
Antibody Titer Kinetics and SARS-CoV-2 Infections Six Months after Administration with the BNT162b2 Vaccine

 ,
,  ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Covidiagnostix Study
2.2. Inclusion Criteria and Methodology
2.3. COVID-19 Diagnostic Data
2.4. Viruses and Cells
2.5. Micro-Neutralization Experiments
2.6. Statistical Analysis
3. Results
3.1. Serological Evaluation at T0
3.2. Serological Evaluation at T1
3.2.1. Seropositive Group
3.2.2. Seronegative Group
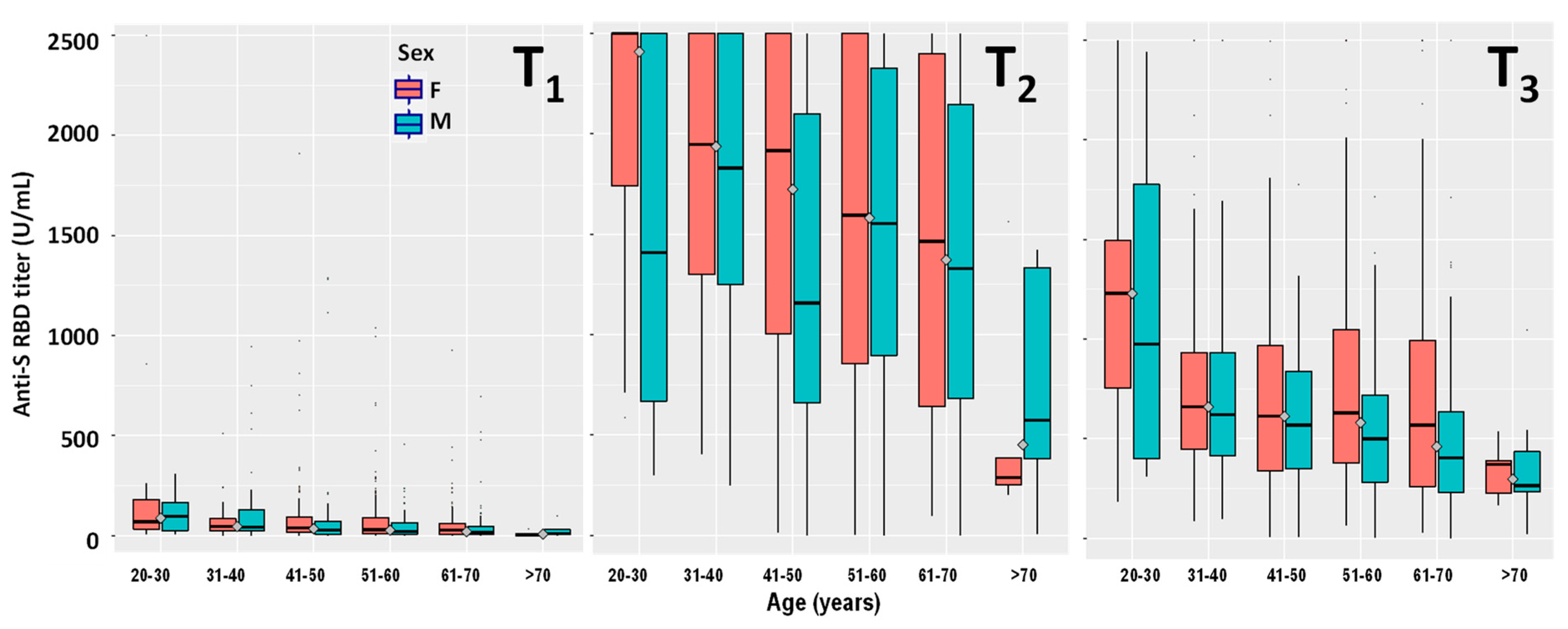
3.3. Serological Evaluation at T2
3.3.1. Seropositive Group
3.3.2. Seronegative Group
3.4. Serological Evaluation at T3
3.4.1. Seropositive Group
3.4.2. Seronegative Group
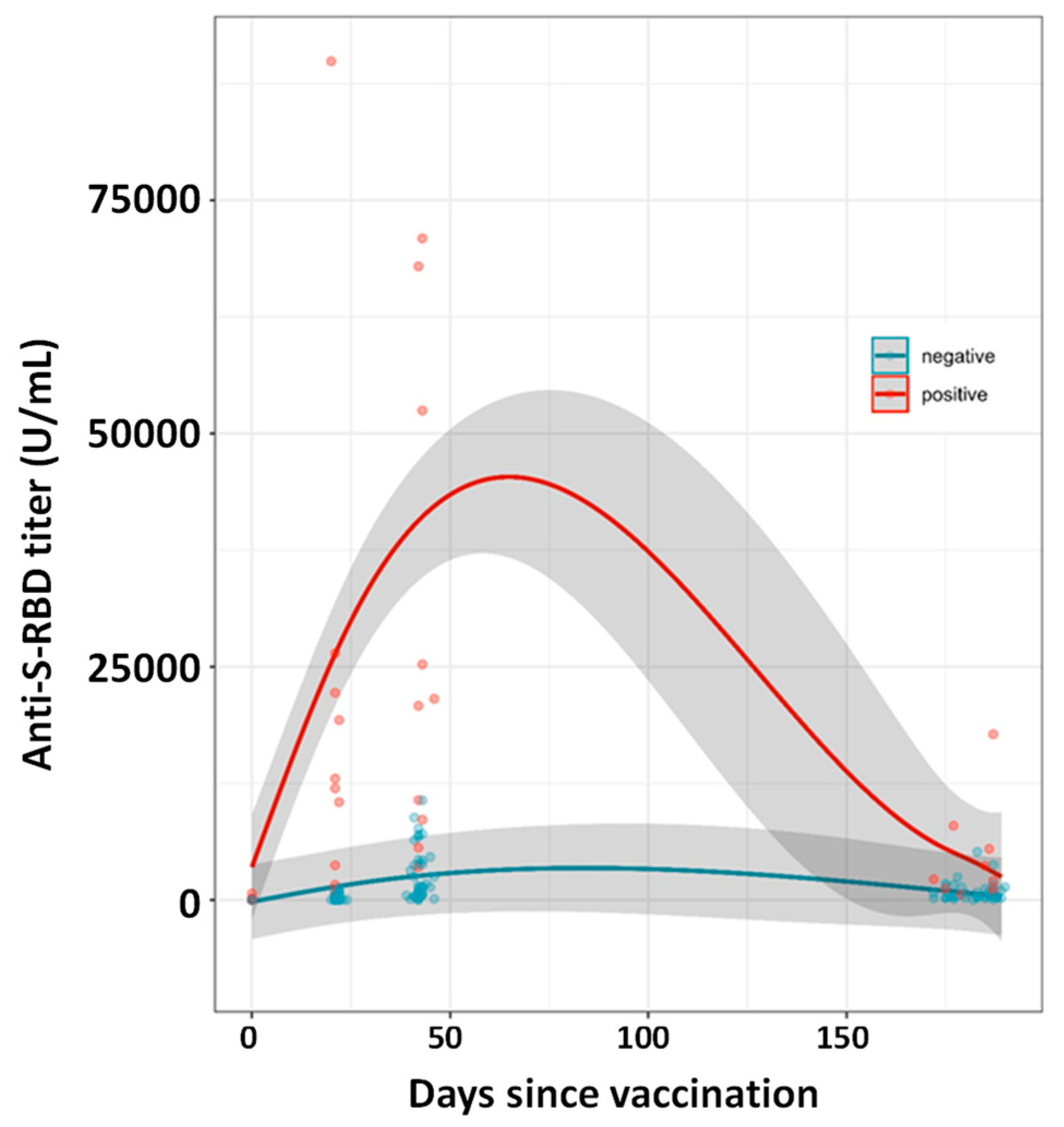
3.5. Post-Vaccination Infections
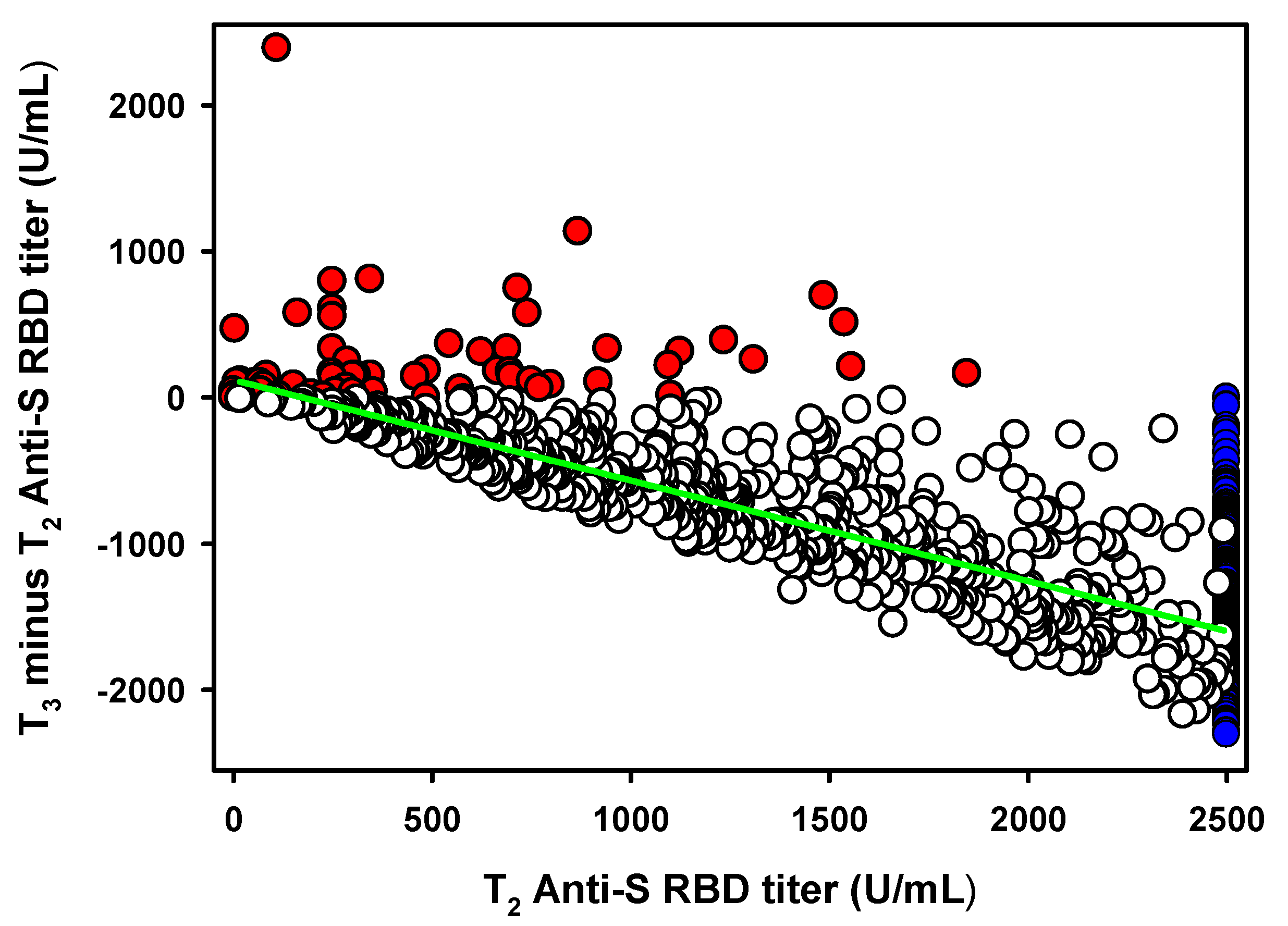
3.6. Antibody Titer Decrease between T2 and T3
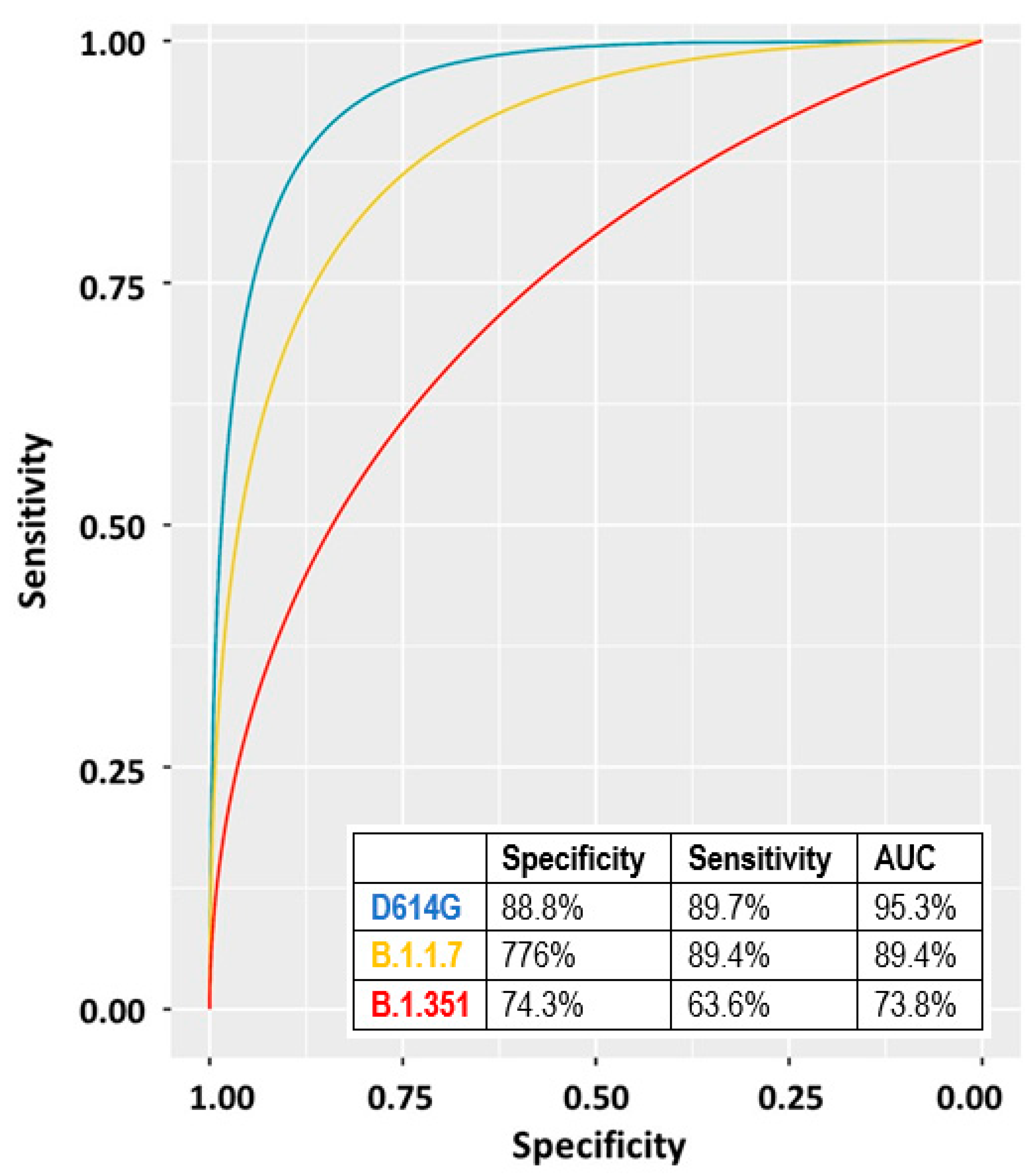
3.7. Neutralization Assays and Diluted Samples
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Worldometers. COVID-19 Statistics. Available online: https://www.worldometers.info/coronavirus/ (accessed on 6 October 2021).
- FDA. FDA Approves First COVID-19 Vaccine. 2021. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine (accessed on 3 September 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef]
- Berkeley, L.J. Pfizer CEO Says Third Covid Vaccine Dose Likely Needed within 12 Months. CNBC. 2021. Available online: https://www.cnbc.com/2021/04/15/pfizer-ceo-says-third-covid-vaccine-dose-likely-needed-within-12-months.html (accessed on 6 October 2021).
- Howard, J. A Third Dose of COVID-19 Vaccine Is Now Authorized for Some. Here’s What You Need to Know about Boosters for All. CNN. 2021. Available online: https://edition.cnn.com/2021/08/14/health/covid-19-vaccine-boosters-explainer-fda-wellness/index.html (accessed on 6 October 2021).
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.L.; Abiona, O.; Graham, B.; Mclellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef] [Green Version]
- Pallesen, J.; Wang, N.; Corbett, K.S.; Wrapp, D.; Kirchdoerfer, R.N.; Turner, H.L.; Cottrell, C.A.; Becker, M.M.; Wang, L.; Shi, W.; et al. Immunogenicity and structures of a rationally designed prefusion MERS-CoV spike antigen. Proc. Natl. Acad. Sci. USA 2017, 114, E7348–E7357. [Google Scholar] [CrossRef] [Green Version]
- Saadat, S.; Rikhtegaran, Z.T.; James, L.; Michelle, N.; Matthew, B.F.; Harris, A.D.; Sajadi, M.M. Binding and Neutralization Antibody Titers After a Single Vaccine Dose in Health CareWorkers Previously InfectedWith SARS-CoV-2. JAMA J. Am. Med. Assoc. 2021, 325, 1467–1469. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody responses in seropositive persons after a single dose of SARS-CoV-2 mRNA vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Prendecki, M.; Clarke, C.; Brown, J.; Cox, A.; Gleeson, S.; Guckian, M.; Randell, P.; Pria, A.D.; Lightstone, L.; Xu, X.-N.; et al. Effect of previous SARS-CoV-2 infection on humoral and T-cell responses to single-dose BNT162b2 vaccine. Lancet 2021, 397, 1178–1181. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/33640037 (accessed on 6 October 2021). [CrossRef]
- Manisty, C.; Otter, A.D.; Treibel, T.A.; McKnight, I.; Altmann, D.M.; Brooks, T.; Noursadeghi, M.; Boyton, R.J.; Semper, A.; Moon, J.C. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021, 397, 1057–1058. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, J.; Xia, H.; Zhang, X.; Fontes-Garfias, C.R.; Swanson, K.A.; Cai, H.; Sarkar, R.; Chen, W.; Cutler, M.; et al. Neutralizing Activity of BNT162b2-Elicited Serum. N. Engl. J. Med. 2021, 384, 1466–1468. [Google Scholar] [CrossRef]
- Ferrari, D.; Di Resta, C.; Sabetta, E.T.R.; Pontillo, M.; Motta, A.; Locatelli, M. Long-term antibody persistence and exceptional vaccination response on previously SARS-CoV-2 infected subjects. Vaccine 2021, 39, 4256–4260. [Google Scholar] [CrossRef]
- Ferrari, D.; Mangia, A.; Spanò, M.S.; Zaffarano, L.; Viganò, M.; Di Resta, C.; Locatelli, M.; Ciceri, F.; De Vecchi, E. Quantitative serological evaluation as a valuable tool in the COVID-19 vaccination campaign. Clin. Chem. Lab. Med. 2021, in press. [Google Scholar] [CrossRef]
- Favresse, J.; Bayart, J.-L.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Wieers, G.; Laurent, C.; Dogné, J.-M.; et al. Antibody titres decline 3-month post-vaccination with BNT162b2. Emerg. Microbes Infect. 2021, 10, 1495–1498. [Google Scholar] [CrossRef] [PubMed]
- Padoan, A.; Dall’Olmo, L.; Rocca, F.D.; Barbaro, F.; Cosma, C.; Basso, D.; Cattelan, A.; Cianci, V.; Plebani, M. Antibody response to first and second dose of BNT162b2 in a cohort of characterized healthcare workers. Clin. Chim. Acta 2021, 519, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Cocomazzi, G.; Piazzolla, V.; Squillante, M.M.; Antinucci, S.; Giambra, V.; Giuliani, F.; Maiorana, A.; Serra, N.; Mangia, A. Early Serological Response to BNT162b2 mRNA Vaccine in Healthcare Workers. Vaccines 2021, 9, 913. [Google Scholar] [CrossRef]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef] [PubMed]
- Tomaiuolo, R.; Derrico, P.; Ritrovato, M.; Locatelli, M.; Milella, F.; Restelli, U.; Lago, P.; Giuliani, F.; Banfi, G. COVIDIAGNOSTIX: Health technology assessment of serological tests for SARS-CoV-2 infection. Int. J. Technol. Assess. Health Care 2021, 37, 1–5. [Google Scholar] [CrossRef]
- Ferrari, D.; Manca, M.; Premaschi, S.; Banfi, G.; Locatelli, M. Toxicological investigation in blood samples from suspected impaired driving cases in the Milan area: Possible loss of evidence due to late blood sampling. Forensic Sci. Int. 2018, 288, 211–217. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Breyer, M.K.; Breyer-Kohansal, R.; Burghuber, O.C.; Hartl, S.; Aletaha, D.; Sieghart, D.; Quehenberger, P.; Marculescu, R.; et al. Side-by-Side Comparison of Three Fully Automated SARS-CoV-2 Antibody Assays with a Focus on Specificity. Clin. Chem. 2020, 66, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Kittel, M.; Muth, M.C.; Zahn, I.; Roth, H.J.; Thiaucourt, M.; Gerhards, C.; Haselmann, V.; Neumaier, M.; Findeisen, P. Clinical evaluation of commercial automated SARS-CoV-2 immunoassays. Int. J. Infect. Dis. 2021, 103, 590–596. [Google Scholar] [CrossRef]
- Favresse, J.; Eucher, C.; Elsen, M.; Tré-Hardy, M.; Dogné, J.M.; Douxfils, J. Clinical Performance of the Elecsys Electrochemiluminescent Immunoassay for the Detection of SARS-CoV-2 Total Antibodies. Clin. Chem. 2020, 66, 1104–1106. [Google Scholar] [CrossRef]
- Ferrari, D.; Clementi, N.; Spanò, S.M.; Albitar-Nehmee, S.; Ranno, S.; Colombini, A.; Criscuolo, E.; Di Resta, C.; Tomaiuolo, R.; Viganó, M.; et al. Harmonization of six quantitative SARS-CoV-2 serological assays using sera of vaccinated subjects. Clin. Chim. Acta 2021, 522, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, D.; Motta, A.; Strollo, M.; Banfi, G.; Locatelli, M. Routine blood tests as a potential diagnostic tool for COVID-19. Clin. Chem. Lab. Med. 2020, 58, 1095–1099. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/32301746 (accessed on 6 October 2021). [CrossRef] [PubMed] [Green Version]
- Castelli, M.; Baj, A.; Criscuolo, E.; Ferrarese, R.; Diotti, R.; Sampaolo, M.; Novazzi, F.; Gasperina, D.D.; Focosi, D.; Ferrari, D.; et al. Characterization of a Lineage C.36 SARS-CoV-2 Isolate with Reduced Susceptibility to Neutralization Circulating in Lombardy, Italy. Viruses 2021, 13, 1514. [Google Scholar] [CrossRef]
- Criscuolo, E.; Diotti, R.A.; Strollo, M.; Rolla, S.; Ambrosi, A.; Locatelli, M.; Burioni, R.; Mancini, N.; Clementi, M.; Clementi, N. Weak correlation between antibody titers and neutralizing activity in sera from SARS-CoV-2 infected subjects. J. Med. Virol. 2021, 93, 2160–2167. [Google Scholar] [CrossRef]
- Jonckheere, A.R. A Distribution-Free k-Sample Test Against Ordered Alternatives. Biometrika 1954, 41, 133. [Google Scholar] [CrossRef]
- Yohai, V.J. High Breakdown-Point and High Efficiency Robust Estimates for Regression. Ann. Stat. 1987, 15, 642–656. [Google Scholar] [CrossRef]
- Liu, W.; Pantoja-Galicia, N.; Zhang, B.; Kotz, R.M.; Pennello, G.; Zhang, H.; Jacob, J.; Zhang, Z. Generalized linear mixed models for multi-reader multi-case studies of diagnostic tests. Stat. Methods Med. Res. 2017, 26, 1373–1388. [Google Scholar] [CrossRef]
- Di Resta, C.; Ferrari, D.; Viganò, M.; Moro, M.; Sabetta, E.; Minerva, M.; Ambrosio, A.; Locatelli, M.; Tomaiuolo, R. The Gender Impact Assessment among Healthcare Workers in the SARS-CoV-2 Vaccination-An Analysis of Serological Response and Side Effects. Vaccines 2021, 9, 522. Available online: https://0-www-mdpi-com.brum.beds.ac.uk/2076-393X/9/5/522 (accessed on 6 October 2021). [CrossRef] [PubMed]
- Wiedermann, U.; Garner-Spitzer, E.; Wagner, A. Primary vaccine failure to routine vaccines: Why and what to do? Hum. Vaccines Immunother. 2016, 12, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Ciabattini, A.; Nardini, C.; Santoro, F.; Garagnani, P.; Franceschi, C.; Medaglini, D. Vaccination in the elderly: The challenge of immune changes with aging. Semin. Immunol. 2018, 40, 83–94. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Crotty, S.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, 1–13. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects (Year ± SD) | N° a | Test Results U/mL | |||
|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | ||
| COV+ (44.3 ± 12.6) | 82 | 58.3 (135.9) | 2500 b | 2500 c | 2500 d |
| M (44.2 ± 14.6) | 30 | 42.9 (79.4) | 2500 b | 2500 c | 2500 d |
| F (44.4 ± 11.5) | 52 | 67.2 (151) | 2500 b | 2500 c | 2500 d |
| COV− (49.4 ± 11.1) | 958 | / | 31.9 (73.0) | 1622 (1613) | 591 (612.8) |
| M (51.1 ± 11.7) | 319 | / | 27 (61.3) | 1427 (1541) | 499 (497) |
| M20–30 | 16 | / | 95.9 (141.3) | 1408 (1831) | 975 (1376) |
| M31–40 | 49 | / | 42.6 (104.7) | 1829 (1249) | 621 (518) |
| M41–50 | 61 | / | 28.3 (63.9) | 1157 (1440) | 568 (491) |
| M51–60 | 103 | / | 20 (57.3) | 1554 (1432) | 500 (436) |
| M61–70 | 83 | / | 16.5 (41.1) | 1329 (1466) | 404 (403) |
| M71–80 | 7 | / | 9.6 (99.8) | 573 (949) | 265 (201) |
| F (48.5 ± 10.7) | 639 | / | 35.8 (75.3) | 1755 (1569) | 645 (658) |
| F20–30 | 39 | / | 69.4 (147.8) | 2500 e | 1229 (741) |
| F 31–40 | 98 | / | 45.5 (58.6) | 1947 (1199) | 660 (483) |
| F 41–50 | 172 | / | 38.2 (78.2) | 1916 (1496) | 614 (628) |
| F 51–60 | 235 | / | 29.6 (79.9) | 1595.5 (1646) | 630 (668) |
| F 61–70 | 90 | / | 26.7 (54.9) | 1464 (1757) | 568 (734) |
| F 71–80 | 5 | / | 3.4 (4.2) | 287 (136) | 370 (164) |
| Subjects’ Age Interval | N a | Linear Regression Parameters | ||
|---|---|---|---|---|
| Slope (95%CI) | p Value | R2 | ||
| 20–30 | 31 | −0.54 (−0.35 to −0.73) | <0.0001 | 0.533 |
| 31–40 | 95 | −0.74 (−0.63 to −0.85) | <0.0001 | 0.660 |
| 41–50 | 151 | −0.72 (−0.66 to −0.79) | <0.0001 | 0.769 |
| 51–60 | 230 | −0.69 (−0.64 to −0.75) | <0.0001 | 0.723 |
| 61–70 | 101 | −0.66 (−0.59 to −0.73) | <0.0001 | 0.778 |
| 71–80 | 5 | −0.88 (−0.40 to −1.36) | <0.05 | 0.912 |
| Males | 227 | −0.73 (−0.68 to −0.79) | <0.0001 | 0.770 |
| Females | 386 | −0.66 (−0.61 to −0.70) | <0.0001 | 0.692 |
| Total | 613 | −0.69 (−0.65 to −0.72) | <0.0001 | 0.720 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrari, D.; Clementi, N.; Criscuolo, E.; Ambrosi, A.; Corea, F.; Di Resta, C.; Tomaiuolo, R.; Mancini, N.; Locatelli, M.; Plebani, M.; et al. Antibody Titer Kinetics and SARS-CoV-2 Infections Six Months after Administration with the BNT162b2 Vaccine. Vaccines 2021, 9, 1357. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111357
Ferrari D, Clementi N, Criscuolo E, Ambrosi A, Corea F, Di Resta C, Tomaiuolo R, Mancini N, Locatelli M, Plebani M, et al. Antibody Titer Kinetics and SARS-CoV-2 Infections Six Months after Administration with the BNT162b2 Vaccine. Vaccines. 2021; 9(11):1357. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111357
Chicago/Turabian StyleFerrari, Davide, Nicola Clementi, Elena Criscuolo, Alessandro Ambrosi, Francesca Corea, Chiara Di Resta, Rossella Tomaiuolo, Nicasio Mancini, Massimo Locatelli, Mario Plebani, and et al. 2021. "Antibody Titer Kinetics and SARS-CoV-2 Infections Six Months after Administration with the BNT162b2 Vaccine" Vaccines 9, no. 11: 1357. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111357