
Influences on Pregnant Women’s and Health Care Professionals’ Behaviour Regarding Maternal Vaccinations: A Qualitative Interview Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting—New Zealand and Specifically the Waikato Region
2.2. Study Design
2.3. Recruitment and Interview Process
2.4. Analysis
2.5. Researchers’ Roles and Perspectives
3. Results
3.1. The Sample
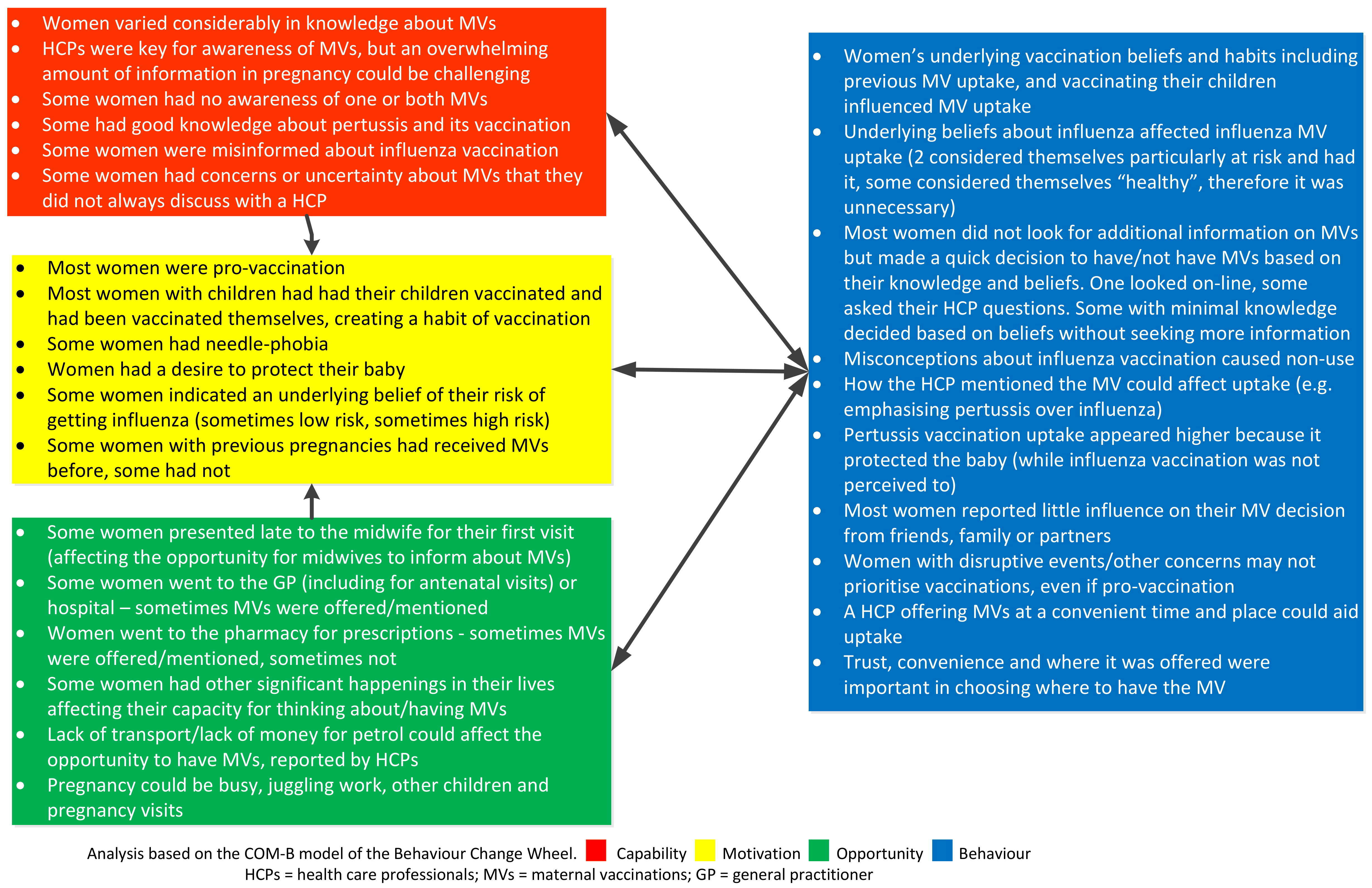
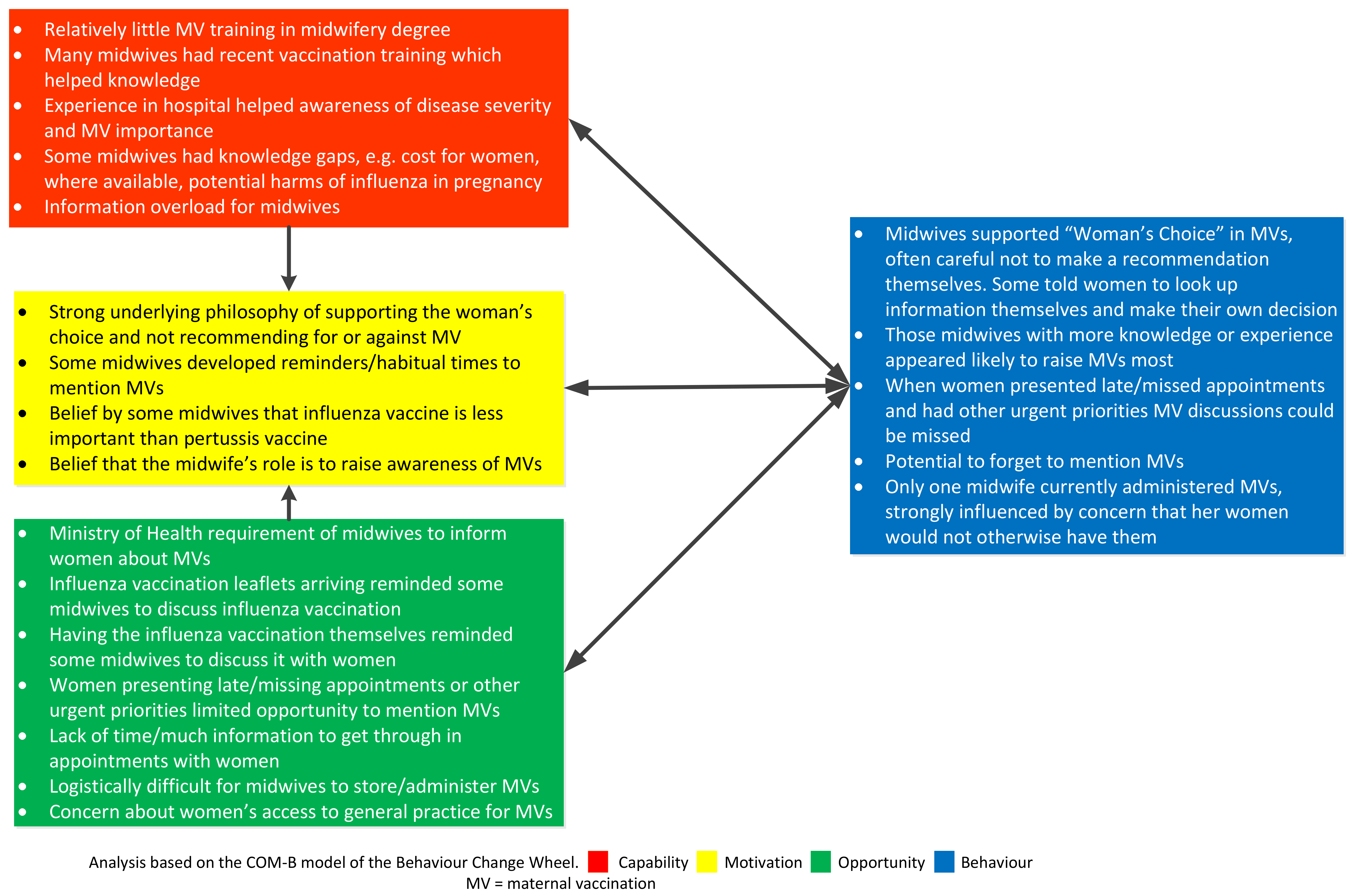
3.2. Capability Opportunity Motivation-Behaviour (COM-B)
3.2.1. Women’s Behaviour with Respect to Maternal Vaccinations
“If I could have just gotten it done [at the pharmacy or hospital] all then and there it would have been fine. You don’t have to think about it, you don’t have to go anywhere. It’s done.”W10
3.2.2. Capability for Women
“…all through my pregnancy of course my midwife recommended… all the shots…”W8 (influenza vaccine only)
“I feel like I’ve had to seek all the information out… I think my first midwife was maybe a bit anti-vaccinations, I got that vibe from her… I think I got a hand-out about whooping cough. And then the second time round… my midwife hasn’t mentioned it at all I don’t think. Then I went to the pharmacy for something else, and the pharmacist just popped her head over and she’s like oh are you pregnant?... [R]eminded me that I needed to get the whooping cough the second time round, coz I actually didn’t know...”W11 (pertussis vaccine only)
“I don’t think I trust much on Facebook myself. I’d be more inclined to probably book an appointment with the doctor or something and ask all those questions.”W1 (neither MV)
“…we can only do so much because immunisations [are] only a small part of our discussions and a lot of women aren’t focused on immunisations when they’re so scared of the… birth.”M2
“… if… my midwife or someone told me I need to be vaccinated against influenza then I would have done it.”W18
3.2.3. Capability for Health Care Professionals
“I forget about these vaccines always. And I go to nurses and they know, and I can’t hold all, so much information…”D2
“… the biggest barrier for a lot of midwives is that you don’t know and… you don’t want to talk about things when you don’t know…”M3
“… even midwives don’t understand [how bad influenza in pregnancy can be] because we don’t see it.”M11
“[Women] have this misconception of when I get the flu vaccine I get the flu... I don’t really know how to kind of demystify that…”M2
“I told my midwife [I’d had the vaccination]… she had heard about it but doesn’t actually know much about it…”W4 (pertussis only)
3.2.4. Opportunity for Women and for Health Professionals
“… because we’ve got the vaccines on site it’s just so much easier and the women go ‘yup, let’s do it.’ I do it at the beginning of our appointment so by the time we’ve finished… they’ve had their observations and they like it like that.”M1
“… more pressing issues like, I don’t know, the grocery shopping or getting all my five kids ready for school and you know it’s things that are like more in the forefront of their mind rather than this vaccination that they should probably think about getting.”M3
“I complain sometimes about my ladies not coming here but sometimes the pregnancy is the smallest issue in their life… Some of it is drugs and alcohol and priorities being askew.”M5
3.2.5. Motivation for Women and for Health Professionals
“… at first [on administering MVs] it was like I did sort of hesitate a little bit… It’s actually knowing that these women are being vaccinated on time and helping to protect the babies, that’s made me realise now that it’s actually an important part of the role.”M1
“I still feel that females were made to do it [carry a baby] I suppose.”W1 (received neither MV)
“I’ve turned so many around when I’ve said, “oh actually it’s recommended” and I show them the posters… and they go ‘oh okay that’s fine because my midwife has suggested it but I’m still a bit…”P10
“I quite like being vaccinated, especially during pregnancy and for baby after baby’s born. I find it most important that my babies are vaccinated when they should be.”W12 (planning to have both MVs)
“I got little text reminders on my phone from the doctors to remind me when my appointment was due to go and get them [MVs] done too, [handy] [e]specially when you’ve got so many children and after one you start losing track.”W12 (planning to have both MVs)
“I usually say Ministry of Health recommends because I don’t want it to be like I’m pushing this on you because I’m not, it’s up to you to make that choice.”M3
“… we’re really passionate about giving choices and options so on some topics that’s really hard… you want to give them the information, but you can’t be too directive.”M6
“… the chance is we might forget about the immunisation because there’s a lot to discuss on the [antenatal appointment] with the excitement and we have 15 min.”D2
“… when you start giving 14 vaccines a day you… get confidence in it and you begin to realise that it is safe.”M4
4. Discussion
4.1. Summary of Findings
4.2. Comparison with Other Literature and Implications
4.3. Strengths and Weaknesses
4.4. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abu-Raya, B.; Edwards, K.M. Optimizing the Timing of Vaccine Administration During Pregnancy. JAMA 2019, 321, 935–936. [Google Scholar] [CrossRef]
- Pertussis vaccines: WHO position paper—September 2015. Wkly Epidemiol. Rec. 2015, 90, 433–458.
- Gopal, D.P.; Barber, J.; Toeg, D. Pertussis (whooping cough). BMJ 2019, 364, 1401. [Google Scholar] [CrossRef] [Green Version]
- Macdonald-Laurs, E.; Ganeshalingham, A.; Lillie, J.; McSharry, B.; Segedin, E.R.; Best, E.; Pillai, A.; Harnden, A.; Gilchrist, C.A.; Grant, C.C. Increasing incidence of life-threatening pertussis: A retrospective cohort study in New Zealand. Pediatr. Infect. Dis. J. 2017, 36, 282–289. [Google Scholar] [CrossRef]
- Amirthalingam, G.; Andrews, N.; Campbell, H.; Ribeiro, S.; Kara, E.; Donegan, K.; Fry, N.K.; Miller, E.; Ramsay, M. Effectiveness of maternal pertussis vaccination in England: An observational study. Lancet 2014, 384, 1521–1528. [Google Scholar] [CrossRef]
- Amirthalingam, G. Strategies to control pertussis in infants. Arch. Dis. Child. 2013, 98, 552–555. [Google Scholar] [CrossRef]
- Prasad, N.; Sue Huang, Q.; Wood, T.; Aminisani, N.; McArthur, C.; Baker, M.G.; Seeds, R.; Thompson, M.G.; Widdowson, M.A.; Claire Newbern, E. Influenza-associated outcomes among pregnant, postpartum, and nonpregnant women of reproductive age. J. Infect. Dis. 2019, 219, 1893–1903. [Google Scholar] [CrossRef]
- Rasmussen, S.A.; Jamieson, D.J.; Uyeki, T.M. Effects of influenza on pregnant women and infants. Am. J. Obstet. Gynecol. 2012, 207, S3–S8. [Google Scholar] [CrossRef]
- Thompson, M.G.; Kwong, J.C.; Regan, A.K.; Katz, M.A.; Drews, S.J.; Azziz-Baumgartner, E.; Klein, N.P.; Chung, H.; Effler, P.V.; Feldman, B.S.; et al. Influenza vaccine effectiveness in preventing influenza-associated hospitalizations during pregnancy: A multi-country retrospective test negative design study, 2010–2016. Clin. Infect. Dis. 2019, 68, 1444–1453. [Google Scholar] [CrossRef] [Green Version]
- Nunes, M.C.; Madhi, S.A. Influenza vaccination during pregnancy for prevention of influenza confirmed illness in the infants: A systematic review and meta-analysis. Hum. Vaccines Immunother. 2018, 14, 758–766. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. Pertussis vaccination programme for pregnant women update: Vaccine coverage in England, April to September 2019. Health Prot. Rep. 2019, 12, 1–9. [Google Scholar]
- Psarris, A.; Sindos, M.; Theodora, M.; Antsaklis, P.; Pergialiotis, V.; Loutradis, D.; Daskalakis, G. Routine immunizations during pregnancy, doctors’ compliance and patient hesitancy: A two stage study on vaccination uptake. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 243, 36–40. [Google Scholar] [CrossRef]
- Descamps, A.; Launay, O.; Bonnet, C.; Blondel, B. Seasonal influenza vaccine uptake and vaccine refusal among pregnant women in France: Results from a national survey. Hum. Vaccines Immunother. 2019, 16, 1093–1100. [Google Scholar] [CrossRef]
- Yuen, C.Y.; Tarrant, M. Determinants of uptake of influenza vaccination among pregnant women—A systematic review. Vaccine 2014, 32, 4602–4613. [Google Scholar] [CrossRef]
- Byrne, L.; Ward, C.; White, J.M.; Amirthalingam, G.; Edelstein, M. Predictors of coverage of the national maternal pertussis and infant rotavirus vaccination programmes in England. Epidemiol. Infect. 2018, 146, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Howe, A.S.; Pointon, L.; Gauld, N.; Paynter, J.; Willing, E.; Turner, N. Pertussis and influenza immunisation coverage of pregnant women in New Zealand. Vaccine 2020, 38, 6766–6776. [Google Scholar] [CrossRef]
- Rowe, S.L.; Perrett, K.P.; Morey, R.; Stephens, N.; Cowie, B.C.; Nolan, T.M.; Leder, K.; Pitcher, H.; Sutton, B.; Cheng, A.C. Influenza and pertussis vaccination of women during pregnancy in Victoria, 2015–2017. Med. J. Aust. 2019, 210, 454–462. [Google Scholar] [CrossRef]
- Kriss, J.L.; Albert, A.P.; Carter, V.M.; Jiles, A.J.; Liang, J.L.; Mullen, J.; Rodriguez, L.; Howards, P.P.; Orenstein, W.A.; Omer, S.B.; et al. Disparities in Tdap Vaccination and Vaccine Information Needs Among Pregnant Women in the United States. Matern. Child Health J. 2019, 23, 201–211. [Google Scholar] [CrossRef]
- Gauld, N.J.; Braganza, C.S.; Babalola, O.O.; Huynh, T.T.; Hook, S.M. Reasons for use and non-use of the pertussis vaccine in pregnancy: An interview study in New Zealand women. J. Prim. Health Care 2016, 8, 344–350. [Google Scholar] [CrossRef]
- Mijović, H.; Greyson, D.; Gemmell, E.; Trottier, M.-È.; Vivion, M.; Graham, J.E.; Dubé, È.; Bettinger, J.A. Perinatal health care providers’ approaches to recommending and providing pertussis vaccination in pregnancy: A qualitative study. CMAJ Open 2020, 8, E377–E382. [Google Scholar] [CrossRef]
- Wilcox, C.R.; Calvert, A.; Metz, J.; Kilich, E.; MacLeod, R.; Beadon, K.; Heath, P.T.; Khalil, A.; Finn, A.; Snape, M.D.; et al. Determinants of influenza and pertussis vaccination uptake in pregnancy a multicenter questionnaire study of pregnant women and healthcare professionals. Pediatr. Infect. Dis. J. 2019, 38, 625–630. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, C.R.; Bottrell, K.; Paterson, P.; Schulz, W.S.; Vandrevala, T.; Larson, H.J.; Jones, C.E. Influenza and pertussis vaccination in pregnancy: Portrayal in online media articles and perceptions of pregnant women and healthcare professionals. Vaccine 2018, 36, 7625–7631. [Google Scholar] [CrossRef]
- Quattrocchi, A.; Mereckiene, J.; Fitzgerald, M.; Cotter, S. Determinants of influenza and pertussis vaccine uptake in pregnant women in Ireland: A cross-sectional survey in 2017/18 influenza season. Vaccine 2019, 37, 6390–6396. [Google Scholar] [CrossRef]
- Chang, Y.W.; Tsai, S.M.; Lin, P.C.; Chou, F.H. Willingness to receive influenza vaccination during pregnancy and associated factors among pregnant women in Taiwan. Public Health Nurs. 2019, 36, 284–295. [Google Scholar] [CrossRef]
- Strassberg, E.R.; Power, M.; Schulkin, J.; Stark, L.M.; Mackeen, A.D.; Murtough, K.L.; Paglia, M.J. Patient attitudes toward influenza and tetanus, diphtheria and acellular pertussis vaccination in pregnancy. Vaccine 2018, 36, 4548–4554. [Google Scholar] [CrossRef]
- Mohammed, H.; McMillan, M.; Roberts, C.T.; Marshall, H.S. A systematic review of interventions to improve uptake of pertussis vaccination in pregnancy. PLoS ONE 2019, 14, e0214538. [Google Scholar] [CrossRef]
- Wales, D.P.; Khan, S.; Suresh, D.; Ata, A.; Morris, B. Factors associated with Tdap vaccination receipt during pregnancy: A cross-sectional study. Public Health 2020, 179, 38–44. [Google Scholar] [CrossRef]
- Loubet, P.; Nguyen, C.; Burnet, E.; Launay, O. Influenza vaccination of pregnant women in Paris, France: Knowledge, attitudes and practices among midwives. PLoS ONE 2019, 14, e0215251. [Google Scholar] [CrossRef] [Green Version]
- Krishnaswamy, S.; Wallace, E.M.; Buttery, J.; Giles, M.L. A study comparing the practice of Australian maternity care providers in relation to maternal immunisation. Aust. N. Z. J. Obstet. Gynaecol. 2019, 59, 408–415. [Google Scholar] [CrossRef]
- Kaufman, J.; Attwell, K.; Hauck, Y.; Omer, S.B.; Danchin, M. Vaccine discussions in pregnancy: Interviews with midwives to inform design of an intervention to promote uptake of maternal and childhood vaccines. Hum. Vaccines Immunother. 2019, 15, 2534–2543. [Google Scholar] [CrossRef]
- Vishram, B.; Letley, L.; Jan Van Hoek, A.; Silverton, L.; Donovan, H.; Adams, C.; Green, D.; Edwards, A.; Yarwood, J.; Bedford, H.; et al. Vaccination in pregnancy: Attitudes of nurses, midwives and health visitors in England. Hum. Vaccines Immunother. 2018, 14, 179–188. [Google Scholar] [CrossRef]
- Vilca, L.M.; Martínez, C.; Burballa, M.; Campins, M. Maternal Care Providers’ Barriers Regarding Influenza and Pertussis Vaccination During Pregnancy in Catalonia, Spain. Matern. Child Health J. 2018, 22, 1016–1024. [Google Scholar] [CrossRef]
- Dubé, E.; Gagnon, D.; Kaminsky, K.; Green, C.R.; Ouakki, M.; Bettinger, J.A.; Brousseau, N.; Castillo, E.; Crowcroft, N.S.; Driedger, S.M.; et al. Vaccination Against Influenza in Pregnancy: A Survey of Canadian Maternity Care Providers. J. Obstet. Gynaecol. Can. 2019, 41, 479–488. [Google Scholar] [CrossRef]
- Hill, L.; Burrell, B.; Walls, T. Factors influencing women’s decisions about having the pertussis-containing vaccine during pregnancy. J. Prim. Health Care 2018, 10, 62–67. [Google Scholar] [CrossRef]
- Howe, A.S.; Gauld, N.J.; Cavadino, A.Y.; Petousis-Harris, H.; Dumble, F.; Sinclair, O.; Grant, C.C. Increasing uptake of maternal pertussis vaccinations through funded administration in community pharmacies. Vaccines 2022, 10, 150. [Google Scholar] [CrossRef]
- Frawley, J.E.; McKenzie, K.; Sinclair, L.; Cummins, A.; Wardle, J.; Hall, H. Midwives’ knowledge, attitudes and confidence in discussing maternal and childhood immunisation with parents: A national study. Vaccine 2020, 38, 366–371. [Google Scholar] [CrossRef]
- Frawley, J.E.; McKenzie, K.; Cummins, A.; Sinclair, L.; Wardle, J.; Hall, H. Midwives’ role in the provision of maternal and childhood immunisation information. Women Birth 2020, 33, 145–152. [Google Scholar] [CrossRef]
- Böhm, S.; Röbl-Mathieu, M.; Scheele, B.; Wojcinski, M.; Wichmann, O.; Hellenbrand, W. Influenza and pertussis vaccination during pregnancy—Attitudes, practices and barriers in gynaecological practices in Germany. BMC Health Serv. Res. 2019, 19, 616. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.; Paterson, P.; Larson, H.J. Strategies to improve maternal vaccination acceptance. BMC Public Health 2019, 19, 342. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Garbutt, J.M.; Dodd, S.; Walling, E.; Lee, A.A.; Kulka, K.; Lobb, R. Theory-based development of an implementation intervention to increase HPV vaccination in pediatric primary care practices. Implement. Sci. 2018, 13, 45. [Google Scholar] [CrossRef]
- Williams, L.; Gallant, A.J.; Rasmussen, S.; Brown Nicholls, L.A.; Cogan, N.; Deakin, K.; Young, D.; Flowers, P. Towards intervention development to increase the uptake of COVID-19 vaccination among those at high risk: Outlining evidence-based and theoretically informed future intervention content. Br. J. Health Psychol. 2020, 25, 1039–1054. [Google Scholar] [CrossRef]
- Gallant, A.J.; Flowers, P.; Deakin, K.; Cogan, N.; Rasmussen, S.; Young, D.; Williams, L. Barriers and enablers to influenza vaccination uptake in adults with chronic respiratory conditions: Applying the behaviour change wheel to specify multi-levelled tailored intervention content. medRxiv 2020. [Google Scholar] [CrossRef]
- Statistics New Zealand. Summary Figures. Available online: https://www.stats.govt.nz/topics/population (accessed on 5 April 2021).
- Statistics New Zealand. 2018 Census—NZ Stat Tables. Available online: https://www.stats.govt.nz/tools/2018-census-place-summaries/new-zealand (accessed on 5 April 2021).
- Waikato District Health Board. Snapshot of Waikato DHB. Available online: https://www.waikatodhb.health.nz/about-us/snapshot-of-waikato-dhb/#:~:text=Waikato%20DHB%20serves%20a%20population,to%20Waihi%20on%20the%20east (accessed on 13 November 2020).
- Waikato District Health Board. Waikato Health System Plan, Te Korowai Wairoa. 2019. Available online: https://waikatodhb.cwp.govt.nz/assets/Docs/About-Us/Key-Publications/Plans/7bf3d1e7ca/Waikato-Health-System-Plan-Te-Korowai-Waiora.pdf (accessed on 26 December 2019).
- The Immunisation Advisory Centre. Influenza Information for Health Professionals: Influenza and Pregnancy. Available online: https://www.influenza.org.nz/influenza-and-pregnancy (accessed on 23 December 2019).
- Best Practice Advocacy Centre New Zealand. News Update: Pertussis vaccine now subsidised for all pregnant women. Best Pract. J. 2015, 60, 46–47. [Google Scholar]
- Gauld, N.; Johnstone, E.; McMichael, I.; Braund, R. Pharmacists’ views and desires regarding pharmacist administration of vaccines in New Zealand. Int. J. Pharm. Pract. 2020, 29, 126–133. [Google Scholar] [CrossRef]
- Gauld, N.; Martin, S.; Sinclair, O.; Petousis-Harris, H.; Dumble, F.; Grant, C.C. A qualitative study of views and experiences of women and health care professionals about free maternal vaccinations administered at community pharmacies. Vaccines 2020, 8, 152. [Google Scholar] [CrossRef] [Green Version]
- Patton, M.Q. Qualitative Research and Evaluation Methods, 3rd ed.; Sage Publications: London, UK, 2002. [Google Scholar]
- O’Shea, A.; Cleary, B.; McEntee, E.; Barrett, T.; O’Carroll, A.; Drew, R.; O’Reilly, F. To vaccinate or not to vaccinate? Women’s perception of vaccination in pregnancy: A qualitative study. BJGP Open 2018, 2, bjgpopen18X101457. [Google Scholar] [CrossRef]
- Maisa, A.; Milligan, S.; Quinn, A.; Boulter, D.; Johnston, J.; Treanor, C.; Bradley, D.T. Vaccination against pertussis and influenza in pregnancy: A qualitative study of barriers and facilitators. Public Health 2018, 162, 111–117. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Māori or Pacific Women n = 10 | Women Who Identified with Neither Māori nor Pacific Ethnicity n = 8 |
|---|---|---|
| Identified ethnicity | 9 Māori and 1 Cook Island Māori. | 4 NZ European; 3 South African European; 1 Chinese (born in China). |
| Rural/urban | 6/4. | 2/6. |
| Age | 18–31 years. | 23–37 years. |
| Number ≤ 25 years | 5 | 1 |
| Number of weeks’ gestation or age of infant when interviewed | 1 was 22 weeks’ gestation and 4 were 31–39 weeks’ gestation. 5 had infants aged 5 weeks to 4 months old. | 3 women were 34–36 weeks’ gestation. 4 had infants 1 week to 4.5 months old; 1 had a 12-month-old infant. |
| Number of children | 2 women had no other children, 3 had 1 other child, 1 had 2 other children, 1 had 3 other children, and 3 had 4 other children. | 3 women had no other children; 4 had 1 other child, and 1 had 2 other children. |
| Lead maternity carer | All used a midwife. | All used a midwife. |
| First presentation to their midwife | 5 women first saw their midwife at 4–7 weeks’ gestation; 2 at 12–15 weeks, and 3 at 25–27 weeks. | All women first presented to the midwife at 4–10 weeks’ gestation. |
| Received no MVs | 2 | 1 |
| Received both MVs (or planned to) | 4 * | 2 |
| Received pertussis vaccine only | 4 | 4 |
| Received influenza vaccine only | 0 | 1 |
| Location of MVs | Pharmacy: 3. General Practice: 4 *. Hospital: 1. | Pharmacy: 6. General practice: 1. Hospital: 0 |
| Variable | Community Pharmacists (n = 12) | Midwives (n = 11) | General Practice Staff (n = 12) |
|---|---|---|---|
| Staff mix | 10 (including 3 pharmacy owners) were trained vaccinators providing vaccinations. 2 were pharmacy owners in pharmacies that did not provide vaccinations, but 1 of these was a trained vaccinator and owned other pharmacies where vaccinations occurred. | 1 worked at a hospital, 10 worked as Lead Maternity Carers (LMCs), 3 of whom had recent or current hospital or district health board experience. | 4 general practitioners (2 practice owners), 7 practice nurses, 1 practice manager. |
| Rural/urban | 7/5. | 7/4. | 8/4. |
| Practice details | 6 worked in high needs areas, 2 were in higher socio-economic areas, the rest had a mixed socio-economic clientele. | 2 described their area served as high socio-economic, the rest were in low socioeconomic or mixed socio-economic areas. The Māori midwives tended to have mainly Māori clients. | All worked in practices with a large proportion of high deprivation, with mixed high and low deprivation, and/or high Māori patient load. 2 worked at a Māori healthcare provider. |
| Work hours | 11 worked full time and 1 worked part-time. | All worked full-time or close to it. A total of 2 worked around 60 h per week or more. | 7 were full-time, 4 part-time and 1 unknown. |
| Identified ethnicity | 6 NZ European, 3 Chinese/Asian), 1 Māori, 1 Fiji Indian, and 1 Middle Eastern. | 5 Māori or part Māori, 4 NZ European, 1 British, and 1 Asian. | 8 NZ European, 1 South Asian, 3 Māori or NZ European/Māori. |
| Experience | 4 had 1–4 years’ experience, 5 had 9–18 years’ experience, and 3 had 30–40 years’ experience. | 3 had 1–5 years’ experience, 4 had 7–15 years and 4 had 20–30 years’ experience. | 2 had 2–5 years’ experience, 4 had 9–16 years’ experience, and 6 had 25–31 years’ experience. |
| Gender | 8 female and 4 male. | All female. | All female. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gauld, N.; Martin, S.; Sinclair, O.; Petousis-Harris, H.; Dumble, F.; Grant, C.C. Influences on Pregnant Women’s and Health Care Professionals’ Behaviour Regarding Maternal Vaccinations: A Qualitative Interview Study. Vaccines 2022, 10, 76. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010076
Gauld N, Martin S, Sinclair O, Petousis-Harris H, Dumble F, Grant CC. Influences on Pregnant Women’s and Health Care Professionals’ Behaviour Regarding Maternal Vaccinations: A Qualitative Interview Study. Vaccines. 2022; 10(1):76. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010076
Chicago/Turabian StyleGauld, Natalie, Samuel Martin, Owen Sinclair, Helen Petousis-Harris, Felicity Dumble, and Cameron C. Grant. 2022. "Influences on Pregnant Women’s and Health Care Professionals’ Behaviour Regarding Maternal Vaccinations: A Qualitative Interview Study" Vaccines 10, no. 1: 76. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10010076