Evaluation of the Burden of HPV-Related Hospitalizations as a Useful Tool to Increase Awareness: 2007–2017 Data from the Sicilian Hospital Discharge Records

 ,
,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
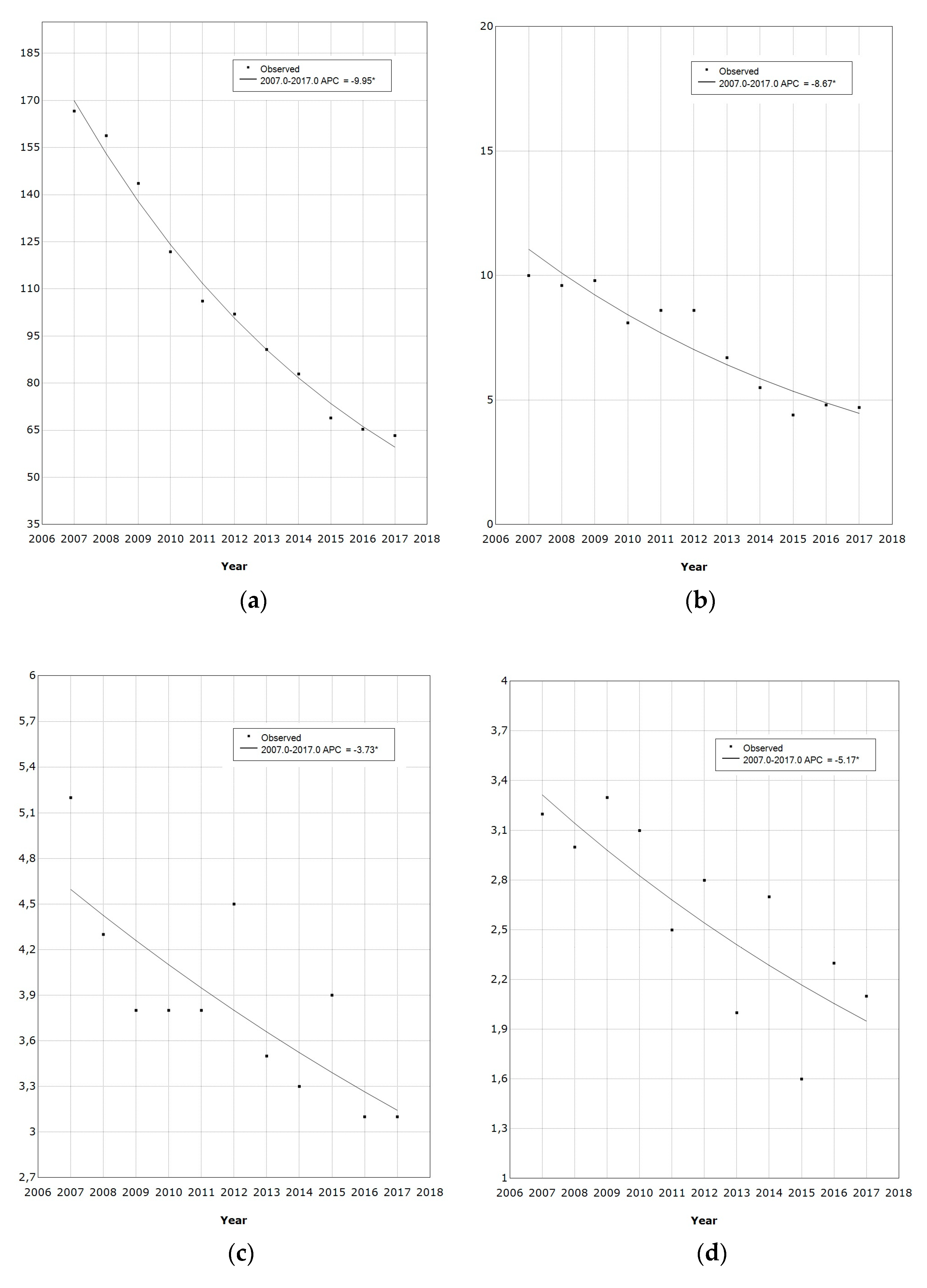
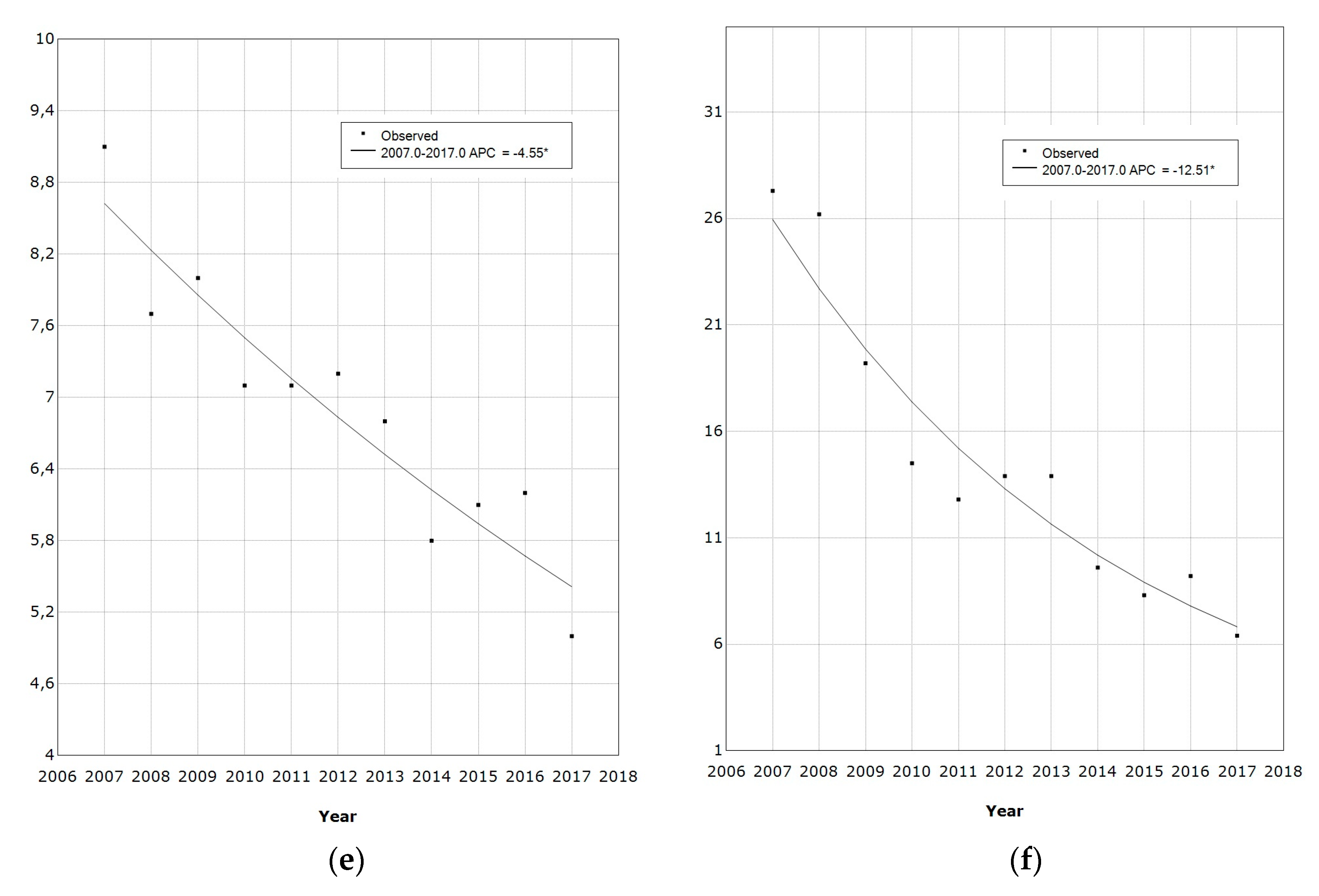
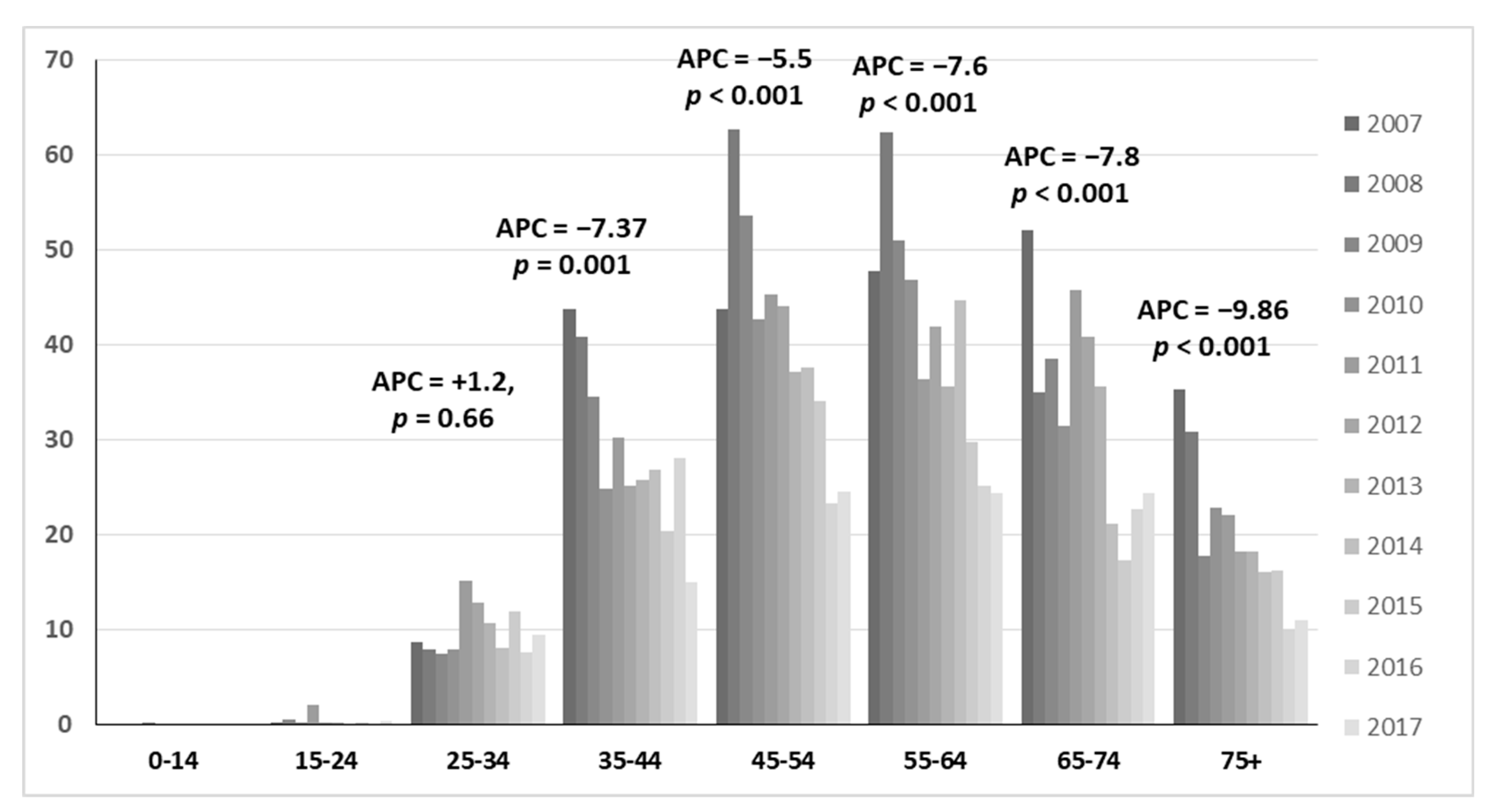
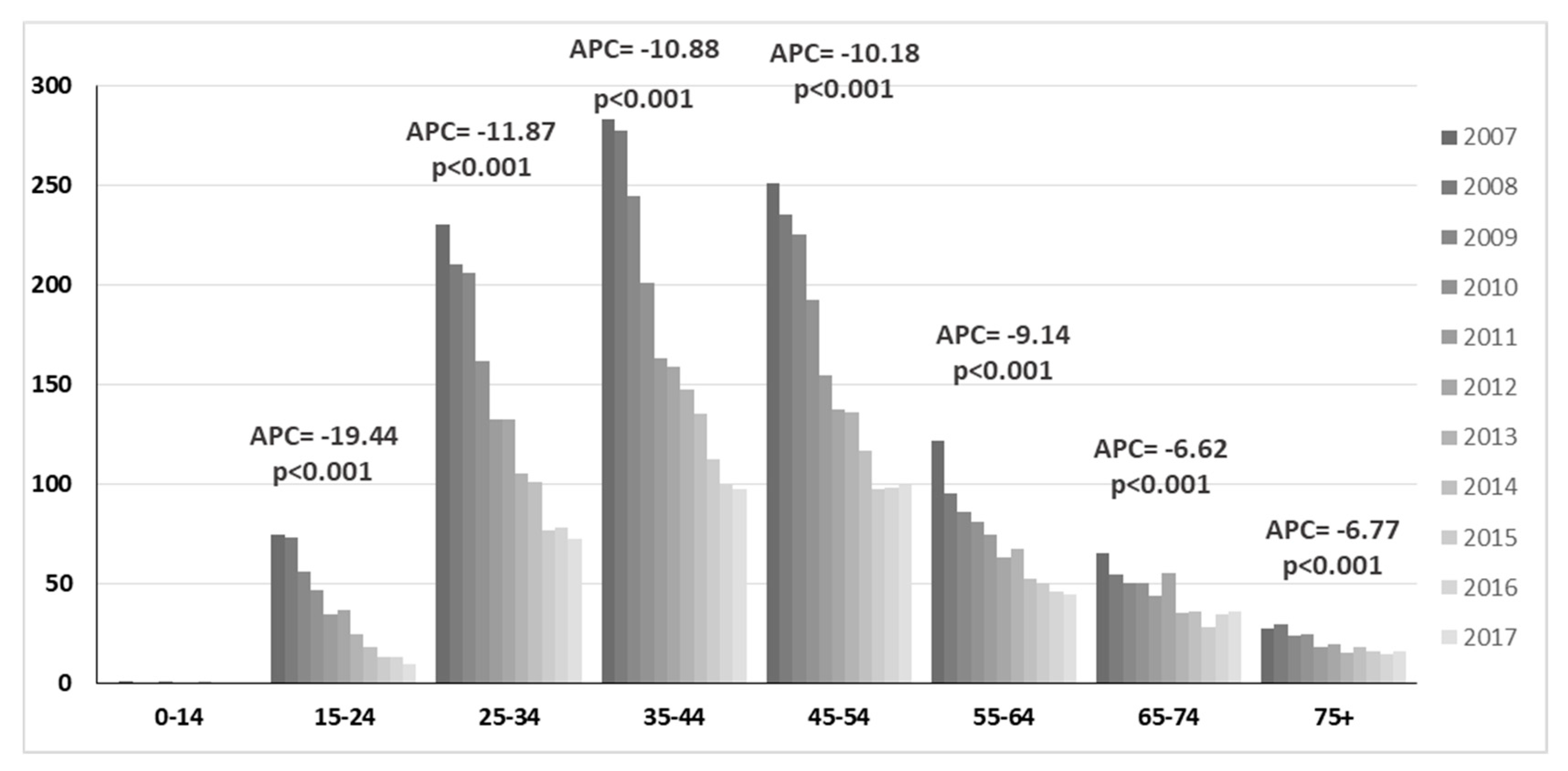
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chauhan, S.C.; Jaggi, M.; Bell, M.C.; Verma, M.; Kumar, D. Epidemiology of Human Papilloma Virus (HPV) in Cervical Mucosa. Methods Mol. Biol. 2009, 471, 439–456. [Google Scholar]
- Baseman, J.G.; Koutsky, L.A. The epidemiology of human papillomavirus infections. J. Clin. Virol. 2005, 32 (Suppl. 1), S16–S24. [Google Scholar] [CrossRef]
- Schiffman, M.; Herrero, R.; Desalle, R.; Hildesheim, A.; Wacholder, S.; Rodriguez, A.C.; Bratti, M.C.; Sherman, M.E.; Morales, J.; Guillen, D.; et al. The carcinogenicity of human papillomavirus types reflects viral evolution. Virology 2005, 337, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, H.; Wagner, M.; Singhal, P.; Kothari, S. Systematic review of the incidence and prevalence of genital warts. BMC Infect. Dis. 2013, 13, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortes, H.R.; von Ranke, F.M.; Escuissato, D.L.; Araujo Neto, C.A.; Zanetti, G.; Hochhegger, B.; Souza, C.A.; Marchiori, E. Recurrent respiratory papillomatosis: A state-of-the-art review. Respir. Med. 2017, 126, 116–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plummer, M.; de Martel, C.; Vignat, J.; Ferlay, J.; Bray, F.; Franceschi, S. Global burden of cancers attributable to infections in 2012: A synthetic analysis. Lancet Glob. Health 2016, 4, e609–e616. [Google Scholar] [CrossRef] [Green Version]
- De Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Hartwig, S.; Baldaufb, J.J.; Dominiak-Felden, G.; Simondon, F.; Alemany, L.; De Sanjosé, S.; Castellsagué, X. Estimation of the epidemiological burden of HPV-related anogenital cancers, precancerous lesions, and genital warts in women and men in Europe: Potential additional benefit of a nine-valent second generation HPV vaccine compared to first generation HPV vaccines. Papillomavirus Res. 2015, 1, 90–100. [Google Scholar]
- Villa, L.L.; Costa, R.L.; Petta, C.A.; Andrade, R.P.; Ault, K.A.; Giuliano, A.R.; Wheeler, C.M.; Koutsky, L.A.; Malm, C.; Lehtinen, M.; et al. Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in young women: A randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol. 2005, 6, 271–278. [Google Scholar] [CrossRef]
- Brotherton, J.M.; Fridman, M.; May, C.L.; Chappell, G.; Saville, A.M.; Gertig, D.M. Early effect of the HPV vaccination programme on cervical abnormalities in Victoria, Australia: An ecological study. Lancet 2011, 377, 2085–2092. [Google Scholar] [CrossRef]
- Gil-Prieto, R.; Ester, P.V.; Alvaro-Meca, A.; Rodríguez, M.S.; De Miguel, A.G. The burden of hospitalizations for anus and penis neoplasm in Spain (1997–2008). Hum. Vaccines Immunother. 2012, 8, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministero Della Salute. Coperture Vaccinali al 31/12/2017 HPV. Available online: http://www.salute.gov.it/imgs/C_17_tavole_27_allegati_iitemAllegati_0_fileAllegati_itemFile_1_file.pdf (accessed on 15 December 2019).
- Assessorato Alla Salute, Regione Sicilia. Adeguamento del Calendario Vaccinale Regionale al “Piano Nazionale di Prevenzione Vaccinale 2017–2019”, Recepito Dalla Regione Sicilia con il D.A. n. 1004 del 22 Maggio 2017. Available online: http://www.gurs.regione.sicilia.it/Gazzette/g17-49/g17-49.pdf (accessed on 15 December 2019).
- Peirson, L.; Fitzpatrick-Lewis, D.; Ciliska, D.; Warren, R. Screening for cervical cancer: A systematic review and meta-analysis. Syst. Rev. 2013, 2, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, G.; Dillner, J.; Elfström, K.M.; Tunesi, S.; Snijders, P.; Arbyn, M.; Kitchener, H.; Segnan, N.; Gilham, C.; Giorgi-Rossi, P.; et al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: Follow-up of four European randomised controlled trials. Lancet 2014, 383, 524–532. [Google Scholar] [CrossRef]
- Ministero Della Salute. Linee di Guida, in Applicazione di Quanto Previsto nel Piano Sanitario Nazionale per il Triennio1994–1996, Relativo All’azione Programmata: “Prevenzione e Cura Delle Malattie Oncologiche” Concernente: L’organizzazione Della Prevenzione e Della Assistenza. in Oncologia. Available online: https://www.gazzettaufficiale.it/atto/vediMenuHTML?atto.dataPubblicazioneGazzetta=1996-02-20&atto.codiceRedazionale=096A1067&tipoSerie=serie_generale&tipoVigenza=originario (accessed on 26 December 2019).
- D.P.C.M. 29-11-2001. Definizione dei Livelli Essenziali di Assistenza. Available online: http://www.salute.gov.it/imgs/C_17_normativa_1479_allegato.pdf (accessed on 24 December 2019).
- Ministero Della Salute. Ricoveri Ospedalieri (SDO). Available online: http://www.salute.gov.it/portale/temi/p2_4.jsp?area=ricoveriOspedalieri (accessed on 15 December 2019).
- Kuhdari, P.; Previato, S.; Giordani, M.; Biavati, P.; Ferretti, S.; Gabutti, G. The burden of HPV-related diseases in Italy, 2001–2012. J. Public Health 2017, 39, 730–737. [Google Scholar] [CrossRef]
- Istat. DemoIstat. Available online: http://demo.istat.it/pop2017/index.html (accessed on 15 December 2019).
- Levi, M.; Bellini, I.; Sinisgalli, E.; Sala, A.; Indiani, L.; Bonanni, P. The burden of hospitalization due to HPV infections in Tuscany, Central Italy. Public Health 2016, 141, 194–197. [Google Scholar] [CrossRef]
- Baldo, V.; Cocchio, S.; Buja, A.; Baldovin, T.; Furlan, P.; Bertoncello, C.; Saia, M. Hospitalization for diseases attributable to human papillomavirus in the Veneto Region (North-East Italy). BMC Infect. Dis. 2013, 13, 462. [Google Scholar] [CrossRef]
- Cocchio, S.; Baldovin, T.; Bertoncello, C.; Buja, A.; Furlan, P.; Saia, M.; Baldo, V. Decline in hospitalization for genital warts in the Veneto region after an HPV vaccination program: An observational study. BMC Infect. Dis. 2017, 17, 249. [Google Scholar] [CrossRef] [Green Version]
- Tan, N.; Sharma, M.; Winer, R.; Galloway, D.; Rees, H.; Barnabas, R.V. Model-estimated effectiveness of single dose 9-valent HPV vaccination for HIV-positive and HIV-negative females in South Africa. Vaccine 2018, 36, 4830–4836. [Google Scholar] [CrossRef]
- Brooks, S.E.; Chen, T.T.; Ghosh, A.; Mullins, C.D.; Gardner, J.F.; Baquet, C.R. Cervical cancer outcomes analysis: Impact of age, race, and comorbid illness on hospitalizations for invasive carcinoma of the cervix. Gynecol. Oncol. 2000, 79, 107–115. [Google Scholar] [CrossRef]
- Firenze, A.; Aleo, N.; Ferrara, C.; Maranto, M.; La Cascia, C.; Restivo, V. the occurrence of diseases and related factors in a center for asylum seekers in Italy. Zdr. Varst. 2015, 55, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firenze, A.; Restivo, V.; Bonanno, V.; Aleo, N.; Pace, S.; Marsala, M.G.; Palermo, M. Health status of immigrants arrived to Italian coast. Epidemiol. Prev. 2014, 38 (Suppl. 2), 78–82. [Google Scholar] [PubMed]
- World Health Organization. WHO Director-General Calls for All Countries to Take Action to Help End the Suffering Caused by Cervical Cancer. Available online: https://www.who.int/reproductivehealth/call-to-action-elimination-cervical-cancer/en/ (accessed on 26 December 2019).
- Burger, E.A.; Kim, J.J.; Sy, S.; Castle, P.E. Age of acquiring causal human papillomavirus (HPV) infections: Leveraging simulation models to explore the natural history of HPV-induced cervical cancer. Clin. Infect. Dis. 2017, 65, 893–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drolet, M.; Bernard, E.; Perez, N.; Brisson, M.; HPV Vaccination Impact Study Group. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: Updated systematic review and meta-analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef] [Green Version]
- Luostarinen, T.; Apter, D.; Dillner, J.; Eriksson, T.; Harjula, K.; Natunen, K.; Paavonen, J.; Pukkala, E.; Lehtinen, M. Vaccination protects against invasive HPV-associated cancers. Int. J. Cancer 2018, 142, 2186–2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, T.; Wallace, L.; Pollock, K.G.; Cuschieri, K.; Robertson, C.; Kavanagh, K.; Cruickshank, M. Prevalence of cervical disease at age 20 after immunisation with bivalent HPV vaccine at age 12- 13 in Scotland: Retrospective population study. BMJ 2019, 365, l1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restivo, V.; Costantino, C.; Marras, A.; Napoli, G.; Scelfo, S.; Scuderi, T.; Casuccio, A.; Cernigliaro, A.; Giusti, A.; Spila Alegiani, S. Pap testing high-income country with suboptimal compliance levels: A survey on acceptance factors among Sicilian women. Int. J. Environ. Res. Public Health 2018, 15, 1804. [Google Scholar] [CrossRef] [Green Version]
- Hall, M.T.; Simms, K.T.; Lew, J.B.; Smith, M.A.; Brotherton, J.M.; Saville, M.; Frazer, I.H.; Canfell, K. The projected timeframe until cervical cancer elimination in Australia: A modelling study. Lancet Public Health 2019, 4, e19–e27. [Google Scholar] [CrossRef] [Green Version]
- Amodio, E.; Tramuto, F.; Costantino, C.; Restivo, V.; Maida, C.; Calamusa, G.; Vitale, F. Diagnosis of influenza: Only a problem of coding? Med. Princ. Pract. 2014, 23, 568–573. [Google Scholar] [CrossRef] [Green Version]
- Tabacchi, G.; Costantino, C.; Cracchiolo, M.; Ferro, A.; Marchese, V.; Napoli, G.; Palmeri, S.; Raia, D.; Restivo, V.; Siddu, A.; et al. Information sources and knowledge on vaccination in a population from southern Italy: The ESCULAPIO project. Hum. Vaccines Immunother. 2017, 13, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Restivo, V.; Costantino, C.; Fazio, T.F.; Casuccio, N.; D’Angelo, C.; Vitale, F.; Casuccio, A. Factors associated with HPV vaccine refusal among young adult women after ten years of vaccine implementation. Int. J. Environ. Res. Public Health 2018, 15, 770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restivo, V.; Orsi, A.; Ciampini, S.; Messano, G.A.; Trucchi, C.; Ventura, G.; Casuccio, A.; Vitale, F. How should vaccination services be planned, organized, and managed? Results from a survey on the Italian vaccination services. Ann. Ig. 2019, 31 (Suppl. 1), 45–53. [Google Scholar]
- Ministero Della Salute. Decreto 09 Dicembre 2015 Condizioni di Erogabilità e Indicazioni di Appropriatezza Prescrittiva Delle Prestazioni di Assistenza Ambulatoriale Erogabili Nell’ambito del Servizio Sanitario Nazionale. Available online: http://www.trovanorme.salute..gov.it/norme/dettaglioAtto?id=53949&completo=true (accessed on 26 December 2019).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Cervical Cancer Rate (SD) | Oropharynx Rate (SD) | Anus Rate (SD) | Penis Rate (SD) | Vulva and Vagina Rate (SD) | Genital Warts Rate (SD) |
|---|---|---|---|---|---|---|
| 2007 | 166.6 (2.5) | 10.0 (0.4) | 5.2 (0.3) | 3.2 (0.4) | 9.1 (0.6) | 27.3 (1.0) |
| 2008 | 158.8 (2.5) | 9.6 (0.4) | 4.3 (0.3) | 3.0 (0.3) | 7.7 (0.5) | 26.2 (1.0) |
| 2009 | 143.6 (2.3) | 9.8 (0.4) | 3.8 (0.3) | 3.3 (0.4) | 8.0 (0.5) | 19.2 (0.9) |
| 2010 | 121.8 (2.2) | 8.1 (0.4) | 3.8 (0.3) | 3.1 (0.3) | 7.1 (0.5) | 14.5 (0.7) |
| 2011 | 106.1 (2.0) | 8.6 (0.4) | 3.9 (0.3) | 2.5 (0.3) | 7.1 (0.5) | 12.8 (0.7) |
| 2012 | 102.0 (2.0) | 8.6 (0.4) | 4.5 (0.3) | 2.9 (0.3) | 7.2 (0.5) | 13.9 (0.7) |
| 2013 | 90.7 (1.9) | 6.7 (0.4) | 3.6 (0.3) | 2.0 (0.3) | 6.8 (0.5) | 13.9 (0.7) |
| 2014 | 82.9 (1.8) | 5.6 (0.3) | 3.3 (0.2) | 2.7 (0.3) | 5.8 (0.5) | 9.6 (0.6) |
| 2015 | 68.9 (1.6) | 4.4 (0.3) | 3.9 (0.3) | 1.7 (0.3) | 6.1 (0.5) | 8.3 (0.6) |
| 2016 | 65.3 (1.6) | 4.9 (0.3) | 3.1 (0.2) | 2.3 (0.3) | 6.2 (0.5) | 9.2 (0.6) |
| 2017 | 63.3 (1.6) | 4.7 (0.3) | 3.1 (0.2) | 2.2 (0.3) | 5.0 (0.4) | 6.4 (0.6) |
| Total | 106.3 (0.6) | 7.4 (0.1) | 3.8 (0.1) | 2.6 (0.1) | 6.9 (0.1) | 14.7 (0.2) |
| Hospital Admissions Year | Age, Median (IQR) | p | Hospital Stay, Median (IQR) | p |
|---|---|---|---|---|
| 2007 | 43 (34–52) | < 0.001 | 4 (2–6) | < 0.001 |
| 2008 | 43 (35–52) | 3 (2–7) | ||
| 2009 | 44 (35–52) | 3 (2–7) | ||
| 2010 | 44 (36–54) | 4 (2–8) | ||
| 2011 | 45 (35–54) | 4 (2–7) | ||
| 2012 | 45 (36–55) | 4 (2–) | ||
| 2013 | 46 (37–55) | 4 (2–8) | ||
| 2014 | 46 (37–55) | 4 (2–9) | ||
| 2015 | 46 (38–55) | 5 (3–8) | ||
| 2016 | 46 (37–56) | 5 (3–9) | ||
| 2017 | 47 (38–57) | 5 (3–9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Restivo, V.; Costantino, C.; Amato, L.; Candiloro, S.; Casuccio, A.; Maranto, M.; Marrella, A.; Palmeri, S.; Pizzo, S.; Vitale, F.; et al. Evaluation of the Burden of HPV-Related Hospitalizations as a Useful Tool to Increase Awareness: 2007–2017 Data from the Sicilian Hospital Discharge Records. Vaccines 2020, 8, 47. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8010047
Restivo V, Costantino C, Amato L, Candiloro S, Casuccio A, Maranto M, Marrella A, Palmeri S, Pizzo S, Vitale F, et al. Evaluation of the Burden of HPV-Related Hospitalizations as a Useful Tool to Increase Awareness: 2007–2017 Data from the Sicilian Hospital Discharge Records. Vaccines. 2020; 8(1):47. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8010047
Chicago/Turabian StyleRestivo, Vincenzo, Claudio Costantino, Livia Amato, Stefania Candiloro, Alessandra Casuccio, Marianna Maranto, Alessandro Marrella, Sara Palmeri, Stefano Pizzo, Francesco Vitale, and et al. 2020. "Evaluation of the Burden of HPV-Related Hospitalizations as a Useful Tool to Increase Awareness: 2007–2017 Data from the Sicilian Hospital Discharge Records" Vaccines 8, no. 1: 47. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8010047