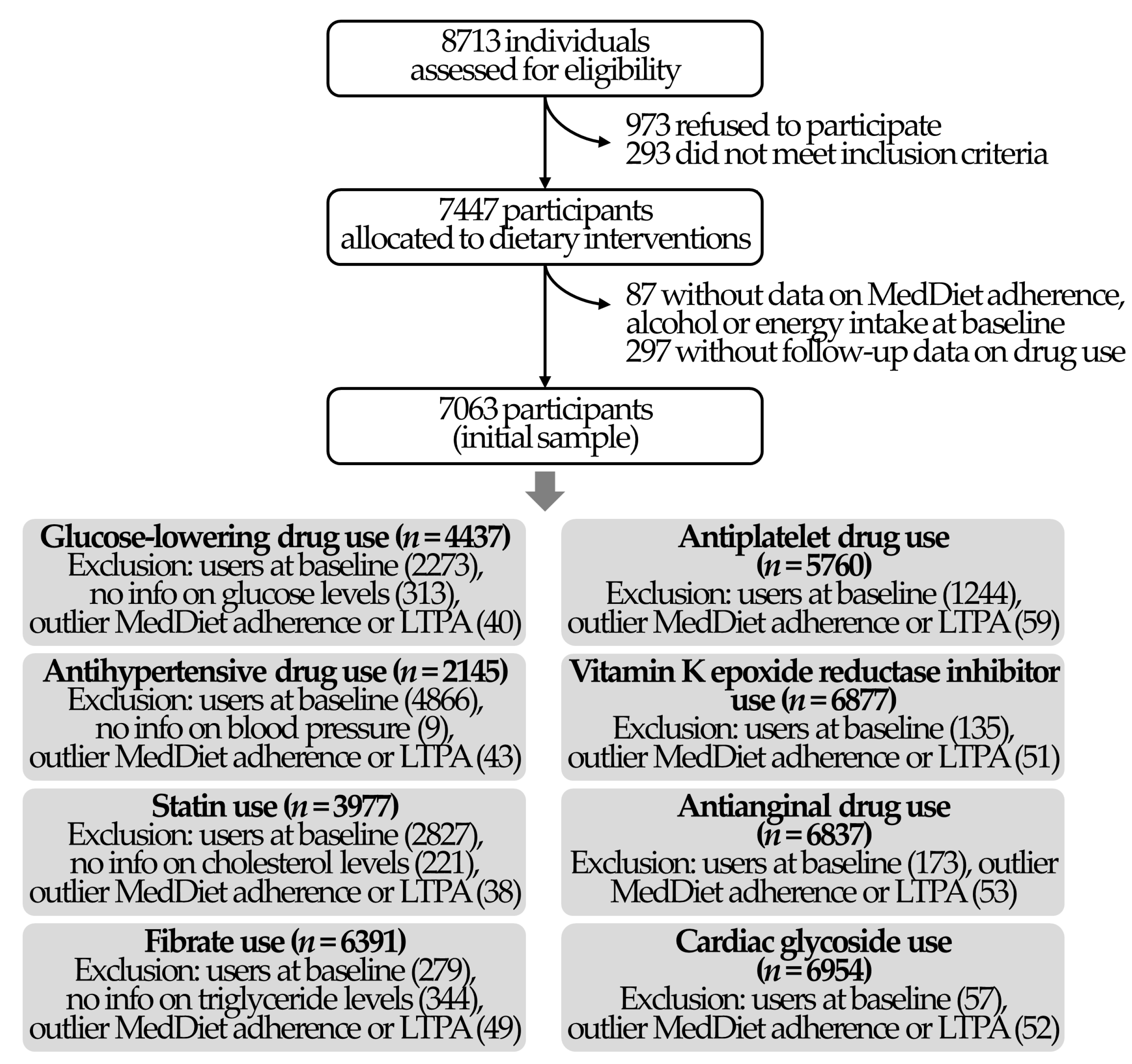
2.1. Study Population
2.2. Outcomes
2.3. Exposure Variables
2.4. Covariates
2.5. Power Analyses
2.6. Statistical Analyses
3. Results
3.1. Study Population
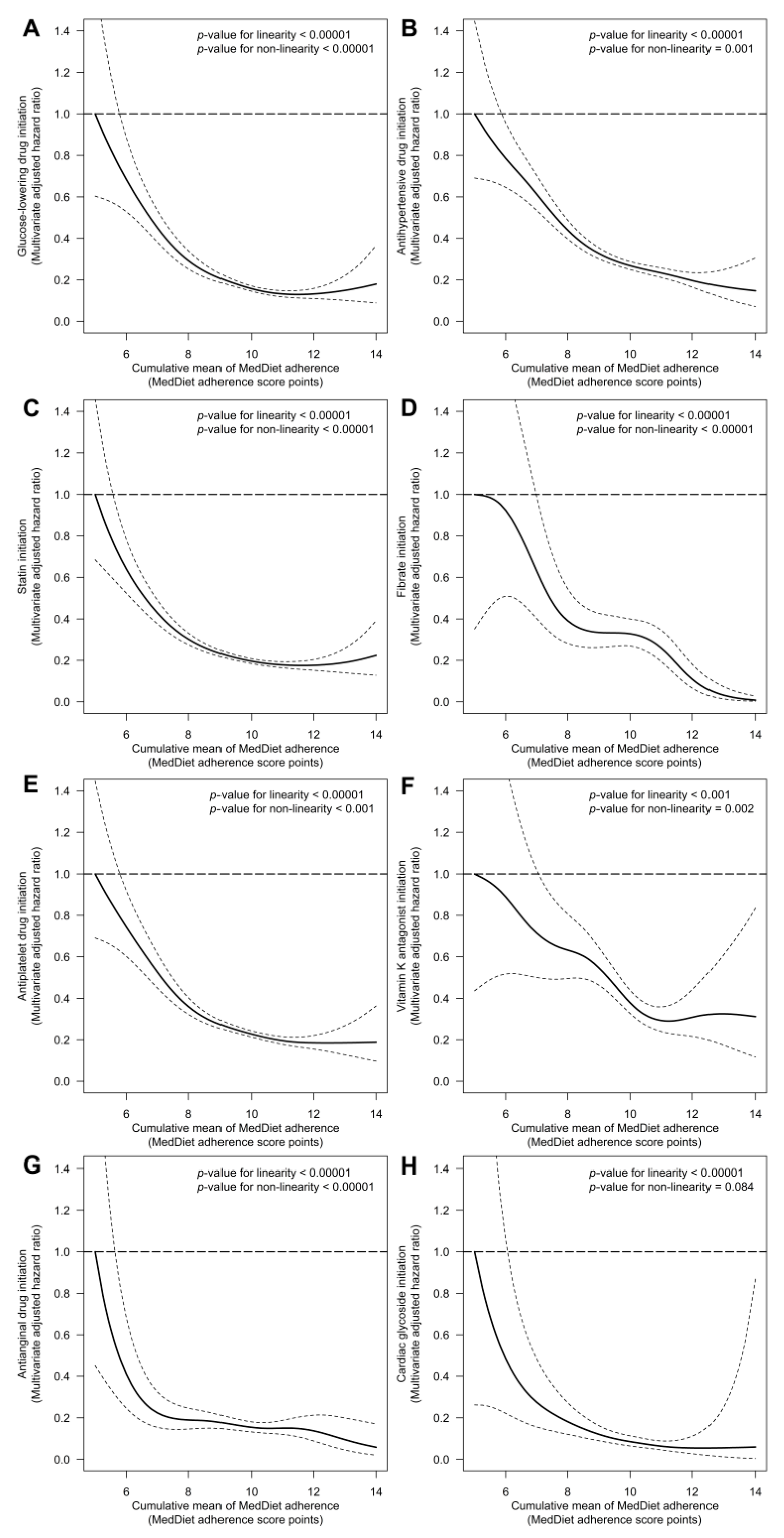
3.2. MedDiet Adherence and Risk of Cardiovascular Drug Initiation
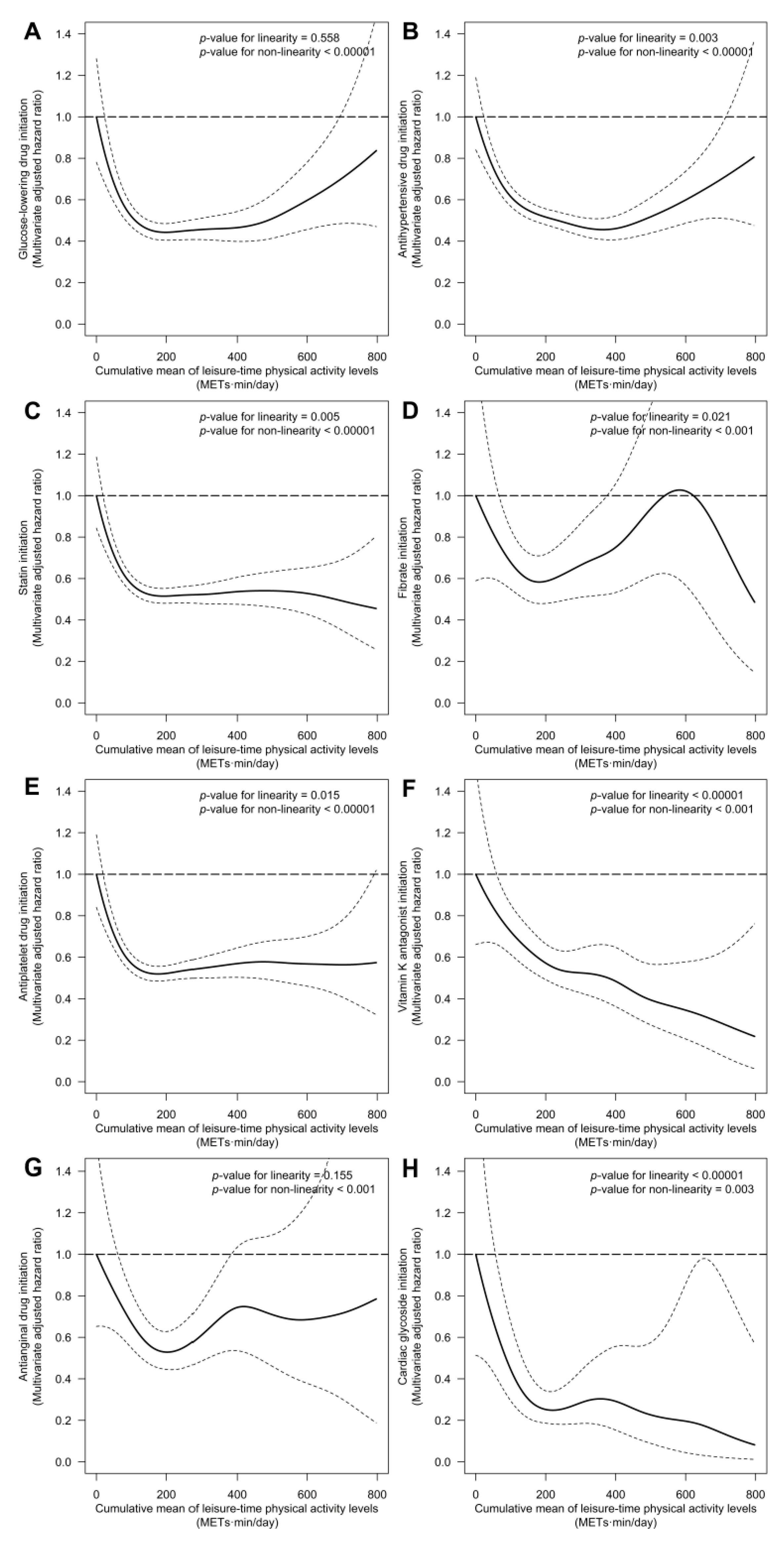
3.3. LTPA Levels and Risk of Cardiovascular Drug Initiation
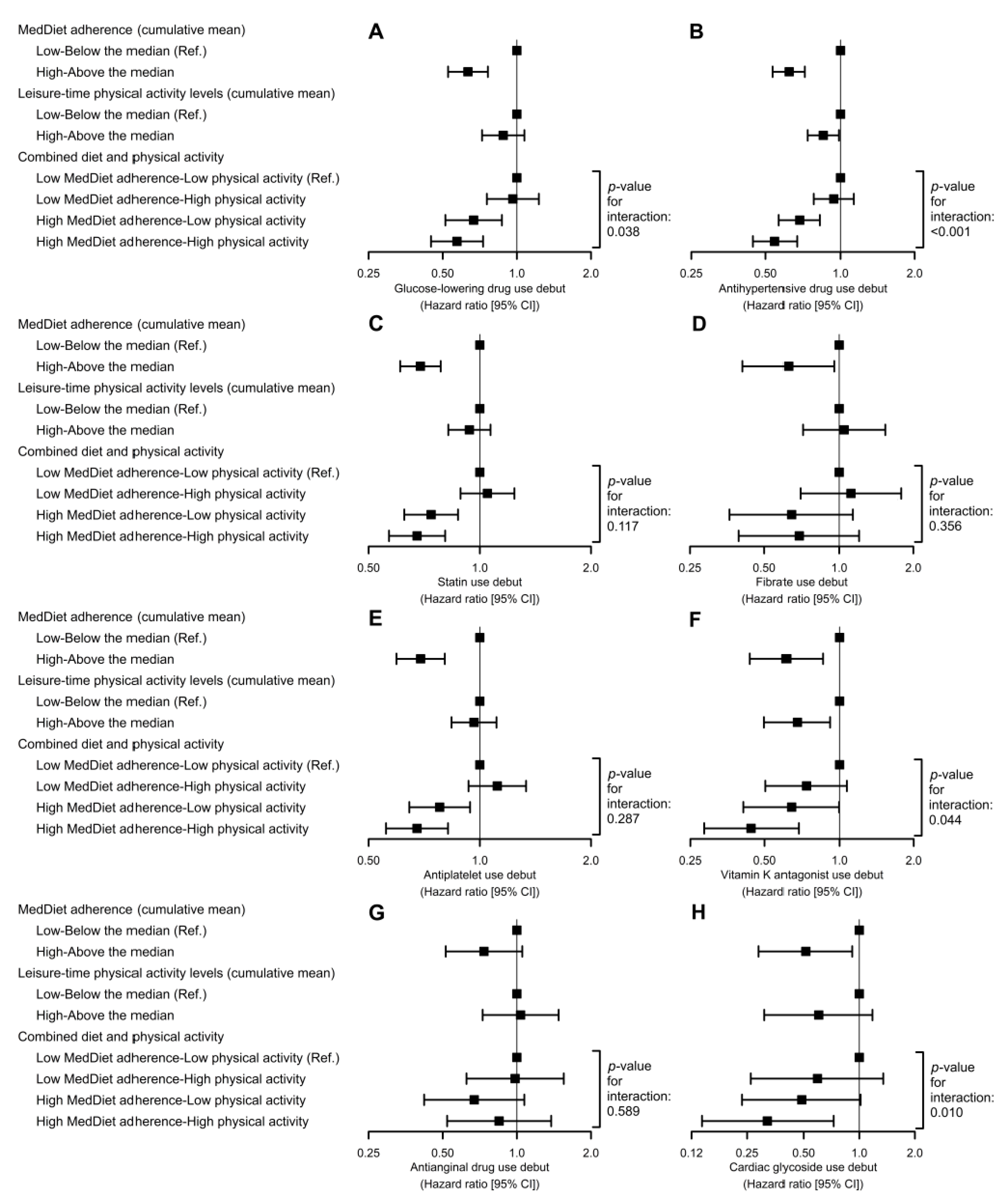
3.4. Adherence to a MedDiet Combined with LTPA Levels and Risk of Cardiovascular Drug Initiation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Wahid, A.; Manek, N.; Nichols, M.; Kelly, P.; Foster, C.; Webster, P.; Kaur, A.; Friedemann Smith, C.; Wilkins, E.; Rayner, M.; et al. Quantifying the association between physical activity and cardiovascular disease and diabetes: A systematic review and meta-analysis. J. Am. Heart Assoc. 2016, 5, e002495. [Google Scholar] [CrossRef] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Pattyn, N.; Cornelissen, V.A.; Eshghi, S.R.T.; Vanhees, L. The effect of exercise on the cardiovascular risk factors constituting the metabolic syndrome: A meta-analysis of controlled trials. Sports Med. 2013, 43, 121–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basterra-Gortari, F.J.; Ruiz-Canela, M.; Martínez-González, M.A.; Babio, N.; Sorlí, J.V.; Fito, M.; Ros, E.; Gómez-Gracia, E.; Fiol, M.; Lapetra, J.; et al. Effects of a Mediterranean eating plan on the need for glucose-lowering medications in participants with type 2 diabetes: A subgroup analysis of the PREDIMED trial. Diabetes Care 2019, 42, 1390–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, K.; Maiorino, M.I.; Petrizzo, M.; Bellastella, G.; Giugliano, D. The effects of a Mediterranean diet on the need for diabetes drugs and remission of newly diagnosed type 2 diabetes: Follow-up of a randomized trial. Diabetes Care 2014, 37, 1824–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, C.S.; Johansen, M.Y.; Nielsen, S.M.; Christensen, R.; Hansen, K.B.; Langberg, H.; Vaag, A.A.; Karstoft, K.; Lieberman, D.E.; Pedersen, B.K.; et al. Dose-response effects of exercise on glucose-lowering medications for type 2 diabetes: A secondary analysis of a randomized clinical trial. Mayo Clin. Proc. 2020, 95, 488–503. [Google Scholar] [CrossRef] [Green Version]
- Shendre, A.; Beasley, T.M.; Brown, T.M.; Hill, C.E.; Arnett, D.K.; Limdi, N.A. Influence of regular physical activity on warfarin dose and risk of hemorrhagic complications. Pharmacotherapy 2014, 34, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Barengo, N.C.; Hu, G.; Kastarinen, M.; Lakka, T.A.; Pekkarinen, H.; Nissinen, A.; Tuomilehto, J. Low physical activity as a predictor for antihypertensive drug treatment in 25–64-year-old populations in Eastern and South-Western Finland. J. Hypertens. 2005, 23, 293–299. [Google Scholar] [CrossRef]
- Alvarez-Alvarez, I.; de Rojas, J.P.; Fernandez-Montero, A.; Zazpe, I.; Ruiz-Canela, M.; Hidalgo-Santamaría, M.; Bes-Rastrollo, M.; Martínez-González, M. Strong inverse associations of Mediterranean diet, physical activity and their combination with cardiovascular disease: The Seguimiento Universidad de Navarra (SUN) cohort. Eur. J. Prev. Cardiol. 2018, 25, 1186–1197. [Google Scholar] [CrossRef]
- Cárdenas-Fuentes, G.; Subirana, I.; Martinez-Gonzalez, M.A.; Salas-Salvadó, J.; Corella, D.; Estruch, R.; Fíto, M.; Muñoz-Bravo, C.; Fiol, M.; Lapetra, J.; et al. Multiple approaches to associations of physical activity and adherence to the Mediterranean diet with all-cause mortality in older adults: The PREvención con DIeta MEDiterránea study. Eur. J. Nutr. 2019, 58, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Malakou, E.; Linardakis, M.; Armstrong, M.; Zannidi, D.; Foster, C.; Johnson, L.; Papadaki, A. The combined effect of promoting the Mediterranean diet and physical activity on metabolic risk factors in adults: A systematic review and meta-analysis of randomised controlled trials. Nutrients 2018, 10, 1577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salas-Salvadó, J.; Díaz-López, A.; Ruiz-Canela, M.; Basora, J.; Fitó, M.; Corella, D.; Serra-Majem, L.; Wärnberg, J.; Romaguera, D.; Estruch, R.; et al. Effect of a lifestyle intervention program with energy-restricted mediterranean diet and exercise on weight loss and cardiovascular risk factors: One-year results of the PREDIMED-plus trial. Diabetes Care 2018, 42, dc180836. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ros, E.; Covas, M.I.; Fiol, M.; Warnberg, J.; Aros, F.; Ruiz-Gutierrez, V.; Lamuela-Raventos, R.M.; et al. Cohort profile: Design and methods of the PREDIMED study. Int. J. Epidemiol. 2012, 41, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the Minnesota leisure time physical activity questionnaire in Spanish men. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Garcia, M.; Aguilar, A.; Molina, L.; Covas, M.I.; Marrugat, J. Validation of the Minnesota leisure time physical activity questionnaire in Spanish women. Investigators of the MARATDON group. Med. Sci. Sports Exerc. 2000, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Weiliang Qiu, A.; Chavarro, J.; Weiliang Qiu, M.; Qiu, W.; Chavarro, J.; Lazarus, R.; Rosner, B.; Ma, J. Package “powerSurvEpi”: Power and Sample Size Calculation for Survival Analysis of Epidemiological Studies. 2018. Available online: https://cran.r-project.org/web/packages/powerSurvEpi/powerSurvEpi.pdf (accessed on 28 January 2021).
- Schmidt, C.O.; Ittermann, T.; Schulz, A.; Grabe, H.J.; Baumeister, S.E. Linear, nonlinear or categorical: How to treat complex associations? Splines and nonparametric approaches. Int. J. Public Health 2013, 58, 161–165. [Google Scholar] [CrossRef]
- Therneau, T.M. Package “Survival”: Survival Analysis. 2018. Available online: https://cran.r-project.org/web/packages/survival/survival.pdf (accessed on 28 January 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Castro-Barquero, S.; Ribó-Coll, M.; Lassale, C.; Tresserra-Rimbau, A.; Castañer, O.; Pintó, X.; Martínez-González, M.Á.; Sorlí, J.V.; Salas-Salvadó, J.; Lapetra, J.; et al. Mediterranean diet decreases the initiation of use of vitamin k epoxide reductase inhibitors and their associated cardiovascular risk: A randomized controlled trial. Nutrients 2020, 12, 3895. [Google Scholar] [CrossRef] [PubMed]
- Nissensohn, M.; Román-Viñas, B.; Sánchez-Villegas, A.; Piscopo, S.; Serra-Majem, L. The effect of the Mediterranean diet on hypertension: A systematic review and meta-analysis. J. Nutr. Educ. Behav. 2016, 48, 42–53.e1. [Google Scholar] [CrossRef]
- Capurso, C.; Massaro, M.; Scoditti, E.; Vendemiale, G.; Capurso, A. Vascular effects of the Mediterranean diet part I: Anti-hypertensive and anti-thrombotic effects. Vascul. Pharmacol. 2014, 63, 118–126. [Google Scholar] [CrossRef]
- Sanches Machado d’Almeida, K.; Ronchi Spillere, S.; Zuchinali, P.; Corrêa Souza, G. Mediterranean diet and other dietary patterns in primary prevention of heart failure and changes in cardiac function markers: A systematic review. Nutrients 2018, 10, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitjavila, M.T.; Fandos, M.; Salas-Salvadó, J.; Covas, M.-I.; Borrego, S.; Estruch, R.; Lamuela-Raventós, R.; Corella, D.; Martínez-Gonzalez, M.A.; Sánchez, J.M.; et al. The Mediterranean diet improves the systemic lipid and DNA oxidative damage in metabolic syndrome individuals. A randomized, controlled, trial. Clin. Nutr. 2013, 32, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Sacanella, E.; Urpí-Sardà, M.; Chiva-Blanch, G.; Ros, E.; Martínez-González, M.-A.; Covas, M.-I.; Salas-Salvadó, J.; Fiol, M.; Arós, F.; et al. The effects of the Mediterranean diet on biomarkers of vascular wall inflammation and plaque vulnerability in subjects with high risk for cardiovascular disease. A randomized trial. PLoS ONE 2014, 9, e100084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health benefits of the Mediterranean diet: Metabolic and molecular mechanisms. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, A.; Garg, S.; Khunger, M.; Darden, D.; Ayers, C.; Kumbhani, D.J.; Mayo, H.G.; De Lemos, J.A.; Berry, J.D. Dose-response relationship between physical activity and risk of heart failure: A meta-analysis. Circulation 2015, 132, 1786–1794. [Google Scholar] [CrossRef] [Green Version]
- Kitzman, D.W.; Brubaker, P.; Morgan, T.; Haykowsky, M.; Hundley, G.; Kraus, W.E.; Eggebeen, J.; Nicklas, B.J. Effect of caloric restriction or aerobic exercise training on peak oxygen consumption and quality of life in obese older patients with heart failure with preserved ejection fraction. JAMA 2016, 315, 36. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Bulló, M.; Babio, N.; Martínez-González, M.Á.; Ibarrola-Jurado, N.; Basora, J.; Estruch, R.; Covas, M.I.; Corella, D.; Arós, F.; et al. Reduction in the incidence of type 2 diabetes with the Mediterranean diet: Results of the PREDIMED-reus nutrition intervention randomized trial. Diabetes Care 2011, 34, 14–19. [Google Scholar] [CrossRef] [Green Version]
- Toledo, E.; Hu, F.B.; Estruch, R.; Buil-Cosiales, P.; Corella, D.; Salas-Salvadó, J.; Covas, M.I.; Arós, F.; Gómez-Gracia, E.; Fiol, M.; et al. Effect of the Mediterranean diet on blood pressure in the PREDIMED trial: Results from a randomized controlled trial. BMC Med. 2013, 11, 207. [Google Scholar] [CrossRef] [Green Version]
- Hernáez, Á.; Castañer, O.; Tresserra-Rimbau, A.; Pintó, X.; Fitó, M.; Casas, R.; Martínez-González, M.Á.; Corella, D.; Salas-Salvadó, J.; Lapetra, J.; et al. Mediterranean diet and atherothrombosis biomarkers: A randomized controlled trial. Mol. Nutr. Food Res. 2020, 64, 2000350. [Google Scholar] [CrossRef] [PubMed]
- Fitó, M.; Estruch, R.; Salas-Salvadó, J.; Martínez-Gonzalez, M.A.; Arós, F.; Vila, J.; Corella, D.; Díaz, O.; Sáez, G.; de la Torre, R.; et al. Effect of the Mediterranean diet on heart failure biomarkers: A randomized sample from the PREDIMED trial. Eur. J. Heart Fail. 2014, 16, 543–550. [Google Scholar] [CrossRef] [Green Version]
- Hurrle, S.; Hsu, W.H. The etiology of oxidative stress in insulin resistance. Biomed. J. 2017, 40, 257–262. [Google Scholar] [CrossRef]
- Schulz, E.; Gori, T.; Münzel, T. Oxidative stress and endothelial dysfunction in hypertension. Hypertens. Res. 2011, 34, 665–673. [Google Scholar] [CrossRef]
- Freedman, J.E. Oxidative stress and platelets. Arterioscler. Thromb. Vasc. Biol. 2008, 28, s11–s16. [Google Scholar] [CrossRef] [Green Version]
- Madamanchi, N.R.; Hakim, Z.S.; Runge, M.S. Oxidative stress in atherogenesis and arterial thrombosis: The disconnect between cellular studies and clinical outcomes. J. Thromb. Haemost. 2005, 3, 254–267. [Google Scholar] [CrossRef]
- Eleuteri, E.; Magno, F.; Gnemmi, I.; Carbone, M.; Colombo, M.; La Rocca, G.; Anzalone, R.; Genta, F.T.; Zummo, G.; Di Stefano, A.; et al. Role of oxidative and nitrosative stress biomarkers in chronic heart failure. Front. Biosci. 2009, 14, 2230–2237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viollet, B.; Andreelli, F. AMP-activated protein kinase and metabolic control. In Diabetes—Perspectives in Drug Therapy; Springer: Berlin/Heidelberg, Germany, 2011; pp. 303–330. [Google Scholar]
- Salt, I.P.; Hardie, D.G. AMP-Activated protein kinase. Circ. Res. 2017, 120, 1825–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herzig, S.; Shaw, R.J. AMPK: Guardian of metabolism and mitochondrial homeostasis. Nat. Rev. Mol. Cell Biol. 2018, 19, 121–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Main Analytical Sample (n = 7063) | |
|---|---|
| Age (years), mean ± SD | 67.0 ± 6.2 |
| Female sex, n (%) | 4080 (57.8) |
| Diabetes, n (%) | 3442 (48.7) |
| Hypercholesterolemia, n (%) | 5087 (72.0) |
| Hypertriglyceridemia, n (%) | 2045 (29.0) |
| Hypertension, n (%) | 5834 (82.6) |
| Smoking habit: | |
| Never smokers, n (%) | 4345 (61.5) |
| Current smokers, n (%) | 985 (13.9) |
| Former smokers, n (%) | 1733 (24.5) |
| Weight status (according to body mass index): | |
| 18.5–24.9 kg/m2, n (%) | 523 (7.40) |
| 25.0–29.9 kg/m2, n (%) | 3207 (45.4) |
| ≥30 kg/m2, n (%) | 3333 (47.2) |
| PREDIMED Study intervention groups: | |
| MedDiet enriched with extra-virgin olive oil, n (%) | 2465 (34.9) |
| MedDiet enriched with mixed nuts, n (%) | 2308 (32.7) |
| Control group, n (%) | 2290 (32.4) |
| MedDiet adherence score, mean ± SD | 8.69 ± 1.90 |
| Leisure-time physical activity (metabolic equivalents of task-min/day), median (1st–3rd quartile) | 175 (66.1–319) |
| Alcohol intake (g/day), median (1st–3rd quartile) | 1.49 (0.00–10.4) |
| Energy intake (kcal/day), mean ± SD | 2274 ± 604 |
| Carbohydrates (g/day), median (1st–3rd quartile) | 227 (182–279) |
| Protein (g/day), median (1st–3rd quartile) | 90.2 (77.0–106) |
| Total fat (g/day), median (1st–3rd quartile) | 96.4 (77.5–116) |
| Saturated fat (g/day), median (1st–3rd quartile) | 24.1 (19.1–30.1) |
| Monounsaturated fat (g/day), median (1st–3rd quartile) | 48.5 (36.4–58.9) |
| Polyunsaturated fat (g/day), median (1st–3rd quartile) | 14.4 (11.0–19.3) |
| Omega-3 polyunsaturated fat (g/day), median (1st–3rd quartile) | 2.04 (1.56–2.68) |
| Fiber (g/day), median (1st–3rd quartile) | 24.0 (19.4–29.9) |
| Dietary cholesterol (mg/day), median (1st–3rd quartile) | 357 (284–429) |
| Sodium (mg/day), median (1st–3rd quartile) | 2263 (1767–2877) |
| Potassium (mg/day), median (1st–3rd quartile) | 4195 (3586–4940) |
| Calcium (mg/day), median (1st–3rd quartile) | 993 (779–1274) |
| Dietary vitamin D (μg/day), median (1st–3rd quartile) | 4.77 (3.33–8.61) |
| Vitamin C (mg/day), median (1st–3rd quartile) | 184 (139–245) |
| Vitamin E (mg/day), median (1st–3rd quartile) | 9.31 (7.57–11.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribó-Coll, M.; Castro-Barquero, S.; Lassale, C.; Sacanella, E.; Ros, E.; Toledo, E.; Sorlí, J.V.; Díaz-López, A.; Lapetra, J.; Muñoz-Bravo, C.; et al. Mediterranean Diet and Physical Activity Decrease the Initiation of Cardiovascular Drug Use in High Cardiovascular Risk Individuals: A Cohort Study. Antioxidants 2021, 10, 397. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10030397
Ribó-Coll M, Castro-Barquero S, Lassale C, Sacanella E, Ros E, Toledo E, Sorlí JV, Díaz-López A, Lapetra J, Muñoz-Bravo C, et al. Mediterranean Diet and Physical Activity Decrease the Initiation of Cardiovascular Drug Use in High Cardiovascular Risk Individuals: A Cohort Study. Antioxidants. 2021; 10(3):397. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10030397
Chicago/Turabian StyleRibó-Coll, Margarita, Sara Castro-Barquero, Camille Lassale, Emilio Sacanella, Emilio Ros, Estefanía Toledo, José V. Sorlí, Andrés Díaz-López, José Lapetra, Carlos Muñoz-Bravo, and et al. 2021. "Mediterranean Diet and Physical Activity Decrease the Initiation of Cardiovascular Drug Use in High Cardiovascular Risk Individuals: A Cohort Study" Antioxidants 10, no. 3: 397. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10030397