Yellow Fever Virus Genotyping Tool and Investigation of Suspected Adverse Events Following Yellow Fever Vaccination

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Clinical Samples
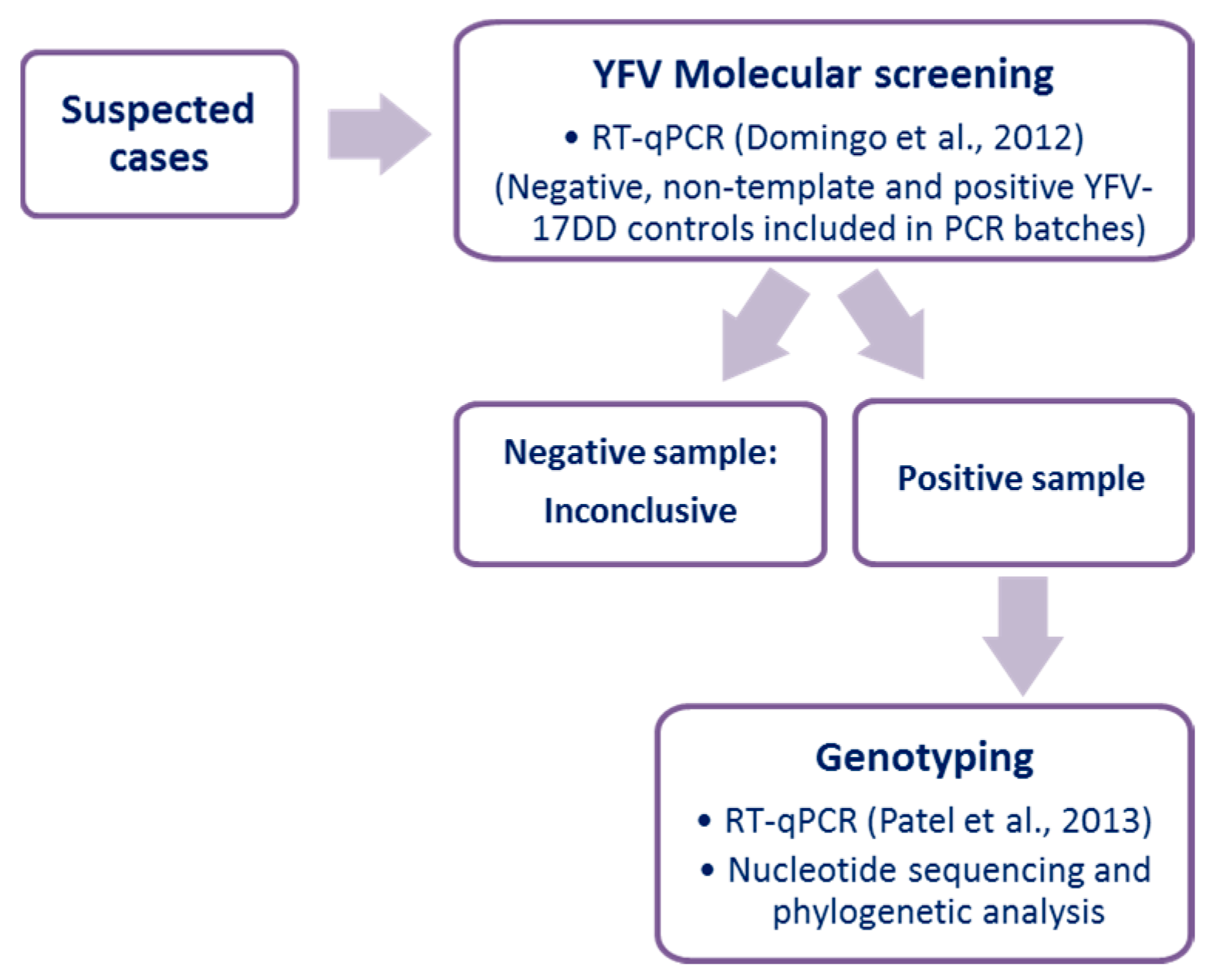
2.2. Yellow Fever Virus Molecular Screening
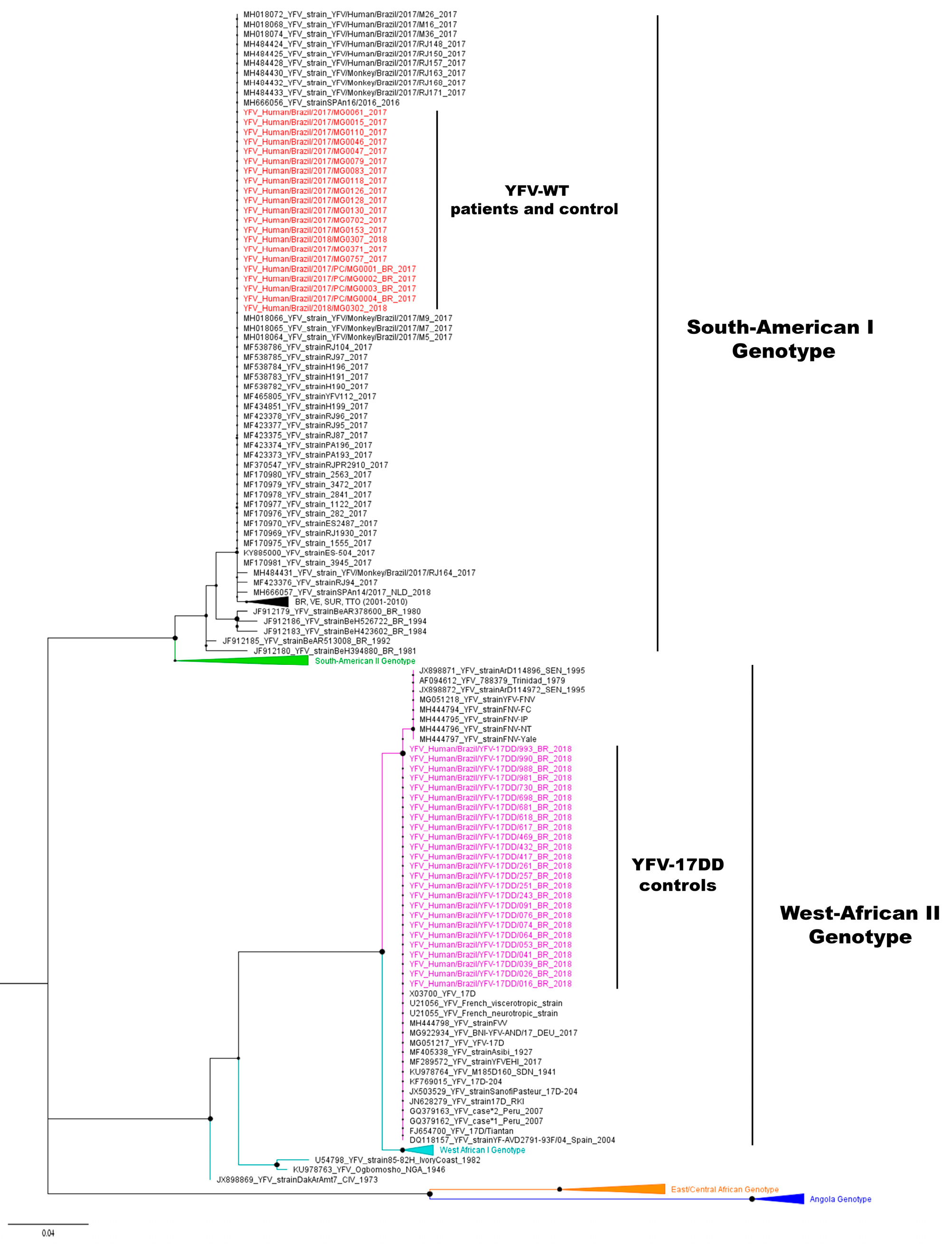
2.3. Yellow Fever Virus Genotyping
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- ICTV International Committee on Taxonomy of Viruses. Available online: https://talk.ictvonline.org/taxonomy/ (accessed on 20 June 2019).
- Monath, T.P.; Vasconcelos, P.F.C. Yellow fever. J. Clin. Virol. 2015, 64, 160–173. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, P.F.D.C. Yellow fever in Brazil: thoughts and hypotheses on the emergence in previously free areas. Rev. Saude Publica 2010, 44, 1144–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theiler, M.; Smith, H. The use of yellow fever virus modified by in vitro cultivation for human immunization. J. Exp. Med. 1937, 65, 787–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Weekly Epidemiological Record: Vaccines and Vaccination against Yellow Fever. WHO Position Paper—June 2013. Available online: https://www.who.int/wer/2013/wer8827.pdf?ua=1&ua=1 (accessed on 3 October 2019).
- Monath, T.P. Yellow fever vaccine. Expert Rev. Vaccines 2005, 4, 553–574. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Detection and Investigation of Serious Adverse Events Following Yellow Fever Vaccination; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Porudominsky, R.; Gotuzzo, E.H. Yellow fever vaccine and risk of developing serious adverse events: a systematic review. Rev. Panam. Salud Pública 2018, 42, e75. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Surveillance of Adverse Events Following Immunization against Yellow Fever; WHO: Geneva, Switzerland, 2010; pp. 1–72. [Google Scholar]
- Ministério da Saúde. Manual de Vigilância Epidemiológica de Eventos Adversos Pós-Vacinação, 3rd ed.; Ministério da Saúde: Brasília, Brazil, 2014; ISBN 9788533421752.
- SES-MG Febre Amarela Silvestre em Minas Gerais. Available online: http://www.saude.mg.gov.br/images/noticias_e_eventos/000_2018/BoletinsEpidemiologicos/Boletim_-_Febre_Amarela_2018_-_Consolidado_V3.pdf (accessed on 10 October 2019).
- Poland, J.D.; Calisher, C.H.; Monath, T.P.; Downs, W.G.; Murphy, K. Persistence of neutralizing antibody 30–35 years after immunization with 17D yellow fever vaccine. Bull. World Health Organ. 1981, 59, 895–900. [Google Scholar]
- Caldas, I.R.; Camacho, L.A.; Martins-Filho, O.A.; Maia Mde, L.; Freire Mda, S.; Torres Cde, R.; Martins Rde, M.; Homma, A.; Farias, R.H.; Yoshida, A.M.; et al. Duration of post-vaccination immunity against yellow fever in adults. Vaccine 2014, 32, 4977–4984. [Google Scholar]
- Costa-Pereira, C.; Campi-Azevedo, A.C.; Coelho-Dos-Reis, J.G.; Peruhype-Magalhaes, V.; Araujo, M.S.S.; do Vale Antonelli, L.R.; Fonseca, C.T.; Lemos, J.A.; Malaquias, L.C.C.; de Souza Gomes, M.; et al. Multi-parameter approach to evaluate the timing of memory status after 17DD-YF primary vaccination. PLoS Negl. Trop. Dis. 2018, 12, e0006462. [Google Scholar] [CrossRef]
- Campi-Azevedo, A.C.; Costa-Pereira, C.; Antonelli, L.R.; Fonseca, C.T.; Teixeira-Carvalho, A.; Villela-Rezende, G.; Santos, R.A.; Batista, M.A.; Campos, F.M.; Pacheco-Porto, L.; et al. Booster dose after 10 years is recommended following 17DD-YF primary vaccination. Hum. Vaccines Immunother. 2016, 12, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Fischer, C.; Torres, M.C.; Patel, P.; Moreira-Soto, A.; Gould, E.A.; Charrel, R.N.; de Lamballerie, X.; Nogueira, R.M.R.; Sequeira, P.C.; Rodrigues, C.D.S.; et al. Lineage-Specific Real-Time RT-PCR for Yellow Fever Virus Outbreak Surveillance, Brazil. Emerg. Infect. Dis. 2017, 23, 1867–1871. [Google Scholar] [CrossRef]
- Faria, N.R.; Kraemer, M.U.G.; Hill, S.C.; De Jesus, J.G.; Aguiar, R.S.; Iani, F.C.M.; Xavier, J.; Quick, J.; Du Plessis, L.; Dellicour, S.; et al. Genomic and epidemiological monitoring of yellow fever virus transmission potential. Science 2018, 361, 894–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soper, F.L. Febre amarela panamericana, 1938–1942. Pan Am. J. Public Health 1942, 1207–1222. [Google Scholar]
- MS-BR Monitoramento do Período Sazonal da Febre Amarela Brasil, 2018/2019. Available online: https://portalarquivos2.saude.gov.br/images/pdf/2019/janeiro/28/informe-FA-n.3-21jan19.pdf (accessed on 3 October 2019).
- MS-BR Monitoramento do Período Sazonal da Febre Amarela Brasil, 2017/2018. Available online: https://portalarquivos2.saude.gov.br/images/pdf/2018/outubro/08/Informe-FA.pdf (accessed on 10 October 2019).
- MS-BR Monitoramento do Período Sazonal da Febre Amarela Brasil, 2016/2017. Available online: http://portalarquivos.saude.gov.br/images/pdf/2017/junho/02/COES-FEBRE-AMARELA---INFORME-43---Atualiza----o-em-31maio2017.pdf (accessed on 10 October 2019).
- SES-MG Febre Amarela Silvestre em Minas Gerais. Available online: http://www.saude.mg.gov.br/images/noticias_e_eventos/000_2018/BoletinsEpidemiologicos/Boletim_-_Febre_Amarela_06_12_Finalizado.pdf (accessed on 3 October 2019).
- SES-MG Eventos Adversos Pós-Vacinação Associados à Vacina Febre Amarela (EAPV-VFA) Minas Gerais, 2016 a 2018. Available online: http://www.saude.mg.gov.br/images/noticias_e_eventos/000_2018/BoletinsEpidemiologicos/Boletim_epidemiológico_EAPV_finalv3.pdf (accessed on 10 October 2019).
- Domingo, C.; Patel, P.; Yillah, J.; Weidmann, M.; Mendez, J.A.; Nakoune, E.R.; Niedrig, M. Advanced Yellow Fever Virus Genome Detection in Point-of-Care Facilities and Reference Laboratories. J. Clin. Microbiol. 2012, 50, 4054–4060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, P.; Landt, O.; Kaiser, M.; Faye, O.; Koppe, T.; Lass, U.; Sall, A.A.; Niedrig, M. Development of one-step quantitative reverse transcription PCR for the rapid detection of flaviviruses. Virol. J. 2013, 10, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Stecher, G.; Tamura, K. MEGA7: Molecular Evolutionary Genetics Analysis Version 7.0 for Bigger Datasets. Mol. Biol. Evol. 2016, 33, 1870–1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darriba, D.; Taboada, G.L.; Doallo, R.; Posada, D. jModelTest 2: More models, new heuristics and parallel computing. Nat. Methods 2012, 9, 772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drummond, A.J.; Suchard, M.A.; Xie, D.; Rambaut, A. Bayesian Phylogenetics with BEAUti and the BEAST 1.7. Mol. Biol. Evol. 2012, 29, 1969–1973. [Google Scholar] [CrossRef] [Green Version]
- Baele, G.; Lemey, P.; Bedford, T.; Rambaut, A.; Suchard, M.A.; Alekseyenko, A.V. Improving the Accuracy of Demographic and Molecular Clock Model Comparison While Accommodating Phylogenetic Uncertainty. Mol. Biol. Evol. 2012, 29, 2157–2167. [Google Scholar] [CrossRef] [Green Version]
- Rambaut, A.; Drummond, A.J.; Xie, D.; Baele, G.; Suchard, M.A. Posterior Summarization in Bayesian Phylogenetics Using Tracer 1.7. Syst. Biol. 2018, 67, 901–904. [Google Scholar] [CrossRef] [Green Version]
- Rambaut, A.; Drummond, A.J. TreeAnnotator. 2015. Available online: https://beast.community/treeannotator (accessed on 15 March 2019).
- Holford, N.C.; Sandhu, H.S.; Thakkar, H.; Butt, A.N.; Swaminathan, R. Stability of β-actin mRNA in plasma. Ann. N. Y. Acad. Sci. 2008, 1137, 108–111. [Google Scholar] [CrossRef]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanger, F.; Nicklen, S. DNA sequencing with chain-terminating inhibitors. Proc. Natl. Acad. Sci. USA 1977, 74, 5463–5467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, A.T.; Derome, N.; Boyle, B.; Culley, A.I.; Charette, S.J. Next-generation sequencing (NGS) in the microbiological world: How to make the most of your money. J. Microbiol. Methods 2017, 138, 60–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Eliminate Yellow Fever Epidemics by 2026; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- PAHO Control of Yellow Fever. Field Guide. Available online: http://www.paho.org/immunization/toolkit/resources/paho-publication/field-guides/Control-of-Yellow-Fever.pdf?ua=1 (accessed on 16 October 2019).



{kind=link}
{kind=link}
| ID | Age | Gender | Day of YFV-17DD Vaccination | Day of Onset of Disease | Tested Sample | GT | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Days After | RT-qPCR (Target Region) | IgM | ||||||||
| Symptoms | Vaccination | 5′-UTR 1 | NS5 2 | |||||||
| 1 | 57 | M | 23/1/17 | 23/1/17 | 3 | 3 | Positive | Positive | N/A | WT |
| 2 | 15 | M | 19/1/17 | 20/1/17 | 3 | 4 | Positive | Positive | N/A | WT |
| 3 | 38 | F | 13/1/17 | 13/1/17 | 7 | 7 | Positive | Positive | Positive | WT |
| 4 | 49 | F | 23/1/17 | 23/1/17 | 4 | 4 | Positive | Positive | N/A | WT |
| 5 | 51 | M | 14/1/18 | 16/1/18 | 2 | 4 | Positive | Positive | Negative | WT |
| 6 | 61 | M | 15/1/18 | 15/1/18 | 2 | 2 | Positive | Positive | Negative | WT |
| 7 | 22 | M | 23/1/17 | 23/1/17 | 5 | 5 | Positive | Positive | N/A | WT |
| 8 | 39 | M | 16/1/17 | 16/1/17 | 3 | 3 | Positive | Positive | N/A | WT |
| 9 | 42 | M | 16/1/17 | 17/1/17 | 3 | 4 | Positive | Positive | N/A | WT |
| 10 | 36 | F | 10/1/17 | 18/1/17 | 5 | 14 | Positive | Positive | Positive | WT |
| 11 | 37 | F | 13/1/17 | 23/1/17 | 5 | 16 | Positive | Positive | Negative | WT |
| 12 | 33 | F | 16/1/17 | 22/1/17 | 5 | 12 | Positive | Positive | Negative | WT |
| 13 | 34 | M | 20/1/17 | 21/117 | 6 | 8 | Positive | Positive | Positive | WT |
| 14 | 62 | F | 14/1/17 | 17/1/17 | 5 | 9 | Positive | Positive | Negative | WT |
| 15 | 57 | M | 20/1/17 | 21/1/17 | 8 | 9 | Positive | Positive | N/A | WT |
| 16 | 60 | M | 10/1/17 | 22/1/17 | 3 | 16 | Positive | Positive | Negative | WT |
| 17 | 42 | M | 15/1/17 | 17/1/17 | 6 | 9 | Positive | Positive | Negative | WT |
| 18 | 27 | M | 12/1/17 | 16/1/17 | 7 | 11 | Positive | Negative | N/A | N/A |
| 19 | 40 | M | 19/1/17 | 21/1/17 | 1 | 2 | Positive | Negative | N/A | N/A |
| 20* | 48 | F | 14/1/17 | 18/1/17 | 7 | 12 | Negative | Negative | Negative | N/A |
| 21** | 32 | F | 14/1/17 | 25/1/17 | 4 | 16 | Negative | Negative | Negative | N/A |
| 22 | 47 | M | 16/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 23 | 54 | F | 16/2/18 | N/A | N/A | 6 | Positive | Positive | N/A | 17DD |
| 24 | 45 | F | 23/2/18 | N/A | N/A | 6 | Positive | Positive | N/A | 17DD |
| 25 | 48 | M | 23/2/18 | N/A | N/A | 4 | Positive | Positive | N/A | 17DD |
| 26 | 26 | F | 21/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 27 | 42 | F | 28/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 28 | 45 | F | 22/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 29 | 75 | M | 23/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 30 | 42 | M | 23/3/18 | N/A | N/A | 6 | Positive | Positive | N/A | 17DD |
| 31 | 51 | M | 26/2/18 | N/A | N/A | 8 | Positive | Positive | N/A | 17DD |
| 32 | 16 | F | 21/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 33 | 58 | F | 21/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 34 | 7 | M | 21/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 35 | 65 | M | 15/2/18 | N/A | N/A | 4 | Positive | Positive | N/A | 17DD |
| 36 | 24 | M | 16/2/18 | N/A | N/A | 4 | Positive | Positive | N/A | 17DD |
| 37 | 50 | M | 19/2/18 | N/A | N/A | 4 | Positive | Positive | N/A | 17DD |
| 38 | 54 | M | 1/3/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 39 | 39 | F | 1/3/18 | N/A | N/A | 6 | Positive | Positive | N/A | 17DD |
| 40 | 59 | F | 5/3/18 | N/A | N/A | 4 | Positive | Positive | N/A | 17DD |
| 41 | 55 | M | 9/3/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 42 | 60 | M | 19/3/18 | N/A | N/A | 1 | Positive | Positive | N/A | 17DD |
| 43 | 62 | M | 19/2/18 | N/A | N/A | 4 | Positive | Positive | N/A | 17DD |
| 44 | 48 | M | 23/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 45 | 55 | M | 21/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 46 | 28 | M | 22/2/18 | N/A | N/A | 5 | Positive | Positive | N/A | 17DD |
| 47 | 31 | M | N/A | 6/1/18 | 4 | N/A | Positive | Positive | N/A | WT |
| 48 | 41 | M | N/A | 10/1/18 | 7 | N/A | Positive | Positive | N/A | WT |
| 49 | 65 | M | N/A | 13/1/18 | 4 | N/A | Positive | Positive | N/A | WT |
| 50 | 62 | M | N/A | 15/1/18 | 3 | N/A | Positive | Positive | N/A | WT |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rezende, I.M.d.; Alves, P.A.; Arruda, M.S.; Gonçalves, A.P.; Oliveira, G.F.G.; Pereira, L.S.; Dutra, M.R.T.; Campi-Azevedo, A.C.; Valim, V.; Tourinho, R.; et al. Yellow Fever Virus Genotyping Tool and Investigation of Suspected Adverse Events Following Yellow Fever Vaccination. Vaccines 2019, 7, 206. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines7040206
Rezende IMd, Alves PA, Arruda MS, Gonçalves AP, Oliveira GFG, Pereira LS, Dutra MRT, Campi-Azevedo AC, Valim V, Tourinho R, et al. Yellow Fever Virus Genotyping Tool and Investigation of Suspected Adverse Events Following Yellow Fever Vaccination. Vaccines. 2019; 7(4):206. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines7040206
Chicago/Turabian StyleRezende, Izabela Maurício de, Pedro Augusto Alves, Matheus Soares Arruda, Andreza Parreiras Gonçalves, Gabriela Fernanda Garcia Oliveira, Leonardo Soares Pereira, Maria Rita Teixeira Dutra, Ana Carolina Campi-Azevedo, Valéria Valim, Renata Tourinho, and et al. 2019. "Yellow Fever Virus Genotyping Tool and Investigation of Suspected Adverse Events Following Yellow Fever Vaccination" Vaccines 7, no. 4: 206. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines7040206