1. Introduction
In Italy the annual incidence rate of invasive meningococcal disease (IMD) declined from 0.6 per 100,000 in 2004 to 0.3 in 2007 [
1] remaining low until 2019 [
2]. This was mainly due to a decrease in meningococcal serogroup C (MenC) cases after the introduction of the MenC conjugate (MCC) vaccine, which was included in the 2005–2007 National Plan for Vaccine Prevention (PNPV) [
3]. The MCC vaccine was recommended to infants in the first year of life and to all individuals presenting splenic dysfunction or immunodeficiency [
3]. As a consequence, a significant impact on MenC disease in infants and children (aged 0 to 4 years) was observed. MenC disease decreased from 1.7 per 100,000 in 2004 to 0.5 per 100,000 in 2007 [
1] and was 0.17 per 100,000 in 2019 in the age group 0–4 years [
2].
In 2008, the MCC vaccine was recommended also to adolescents aged 11–18 years old within the 2012–2014 PNPV [
4]. In 2012, the tetravalent meningococcal serogroup ACWY conjugate (MenACWY) vaccine was introduced and in the 2017–2019 PNPV it was recommended for individuals (aged from 12 to 18 years) and not previously vaccinated and for children already immunized [
5].
Since their introduction in Italy, the vaccine coverage rate for MCC and MenACWY vaccines increased up to 2018: the vaccine coverage rate was highest in children aged 24–36 months for the MCC vaccine and in adolescents aged 16 years for the MenACWY vaccine [
6]. In 2019–2020, MCC vaccine coverage decreased while MenACWY vaccination rates tended to increase [
7].
The protective effect against the capsular polysaccharide C included in the MCC vaccine is associated with the decline in the number of MenC cases in the targeted age groups in different countries. In the United Kingdom (UK), the MCC vaccine introduction at the end of 1999 in children and young adults markedly reduced the incidence of MenC disease, in the first two years [
8]. Since then, other European countries, Canada and Australia, who also introduced the MCC vaccine, have reported a substantial decline in MenC disease incidence [
9,
10,
11].
Although many clinical studies showed high effectiveness and immune memory of different meningococcal conjugate vaccines, a waning of bactericidal antibodies following primary vaccination in young children was evidenced [
12,
13,
14]. For example, two studies in the United Kingdom reported a decrease of SBA titers after 3 doses of MCC vaccine during the first year of life and after a single dose at 1–3 years of age of MCC vaccine two years after vaccination [
15,
16].
Other studies have shown that protection against MenC disease provided by quadrivalent conjugate vaccines received in toddlers and children may decline over time [
17,
18,
19].
Since antibody persistence is important as a parameter to monitor protection against meningococcal disease, we conducted a study to assess serum bactericidal antibody (SBA) persistence against serogroup C polysaccharide in samples of children who received primary vaccination with MCC or MenACWY vaccines.
2. Methods
This study was conducted at the National Reference Laboratory (NRL) for IMD at Istituto Superiore di Sanità (ISS) in collaboration with three centers: St. Orsola-Malpighi Polyclinic, in Bologna, Molinette Hospital, in Turin and Central Tuscany Local Health Authority, in Florence. The protocol including recruitment and serum sampling of MenC vaccinated individuals, was drawn up by the NRL. The enrolment of participating was from February 2016 to December 2017. Serum samples were collected from healthy children who belonged to birth cohort from 2004 to 2016 and who had received the primary MenC vaccination, with the MCC or MenACYW vaccine. These children were recruited after the approval of all parents who responded to the letter sent to them. All participants were divided into two groups: children who received the MCC vaccine (MCC-CRM197), one or three doses (3, 5 and >12 months), or children who received one dose of the MenACYW vaccine (MenACYW-TT and MenACYW-CRM197). An additional group enclosing children who received a booster dose with the MCC vaccine or MenACYW vaccine given 4 to 10 years after primary MCC vaccination (one or three doses of MCC vaccine) was analyzed separately to other groups of enrolled individuals. Exclusion criteria included immunosuppression and any acute or chronic infection.
Information on the date of birth, date of sample collection, and date of vaccination of the children was available. Written informed consent was obtained from parents or legally authorized representatives prior to the performance of any procedures.
All serum samples collected from each individual were sent to the NRL for IMD of the ISS and stored at −80 °C. Serum samples were taken from <1 year up to 5 years after vaccination, to determine the persistence of specific bactericidal antibody against serogroup C meningococcus.
2.1. Ethical Committee Approval
This study was approved by the ISS Ethical Committee and by the Local EC (ISS EC reference number PRE 926/15).
2.2. Serological Assay
A standardized SBA assay was performed according to the procedure described by Maslanka et al. [
20], using baby rabbit complement (rSBA), as the source of exogenous complement. The complement source was a pooled serum from 3 or 4-week-old–rabbits (Cederlaine Corporation, 4410 Paletta Court, Burlington, Ontario, Canada). Titers were expressed as the reciprocal serum dilutions yielding ≥ 50% killing after 60 min. The titer of ≥1:8 was the protective threshold, that has been established to be the correlated of protection for meningococcal serogroup C [
21]. The lower limit of detection was a titer of 4. Negative results were given a value of half the lowest level of detection. rSBA assays were performed against the serogroup C target strain C11 (C:16: P1.7-1,1). A positive control serum with an assigned serogroup C titer was included to quality control the assay.
2.3. Statistical Analysis
We described the main characteristics of the study sample using counts with percentages and range values. Based on date of birth, date of vaccination, and date of serum sampling we calculated the age at vaccination, the age at serum sampling, and the time interval from vaccination to serum sampling. We then estimated the proportion of children with a bactericidal antibody response (rSBA MenC titers ≥ 1:8), together with a 95% exact binomial confidence interval (CI), by age at serum sampling and different time intervals from serum sampling to vaccination, separately for each vaccine type (MCC and MenACYW). Changes in the proportion of children with bactericidal antibody response over the age at serum sampling and time from vaccination were evaluated through the chi-square test for linear trend.
Finally, separately for each vaccine type, we used a multivariable Poisson regression model with robust variance estimator to evaluate the association of bactericidal antibody response with age at vaccination and time from vaccination. The latter variables were included as continuous covariates in the model and the strength of the associations was described using adjusted prevalence proportion ratios (PPR) with 95% CI. All tests were two-sided and statistical significance was set at p < 0.05. The analyses were performed using Stata/SE version 16.1 (StataCorp LLC, Lakeway Dr, College Station, TX, USA).
3. Results
The study sample consisted of 348 enrolled participants, 272 of whom were included in the analysis. The exclusion from the analysis was due to serological data missing or to blood samples drawn before MenC immunization.
The age at the time of blood sampling of all investigated children ranged from 1 year to 12 years. These subjects were grouped based on the type of MenC vaccine administered: 203 (74.6%) had received MCC vaccine (one dose or three doses), 53 (19.5%) had received one dose of MenACYW vaccine and 16 children (5.9%) had received a booster dose with MCC or MenACYW vaccine.
The age at MCC vaccination was between 7 months and 23 months for the 93.1% (189/203) and only four children (2%; 4/203) were vaccinated at the age of 5–11 years (
Table 1). Children vaccinated with one dose of the MCC vaccine were the majority (94%; 191/203), while the remaining children received three doses (6%; 12/203).
The percentages of children in the MCC vaccine group with rSBA MenC titers ≥ 1:8 are presented in
Figure 1 according to the age at enrollment. The highest percentages with bactericidal titers resulted in children under two years of age (90.9%, 95% CI: 70.8–98.9%) and at two years of age (70.4%, 95% CI: 49.8–86.2%). Another high percentage of children with bactericidal titers was found in the age group 7 to 12 years at enrollment (88.9%, 95% CI: 51.8–99.7%), vaccinated at the median age of 5.0 years (from 2.1 to 5.5 years). While children aged 3, 4, 5 and 6 years at enrollment showed the lowest percentages of bactericidal titers: 50% (95% CI: 31.3–68.7%), 46.2% (95% CI: 26.6–66.7%), 25.5% (95% CI: 14.7–39.0%), and 23.5% (95% CI: 10.7–41.2%), respectively (
Figure 1). This decline (from 3 to 6 years of age at enrollment) was found to be statistically significant (chi-square for trend,
p = 0.006).
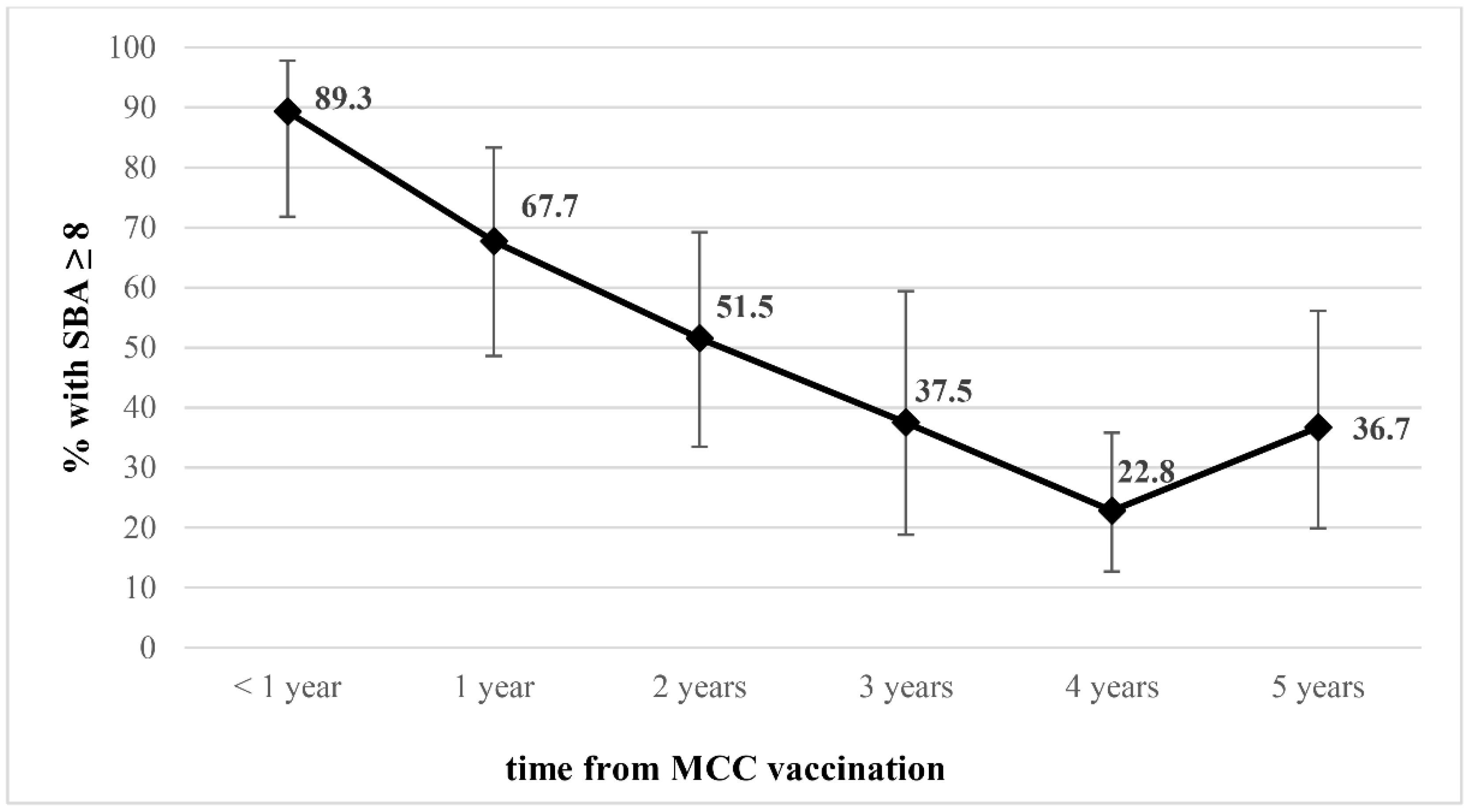
In order to assess bactericidal antibody persistence over time, we analyzed the serum samples according to time since MCC vaccination.
Figure 2 shows a decreasing trend of antibody levels of rSBA MenC titres ≥ 1:8 from 67.7% (95% CI: 48.6–83.3%) at one year after vaccination to 36.7% (95% CI: 19.9–56.1%) at five years after vaccination (chi-square for linear trend,
p < 0.001).
Selecting only children who have been vaccinated for more than four years with the MCC vaccine, the proportion with rSBA MenC titers ≥ 1:8 was higher in children vaccinated at more than 5 years old (75%) than in those who received the vaccine at under 2 years old (29.7%). This difference was not significant due to the little number of children immunized at >5 years old (data not shown).
As showed in
Table 1 the percentage of the children who received one dose of the MenACYW vaccine was 84.9%, between 1 to 2 years of age and only three children were vaccinated between 5 and 7 years. Among these subjects, the majority, showed a high percentage of rSBA MenC titers ≥ 1:8 (90.6%, 95% CI: 79.3–96.9%) after a mean time of 7 months (range 1 month–17 months).
We finally evaluated the percentage of rSBA MenC titers ≥ 1:8 in a small group (n = 16) of children who received a booster dose of MCC or MenACYW vaccine 4 to 10 years after primary MCC vaccination, performed at one year. All the children showed rSBA MenC titers ≥1:256 in a mean time of 4 months (range 1 month–13 months) after the booster dose (data not shown).
According to results from the multivariable Poisson regression analysis model presented in
Table 2, independently of the age at vaccination, the proportion of children vaccinated with the MCC vaccine with a bactericidal antibody response (rSBA titers ≥1:8) significantly decreased by 23% for every 1-year increase in time from vaccination (Adjusted PR = 0.77, 95% CI:0.71–0.84). Conversely, independently of the time since vaccination, it significantly increased by 10% for every 1-year unit increase in age at vaccination (Adjusted PR = 1.10, 95% CI: 1.01–1.20). No statistically significant trends were observed among children vaccinated with the MenACYW vaccine.
4. Discussion
Meningococcal disease is still a devastating threat characterized by high fatality rates due to the rapid progression of the disease [
22]. An important advance against this public health problem was the development and introduction of polysaccharide-protein conjugate vaccines. In particular, the introduction of the monovalent serogroup C meningococcal conjugate vaccine had great success in the direct protection against meningococcal disease [
23].
It is known that protection against meningococcal disease is mediated by the presence of serum bactericidal antibodies induced by meningococcal polysaccharide protein conjugates vaccines [
24]. The capsule polysaccharide is the major virulence determinant that allows the meningococcus to survive in the blood and in the intracellular environment [
25]. In addition, meningococcal capsule polysaccharide can interfere with the complement activation of both classical and alternative pathways [
26]. The complement system has an important role in protection against meningococcal disease, evidenced by the increased susceptibility of individuals with known terminal complement deficiencies [
27].
The rSBA assay was used in this study to measure the levels of the bactericidal antibodies for MenC in a sample of children who received primary vaccination with the MCC and MenACWY vaccine.
At the time of our study, meningococcal vaccination against serogroup C was recommended for all children aged 13–15 months with a single dose of MCC or MenACWY vaccine [
28]. Consequently, mostly of the children enrolled in this study received a single dose of the MCC vaccine between 7 and 23 months of age. As expected, the high proportion of samples with a rSBA value ≥ 1:8 was found among children under two years of age at the time of sampling, followed by children aged between 7 and 12 years. Thus was probably due to the age of immunization because these older children received a single dose of the MenC vaccine at a median age of 5 years. Previous data underlined how the SBA protective titers against serogroup C meningococci, after the MCC vaccine, increase with increasing age at the time of vaccination [
29].
Considering that the majority of children in this study were vaccinated at one or two years of age and that they belonged to different birth cohorts (from 2004 to 2016), we analyzed the serum samples in relation to the time of vaccination. We found that bactericidal antibodies declined over time from 89.3% at one year, to 36.7% 5 years after MCC vaccination. This percentage is consistent with previous studies that demonstrated marked waning in rSBA MenC titers at 2 and 4 years after MCC immunization of children at a younger age [
16,
30].
Long-term protection after a single dose of the MenACWY vaccine has been evidenced in children and adolescents and revealed the serogroup-specific decline in titers, from 2 years up to 10 years [
31,
32,
33,
34]. In this study, the high proportion of protective rSBA MenC titers was found in a group of children immunized with the MenACYW vaccine, approximately at a mean time of 7 months after vaccination. This result is in line with what was reported in a previous study in which most children showed a rSBA MenC ≥1:128 after 1-month post-vaccination with the MenACYW vaccine [
35].
The evaluation of the persistence of bactericidal antibodies in the serum, it is important not only because is associated with protection but also to provide evidence for vaccination programs and to determine the need of booster dose, required after primary vaccination [
19]. The immune response to booster dose with MenACWY vaccine has been evaluated in toddlers, children, and adolescents as already reported [
23].
Here, it was evaluated the presence of rSBA titers against serogroup C in a small group of children who received a MenACWY booster dose from 4 to 10 years after primary vaccination with MCC. This group showed a robust response due to the key role of the immunological memory [
31].
In conclusion, our findings provide additional evidences on the presence of bactericidal antibodies after MCC or MenACWY vaccination. As already known, meningococcal bactericidal antibodies against serogroup C were observed to decline over time after infant and child MenC immunization. A significant proportion of children, vaccinated at 1–2 years showed low bactericidal antibody levels five years after MenC immunization. The impact of MenC disease on different age groups should be closely monitored to evaluate whether it is necessary to recommend booster doses of the meningococcal conjugate vaccine to maintain elevated bactericidal antibody levels.
Author Contributions
Conceptualization and supervision, P.S.; writing—original draft, A.N. and P.S.; methodology, A.N.; investigation, A.N., C.F., A.C., A.P., P.V. and L.A.; formal analysis, M.F.; investigation and resources, A.M.B., C.V. and A.M.; writing—review and editing, P.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Italian Ministry of Health-CCM Project Fasc. ISS: 1S04 “Studio di ceppi di meningococco circolanti in Italia e valutazione della copertura offerta dai vaccini”, from 28 March 2016 to 27 March 2017.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Istituto Superiore di Sanità, Ethical Committee and by the Local EC (ISS EC reference number PRE 926/15).
Informed Consent Statement
Written Informed consent was obtained from all subjects involved in the study to finalize the project.
Acknowledgments
The authors want to thank Stefania Iannazzo, Organizational Medical Direction, Regional Health Emergency Agency 118, Rome, Italy. We thank the children and their parents, as well as nurses and laboratory technicians who were involved in this study. We thank Raffaella Cipriani, Microbiology and Virology Laboratory, Città della Salute e della Scienza Hospital, Torino, Italy for the collection and shipping the sera. We also thank Giovanna Mereu, Central Tuscany Health Authority, Florence, Italy for her contribution as regional health authority.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Stefanelli, P.; Fazio, C.; Sofia, T.; Neri, A.; Mastrantonio, P. Serogroup C meningococci in Italy in the era of conjugate menC vaccination. BMC Infect. Dis. 2009, 9, 135. [Google Scholar] [CrossRef] [PubMed]
- Istituto Superiore Di Sanità. ISS Surveillance Data on Invasive Bacterial Diseases, Consolidated Report 2019. Available online: https://www.iss.it/-/rapporto-consolidato-mib-2019 (accessed on 20 April 2022).
- PNPV 2005–2007. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_543_allegato.pdf (accessed on 20 April 2022).
- PNPV 2012–2014. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_1721_allegato.pdf (accessed on 20 April 2022).
- PNPV 2017-2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 20 April 2022).
- Ministry of Health. Vaccine Coverage. Available online: https://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=20 (accessed on 20 April 2022).
- Sabbatucci, M.; Odone, A.; Signorelli, C.; Siddu, A.; Maraglino, F.; Rezza, G. Improved Temporal Trends of Vaccination Coverage Rates in Childhood after the Mandatory Vaccination Act, Italy 2014–2019. Vaccines 2022, 10, 2540. [Google Scholar] [CrossRef] [PubMed]
- Maiden, M.C.J.; Ibarz-Pavo´n, A.B.; Urwin, R.; Gray, S.J.; Andrews, N.J.; Clarke, S.C.; Walker, A.M.; Evans, M.R.; Kroll, J.S.; Neal, K.R.; et al. Impact of meningococcal serogroup C conjugate vaccines on carriage and herd immunity. J. Infect. Dis. 2008, 197, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Trotter, C.L.; Chandra, M.; Cano, R.; Larrauri, A.; Ramsay, M.E.; Brehony, C.; Jolley, K.A.; Maiden, M.C.; Heuberger, S.; Frosch, M. A surveillance network for meningococcal disease in Europe. FEMS Microbiol. Rev. 2007, 31, 27–36. [Google Scholar] [CrossRef]
- Bettinger, J.A.; Scheifele, D.W.; Saux, N.L.; Halperin, S.A.; Vaudry, W.; Tsang, R. The impact of childhood meningococcal serogroup C conjugate vaccine programs in Canada, Canadian Immunization Monitoring Program, Active (IMPACT). Pediatr. Infect. Dis. J. 2009, 28, 220–224. [Google Scholar] [CrossRef]
- Booy, R.; Jelfs, J.; El Bashir, H.; Nissen, M.D. Impact of meningococcal C conjugate vaccine use in Australia (Editorial). MJA 2007, 186, 108–109. [Google Scholar]
- Borrow, R.; Abad, R.; Trotter, C.; van der Klis, F.R.M.; Vazquez, J.A. Effectiveness of meningococcal serogroup C vaccine programmes. Vaccine 2013, 31, 4477–4486. [Google Scholar] [CrossRef]
- Goldblatt, D. Conjugate vaccines. Clin. Exp. Immunol. 2000, 119, 1–3. [Google Scholar] [CrossRef]
- Richmond, P.; Borrow, R.; Goldblatt, D.; Findlow, J.; Martin, S.; Morris, R.; Cartwright, K.; Miller, E. Ability of 3 different meningococcal C conjugate vaccines to induce immunologic memory after a single dose in UK toddlers. J. Infect. Dis. 2001, 183, 160–163. [Google Scholar] [CrossRef]
- Southern, J.; Crowley-Luke, A.; Borrow, R.; Andrews, N.; Miller, E. Immunogenicity of one, two or three doses of a meningococcal C conjugate vaccine conjugated to tetanus toxoid, given as a three-dose primary vaccination course in UK infants at 2, 3 and 4 months of age with acellular pertussis-containing DTP/Hib vaccine. Vaccine 2006, 24, 215–219. [Google Scholar] [CrossRef]
- Snape, M.D.; Kelly, D.F.; Green, B.; Moxon, E.R.; Borrow, R.; Pollard, A.J. Lack of serum bactericidal activity in preschool children two years after a single dose of serogroup C meningococcal polysaccharide-protein conjugate vaccine. Pediatr. Infect. Dis. J. 2005, 24, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Cohn, A.C.; MacNeil, J.R.; Harrison, L.H.; Lynfield, R.; Reingold, A.; Schaffner, W.; Zell, E.R.; Plikaytis, B.; Wang, X.; Messonnier, N.E. Active Bacterial Core Surveillance (ABCs) Team and MeningNet Surveillance Partners. Effectiveness and Duration of Protection of One Dose of a Meningococcal Conjugate Vaccine. Pediatrics 2017, 139, e20162193. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R.; Keshavan, P.; Welsch J., A.; Han, L.; Smolenov, I. Persistence of the immune response after MenACWY-CRM vaccination and response to a booster dose, in adolescents, children and infants. Hum. Vaccin. Immunother. 2016, 12, 1300–1310. [Google Scholar] [CrossRef] [PubMed]
- Vesikari, T.; Borrow, R.; Forsten, A.; Findlow, I.; Dhingra, M.S.; Jordanov, E. Immunogenicity and safety of a quadrivalent meningococcal tetanus toxoid-conjugate vaccine (MenACYW-TT) in healthy toddlers: A Phase II randomized study. Hum. Vaccin. Immunother. 2020, 16, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Maslanka, S.E.; Gheesling, D.E.; LiButti, K.; Donaldson, B.J.; Harakeh, H.S.; Dykes, J.K.; Arhin, F.F.; Devi, S.J.N.; Frasch, C.E.; Huang, J.C.; et al. Standardization and a multi-laboratory comparison of Neisseria meningitidis serogroup A and C serum bactericidal assays. Clin. Diagn. Lab. Immunol. 1997, 4, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Borrow, R.; Balmer, P.; Miller, E. Meningococcal surrogates of protection--serum bactericidal antibody activity. Vaccine 2005, 23, 2222–2227. [Google Scholar] [CrossRef]
- Jafri, R.Z.; Ali, A.; Messonnier, N.E.; Tevi-Benissan, C.; Durrheim, D.; Eskola, J.; Fermon, F.; Klugman, K.P.; Ramsay, M.; Sow, S.; et al. Global epidemiology of invasive meningococcal disease. Popul. Health Metr. 2013, 11, 17. [Google Scholar] [CrossRef]
- Trotter, C.L.; Maiden, M.C. Meningococcal vaccines and herd immunity: Lessons learned from serogroup C conjugate vaccination programs. Expert Rev. Vaccines 2009, 8, 851–861. [Google Scholar] [CrossRef]
- Frasch, C.E.; Borrow, R.; Donnelly, J. Bactericidal antibody is the immunologic surrogate of protection against meningococcal disease. Vaccine 2009, 27 (Suppl. 2), B112–B116. [Google Scholar] [CrossRef]
- Spinosa, M.R.; Progida, C.; Talà, A.; Cogli, L.; Alifano, P.; Bucci, C. The Neisseria meningitidis capsule is important for intracellular survival in human cells. Infect. Immun. 2007, 75, 3594–3603. [Google Scholar] [CrossRef]
- Lewis, L.A.; Ram, S. Meningococcal disease and the complement system. Virulence 2014, 5, 98–126. [Google Scholar] [CrossRef] [PubMed]
- Emonts, M.; Hazelzet, J.A.; de Groot, R.; Hermans, P.W. Host genetic determinants of Neisseria meningitidis infections. Lancet Infect. Dis. 2003, 3, 565–577. [Google Scholar] [CrossRef]
- Presa, J.; Findlow, J.; Vojicic, J.; Williams, S.; Serra, L. Epidemiologic Trends, Global Shifts in Meningococcal Vaccination Guidelines, and Data Supporting the Use of MenACWY-TT Vaccine: A Review. Infect. Dis. Ther. 2019, 8, 307–333. [Google Scholar] [CrossRef] [PubMed]
- Sakou, I.I.; Tzanakaki, G.; Tsolia, M.N.; Sioumala, M.; Barbouni, A.; Kyprianou, M.; Papaevangelou, V.; Tsitsika, A.; Blackwell, C.C.; Kafetzis, D.; et al. Investigation of serum bactericidal activity in childhood and adolescence 3-6 years after vaccination with a single dose of serogroup C meningococcal conjugate vaccine. Vaccine 2009, 27, 4408–4411. [Google Scholar] [CrossRef] [PubMed]
- Borrow, R.; Goldblatt, D.; Andrews, N.; Southern, J.; Ashton, L.; Deane, S.; Morris, R.; Cartwright, K.; Miller, E. Antibody persistence and immunological memory at age 4 years after meningococcal group C conjugate vaccination in children in the United Kingdom. J. Infect. Dis. 2002, 186, 1353–1357. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R.; Reisinger, K.; Block, S.L.; Percell, S.; Odrljin, T.; Dull, P.M.; Smolenov, I. Antibody persistence after primary and booster doses of a quadrivalent meningococcal conjugate vaccine in adolescents. Pediatr. Infect. Dis. J. 2014, 33, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Block, S.L.; Christensen, S.; Verma, B.; Xie, F.; Keshavan, P.; Dull, P.M.; Smolenov, I. Antibody persistence 5 years after vaccination at 2 to 10 years of age with Quadrivalent MenACWY-CRM conjugate vaccine, and responses to a booster vaccination. Vaccine 2015, 33, 2175–2182. [Google Scholar] [CrossRef]
- Vesikari, T.; Forsten, A.; Bianco, V.; Van der Wielen, M.; Miller, J.M. Antibody persistence up to 5 years after vaccination of toddlers and children between 12 months and 10 years of age with a quadrivalent meningococcal ACWY-tetanus toxoid conjugate vaccine. Hum. Vaccin. Immunother. 2016, 12, 132–139. [Google Scholar] [CrossRef]
- Knuf, M.; Romain, O.; Kindler, K.; Walther, U.; Tran, P.M.; Pankow-Culot, H.; Fischbach, T.; Kieninger-Baum, D.; Bianco, V.; Baine, Y.; et al. Immunogenicity and safety of the quadrivalent meningococcal serogroups A, C, W-135 and Y tetanus toxoid conjugate vaccine (MenACWY-TT) in 2–10-year-old children: Results of an open, randomised, controlled study. Eur. J. Pediatr. 2013, 172, 601–612. [Google Scholar] [CrossRef]
- Borrow, R.; Andrews, N.; Findlow, H.; Waight, P.; Southern, J.; Crowley-Luke, A.; Stapley, L.; England, A.; Findlow, J.; Miller, E. Kinetics of antibody persistence following administration of a combination meningococcal serogroup C and haemophilus influenzae type b conjugate vaccine in healthy infants in the United Kingdom primed with a monovalent meningococcal serogroup C vaccine. Clin. Vaccine Immunol. 2010, 17, 154–159. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 


{kind=link}
{kind=link}