Comparison of Two Hepatitis B Vaccination Strategies Targeting Vertical Transmission: A 10-Year Japanese Multicenter Prospective Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
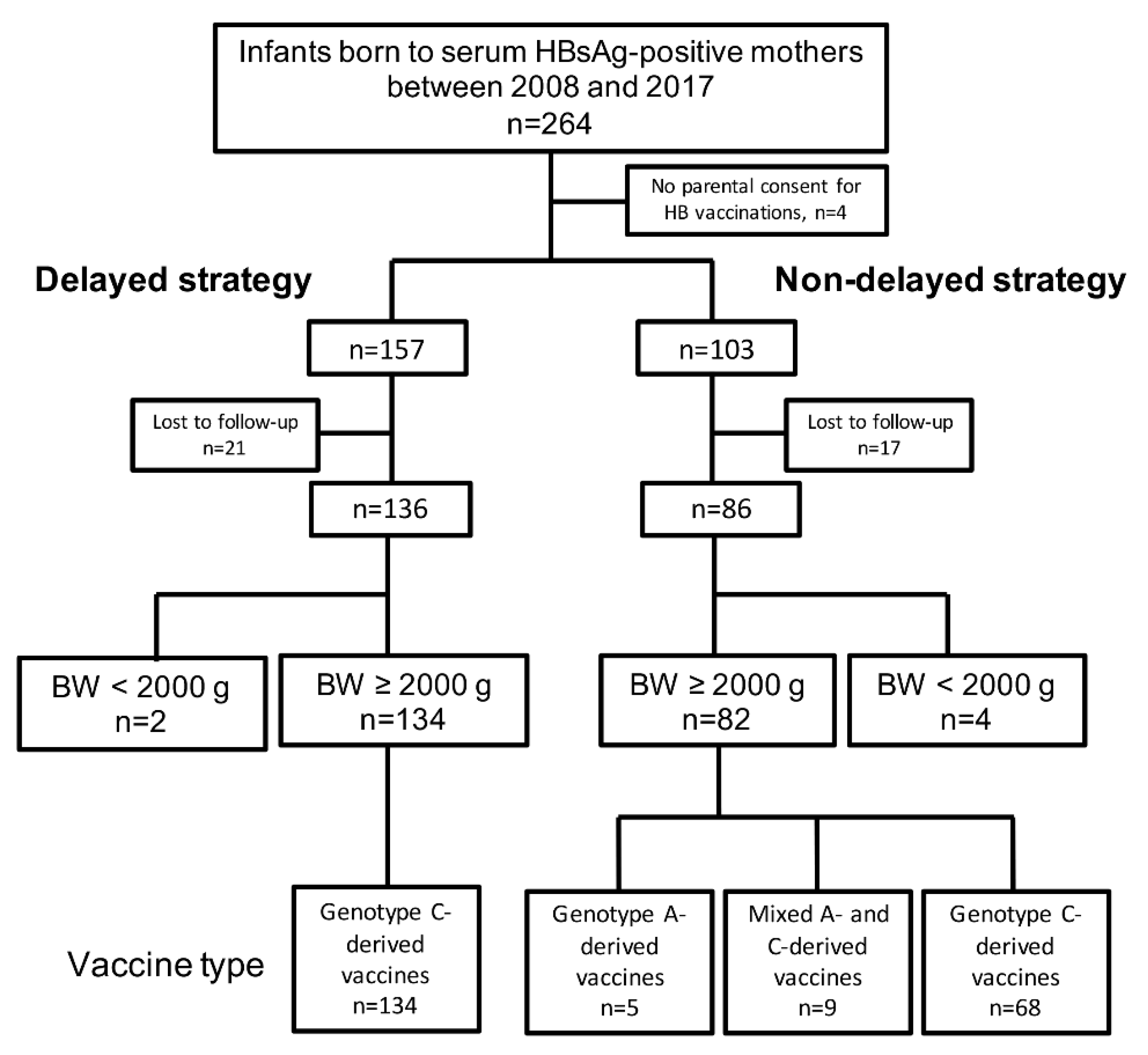
2.1. Study Design and Subjects
2.2. Methods
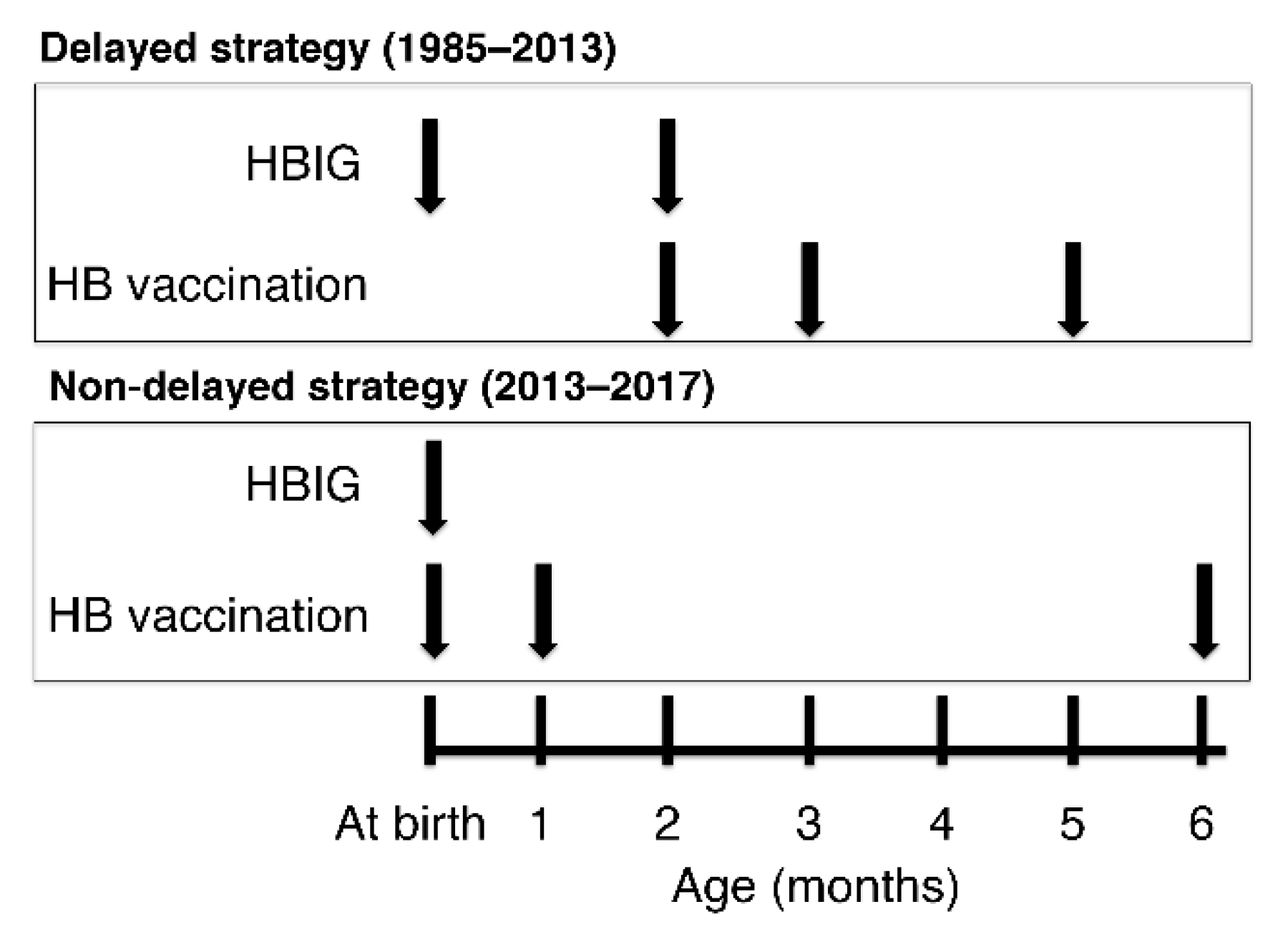
2.2.1. Delayed and Non-Delayed Strategies
2.2.2. Evaluation for Prophylaxis Success or Failure
2.2.3. Measurement Methods and Cut-off Values for Serum HB Markers
2.2.4. Study Variables and Main Outcome
2.3. Statistical Analyses
3. Results
3.1. Background Characteristics in Mothers and Infants
3.2. Serum Positive HBsAg and Positive Anti-HBs Titer Rates after Completing the HB Vaccines
3.3. Serum Anti-HBs Titer Levels in Infants with Birth Weight ≥ 2000 g
3.4. Positive Anti-HBs Titer Rates after Completing the Genotype C- or A-Derived HB Vaccines
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). Implementation of newborn hepatitis B vaccination--worldwide, 2006. Morb. Mortal Wkly. Rep. 2008, 57, 1249–1252. [Google Scholar]
- American Academy of Pediatrics. Hepatitis B. In RED BOOK 2015: Report of the Committee on Infectious Diseases, 30th ed.; Kimberlin, D.W., Brady, M.T., Jackson, M.A., Long, S.S., Eds.; American Academy of Pediatrics: Elk Grove Village, IL, USA, 2015; pp. 400–423. [Google Scholar]
- Beasley, R.P.; Hwang, L.Y.; Lee, G.C.; Lan, C.C.; Roan, C.H.; Huang, F.Y.; Chen, C.L. Prevention of perinatally transmitted hepatitis B virus infections with hepatitis B immune globulin and hepatitis B vaccine. Lancet 1983, 2, 1099–1102. [Google Scholar] [CrossRef]
- Lin, X.; Guo, Y.; Zhou, A.; Zhang, Y.; Cao, J.; Yang, M.; Xiao, F.; Zhang, B.; Du, Y. Immunoprophylaxis failure against vertical transmission of hepatitis B virus in the Chinese population: A hospital-based study and a meta-analysis. Pediatr. Infect. Dis. J. 2014, 33, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, C.; Jia, Z.F.; Wu, X.; Wen, S.M.; Kong, F.; Hu, K.Q.; Li, J.; Jiang, J.; Niu, J.Q. Protective effect of an improved immunization practice of mother-to-infant transmission of hepatitis B virus and risk factors associated with immunoprophylaxis failure. Medicine 2016, 95, e4390. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Gui, X.E.; Teter, C.; Zhong, H.; Pang, Z.; Ding, L.; Li, F.; Zhou, Y.; Zhang, L. Effects of hepatitis B immunization on prevention of mother-to-infant transmission of hepatitis B virus and on the immune response of infants towards hepatitis B vaccine. Vaccine 2014, 32, 6091–6097. [Google Scholar] [CrossRef]
- Eto, T.; Shiraki, K. National project on the prevention of mother-to-infant infection by hepatitis B virus in Japan. Acta Paediatr. Jpn. 1989, 31, 681–684. [Google Scholar] [CrossRef] [PubMed]
- Nagano, N.; Kitajima, H.; Morioka, I. Japanese original delayed hepatitis B vaccination provides adequate immunogenicity against mother-to-child hepatitis B virus infection in preterm infants: A nationwide survey in Japan. J. Infect. Chemother. 2020, 26, 385–388. [Google Scholar] [CrossRef]
- Shiraki, K.; For the Study Group for the Prevention of Vertical Transmission of Hepatitis B Virus. Clinical trials of HBIG and hepatitis B vaccine (Green cross) for the prevention of mother-to-infant infection of HBV. In Viral Hepatitis Infection in the Western Pacific Region; Lam, S.K., Lai, C.L., Yeoh, E.K., Eds.; World Scientific Publishing: Singapore, 1984; pp. 189–198. [Google Scholar]
- Komatsu, H.; Inui, A.; Sogo, T.; Fujisawa, T. Comparison of the Japanese and the international hepatitis B vaccine schedule. Kanzo 2010, 51, 92–94. (In Japanese) [Google Scholar] [CrossRef]
- Hokama, T.; Yara, A.; Hirayama, K.; Itokazu, K.; Uema, N.; Kinjho, R.; Yabu, E.; Toma, F. A survey on the vaccination practice for perinatal hepatitis B virus infection at a clinic in Okinawa, Japan. Asia Pac. J. Public Health 1998, 10, 46–48. [Google Scholar] [CrossRef]
- Japan Pediatric Society. New Guidelines for the Prevention of Mother-to-Child Hepatitis B Virus Infection. 2013. Available online: http://www.jpeds.or.jp/uploads/files/HBV20131218.pdf (accessed on 7 January 2021). (In Japanese).
- Japan Pediatric Society. Prevention of Hepatitis B Virus Mother-to-Child Infection: A Concept for Low Birth Weight Infants in Japanese Pediatric Society. 2014. Available online: http://www.jpeds.or.jp/uploads/files/hbboshikansen.pdf (accessed on 7 January 2021). (In Japanese).
- Yamana, K.; Iwatani, S.; Fujioka, K.; Iijima, K.; Morioka, I. Hepatitis B vaccine: Immunogenicity in an extremely low-birthweight infant. Pediatr. Int. 2018, 60, 489–490. [Google Scholar] [CrossRef]
- Jack, A.D.; Hall, A.J.; Maine, N.; Mendy, M.; Whittle, H.C. What level of hepatitis B antibody is protective? J. Infect. Dis. 1999, 179, 489–492. [Google Scholar] [CrossRef] [PubMed]
- West, D.J.; Calandra, G.B. Vaccine induced immunologic memory for hepatitis B surface antigen: Implications for policy on booster vaccination. Vaccine 1996, 14, 1019–1027. [Google Scholar] [CrossRef]
- Saari, T.N.; American Academy of Pediatrics Committee on Infectious Diseases. Immunization of preterm and low birth weight infants. Pediatrics 2003, 112, 193–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, C.Q.; Duan, Z.; Dai, E.; Zhang, S.; Han, G.; Wang, Y.; Zhang, H.; Zou, H.; Zhu, B.; Zhao, W.; et al. Tenofovir to Prevent Hepatitis B Transmission in Mothers with High Viral Load. N. Engl. J. Med. 2016, 374, 2324–2334. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prevention of Mother-to-Child Transmission of Hepatitis B Virus: Guidelines on Antiviral Prophylaxis in Pregnancy. 2020. Available online: https://www.who.int/publications/i/item/978-92-4-000270-8 (accessed on 7 January 2021).
- The Japan Society of Hepatology. Guidelines for the Treatment of Hepatitis B, Version 3.2. 2020. Available online: http://www.jsh.or.jp/files/uploads/HBV_GL_ver3.2_20200926.pdf (accessed on 7 January 2021). (In Japanese).
- Nishida, N.; Sugiyama, M.; Sawai, H.; Nishina, S.; Sakai, A.; Ohashi, J.; Khor, S.S.; Kakisaka, K.; Tsuchiura, T.; Hino, K.; et al. Key HLA-DRB1-DQB1 haplotypes and role of the BTNL2 gene for response to a hepatitis B vaccine. Hepatology 2018, 68, 848–858. [Google Scholar] [CrossRef]
- Carman, W.F.; Zanetti, A.R.; Karayiannis, P.; Waters, J.; Manzillo, G.; Tanzi, E.; Zuckerman, A.J.; Thomas, H.C. Vaccine-induced escape mutant of hepatitis B virus. Lancet 1990, 336, 325–329. [Google Scholar] [CrossRef]
- Purdy, M.A. Hepatitis B virus S gene escape mutants. Asian J. Transfus. Sci. 2007, 1, 62–70. [Google Scholar] [CrossRef]
- Kramvis, A.; Kew, M.; Francois, G. Hepatitis B virus genotypes. Vaccine 2005, 23, 2409–2423. [Google Scholar] [CrossRef]
- Tamada, Y.; Yatsuhashi, H.; Masaki, N.; Nakamuta, M.; Mita, E.; Komatsu, T.; Watanabe, Y.; Muro, T.; Shimada, M.; Hijioka, T.; et al. Hepatitis B virus strains of subgenotype A2 with an identical sequence spreading rapidly from the capital region to all over Japan in patients with acute hepatitis B. Gut 2012, 61, 765–773. [Google Scholar] [CrossRef] [Green Version]
- Komatsu, H.; Umetsu, S.; Inui, A.; Sogo, T.; Fujisawa, T. Interchangeability of genotype C‒derived and genotype A‒derived hepatitis B vaccines in children. J. Pediatr. Infect. Dis. Immunol. 2016, 28, 179–183. (In Japanese) [Google Scholar]
- Tregnaghi, M.; Ussher, J.; Baudagna, A.M.; Calvari, M.; Grana, G. Comparison of two recombinant hepatitis B vaccines and their interchangeability in Argentine infants. Rev. Panam. Salud. Publica 2004, 15, 35–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Momose, H.; Kato, T.; Hamaguchi, I. Evaluation of in vitro diagnostic kits for anti-HBs quantitative assays using the international standard and Japanese national standard. Jpn. J. Transfus. Cell Ther. 2020, 66, 629–633. (In Japanese) [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | All Subjects n = 222 | Delayed Strategy n = 136 | Non-Delayed Strategy n = 86 | p Value |
|---|---|---|---|---|
| Mother | ||||
| Positive HBsAg rate | 222/222 (100.0%) | 136/136 (100.0%) | 86/86(100.0%) | |
| HBsAg levels, IU/mL | ||||
| 0.05–1999 | 38/142 (26.7%) | 23/84 (27.3%) | 15/58 (25.8%) | 0.99 |
| ≥2000 | 104/142 (73.2%) | 61/84 (72.6%) | 43/58 (74.1%) | |
| Positive anti-HBs titer rate | 5/155 (3.2%) | 3/88 (3.4%) | 2/67 (3.0%) | 0.88 |
| Anti-HBs titer level, mIU/mL | 0.3 (0.0–250) | 0.3 (0.0–250) | 0.4 (0.0–20) | 0.83 |
| <10 | 48/52 (92.3%) | 32/34 (94.1%) | 16/18 (88.9%) | 0.90 |
| 10–299 | 4/52 (87.7%) | 2/34 (5.9%) | 2/18 (11.1%) | |
| 300–999 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| ≥1000 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Positive HBeAg rate | 61/205 (29.8%) | 41/126 (32.5%) | 20/79 (25.3%) | 0.30 |
| HBeAg level, cut-off index | 0.4 (0.2–2.297) | 0.4 (0.2–1.885) | 0.4 (0.2–2.297) | 0.20 |
| Positive anti-HBe titer rate | 110/165 (66.7%) | 60/98 (61.2%) | 50/67 (74.6%) | 0.87 |
| HBV-DNA level, Log copy/mL | 5.0 (2.1–9.0) | 5.1 (2.1–9.0) | 4.2 (2.1–9.0) | 0.34 |
| <2.1 | 10/87 (11.5%) | 4/51 (7.8%) | 6/36 (16.7%) | 0.45 |
| 2.1–8.9 | 62/87 (71.3%) | 36/51 (70.1%) | 26/36 (72.2%) | |
| ≥9.0 | 15/87 (17.2%) | 11/51 (21.6%) | 4/36 (11.1%) | |
| Infants | ||||
| Gestational age at birth, weeks | 39 (25–41) | 38 (27–41) | 39 (25–41) | 0.81 |
| Birth weight, g | 3077(918–4160) | 3077(1212–4138) | 3077(918–4160) | 0.98 |
| Male | 117/222 (52.7%) | 71/136 (52.2%) | 46/86 (53.5%) | 0.98 |
| Variables | Subjects n = 38 | Delayed Strategy n = 21 | Non-Delayed Strategy n = 17 | p Value |
|---|---|---|---|---|
| Mother | ||||
| Positive HBsAg rate | 38/38 (100.0%) | 21/21 (100.0%) | 17/17(100.0%) | |
| HBsAg levels, IU/mL | ||||
| 0.05–1999 | 6/35 (17.1%) | 4/19 (21.1%) | 2/16 (12.5%) | 0.67 |
| ≥2000 | 29/35 (82.9%) | 15/19 (78.9%) | 14/16 (87.5%) | |
| Positive anti-HBs titer rate | 0/14 (0%) | 0/8 (3%) | 0/6 (3%) | |
| Anti-HBs titer level, mIU/mL | 0.35 (0.1–6.6) | 1.3 (0.1–6.6) | 0.25 (0.1–1.3) | 0.15 |
| <10 | 14/14 (100.0%) | 8/8 (100.0%) | 6/6 (100.0%) | |
| 10–299 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 300–999 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| ≥1000 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Positive HBeAg rate | 10/33 (30.3%) | 5/19 (26.3%) | 5/14 (35.7%) | 0.71 |
| HBeAg level, cut-off index | 0.4 (0.2–1,681) | 0.4 (0.2–1,443) | 0.3 (0.3–1,681) | 0.71 |
| Positive anti-HBe titer rate | 18/27 (66.7%) | 10/15 (66.7%) | 8/12 (66.7%) | 1.00 |
| HBV-DNA level, Log copy/mL | 4.3 (2.1–9.0) | 4.3 (2.6–7.6) | 6.2 (2.1–9.0) | 0.60 |
| <2.1 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 2.1–8.9 | 12/15 (80.0%) | 7/7 (100.0%) | 5/8 (62.5%) | |
| ≥9.0 | 3/15 (20.0%) | 0 (0.0%) | 3/8 (37.5%) | |
| Infants | ||||
| Gestational age at birth, weeks | 39 (36–41) | 40 (36–41) | 39 (37–40) | 0.13 |
| Birth weight, g | 3140 (2360–4025) | 3146 (2775–4025) | 3140 (2360–3755) | 0.13 |
| Male | 18/38 (47.4%) | 11/21 (52.4%) | 7/17 (41.2%) | 0.53 |
| Subjects | Delayed Strategy | Non-Delayed Strategy | |
|---|---|---|---|
| All infants | N | 136 | 86 |
| Positive HBsAg rate | 0 (0.0%, 0.0–2.7%) | 2 (2.3%, 0.3–8.1%) | |
| Positive anti-HBs titer rate | 136 (100.0%, 97.3–100.0%) | 84 (97.7%, 91.9–99.7%) | |
| Infants with BW ≥2000 g | N | 134 | 82 |
| Positive HBsAg rate | 0 (0.0%, 0.0–2.7%) | 2 (2.4%, 0.3–8.5%) | |
| Positive anti-HBs titer rate | 134 (100.0%, 97.3–100.0%) | 80 (97.6%, 91.5–99.7%) | |
| Infants with BW <2000 g | N | 2 | 4 |
| Positive HBsAg rate | 0 (0.0%, 0.0–84.2%) | 0 (0.0%, 0.0–60.2%) | |
| Positive anti-HBs titer rate | 2 (100.0%, 15.8–100.0%) | 4 (100.0%, 39.8–100.0%) |
| Variables | Case 1 | Case 2 |
|---|---|---|
| Gestational age at birth | 39 weeks | 39 weeks |
| Birth weight | 2716 g | 3262 g |
| Gender | Male | Female |
| Year | 2016 | 2016 |
| Evaluation age | 10 months | 11 months |
| HBsAg levels, IU/mL | 31,497 | 56,465 |
| Anti-HBs titer level, mIU/mL | 0.4 | 5.5 |
| Anti-HBc titer | Positive | Positive |
| HBeAg level, cut-off index | 1740 | 1490 |
| Anti-HBe titer, the cut-off value for the inhibition rate | <1 | <1 |
| HBV-DNA level, Log copy/mL | Not examined | 8.9 |
| Genotype | Not examined | B |
| Anti-HBs Titer Level, mIU/mL | All Subjects n = 216 | Delayed Strategy n = 134 | Non-Delayed Strategy n = 82 | p Value |
|---|---|---|---|---|
| <10 | 2 (0.9%) | 0 (0.0%) | 2 (2.4%) | 0.45 |
| 10–299 | 56 (25.9%) | 38 (28.4%) | 18 (22.0%) | |
| 300–999 | 92 (42.6%) | 59 (44.0%) | 33 (40.2%) | |
| ≥1000 | 66 (30.6%) | 37 (27.6%) | 29 (35.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimura, K.; Yamana, K.; Fukushima, S.; Fujioka, K.; Miyabayashi, H.; Murabayashi, M.; Masunaga, K.; Okahashi, A.; Nagano, N.; Morioka, I. Comparison of Two Hepatitis B Vaccination Strategies Targeting Vertical Transmission: A 10-Year Japanese Multicenter Prospective Cohort Study. Vaccines 2021, 9, 58. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010058
Nishimura K, Yamana K, Fukushima S, Fujioka K, Miyabayashi H, Murabayashi M, Masunaga K, Okahashi A, Nagano N, Morioka I. Comparison of Two Hepatitis B Vaccination Strategies Targeting Vertical Transmission: A 10-Year Japanese Multicenter Prospective Cohort Study. Vaccines. 2021; 9(1):58. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010058
Chicago/Turabian StyleNishimura, Koji, Keiji Yamana, Sachiyo Fukushima, Kazumichi Fujioka, Hiroshi Miyabayashi, Masao Murabayashi, Ken Masunaga, Aya Okahashi, Nobuhiko Nagano, and Ichiro Morioka. 2021. "Comparison of Two Hepatitis B Vaccination Strategies Targeting Vertical Transmission: A 10-Year Japanese Multicenter Prospective Cohort Study" Vaccines 9, no. 1: 58. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010058