
Factors Associated with COVID-19 Vaccine Acceptance in Morocco: Applying the Health Belief Model

 , and
, and
Abstract
:1. Introduction
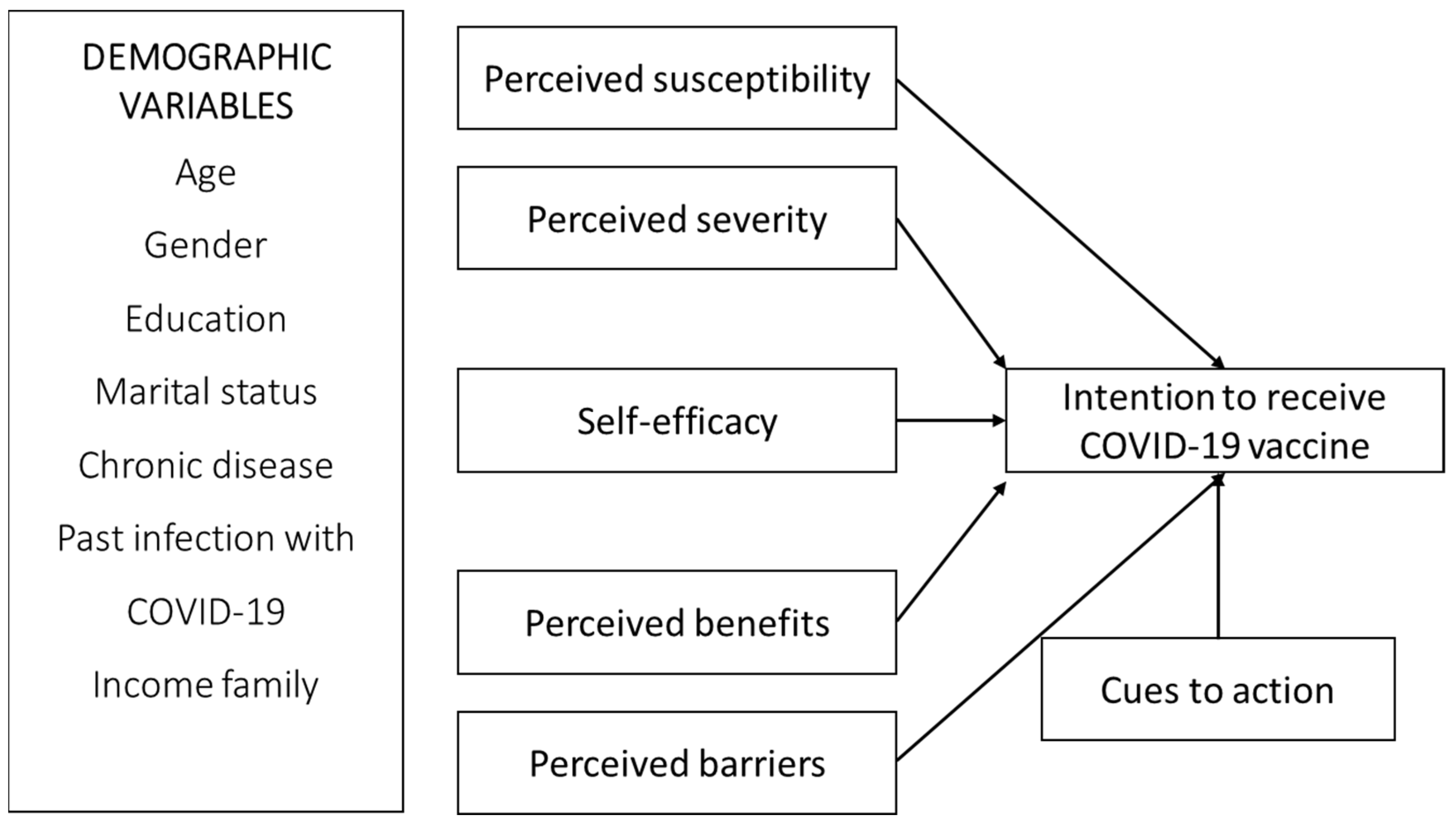
Theoretical Framework and Hypotheses Development
2. Methods
2.1. Study Design
2.2. Participants
2.3. Survey Content
2.4. Statistical Analysis
3. Results
3.1. Descriptive Information of the Sample
3.2. Sociodemographic Factors Associated with Acceptance of COVID-19 Vaccine
3.3. Statistics of Key Variables
3.4. Predictors of Intention to Vaccinate against COVID-19
3.4.1. Measurement Model
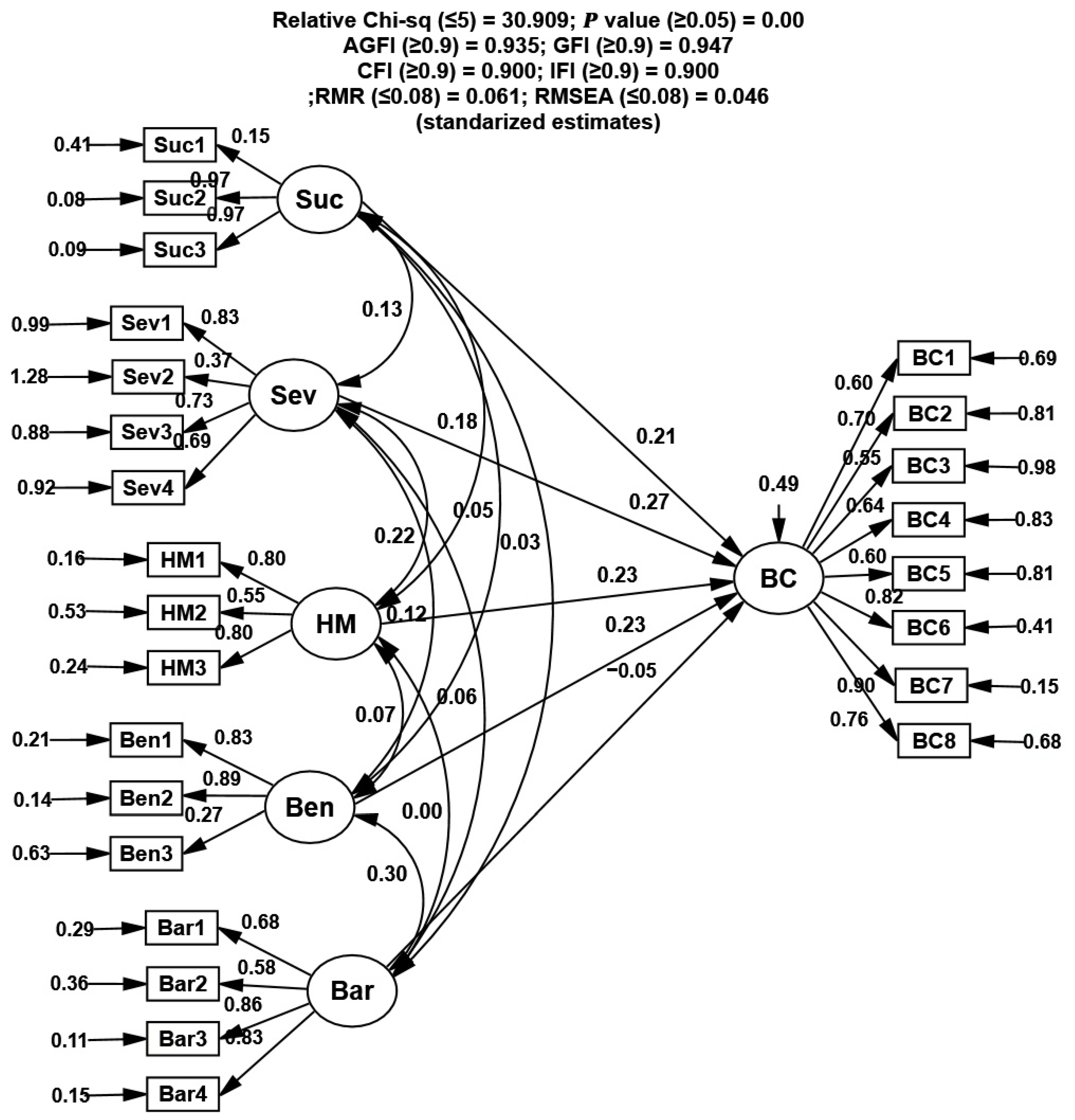
3.4.2. Structural Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Menouni, A.; Berni, I.; Abchouch, T.; Khouchoua, M.; Filali-Zegzouti, Y.; Janssen, P.; Kestemont, M.P.; Godderis, L.; El Jaafari, S. Mental Health among the Moroccan Population during SARS-CoV-2 Outbreak: MAROCOVID Study. J. Affect. Disord. 2022, 308, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Altmann, D.M.; Douek, D.C.; Boyton, R.J. What Policy Makers Need to Know about COVID-19 Protective Immunity. Lancet 2020, 395, 1527–1529. [Google Scholar] [CrossRef]
- World Health Organization COVID-19 Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 13 July 2021).
- Ministère de La Santé Campagne Nationale de Vaccination Contre Le Virus de La COVID-19. Available online: https://www.sante.gov.ma/Pages/actualites.aspx?IDActu=431 (accessed on 13 July 2021).
- Buglar, M.E.; White, K.M.; Robinson, N.G. The Role of Self-Efficacy in Dental Patients’ Brushing and Flossing: Testing an Extended Health Belief Model. Patient Educ. Couns. 2010, 78, 269–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.; Kim, S. Analysis of the Impact of Health Beliefs and Resource Factors on Preventive Behaviors against the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8666. [Google Scholar] [CrossRef]
- Gerend, M.A.; Shepherd, J.E. Predicting Human Papillomavirus Vaccine Uptake in Young Adult Women: Comparing the Health Belief Model and Theory of Planned Behavior. Ann. Behav. Med. 2012, 44, 171–180. [Google Scholar] [CrossRef] [Green Version]
- Jose, R.; Narendran, M.; Bindu, A.; Beevi, N.; Manju, L.; Benny, P.V. Public Perception and Preparedness for the Pandemic COVID 19: A Health Belief Model Approach. Clin. Epidemiol. Glob. Health 2021, 9, 41–46. [Google Scholar] [CrossRef]
- Santos, A.J.; Kislaya, I.; Machado, A.; Nunes, B. Beliefs and Attitudes towards the Influenza Vaccine in High-Risk Individuals. Epidemiol. Infect. 2017, 145, 1786–1796. [Google Scholar] [CrossRef] [Green Version]
- Champion, V.L.; Skinner, C.S. The Health Belief Model. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Brien, S.; Kwong, J.C.; Buckeridge, D.L. The determinants of 2009 pandemic A/H1N1 influenza vaccination: A systematic review. Vaccine 2012, 30, 1255–1264. [Google Scholar] [CrossRef]
- Weinstein, N.D. Testing Four Competing Theories of Health-Protective Behavior. Health Psychol 1993, 12, 324–333. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Bles, A.M.; Spiegelhalter, D.; Linden, S. Risk Perceptions of COVID-19 around the World. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Kreps, S.E.; Kriner, D.L. Factors Influencing COVID-19 Vaccine Acceptance across Subgroups in the United States: Evidence from a Conjoint Experiment. Vaccine 2021, 39, 3250–3258. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.; Liu, S. Integrating Health Behavior Theories to Predict American’s Intention to Receive a COVID-19 Vaccine. Patient Educ. Couns. 2021, 104, 1878–1886. [Google Scholar] [CrossRef] [PubMed]
- Hanson, J.A.; Benedict, J.A. Use of the Health Belief Model to Examine Older Adults’ Food-Handling Behaviors. J. Nutr. Educ. Behav. 2002, 34, 25–30. [Google Scholar] [CrossRef]
- Mukhtar, S. Mental Health and Emotional Impact of COVID-19: Applying Health Belief Model for Medical Staff to General Public of Pakistan. Brain Behav. Immun. 2020, 87, 28–29. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F.; et al. Acceptance of the COVID-19 Vaccine Based on the Health Belief Model: A Population-Based Survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef]
- Alhalaseh, L.; Fayoumi, H.; Khalil, B. The Health Belief Model in Predicting Healthcare Workers’ Intention for Influenza Vaccine Uptake in Jordan. Vaccine 2020, 38, 7372–7378. [Google Scholar] [CrossRef]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A Novel Coronavirus Outbreak of Global Health Concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Berni, I.; Menouni, A.; Ghazi El, I.; Duca, R.-C.; Kestemont, M.-P.; Godderis, L.; EL Jaafari, S. Understanding Farmers’ Safety Behavior Regarding Pesticide Use in Morocco. Sustain. Prod. Consum. 2021, 25, 471–483. [Google Scholar] [CrossRef]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How Will Country-Based Mitigation Measures Influence the Course of the COVID-19 Epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Rezaei, R.; Safa, L.; Damalas, C.A.; Ganjkhanloo, M.M. Drivers of Farmers’ Intention to Use Integrated Pest Management: Integrating Theory of Planned Behavior and Norm Activation Model. J. Environ. Manag. 2019, 236, 328–339. [Google Scholar] [CrossRef]
- Bagheri, A.; Bondori, A.; Allahyari, M.S.; Damalas, C.A. Modeling Farmers’ Intention to Use Pesticides: An Expanded Version of the Theory of Planned Behavior. J. Environ. Manag. 2019, 248, 109291. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Education Ltd.: Essex, UK, 2010; ISBN 978-1-292-02190-4. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Carico, R.; Sheppard, J.; Thomas, C.B. Ron. Res. Soc. Adm. Pharm. 2021, 17, 1984–1987. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 Vaccine Acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Qattan, A.M.N.; Alshareef, N.; Alsharqi, O.; Al Rahahleh, N.; Chirwa, G.C.; Al-Hanawi, M.K. Acceptability of a COVID-19 Vaccine Among Healthcare Workers in the Kingdom of Saudi Arabia. Front. Med. 2021, 8, 83. [Google Scholar] [CrossRef]
- Department of Health and Social Care. Available online: https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi/interim-advice-on-priority-groups-for-covid-19-vaccination (accessed on 13 May 2022).
- Sun, S.; Lin, D.; Operario, D. Interest in COVID-19 Vaccine Trials Participation among Young Adults in China: Willingness, Reasons for Hesitancy, and Demographic and Psychosocial Determinants. Prev. Med. Rep. 2021, 22, 101350. [Google Scholar] [CrossRef] [PubMed]
- Hawlader, M.D.H.; Rahman, M.L.; Nazir, A.; Ara, T.; Haque, M.M.A.; Saha, S.; Barsha, S.Y.; Hossian, M.; Matin, K.F.; Siddiquea, S.R.; et al. COVID-19 Vaccine Acceptance in South Asia: A Multi-Country Study. Int. J. Infect. Dis. 2022, 114, 1–10. [Google Scholar] [CrossRef]
- Guha, N. India’s COVID Gender Gap: Women Left behind in Vaccination Drive. The Guardian, 28 June 2021. [Google Scholar]
- Schwarzinger, M.; Flicoteaux, R.; Cortarenoda, S.; Obadia, Y.; Moatti, J.-P. Low Acceptability of A/H1N1 Pandemic Vaccination in French Adult Population: Did Public Health Policy Fuel Public Dissonance? PLoS ONE 2010, 5, 10199. [Google Scholar] [CrossRef]
- Ludolph, R.; Nobile, M.; Hartung, U.; Castaldi, S.; Schulz, P.J. H1N1 Influenza Pandemic in Italy Revisited: Has the Willingness to Get Vaccinated Suffered in the Long Run? J. Public Health Res. 2015, 4, 559. [Google Scholar] [CrossRef] [Green Version]
- Dini, G.; Toletone, A.; Sticchi, L.; Orsi, A.; Bragazzi, N.L.; Durando, P. Influenza Vaccination in Healthcare Workers: A Comprehensive Critical Appraisal of the Literature. Hum. Vaccines Immunother. 2018, 14, 772–789. [Google Scholar] [CrossRef] [Green Version]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Reports. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 26 April 2020).
- Musa Ibrahim, A. Using Health Beliefs Model as an Intervention to Non Compliance with Hypertension Information among Hypertensive Patient. Int. Organ. Sci. Res. J. Hum. Soc. Sci. 2015, 20, 11–16. [Google Scholar] [CrossRef]
- Hammoumi, A.; Qesmi, R. A First Study on the Impact of Containment Measure on COVID-19 Spread in Morocco. medRxiv 2020, 140, 110231. [Google Scholar] [CrossRef]
- Berni, I.; Menouni, A.; Zegzouti, Y.F.; Kestemont, M.-P.; Godderis, L.; El Jaafari, S. MAROCOVID: Snapshot Monitoring of Knowledge and Perceptions of Safety Behaviors during the COVID-19 Outbreak in Morocco. Int. J. Environ. Res. Public Health 2021, 18, 5745. [Google Scholar] [CrossRef] [PubMed]
- Maraqa, B.; Nazzal, Z.; Rabi, R.; Sarhan, N.; Al-Shakhra, K.; Al-Kaila, M. COVID-19 Vaccine Hesitancy among Health Care Workers in Palestine: A Call for Action. Prev. Med. 2021, 149, 106618. [Google Scholar] [CrossRef] [PubMed]
- Gargano, L.M.; Painter, J.E.; Sales, J.M.; Morfaw, C.; Jones, L.M.; Murray, D.; Wingood, G.M.; DiClemente, R.J.; Hughes, J.M. Seasonal and 2009 H1N1 influenza vaccine uptake, predictors of vaccination, and self-reported barriers to vaccination among secondary school teachers and staff. Hum. Vaccines 2011, 7, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministère de la Santé Covidvax.live: Live COVID-19 Vaccination Tracker—Voir les Vaccinations en Temps Réel! Available online: http://covidvax.live/fr/location/mar (accessed on 15 March 2022).



{kind=link}
{kind=link}
| Characteristics | Total Number (%) | I Intend to Get Vaccinated | Not Intending to Vaccinate | p-Value |
|---|---|---|---|---|
| Total, No (%) | 3800 (100) | 1521 (40) | 2279 (60) | |
| Gender | ||||
| Men | 2175 (57.2) | 829 (38.1) | 1346 (61.8) | 0.003 |
| Women | 1625 (42.8) | 692 (42.6) | 933 (57.4) | |
| Age group | ||||
| 18–29 | 806 (21.2) | 36 (42.9) | 460 (57.1) | 0.046 |
| 30–44 | 1690 (44.5) | 661 (39.1) | 1029 (60.9) | |
| 45–59 | 1114 (29.3) | 430 (38.6) | 684 (61.4) | |
| >60 | 190 (5) | 84 (44.2) | 106 (55.8) | |
| Marital status | ||||
| Others | 1693 (44.6) | 617 (36.4) | 1076 63.6) | 0.000 |
| Married | 2107 (55.4) | 904 (42.9) | 1203 (57.1) | |
| Educational level | ||||
| >Primary school | 617 (16.2) | 228 (37) | 389 (63) | 0.033 |
| Secondary school | 1003 (26.4) | 377 (37.6) | 626 (62.4) | |
| Bachelor’s degree | 963 (25.3) | 409 (42.5) | 554 (57.5) | |
| Master’s and PhD | 1217 (32) | 507 (41.7) | 710 (58.3) | |
| Chronic disease | ||||
| None | 2439 (64.2) | 1000 (41) | 1439 (59) | 0.041 |
| Present | 1361 (35.8) | 521 (38.7) | 840 (61.7) | |
| Influenza vaccine | ||||
| Never | 3271 (86.1) | 1334 (40.8) | 1937 (59.2) | 0.01 |
| Once a year or more | 529 (13.9) | 187 (35.3) | 342 (64.7) | |
| Infection with COVID-19 | ||||
| Not infected | 2171 (57.1) | 837 (38.6) | 1334 (61.4) | 0.019 |
| Confirmed cases | 1629 (42.9) | 684 (42.0) | 945 (58.0) | |
| Monthly family income (MAD) | ||||
| <2000, | 1198 (31.5) | 510 (42.6) | 688 (57.4) | 0.043 |
| 2000–4000, | 197 (5.2) | 74 (37.6) | 123 (62.4) | |
| 4000–8000, | 449 (11.8) | 178 (39.6) | 271 (60.4) | |
| 8000–12,000, | 921 (24.2) | 364 (39.5) | 557 (60.5) | |
| >12,000 | 1035 (27.2) | 395 (38.5) | 640 (61.5) | |
| Total, No (%) | n | Vaccine Acceptance % | Odds Ratios | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|
| Gender | |||||
| Men | 2175 | 38.1 | Ref | ||
| Women | 1625 | 42.6 | 1.24 | 1.09–1.42 | 0.001 |
| Age group | |||||
| 18–29 | 806 | 42.9 | ref | ||
| 30–44 | 1690 | 39.1 | 1.19 | 1.05–1.67 | 0.030 |
| 45–59 | 1114 | 38.6 | 1.27 | 1.13–1.68 | 0.023 |
| >60 | 190 | 44.2 | 1.32 | 1.18–1.74 | 0.047 |
| Marital status | |||||
| Others | 1693 | 36.4 | ref | ||
| Married | 2107 | 42.9 | 1.31 | 1.16–1.50 | 0.000 |
| Educational level | |||||
| >Primary school | 617 | 37 | ref | ||
| Secondary school | 1003 | 37.6 | 0.98 | 0.82–1.16 | 0.831 |
| Bachelor’s degree | 963 | 42.5 | 1.18 | 0.99–1.40 | 0.055 |
| Master’s and PhD | 1217 | 41.7 | 1.21 | 0.99–1.48 | 0.059 |
| Chronic disease | |||||
| None | 2439 | 41 | ref | ||
| Present | 1361 | 38.3 | 1.24 | 1.09–1.62 | 0.004 |
| Influenza vaccine | |||||
| Never | 3271 | 40.8 | ref | ||
| Once a year or more | 529 | 35.3 | 1.07 | 0.93–1.23 | 0.322 |
| Infection with COVID-19 | |||||
| No infected | 2171 | 38.6 | ref | ||
| Confirmed cases | 1629 | 42 | 1.20 | 1.05–1.38 | 0.007 |
| Monthly income family (MAD) | |||||
| <2000, | 1198 | 42.6 | ref | ||
| 2000–4000, | 197 | 37.6 | 0.83 | 0.69–1.02 | 0.078 |
| 4000–8000, | 449 | 39.6 | 1.05 | 0.76–1.444 | 0.774 |
| 8000–12,000, | 921 | 39.5 | 0.96 | 0.76–1.21 | 0.727 |
| >12,000 | 1035 | 38.3 | 0.95 | 0.80–1.15 | 0.632 |
| Construct | Variable Description (Symbols) | Mean (SD) |
|---|---|---|
| Perceived susceptibility (Sus) | 3.90 (1.22) | |
| I am at risk of getting COVID-19 (Suc1) | 3.88 (1.3) | |
| It is likely that my children will be infected by the Coronavirus (Suc2) | 3.92 (1.19) | |
| It is possible that the elderly will get COVID-19 in the coming 9 months (Suc3) | 3.92 (1.18) | |
| Cronbach’s α | 0.778 | |
| Severity of COVID-19 (Sev) | 3.28 (1.23) | |
| I think that COVID-19 is a serious threat to human health (Sev1) | 4.12 (1.05) | |
| I believe that if I catch COVID-19 it will have a serious consequence for my life (Sev2) | 2.42 (1.21) | |
| I believe that COVID-19 can lead to death of my loves one if they get infected (Sev3) | 2.97 (1.36) | |
| I’m afraid to catch COVID-19 (Sev4) | 3.62 (1.32) | |
| Cronbach’s α | 0.703 | |
| Perceived barriers (Bar) | 4.53 (0.63) | |
| I have concerns about COVID-19 vaccine long-term side effects (Bar1) | 4.78 (0.57) | |
| Not enough research done about COVID-19 vaccine (Bar2) | 4.45 (0.64) | |
| The COVID-19 vaccine causes a person to get COVID-19 (Bar3) | 4.45 (0.66) | |
| I am not sure if COVID-19 vaccine is effective in preventing the disease (Bar4) | 4.45 (0.64) | |
| Cronbach’s α | 0.701 | |
| Perceived benefits (Ben) | 4.5 (0.82) | |
| COVID-19 vaccine will be effective in preventing Coronavirus (Ben1) | 4.67 (0.82) | |
| If I get the vaccines, I will be less likely to get COVID-19 (Ben2) | 4.57 (0.83) | |
| I think COVID-19 vaccine can prevent people from spreading the virus to others (Ben3) | 4.27 (0.82) | |
| Cronbach’s α | 0.665 | |
| Self-efficacy (SE) | 4.5 (0.84) | |
| I will be able to get the vaccines to prevent contracting COVID-19 (SE1) | 4.76 (0.66) | |
| It will be easy for me to get the vaccines to protect myself from COVID-19 (SE2) | 4.28 (0.87) | |
| Getting vaccinated to prevent COVID-19 is convenient (SE3) | 4.47 (1.00) | |
| Cronbach’s α | 0.763 | |
| Cues to action (CtA) | 4.31 (0.89) | |
| I will be more optimistic about COVID-19 vaccine if I know more about it (CtA1) | 4.05 (0.96) | |
| The type of vaccine that is available would affect my decision (CtA2) | 4.39 (0.94) | |
| I would be more confident if experts or people I trust would recommend the vaccine (CtA3) | 4.49 (0.76) | |
| Cronbach’s α | 0.668 | |
| Intention to receive a COVID-19 vaccine (Int) | 3.56 (1.28) | |
| I intend to get vaccinated as soon as possible (Int1) | 3.49 (1.39) | |
| I probably get it but not as soon as possible (Int2) | 3.84 (1.19) | |
| I get vaccinated if an expert or doctor I trust recommend me COVID-19 vaccines (Int3) | 2.74 (1.41) | |
| I am currently undecided (Int4) | 4.18 (1.16) | |
| Cronbach’s α | 0.718 | |
| Constructs | Measurement Items | Std. Loading | t-Value | Reliability and Variability |
|---|---|---|---|---|
| Perceived susceptibility (Sus) | Sus1 | 0.281 | 29.579 | AVE = 0.656; CR = 0.828; ASV = 0.017; MSV = 0.033 |
| Sus2 | 0.977 | 93.517 | ||
| Sus3 | 0.963 | fixed | ||
| Severity of COVID-19 (Sev) | Sev1 | 0.856 | 16.052 | AVE = 0.502; CR = 0.789; ASV= 0.024; MSV = 0.062 |
| Sev2 | 0.36 | 17.342 | ||
| Sev3 | 0.721 | fixed | ||
| Sev4 | 0.7 | 23.626 | ||
| Perceived barriers (Bar) | Bar1 | 0.681 | 29.601 | AVE = 0.509; CR = 0.794; ASV = 0.025; MSV = 0.098 |
| Bar2 | 0.391 | 21.988 | ||
| Bar3 | 0.859 | fixed | ||
| Bar4 | 0.826 | 51.166 | ||
| Perceived benefits (Ben) | Ben1 | 0.839 | fixed | AVE = 0.524; CR = 0.740; ASV = 0.026; MSV = 0.171 |
| Ben2 | 0.887 | 32.896 | ||
| Ben3 | 0.289 | 16.638 | ||
| Self-efficacy (SE) | SE1 | 0.825 | 20.785 | AVE = 0.548; CR = 0.779; ASV = 0.051; MSV = 0.098 |
| SE2 | 0.563 | 16.638 | ||
| SE3 | 0.804 | fixed | ||
| Cues to action (CtA) | CtA1 | 0.613 | 27.509 | AVE = 0.528; CR = 0.767; ASV = 0.030; MSV = 0.171 |
| CtA2 | 0.688 | 31.806 | ||
| CtA3 | 0.858 | fixed | ||
| Intention (Int) | Int1 | 0.8 | fixed | AVE = 0.504; CR = 0.866; ASV = 0.051; MSV = 0.171 |
| Int2 | 0.666 | 26.623 | ||
| Int3 | 0.759 | 20.535 | ||
| Int4 | 0.828 | 23.626 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berni, I.; Menouni, A.; Filali Zegzouti, Y.; Kestemont, M.-P.; Godderis, L.; El Jaafari, S. Factors Associated with COVID-19 Vaccine Acceptance in Morocco: Applying the Health Belief Model. Vaccines 2022, 10, 784. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050784
Berni I, Menouni A, Filali Zegzouti Y, Kestemont M-P, Godderis L, El Jaafari S. Factors Associated with COVID-19 Vaccine Acceptance in Morocco: Applying the Health Belief Model. Vaccines. 2022; 10(5):784. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050784
Chicago/Turabian StyleBerni, Imane, Aziza Menouni, Younes Filali Zegzouti, Marie-Paule Kestemont, Lode Godderis, and Samir El Jaafari. 2022. "Factors Associated with COVID-19 Vaccine Acceptance in Morocco: Applying the Health Belief Model" Vaccines 10, no. 5: 784. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050784