
Level of Acceptance of Mandatory Vaccination and Legal Sanctions for Refusing Mandatory Vaccination of Children


Abstract
:1. Introduction
2. Materials and Methods
2.1. General Description of the Study
2.2. Sampling Design
2.3. Research Tool
2.4. Statistical Design
2.5. Ethical Review
3. Results
3.1. Characterisation of Study Group
3.2. Attitude to Mandatory Vaccination
4. Discussion
4.1. Key Results
4.2. Limitations
4.3. Interpretations
5. Conclusions
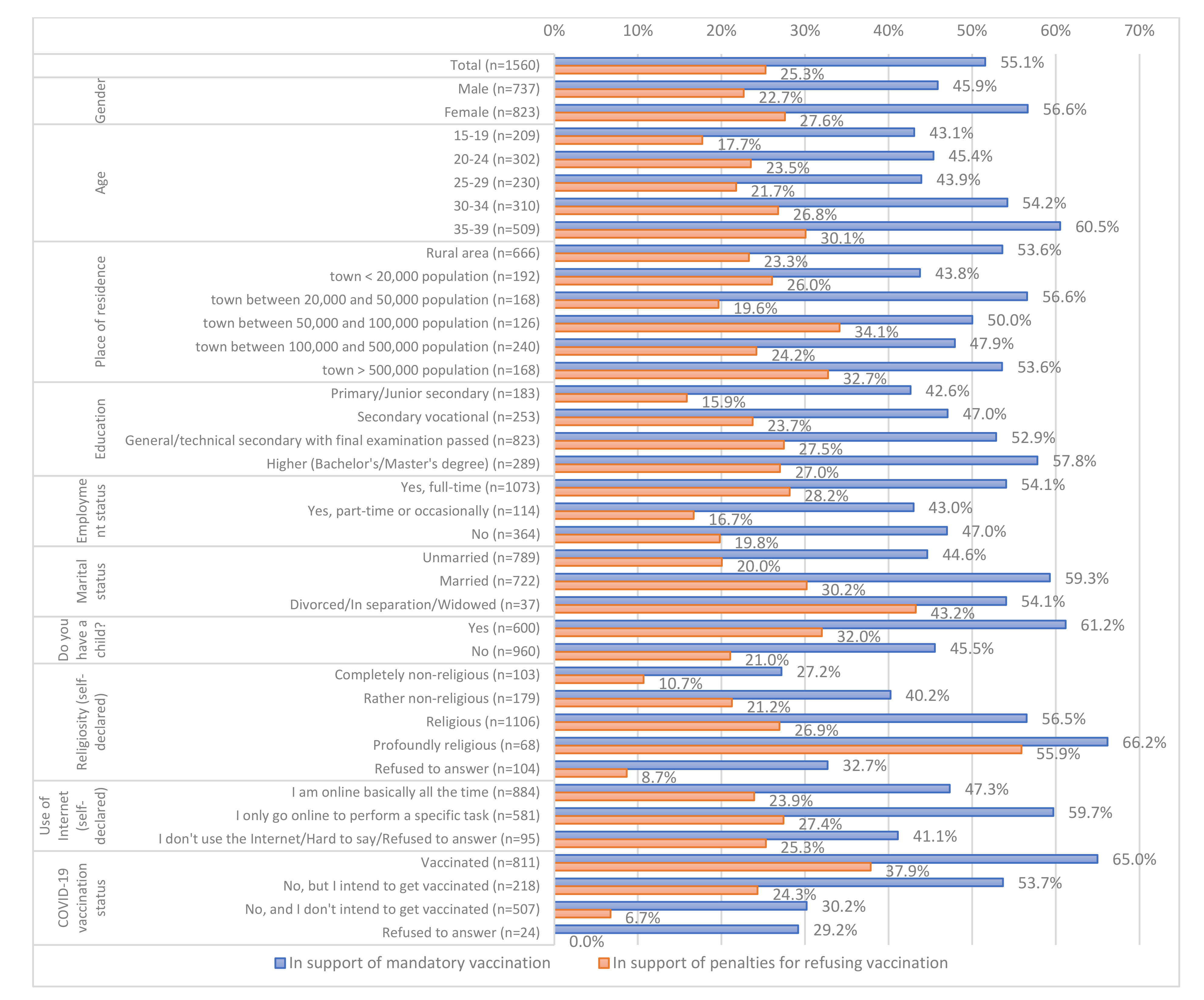
- Even though a mandatory vaccination scheme has been operating in Poland since the 1960s, the opinions about mandatory vaccination are divided. Only more than half of those aged 15–39 years are in favor of mandatory vaccination.
- One in four respondents declared support for legal or financial sanctions against those refusing mandatory vaccination of their children.
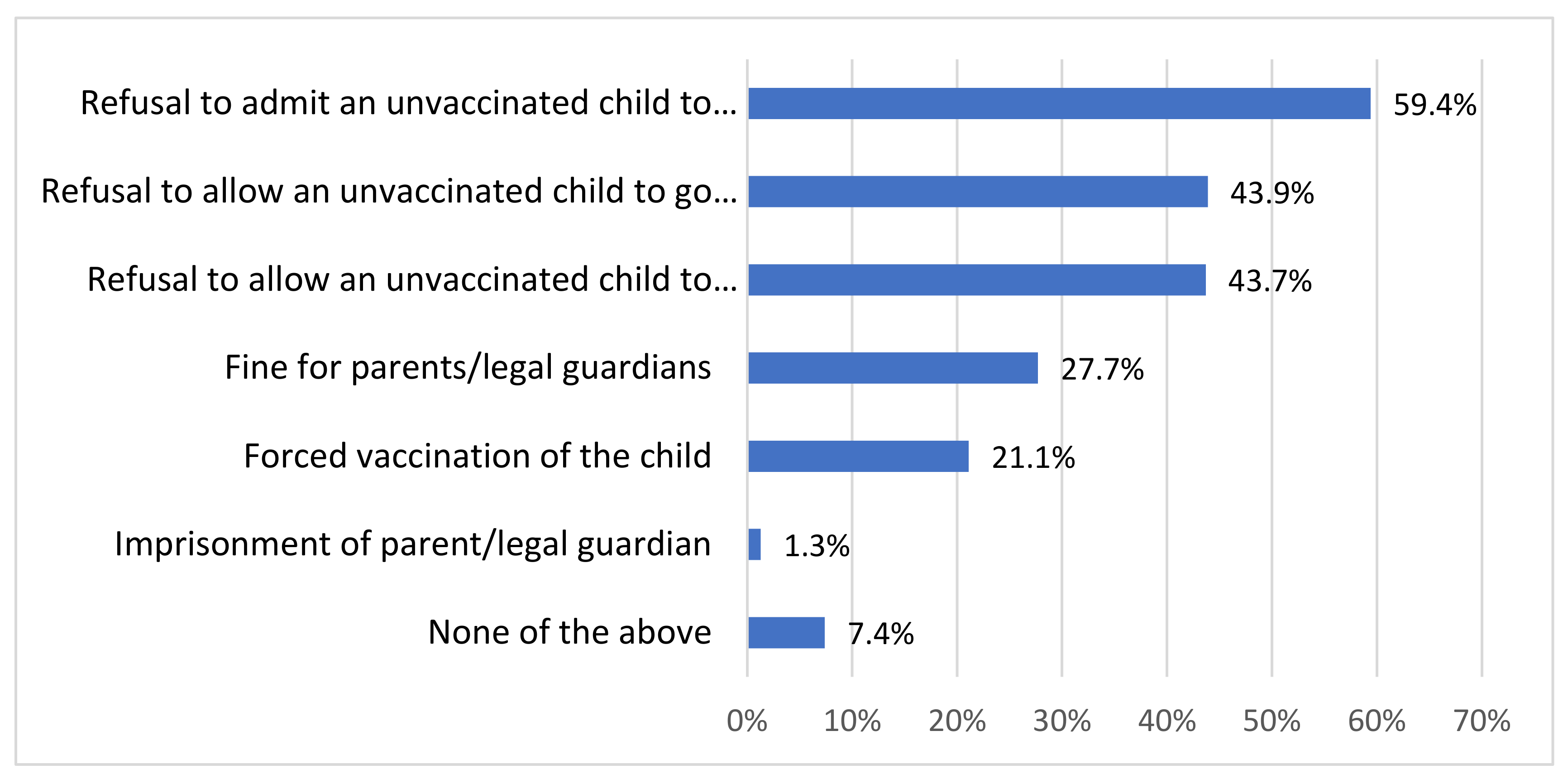
- The most widely accepted sanctions for refusing to vaccinate children include the refusal to admit an unvaccinated child to a nursery or kindergarten, refusal to allow such children to go on organized holiday trips, and refusal to allow such children to take part in extracurricular activities offered by state-owned institutions.
- More extensive statistical analyses based on multivariate models revealed no effect of most typical sociodemographic variables (e.g., gender, education, size of population in place of residence) on respondents’ attitudes to mandatory vaccination and penalization of vaccination refusal. Significant factors comprised self-declared religiosity and a positive COVID-19 vaccination status.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grzybowski, A.; Patryn, R.K.; Sak, J.; Zagaja, A. Vaccination refusal. Autonomy and permitted coercion. Pathog. Glob. Health 2017, 111, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Mallory, M.L.; Lindesmith, L.C.; Baric, R.S. Vaccination-induced herd immunity: Successes and challenges. J. Allergy Clin. Immunol. 2018, 142, 64–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieszka, M.; Waksmańska, W.; Woś, H. Wiedza rodziców dzieci do drugiego roku życia na temat szczepień ochronnych. Med. Ogólna Nauk. Zdrowiu 2016, 22, 221–226. [Google Scholar] [CrossRef]
- Czechowicz, S. Problem wielości sankcji represyjnych za nieszczepienie dziecka z perspektywy skutecznego wykonania obowiązku szczepień. Ruch Praw. Èkon. Socjol. 2021, 83, 37–46. [Google Scholar] [CrossRef]
- Szalonka, A. Antagonistyczne Postawy Wobec Szczepień Zagrożeniem Dla Cywilizacji [Antagonistic Attitudes towards Vaccination as a Threat to Civilization]; Uniwersytet Wrocławski: Wrocław, Poland, 2019. [Google Scholar]
- Księska-Koszałka, J.M. Vaccination decision-making problems among parents. Implications for the doctor–patient relationship. PiMR 2020, 17, 111–115. [Google Scholar] [CrossRef]
- Wilińska, M.; Warakomska, M. Parents avoiding child vaccination in the neonatal period—An analysis of attitudes. Dev. Period Med. 2018, 22, 315–322. [Google Scholar] [CrossRef]
- Hakim, H.; Bettinger, J.A.; Chambers, C.T.; Driedger, S.M.; Dubé, E.; Gavaruzzi, T.; Giguere, A.M.C.; Kavanagh, É.; Leask, J.; MacDonald, S.E.; et al. A Web Application About Herd Immunity Using Personalized Avatars: Development Study. J. Med. Internet Res. 2020, 22, e20113. [Google Scholar] [CrossRef]
- Hakim, H.; Provencher, T.; Chambers, C.T.; Driedger, S.M.; Dube, E.; Gavaruzzi, T.; Giguere, A.M.C.; Ivers, N.M.; MacDonald, S.; Paquette, J.-S.; et al. Interventions to help people understand community immunity: A systematic review. Vaccine 2019, 37, 235–247. [Google Scholar] [CrossRef] [Green Version]
- Guerra, F.M.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Li, Y.; Crowcroft, N.S. The basic reproduction number (R0) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef]
- Bester, J.C. Measles and Measles Vaccination: A review. JAMA Pediatr. 2016, 170, 1209–1215. [Google Scholar] [CrossRef]
- Żuradzki, T. Szczepienia Obowiązkowe a Efekt Ofiary Zidentyfikowanej. Filozofia w Praktyce 2016, 2, 4. [Google Scholar]
- Konstytucja Rzeczypospolitej Polskiej, Z Dnia 2 Kwietnia 1997 R., Dz. U. Z 1997 R. Nr 78, Poz. 483. Available online: https://www.sejm.gov.pl/prawo/konst/polski/kon1.htm (accessed on 5 November 2021).
- Ustawa z Dnia 5 Grudnia 2008 R.O Zapobieganiu Oraz Zwalczaniu Zakażeń I Chorób Zakaźnych U Ludzi, Dz. U. 2008 Nr 234 Poz. 1570. Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20082341570/U/D20081570Lj.pdf (accessed on 5 November 2021).
- Czechowicz, S. Charakter prawny odpowiedzialności za nieszczepienie dziecka [Legal nature of liability for non-vaccinating a child]. Studia Prawnicze KUL 2021, 267–282. [Google Scholar] [CrossRef]
- Szczęch, N. Problematyka przymusowych szczepień ochronnych u dzieci na tle orzecznictwa sądów administracyjnych. Rocz. Adm. Prawa 2016, XVI, 187–211. [Google Scholar]
- Haberko, J. Administracyjnoprawny obowiązek szczepienia dzieci a zgoda przedstawiciela ustawowego. Uniw. Adama Mickiewicza Pozn. 2017, 9–28. [Google Scholar] [CrossRef]
- Wyrok SN Z Dnia 8 Stycznia 2016 r., V KK 306/15, LEX nr 1963649. Available online: https://www.sn.pl (accessed on 5 November 2021).
- Czechowicz, S. Efektywność sankcji za uchylanie się od obowiązkowych szczepień ochronnych, Uniwersytet Łódzki. Studia Prawnoustr. 2020, 49, 15–26. [Google Scholar]
- Wyrok WSA w Warszawie z 19 Października 2016 r., VII SA/Wa 2537/15, Lex nr 2090334. Available online: https://orzeczenia.nsa.gov.pl (accessed on 5 November 2021).
- NBP, 7.11.2021. Available online: https://www.nbp.pl (accessed on 7 November 2021).
- Ustawa z Dnia 17 Czerwca 1966 R. O Postępowaniu Egzekucyjnym, W. Administracji, Dz.U. 1966 Nr 24 Poz. 151. Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU19660240151/U/D19660151Lj.pdf (accessed on 5 November 2021).
- Ustawa z Dnia 20 Maja 1971 r. Kodeks Wykroczeń, Dz. U. 1971 Nr 12 Poz. 114. Available online: https://www.isap.sejm.gov.pl (accessed on 5 November 2021).
- PZH. Available online: https://www.pzh.gov.pl (accessed on 20 February 2022).
- Włodarska, A.; Gujski, M.; Pinkas, J.; Raciborski, F. The influence of socio-demographic characteristics on attitudes towards prophylactic vaccination in Poland. Occup. Med. Environ. Health 2021, 34, 121–132. [Google Scholar] [CrossRef]
- Brunelli, L.; Valent, F.; Romanese, F.; Tricarico, P.; Pellizzaro, A.; D’Angelo, M.; Benetollo, P.P.; Iob, A.; Forgiarini, M.; Brusaferro, S. Parental trust and beliefs after the discovery of a six-year-long failure to vaccinate. Hum. Vaccines Immunother. 2021, 17, 583–587. [Google Scholar] [CrossRef]
- Bramušková, J.; Balogová, E.; Spodniaková, M. Parental Attitudes towards Children’s Vaccination; Slovak Medical University: Bratislava, Slovakia, 2016. [Google Scholar]
- Offit, P.A.; Quarles, J.; Gerber, M.A.; Hackett, C.J.; Marcuse, E.K.; Kollmann, T.R.; Gellin, B.G.; Landry, S. Addressing Parents’ Concerns: Do Multiple Vaccines Overwhelm or Weaken the Infant’s Immune System? Pediatrics 2002, 109, 124–129. [Google Scholar] [CrossRef] [Green Version]
- Heininger, U. An internet-based survey on parental attitudes towards immunization. Vaccine 2006, 24, 6351–6355. [Google Scholar] [CrossRef]
- Szalonka, A. Społeczne Uwarunkowania Szczepień W Polsce W Świetle Badań Ankietowych [Health Conditions of Preventive Vaccination in Poland in the Light of Surveys]; Uniwersytet Wrocławski: Wrocław, Poland, 2020. [Google Scholar]
- Gravagna, K.; Becker, A.; Valeris-Chacin, R.; Mohammed, I.; Tambe, S.; Awan, F.A.; Toomey, T.L.; Basta, N.E. Global assessment of national mandatory vaccination policies and consequences of non-compliance. Vaccine 2020, 38, 7865–7873. [Google Scholar] [CrossRef]
- Dońska, K.; Suwała, M.; Zarzycka, D. Postawy i edukacja wakcynologiczna rodziców, Uniwersytet Medyczny w Lublinie. Pielęgniarstwo XXI Wieku/Nurs. 21st Century 2018, 17, 58–64. [Google Scholar]
- Duda, S.; Głogowska-Gruszka, A.; Buczkowska, M. Attitudes and Opinions of Parents of Children at the Age of up to 6 Years Who Inhabit the Silesian Province Concerning Vaccination in Relation to the Implementation of Obligatory Vaccinations; PHiE: Delhi, India, 2019; Volume 100, pp. 115–123. [Google Scholar]
- Carrieri, V.; Madio, L.; Principe, F. Vaccine hesitancy and (fake) news: Quasi-experimental evidence from Italy. Health Econ. 2019, 28, 1377–1382. [Google Scholar] [CrossRef]
- Mathieu, P.; Gautier, A.; Raude, J.; Goronflot, T.; Launay, T.; Debin, M.; Guerrisi, C.; Turbelin, C.; Hanslik, T.; Jestin, C.; et al. Population perception of mandatory childhood vaccination programme before its implementation, France, 2017. Eurosurveillance 2019, 24, 1900053. [Google Scholar] [CrossRef]
- Helps, C.; Leask, J.; Barclay, L. “It just forces hardship”: Impacts of government financial penalties on non-vaccinating parents. J. Public Health Policy 2018, 39, 156–169. [Google Scholar] [CrossRef]
- Casula, M.; Toth, F. The 2017 Italian reform on mandatory childhood vaccinations: Analysis of the policy process and early implementation. Health Policy 2021, 125, 7–11. [Google Scholar] [CrossRef]
- Wyrok Europejskiego Trybunału Praw Człowiekaz Dnia 8 Kwietnia 2021 R. Syg.47621/13. Available online: https://sip.lex.pl/akty-prawne/dzu-dziennik-ustaw/konwencja-o-ochronie-praw-czlowieka-i-podstawowych-wolnosci-16795332/art-38 (accessed on 8 May 2022).
- Patryn, R.K.; Zagaja, A. Vaccinations—Between free will and coercion. Hum. Vaccines Immunother. 2016, 12, 2204–2205. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Total | 1560 | 100 |
| Gender | ||
| Male | 737 | 47.2 |
| Female | 823 | 52.8 |
| Age | ||
| 15–19 | 209 | 13.4 |
| 20–24 | 302 | 19.4 |
| 25–29 | 230 | 14.7 |
| 30–34 | 310 | 19.9 |
| 35–39 | 509 | 32.6 |
| Place of residence | ||
| rural area | 666 | 42.7 |
| town < 20,000 population | 192 | 12.3 |
| town between 20,000 and 50,000 population | 168 | 10.8 |
| town between 50,000 and 100,000 population | 126 | 8.1 |
| town between 100,000 and 500,000 population | 240 | 15.4 |
| town > 500,000 population | 168 | 10.8 |
| Education | ||
| Primary/Junior secondary | 183 | 11.8 |
| Secondary vocational | 253 | 16.3 |
| General/technical secondary with final examination passed | 823 | 53.2 |
| Higher (Bachelor’s/Master’s degree) | 289 | 18.7 |
| Employment status | ||
| Yes, full-time | 1073 | 69.2 |
| Yes, part-time or occasionally | 114 | 7.4 |
| No | 364 | 23.5 |
| Marital status | ||
| Unmarried | 789 | 51 |
| Married | 722 | 46.6 |
| Divorced/In separation/Widowed | 37 | 2.4 |
| Do you have a child? | ||
| Yes | 600 | 38.5 |
| No | 960 | 61.5 |
| Religiosity (self-declared) | ||
| Completely non-religious | 103 | 6.6 |
| Rather non-religious | 179 | 11.5 |
| Religious | 1106 | 70.9 |
| Profoundly religious | 68 | 4.4 |
| Refused to answer | 104 | 6.7 |
| COVID-19 vaccination status | ||
| Vaccinated | 811 | 52 |
| No, but I intend to get vaccinated | 218 | 14 |
| No, and I don’t intend to get vaccinated | 507 | 32.5 |
| Refused to answer | 24 | 1.5 |
| Mandatory Vaccination | Penalties for Refusing Vaccination | ||||
|---|---|---|---|---|---|
| n | Sig. | OR (95% CI OR) | Sig. | OR (95% CI OR) | |
| Gender | |||||
| Male | 737 | Ref. | Ref. | Ref. | Ref. |
| Female | 823 | 0.145 | 1.18 (0.94–1.48) | 0.896 | 1.02 (0.78–1.32) |
| Age | |||||
| 15–24 years | 511 | Ref. | Ref. | Ref. | Ref. |
| 25–39 years | 1049 | 0.981 | 1 (0.72–1.39) | p < 0.05 | 0.67 (0.45–0.98) |
| Place of residence | |||||
| rural area | 666 | Ref. | Ref. | Ref. | Ref. |
| town < 50,000 population | 360 | 0.447 | 0.90 (0.68–1.19) | 0.865 | 1.03 (0.74–1.43) |
| town between 50,000 and 100,000 population | 126 | 0.588 | 0.89 (0.59–1.36) | 0.055 | 1.57 (0.99–2.49) |
| town between 100,000 and 500,000 population | 240 | 0.221 | 0.82 (0.59–1.13) | 0.708 | 1.08 (0.74–1.57) |
| town > 500,000 population | 168 | 0.553 | 0.89 (0.62–1.3) | 0.162 | 1.35 (0.89–2.05) |
| Education | |||||
| Primary/Junior secondary | 183 | Ref. | Ref. | Ref. | Ref. |
| Secondary vocational | 253 | 0.887 | 0.97 (0.6–1.56) | 0.358 | 1.33 (0.73–2.42) |
| General/technical secondary with final examination passed | 823 | 0.572 | 1.13 (0.75–1.7) | 0.332 | 1.3 (0.77–2.21) |
| Higher (Bachelor’s/Master’s degree) | 289 | 0.519 | 1.18 (0.72–1.93) | 0.718 | 1.12 (0.61–2.06) |
| Employment status | |||||
| Yes, full-time | 1073 | 0.429 | 0.87 (0.61–1.24) | 0.338 | 1.23 (0.81–1.86) |
| Yes, part-time or occasionally | 114 | 0.27 | 0.76 (0.47–1.24) | 0.288 | 0.71 (0.38–1.33) |
| No | 364 | Ref. | Ref. | Ref. | Ref. |
| Having children | |||||
| children 0–6 years old = NO | 1241 | Ref. | Ref. | Ref. | Ref. |
| children 0–6 years old = YES | 319 | 0.684 | 0.94 (0.71–1.25) | p < 0.05 | 1.42 (1.04–1.94) |
| children 7–15 years old = NO | 1185 | Ref. | Ref. | Ref. | Ref. |
| children 7–15 years old = YES | 375 | p < 0.05 | 1.42 (1.07–1.88) | 0.125 | 1.27 (0.94–1.73) |
| children 16 years old and older = NO | 1513 | Ref. | Ref. | Ref. | Ref. |
| children 16 years old and older = YES | 47 | 0.411 | 1.32 (0.68–2.56) | 0.701 | 0.87 (0.42–1.78) |
| Religiosity (self-declared) | |||||
| Completely non-religious | 103 | Ref. | Ref. | Ref. | Ref. |
| Rather non-religious | 179 | 0.156 | 1.5 (0.86–2.63) | 0.145 | 1.77 (0.82–3.8) |
| Religious | 1106 | p < 0.001 | 2.28 (1.41–3.68) | 0.054 | 1.95 (0.99–3.86) |
| Profoundly religious | 68 | p < 0.001 | 3.31 (1.64–6.71) | p < 0.001 | 6.39 (2.72–14.97) |
| Refused to answer | 104 | 0.631 | 1.17 (0.62–2.19) | 0.451 | 0.69 (0.26–1.82) |
| Use of Internet (self-declared) | |||||
| I am online basically all the time | 884 | Ref. | Ref. | Ref. | Ref. |
| I only go online to perform a specific task | 581 | p < 0.01 | 1.39 (1.1–1.77) | 0.603 | 1.08 (0.82–1.42) |
| I don’t use the Internet/Hard to say/Refused to answer | 95 | 0.301 | 0.78 (0.49–1.25) | 0.559 | 1.18 (0.68–2.02) |
| COVID-19 vaccination status | |||||
| Vaccinated | 811 | p < 0.001 | 3.69 (2.88–4.74) | p < 0.001 | 7.84 (5.31–11.56) |
| No, but I intend to get vaccinated | 218 | p < 0.001 | 2.52 (1.81–3.53) | p < 0.001 | 4.6 (2.86–7.39) |
| No, and I don’t intend to get vaccinated | 531 | Ref. | Ref. | Ref. | Ref. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reczulska, A.; Tomaszewska, A.; Raciborski, F. Level of Acceptance of Mandatory Vaccination and Legal Sanctions for Refusing Mandatory Vaccination of Children. Vaccines 2022, 10, 811. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050811
Reczulska A, Tomaszewska A, Raciborski F. Level of Acceptance of Mandatory Vaccination and Legal Sanctions for Refusing Mandatory Vaccination of Children. Vaccines. 2022; 10(5):811. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050811
Chicago/Turabian StyleReczulska, Aneta, Aneta Tomaszewska, and Filip Raciborski. 2022. "Level of Acceptance of Mandatory Vaccination and Legal Sanctions for Refusing Mandatory Vaccination of Children" Vaccines 10, no. 5: 811. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050811