
A Belgian Serosurveillance/Seroprevalence Study of Diphtheria, Tetanus and Pertussis Using a Luminex xMAP Technology-Based Pentaplex


Abstract
:1. Introduction
2. Materials and Methods
2.1. Antigens and Reagents
2.2. Reference, Control and Validation Sera
2.3. ELISA
2.4. Conjugation of Capture Antigens to Microspheres
2.5. Pentaplex MIA
3. Results
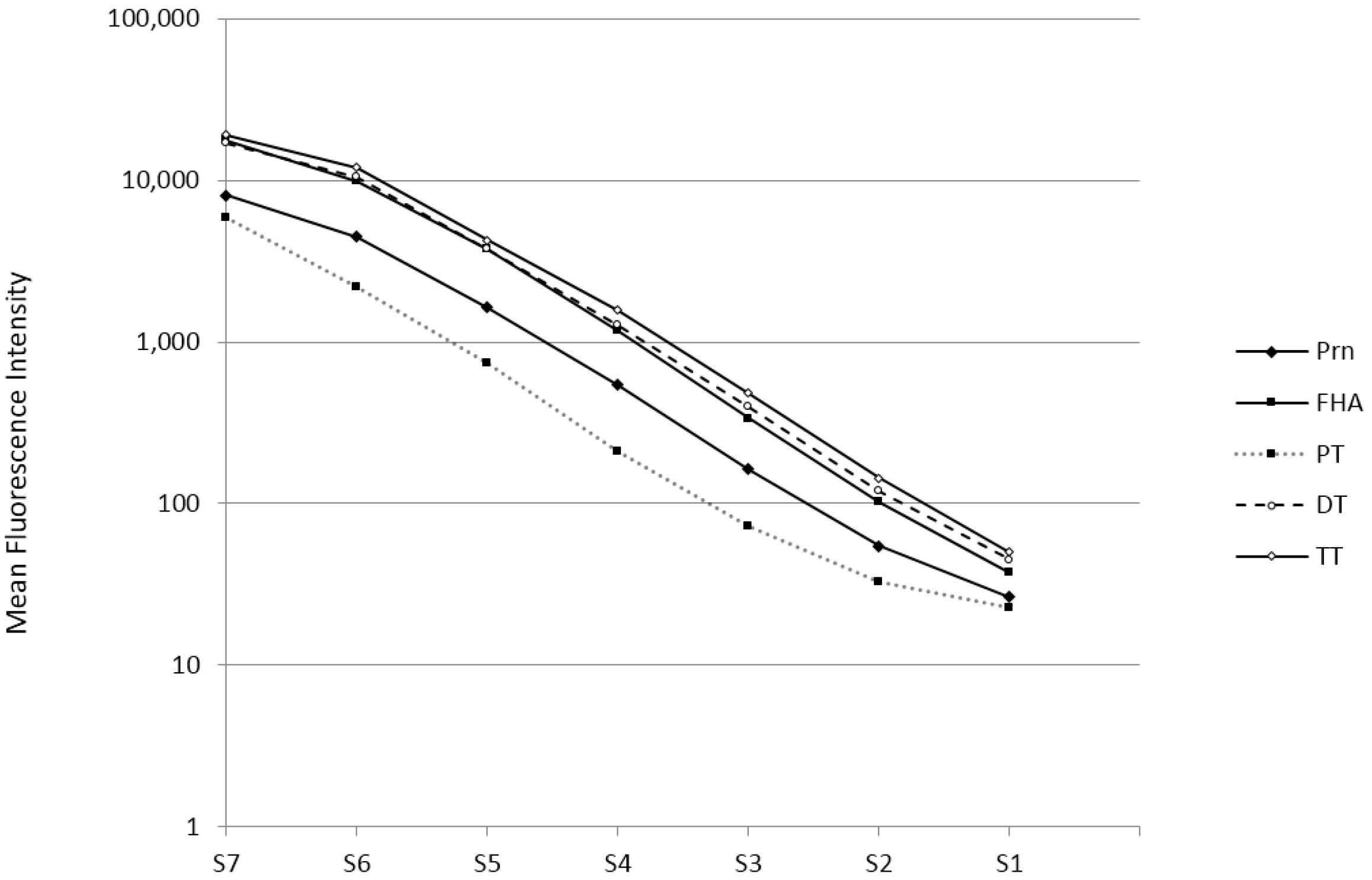
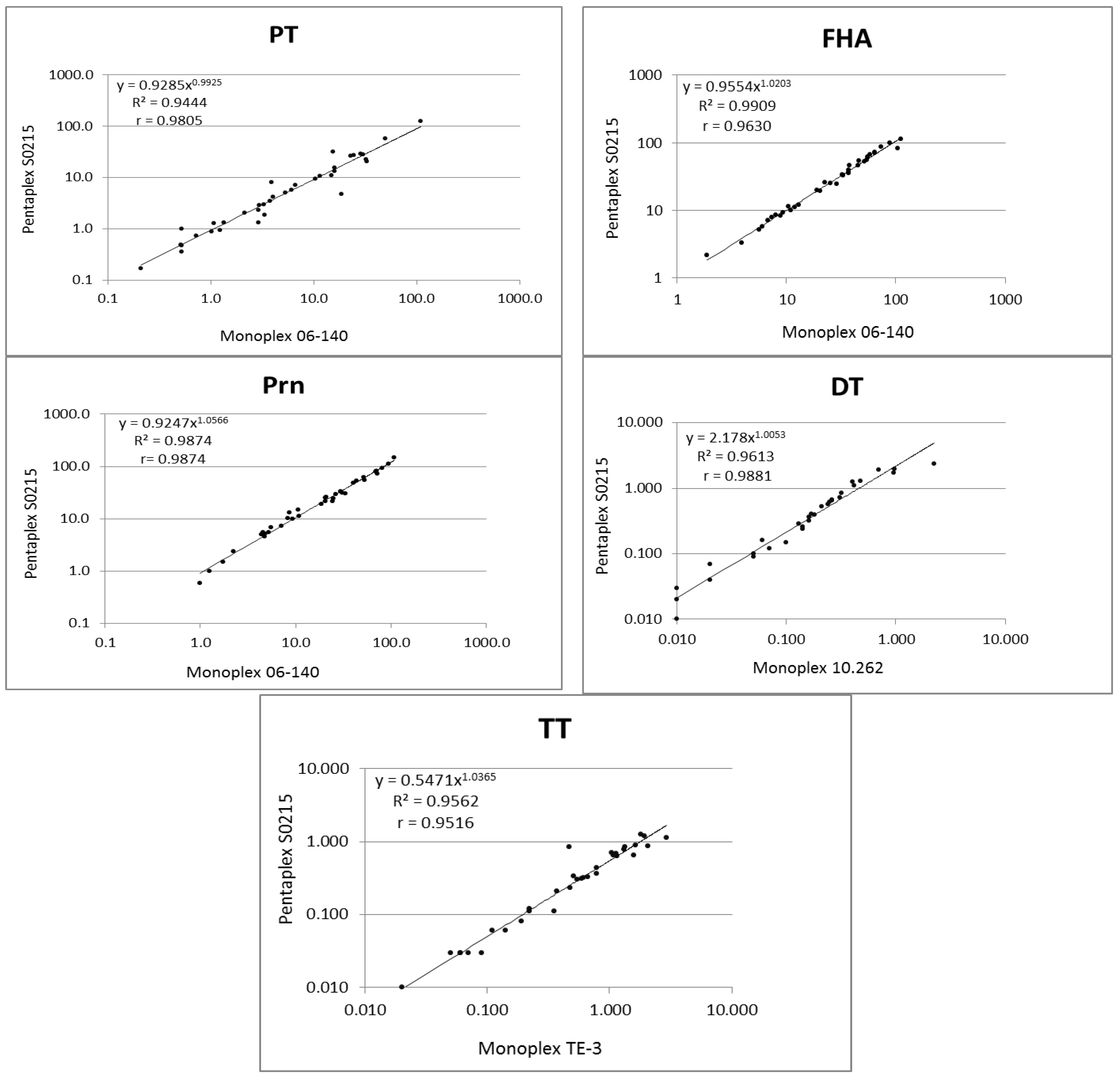
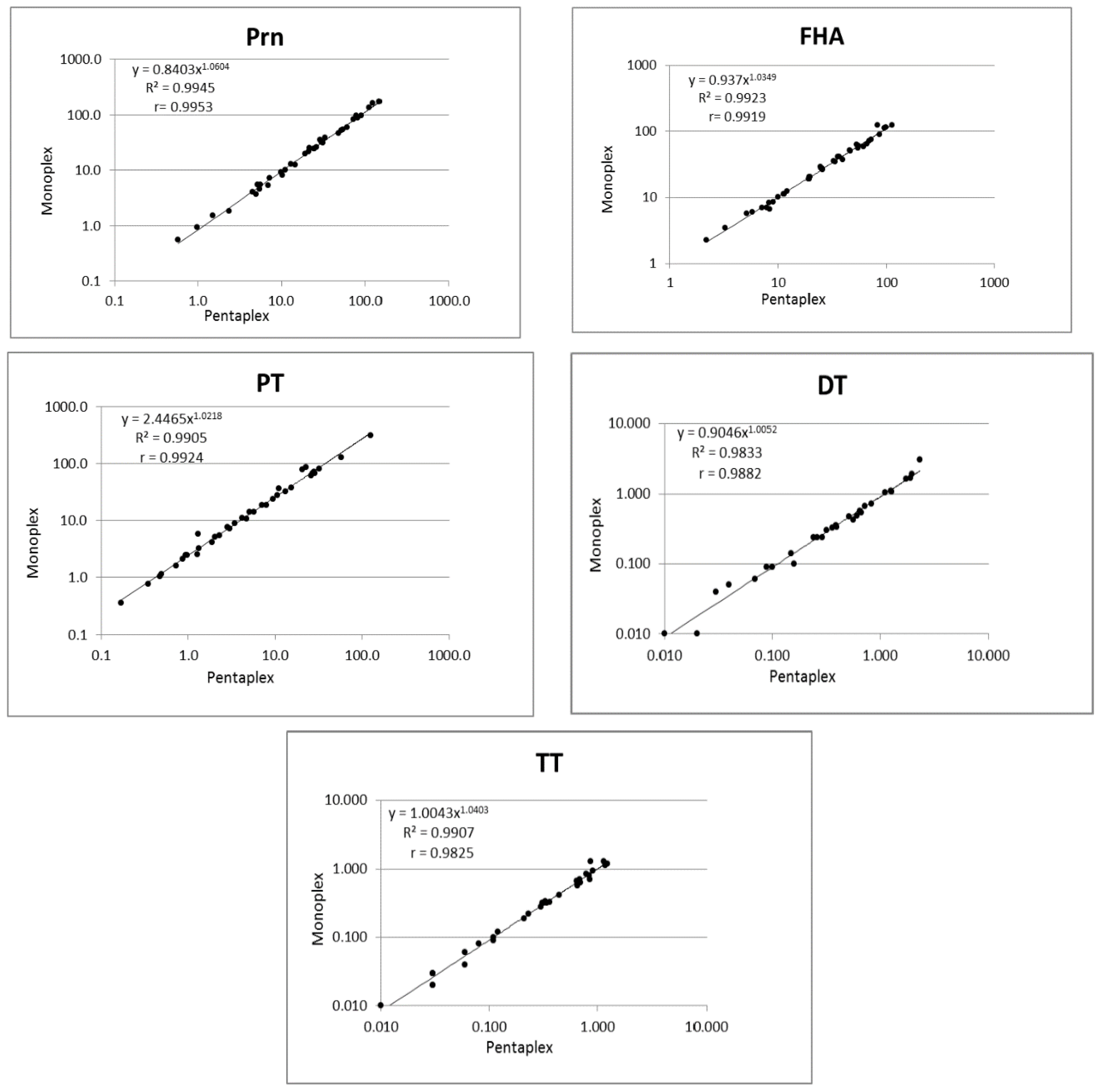
3.1. Validation of the Pentaplex Immunoassay
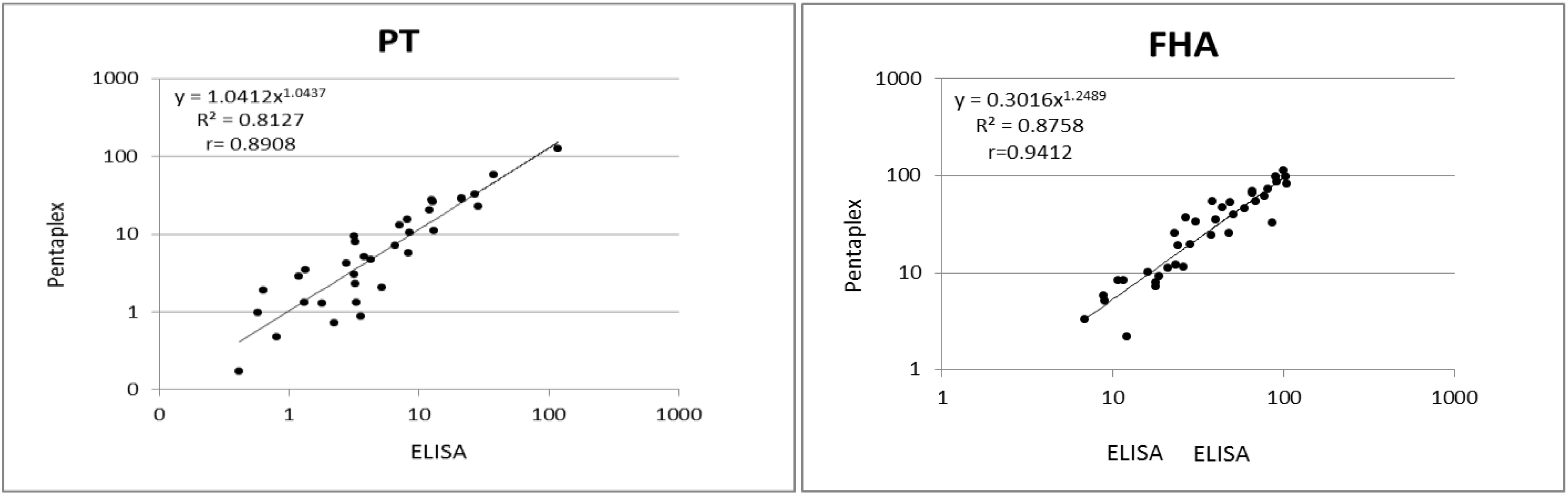
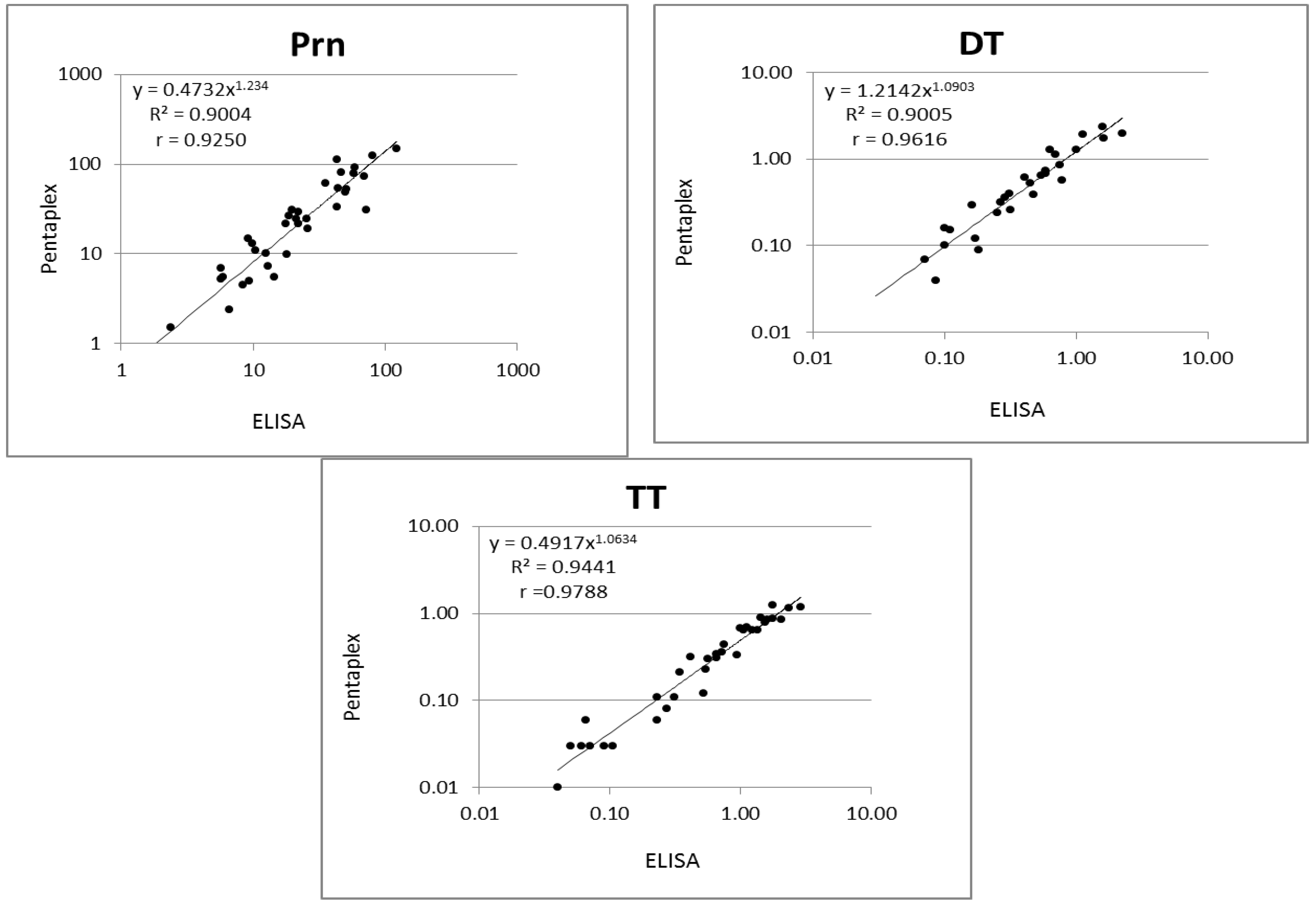
3.2. Validation of the Pentaplex on a Small Serum Panel
3.3. Results of the Serosurveillance/Seroprevalence Study
4. Discussions and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix

References
- Theeten, H.; Hutse, V.; Hens, N.; Yavuz, Y.; Hoppenbrouwers, K.; Beutels, P.; Vranckx, R.; van Damme, P. Are we hitting immunity targets? The 2006 age-specific seroprevalence of measles, mumps, rubella, diphteria and tetanus in Belgium. Epidemiol. Infect. 2011, 139, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Van der Wielen, M.; van Damme, P.; van Herck, K.; Schlegel-Haueter, S.; Siegrist, C.A. Seroprevalence of Bordetella pertussis antibodies in Flanders (Belgium). Vaccine 2003, 21, 2412–2417. [Google Scholar] [CrossRef]
- Huygen, K.; Rodeghiero, C.; Govaerts, D.; Leroux-Roels, I.; Melin, P.; Reynders, M.; van Der Meeren, S.; van den Wijngaert, S.; Piérard, D. Bordetella pertussis seroprevalence in Belgian adults 20–39 years old, anno 2012. Epidemiol. Infect. 2014, 142, 724–728. [Google Scholar] [CrossRef] [PubMed]
- Prince, H.E.; Lape-Nixon, M.; Matud, J. Evaluation of a tetraplex microsphere assay for Bordetella pertussis antibodies. Clin. Vaccine Immunol. 2006, 13, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Reder, S.; Riffelmann, M.; Becker, C.; Wirsing von Konig, C.H. Measuring immunoglobulin g antibodies to tetanus toxin, diphtheria toxin, and pertussis toxin with single-antigen enzyme-linked immunosorbent assays and a bead-based multiplex assay. Clin. Vaccine Immunol. 2008, 15, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Van Gageldonk, P.G.; van Schaijk, F.G.; van der Klis, F.R.; Berbers, G.A. Development and validation of a multiplex immunoassay for the simultaneous determination of serum antibodies to Bordetella pertussis, diphtheria and tetanus. J. Immunol. Methods 2008, 335, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Van Gageldonk, P.G.; von Hunolstein, H.C.; van der Klis, F.R.; Berbers, G.A. Improved specificity of a multiplex immunoassay for quantitation of anti-diphtheria toxin antibodies with the use of diphtheria toxoid. Clin. Vaccine Immunol. 2011, 18, 1183–1186. [Google Scholar] [CrossRef] [PubMed]
- Stenger, R.M.; Smits, M.; Kuipers, B.; Kessen, S.F.; Boog, C.J.; van Els, C.A. Fast, antigen-saving multiplex immunoassay to determine levels and avidity of mouse serum antibodies to pertussis, diphtheria, and tetanus antigens. Clin. Vaccine Immunol. 2011, 18, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Maertens, K.; Caboré, R.N.; Huygen, K.; Hens, N.; van Damme, P.; Leuridan, E. Pertussis vaccination during pregnancy in Belgium: Results of a prospective controlled cohort study. Vaccine 2016, 34, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Huygen, K.; Cabore, R.N.; Maertens, K.; Van, D.P.; Leuridan, E. Humoral and cell mediated immune responses to a pertussis containing vaccine in pregnant and nonpregnant women. Vaccine 2015, 33, 4117–4123. [Google Scholar] [CrossRef] [PubMed]
- Luminex cookbook 2nd Edition. Available online: http://info.luminexcorp.com/xmap-cookbook-2nd-edition-free-download (accessed on 10 September 2015).
- Waterboer, T.; Sehr, P.; Pawlita, M. Suppression of non-specific binding in serological Luminex assays. J. Immunol. Methods 2006, 309, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Bolstad, N.; Warren, D.J.; Nustad, K. Heterophilic antibody interference in immunometric assays. Best. Pract. Res. Clin. Endocrinol. Metab 2013, 27, 647–661. [Google Scholar] [CrossRef] [PubMed]
- Amarasiri Fernando, S.; Wilson, G.S. Studies of the 'hook' effect in the one-step sandwich immunoassay. J. Immunol. Methods 1992, 151, 47–66. [Google Scholar] [CrossRef]
- Wagner, K.S.; White, J.M.; Lucenko, I.; Mercer, D.; Crowcroft, N.S.; Neal, S.; Efstratiou, A. Diphtheria in the postepidemic period, Europe, 2000–2009. Emerg. Infect. Dis. 2012, 18, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Detemmerman, L.; Rousseaux, D.; Efstratiou, A.; Schirvel, C.; Emmerechts, K.; Wybo, I.; Soetens, O.; Pierard, D. Toxigenic Corynebacterium ulcerans in human and non-toxigenic Corynebacterium diphtheriae in cat. New Microbes. New Infect. 2013, 1, 18–19. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Rapid risk assessment: A fatal case of diphtheria in Belgium. Available online: http://ecdc.europa.eu/en/publications/_layouts/forms/Publication_DispForm.aspx?List=4f55ad51-4aed-4d32-b960-af70113dbb90&ID=1458 (accessed on 4 May 2016).
- WHO. Immunization, Vaccines and Biologicals: Pertussis. 2014. Available online: http://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/passive/pertussis/en/ (accessed on 14 October 2015).
- Crowcroft, N.S.; Pebody, R.G. Recent developments in pertussis. Lancet 2006, 367, 1926–1936. [Google Scholar] [CrossRef]
- Crowcroft, N.S.; Stein, C.A.; Duclos, P.; Birmingham, M. How best to estimate the global burden of pertussis? Lancet Infect. Dis 2003, 3, 413–418. [Google Scholar] [CrossRef]
- Van der Zee, A.; Schellekens, J.F.; Mooi, F.R. Laboratory Diagnosis of Pertussis. Clin. Microbiol. Rev. 2015, 28, 1005–1026. [Google Scholar] [CrossRef] [PubMed]
- Baughman, A.L.; Bisgard, K.M.; Edwards, K.M.; Guris, D.; Decker, M.D.; Holland, K.; Meade, B.D.; Lynn, F. Establishment of diagnostic cutoff points for levels of serum antibodies to pertussis toxin, filamentous hemagglutinin, and fimbriae in adolescents and adults in the United States. Clin. Diagn. Lab. Immunol. 2004, 11, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Guiso, N.; Berbers, G.; Fry, N.K.H.Q.; Riffelmann, M.; Wirsing von König, C.H. EU Pertstrain group, What to do and what not to do in serological diagnosis of pertussis: Recommendations from EU reference laboratories. Eur J. Clin Microbiol. Infect. Dis. 2011, 30, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Wirsing von Konig, C.H. Pertussis diagnostics: Overview and impact of immunization. Expert. Rev.Vaccines 2014, 13, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- De Greeff, S.C.; de Melker, H.E.; van Gageldonk, P.G.M.; Schellekens, J.F.P.; van der Klis, F.R.M.; Mollema, L.; Mooi, F.; Berbers, G.A.M. Seroprevalence of Pertussis in the Netherlands: Evidence for Increased Circulation of Bordetella pertussis. PLoS ONE 2010, 5, e14183. [Google Scholar] [CrossRef] [PubMed]
- Teepe, J.; Broekhuizen, B.; Ieven, M.; Loens, K.; Huygen, K.; Kretzschmar, M.; de Melker, E.; Butler, C.L.P.; Stuart, B.; Coenen, S.G.V.T. Prevalence, diagnosis and disease course of pertussis in adults with acute cough in primary care. Br. J. General Pract. 2015, 65, e662–e667. [Google Scholar] [CrossRef] [PubMed]
- Braeye, T.; De Schrijver, K.; Piérard, D.; Huygen, K. Kinkhoest. In Infectieziekten bij kinderen die voorkomen kunnen worden door vaccinatie.Trends en Ontwikkelingen in België en de Gemeenschappen. 2012; Wetenschappelijk Instituut Volksgezondheid: Brussels, Belgium, 2014; pp. 23–32. (In Dutch) [Google Scholar]
- Barkoff, A.M.; Grondahl-Yli-Hannuksela, K.; He, Q. Seroprevalence studies of pertussis: what have we learned from different immunized populations. Pathog.Dis. 2015. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.; van der Sande, M.; Faye-Joof, T.; Mendy, M.; Sanneh, B.; Barry, J.F.; de Melker, H.; van der Klis, F.; van Gageldonk, P.; Mooi, F.; et al. Seroprevalence of pertussis in the Gambia: evidence for continued circulation of bordetella pertussis despite high vaccination rates. Pediatr. Infect. Dis. J. 2015, 34, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Hallander, H.O.; Ljungman, M.; Storsaeter, J.; Gustafsson, L. Kinetics and sensitivity of ELISA IgG pertussis antitoxin after infection and vaccination with Bordetella pertussis in young children. APMIS Authors J. Compil. 2009, 117, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Xing, D.; Markey, K.; Newland, P.; Rigsby, P.; Hockley, J.; He, Q. EUVAC.NET collaborative study: evaluation and standardisation of serology for diagnosis of pertussis. J. Immunol. Methods 2011, 372, 137–145. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analyte | LLOD (IU/mL) | Intra-Assay (CV%) | Inter-Assay (CV%) |
|---|---|---|---|
| Prn | 0.2 | 2.15 | 2.38 |
| FHA | 0.032 | 2.47 | 2.60 |
| PT | 0.012 | 1.97 | 2.67 |
| DT | 0.00031 | 1.45 | 2.37 |
| TT | 0.00035 | 0.44 | 2.11 |
| Antigen | age (year) | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | Adjusted |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 29 | 50 | 54 | 63 | 70 | 77 | 64 | 92 | 110 | 61 | ||
| DT | GMC | 0.28 | 0.24 | 0.19 | 0.28 | 0.22 | 0.21 | 0.18 | 0.17 | 0.14 | 0.17 | 0.20 |
| Lower 95% CI | 0.16 | 0.16 | 0.12 | 0.19 | 0.15 | 0.15 | 0.12 | 0.12 | 0.10 | 0.11 | 0.13 | |
| Upper 95% CI | 0.49 | 0.37 | 0.31 | 0.41 | 0.32 | 0.30 | 0.27 | 0.24 | 0.18 | 0.28 | 0.29 | |
| TT | GMC | 0.91 | 0.50 | 0.51 | 0.61 | 0.64 | 0.69 | 0.75 | 0.56 | 0.64 | 0.49 | 0.63 |
| Lower 95% CI | 0.58 | 0.31 | 0.32 | 0.44 | 0.46 | 0.53 | 0.55 | 0.42 | 0.50 | 0.32 | 0.45 | |
| Upper 95% CI | 1.43 | 0.80 | 0.82 | 0.85 | 0.89 | 0.91 | 1.03 | 0.75 | 0.81 | 0.73 | 0.87 | |
| PT | GMC | 3.7 | 3.7 | 2.7 | 4.2 | 2.4 | 4.5 | 3.9 | 4.1 | 4.4 | 3.8 | 3.9 |
| Lower 95% CI | 1.9 | 2.4 | 1.6 | 2.9 | 1.6 | 3.1 | 2.6 | 3.1 | 3.1 | 2.4 | 2.6 | |
| Upper 95% CI | 7.5 | 5.9 | 4.5 | 6.0 | 3.8 | 6.7 | 5.9 | 5.6 | 6.3 | 6.2 | 5.8 | |
| FHA | GMC | 15.8 | 12.5 | 15.4 | 14.7 | 17.0 | 18.8 | 16.5 | 16.4 | 15.6 | 18.3 | 16.3 |
| Lower 95% CI | 8.1 | 8.5 | 10.1 | 10.8 | 12.2 | 14.2 | 12.0 | 12.2 | 12.3 | 12.8 | 11.7 | |
| Upper 95% CI | 30.8 | 18.3 | 23.4 | 20.0 | 23.8 | 24.9 | 22.6 | 22.1 | 19.8 | 26.2 | 22.7 | |
| Prn | GMC | 13.2 | 11.6 | 9.7 | 18.1 | 13.9 | 23.4 | 18.1 | 11.3 | 16.9 | 13.9 | 15.4 |
| Lower 95% CI | 6.3 | 7.3 | 5.9 | 11.3 | 9.5 | 15.8 | 12.1 | 7.8 | 12.0 | 8.4 | 10.1 | |
| Upper 95% CI | 27.8 | 18.5 | 15.8 | 29.1 | 20.4 | 34.8 | 27.2 | 16.5 | 23.8 | 23.0 | 23.6 |
| Antigen | IgG titer | E Flanders | W Flanders | Liège | Hainaut | Brussel | Bruxelles | Adjusted % |
|---|---|---|---|---|---|---|---|---|
| n | 120 | 127 | 122 | 61 | 123 | 116 | ||
| Diphtheria | <0.1 IU/mL | 26 (22%) | 23 (18%) | 38 (31%) | 18 (29%) | 48 (39%) | 60 (52%) | 26.4 |
| Tetanus | <0.1 IU/mL | 10 (8.3%) | 3 (2.4%) | 12 (9.8%) | 6 (9.8%) | 14 (11.4%) | 34 (29.3% | 8.6 |
| Pertussis (PT) | >50 IU/mL | 8 (6.7%) | 13 (10.2%) | 4 (3.2%) | 8 (13.1%) | 6 (4.8%) | 7 (6.0%) | 8 |
| GMC | DT | TT | PT | FHA | Prn |
|---|---|---|---|---|---|
| GMC A (n = 38) | 0.34 | 1.06 | 74.9 | 64.4 | 66.4 |
| Lower 95% CI | 0.19 | 0.71 | 68.3 | 45.1 | 33.1 |
| Upper 95% CI | 0.59 | 1.59 | 82.2 | 91.9 | 133 |
| GMC B (n = 8) | 0.41 | 1.52 | 172 | 116 | 161 |
| Lower 95% CI | 0.17 | 0.74 | 135 | 53.4 | 38.4 |
| Upper 95% CI | 0.98 | 3.13 | 219 | 251 | 674 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caboré, R.N.; Piérard, D.; Huygen, K. A Belgian Serosurveillance/Seroprevalence Study of Diphtheria, Tetanus and Pertussis Using a Luminex xMAP Technology-Based Pentaplex. Vaccines 2016, 4, 16. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines4020016
Caboré RN, Piérard D, Huygen K. A Belgian Serosurveillance/Seroprevalence Study of Diphtheria, Tetanus and Pertussis Using a Luminex xMAP Technology-Based Pentaplex. Vaccines. 2016; 4(2):16. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines4020016
Chicago/Turabian StyleCaboré, Raissa Nadège, Denis Piérard, and Kris Huygen. 2016. "A Belgian Serosurveillance/Seroprevalence Study of Diphtheria, Tetanus and Pertussis Using a Luminex xMAP Technology-Based Pentaplex" Vaccines 4, no. 2: 16. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines4020016