
A Community-Based Management of COVID-19 in a Mobile Container Unit

 ,
,
Abstract
:1. Introduction
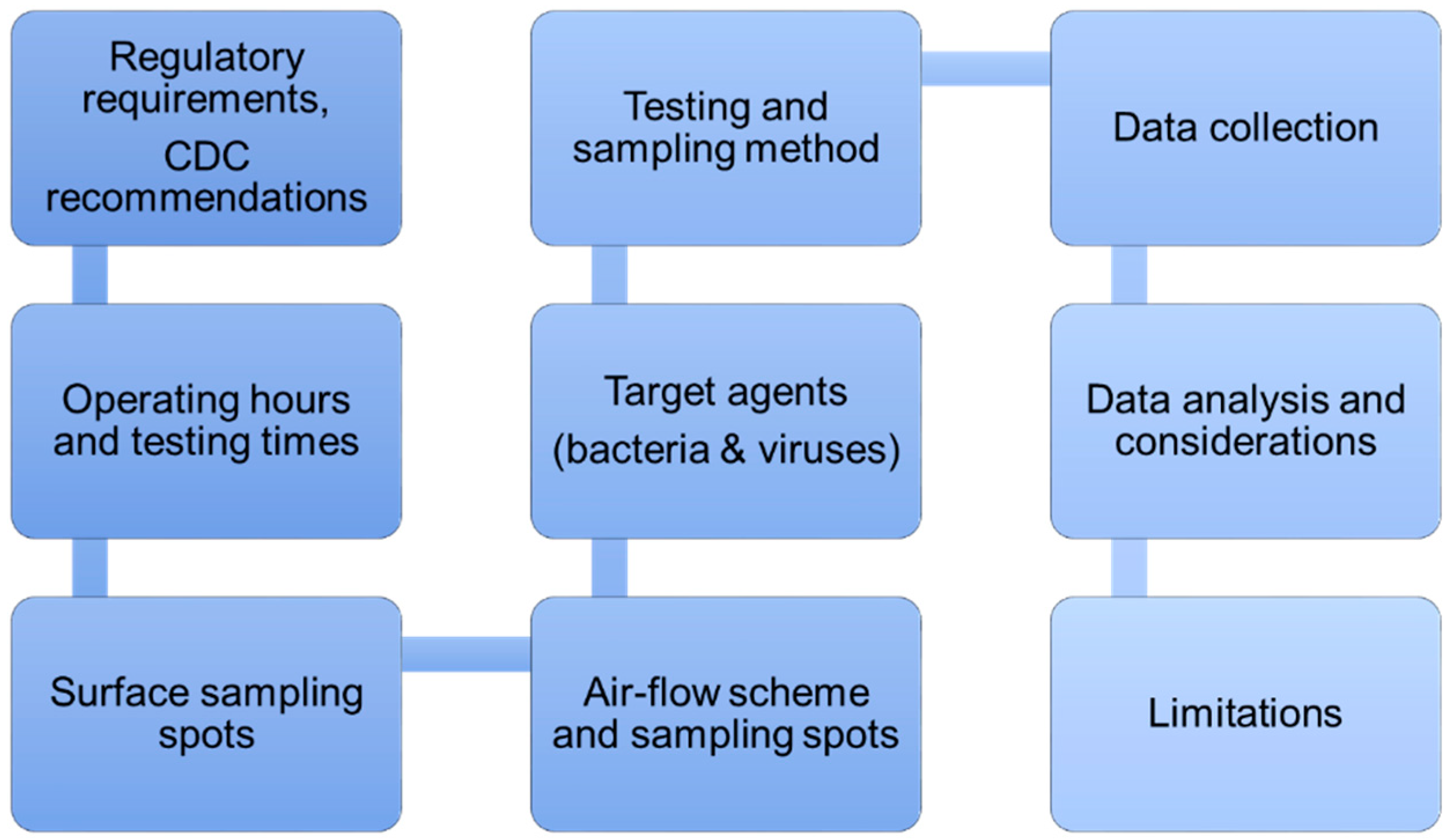
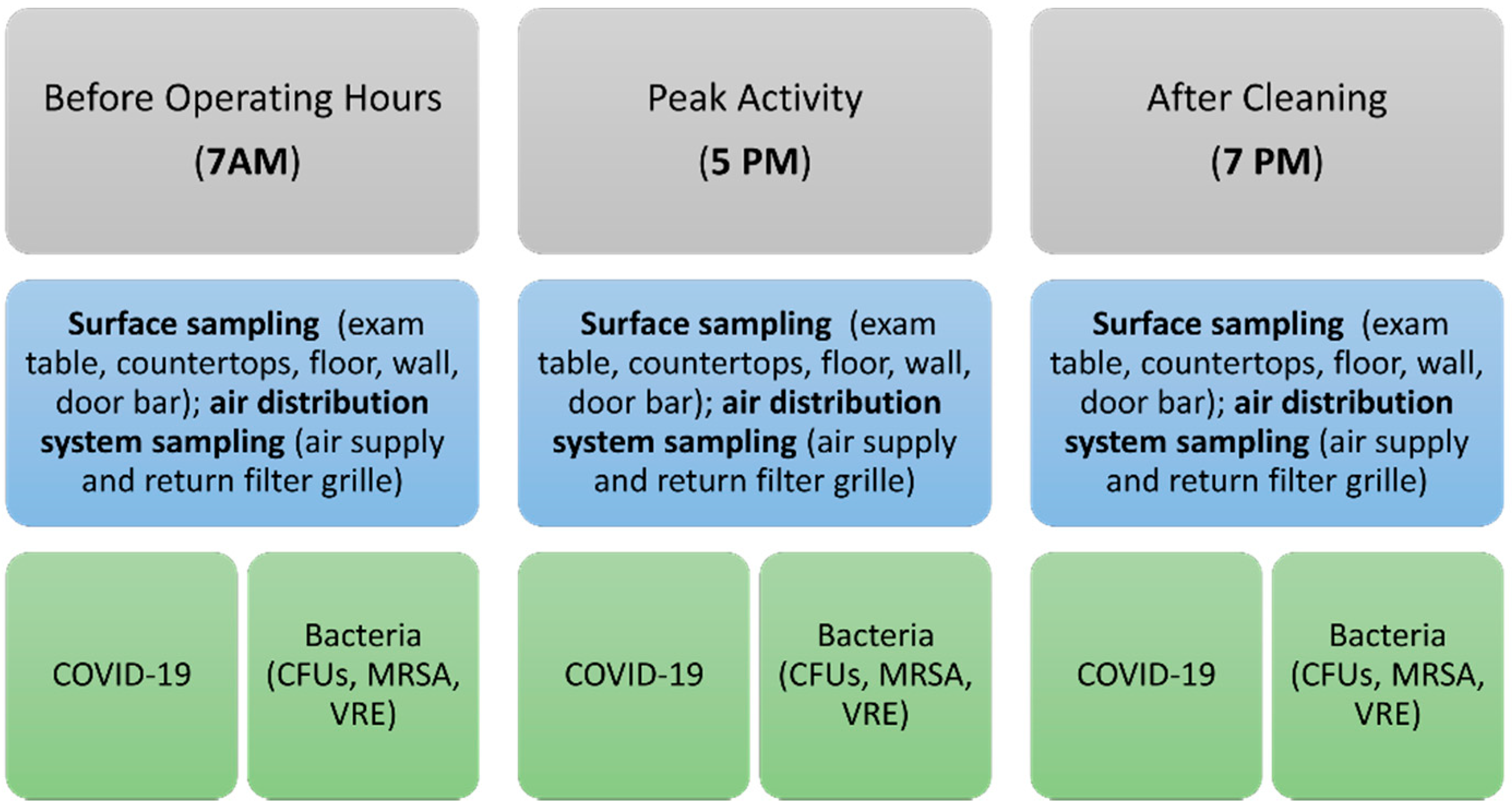
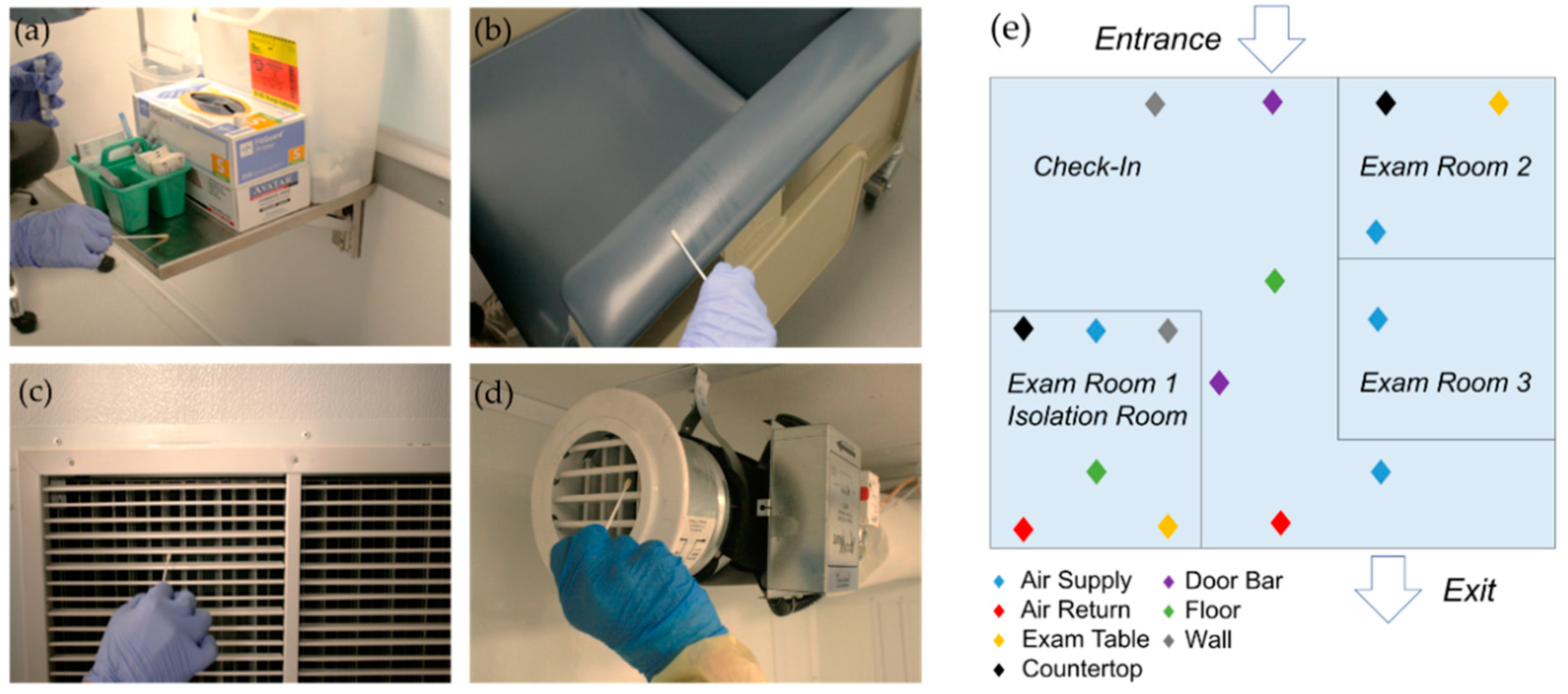
2. Materials and Methods
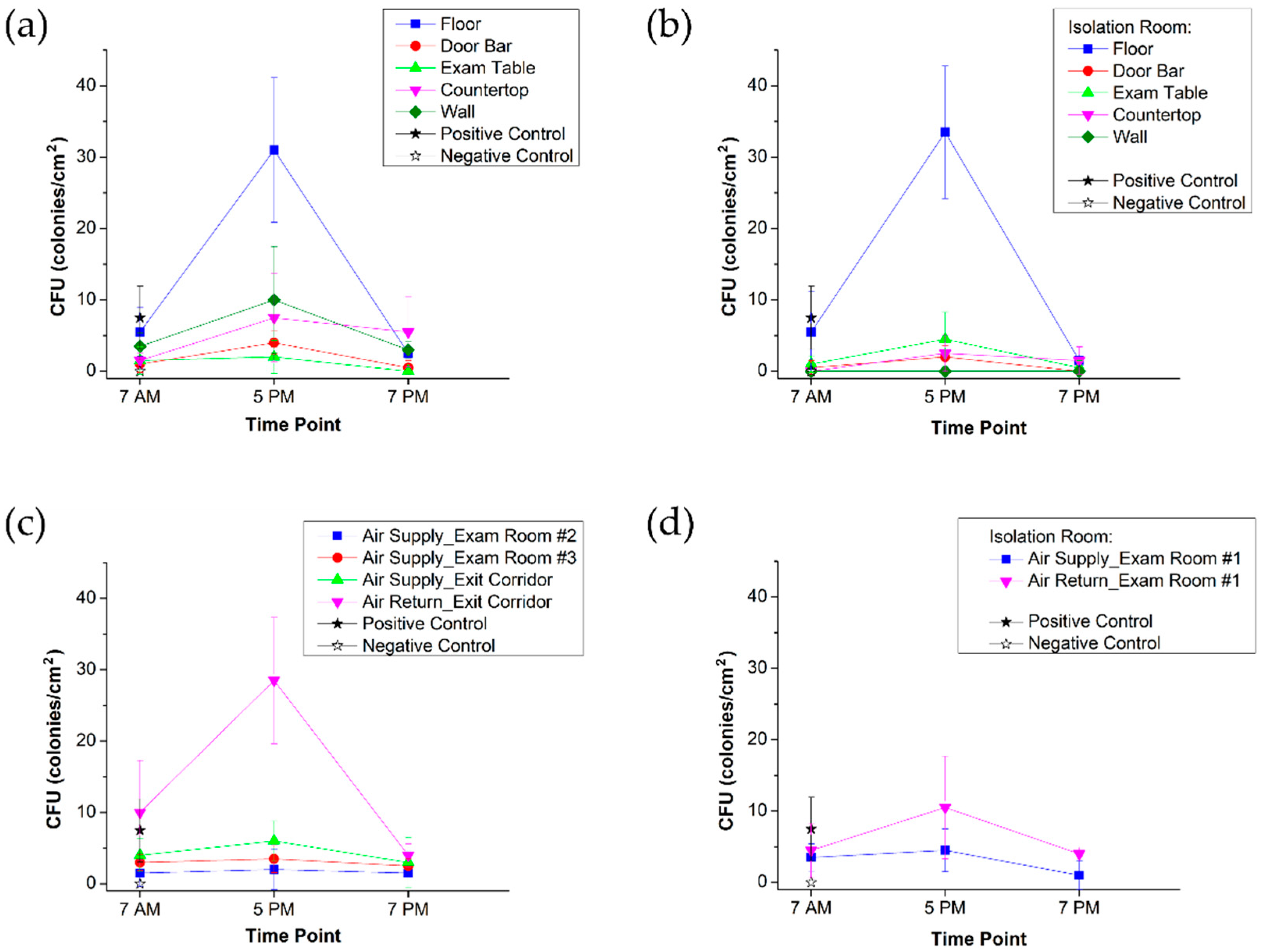
3. Results
- -
- Visit type: sick visit—5, annual physical—1, other vaccine—1;
- -
- COVID-19: vaccine—16; test—14, positive—2, negative—11.
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nelson, R. COVID-19 disrupts vaccine delivery. Lancet Infect. Dis. 2020, 20, 546. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Gianfredi, V.; Pennisi, F.; Lume, A.; Ricciardi, G.E.; Minerva, M.; Riccò, M.; Odone, A.; Signorelli, C. Challenges and Opportunities of Mass Vaccination Centers in COVID-19 Times: A Rapid Review of Literature. Vaccines 2021, 9, 574. [Google Scholar] [CrossRef]
- CDC. Community, Work, and School. 2019. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html (accessed on 3 August 2021).
- Lopez, L.; Hart, L.H.; Katz, M.H. Racial and Ethnic Health Disparities Related to COVID-19. JAMA 2021, 325, 719–720. [Google Scholar] [CrossRef] [PubMed]
- Abedi, V.; Olulana, O.; Avula, V.; Chaudhary, D.; Khan, A.; Shahjouei, S.; Li, J.; Zand, R. Racial, Economic, and Health Inequality and COVID-19 Infection in the United States. J. Racial Ethn. Health Disparities 2021, 8, 732–742. [Google Scholar] [CrossRef] [PubMed]
- Shadmi, E.; Chen, Y.; Dourado, I.; Faran-Perach, I.; Furler, J.; Hangoma, P.; Hanvoravongchai, P.; Obando, C.; Petrosyan, V.; Rao, K.D.; et al. Health equity and COVID-19: Global perspectives. Int. J. Equity Health 2020, 19, 104. [Google Scholar] [CrossRef]
- Table 62. No Usual Source of Health Care Among Adults Aged 18–64, by Selected Characteristics: United States, Average Annual, Selected Years 1993–1994 through 2015–2016. Available online: https://www.cdc.gov/nchs/data/hus/2017/062.pdf (accessed on 3 August 2021).
- MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.J.; Strych, U.; Dor, A.; Fowler, E.F.; Motta, M. Correlates and disparities of COVID-19 vaccine hesitancy. SSRN 2020, 272, 113638. [Google Scholar] [CrossRef]
- Bertoncello, C.; Ferro, A.; Fonzo, M.; Zanovello, S.; Napoletano, G.; Russo, F.; Baldo, V.; Cocchio, S. Socioeconomic Determinants in Vaccine Hesitancy and Vaccine Refusal in Italy. Vaccines 2020, 8, 276. [Google Scholar] [CrossRef]
- Momplaisir, F.M.; Kuter, B.J.; Ghadimi, F.; Browne, S.; Nkwihoreze, H.; Feemster, K.A.; Frank, I.; Faig, W.; Shen, A.K. Offit PA, Green-McKenzie, J. Racial/Ethnic Differences in COVID-19 Vaccine Hesitancy Among Health Care Workers in 2 Large Academic Hospitals. JAMA Netw. Open 2021, 4, e2121931. [Google Scholar] [CrossRef]
- Yu, S.W.Y.; Hill, C.; Ricks, M.L.; Bennet, J.; Oriol, N.E. The scope and impact of mobile health clinics in the United States: A literature review. Int. J. Equity Health 2017, 16, 178. [Google Scholar] [CrossRef]
- George, S. IHI Teams up with Leading Mobile Health Clinics to Spotlight Innovative Approaches to Improving Health and Health Care Services; Institute for Healthcare Improvement: Boston, MA, USA, 2014; pp. 1–3. [Google Scholar]
- Samouei, R.; Abbasi, S.; Mohajer, H. Investigation of mobile clinics and their challenges. Int. J. Health Syst. Disaster Manag. 2016, 4, 1–5. [Google Scholar] [CrossRef]
- Aung, K.; Hill, C.; Bennet, J.; Song, Z.; Oriol, N. The Emerging Business Models and Value Proposition of Mobile Health Clinics. AJMC.com. 2015. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC5837864/ (accessed on 26 March 2017).
- Krol, D.M.; Redlener, M.; Shapiro, A.; Wajnberg, A. A Mobile Medical Care Approach Targeting Underserved Populations in post-Hurricane Katrina Mississippi. J. Health Care Poor Underserved 2007, 18, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Dash, U.; Muraleedharan, V.R.; Prasad, B.M.; Dash, S.D.; Acharya, D.; Lakshminarasimhan, S. Access to Health Services in Under Privileged Areas; A Case Study of Mobile Health Units in Tamil Nadu and Orissa; Department of Humanities and Social Sciences Indian Institute of Technology Madras: Tamil Nadu, India, 2008. [Google Scholar]
- Corwin, C.; Sinnwell, E.; Culp, K. A Mobile Primary Care Clinic Mitigates an Early COVID-19 Outbreak among Migrant Farmworkers in Iowa. J. Agromed. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tulledge-Scheitel, S.; Bell, S.J.; Larsen, J.J.; Bierle, D.M.; Takahashi, P.; Moehnke, D.E.; Borgen, M.J.D.; Springer, D.J.; Reinschmidt, K.J.; Baumbach, L.J.; et al. A mobile unit overcomes the challenges to monoclonal antibody infusion for COVID-19 in skilled care facilities. J. Am. Geriatr. Soc. 2021, 69, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.R.; Cadet, K.; Mani, S. COVID-19 Testing and Social Determinants of Health among Disadvantaged Baltimore Neighborhoods: A Community Mobile Health Clinic Outreach Model. Population Health Management. Popul. Health Manag. 2021. [Google Scholar] [CrossRef]
- Lei, H.; Ye, F.; Liu, X.; Huang, Z.; Ling, S.; Jiang, Z.; Cheng, J.; Huang, X.; Wu, Q.; Wu, S.; et al. SARS-CoV-2 environmental contamination associated with persistently infected COVID-19 patients. Influenza Other Respir. Viruses 2020, 14, 688–699. [Google Scholar] [CrossRef]
- Sydnor, E.R.; Perl, T.M. Hospital epidemiology and infection control in acute-care settings. Clin. Microbiol. Rev. 2011, 24, 141–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chirico, F.; Sacco, A.; Bragazzi, N.L.; Magnavita, N. Can Air-Conditioning Systems Contribute to the Spread of SARS/MERS/COVID-19 Infection? Insights from a Rapid Review of the Literature. Int. J. Environ. Res. Public Health 2020, 17, 6052. [Google Scholar]
- Correia, G.; Rodrigues, L.; Gameiro da Silva, M.; Gonçalves, T. Airborne route and bad use of ventilation systems as non-egligible factors in SARS-CoV-2 transmission. Med. Hypotheses 2020, 141, 109781. [Google Scholar] [CrossRef]
- Harris County’s New Smart Pod Mobile ACCESS2Health First in U.S. Available online: https://www.fox26houston.com/news/harris-countys-new-smart-pod-mobile-access2health-first-in-u-s (accessed on 3 August 2021).
- Petrova, E.V.; Xu, H.; Franklin, B.A.; Woc-Colburn, L.E.; Anandasabapathy, S. COVID-19/Coronavirus Outbreak: A Rapidly Deployable Medical Facility Optimized for Epidemics (Smart Pod). J. Vis. Exp. 2020, e6423. [Google Scholar]
- Global Perspective. TMC News. Available online: https://www.tmc.edu/news/2015/03/global-perspective/ (accessed on 3 August 2021).
- USAID Funds Ebola “Smart Pod” Project [Internet]. Available online: https://www.federaltimes.com/govcon/2015/02/20/usaid-funds-ebola-smart-pod-project/ (accessed on 3 August 2021).
- Emergency Smart Pods—Transforming Containers into Modern Medical Clinics. Available online: https://2017-2021.state.gov/emergency-smart-pods-transforming-containers-into-modern-medical-clinics/ (accessed on 3 August 2021).
- Petrova, E.V.; Avadhanula, V.; Michel, S.; Gincoo, K.E.; Piedra, P.A.; Anandasabapathy, S. Remote Laboratory Management: Respiratory Virus Diagnostics. J. Vis. Exp. 2019, e59188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allman, M.; Bhushan, S.; Montealegre, J.; Hilmers, D.; Petrova, E.; Anandasabapathy, S. Rapidly Deployable “Smart” Labs in Epidemics: Barriers and Facilitators to Implementation, Washington, DC, USA, 18–20 April 2020.
- Liberia Gets Virus Specimen Testing Lab For Rapid Diagnostic Response. Available online: https://frontpageafricaonline.com/news/liberia-gets-virus-specimen-testing-lab-for-rapid-diagnostic-response/ (accessed on 3 August 2021).
- Bhushan, S.; Allman, M.; Montealegre, J.; Petrova, E.; Anandasabapathy, S. Improving Health Equity Post-Ebola: Evaluating Acceptability of Augmented Reality Technologies for Standardized and Safe Laboratory Training in Liberia; Health Equity Summer Research Summit: Houston, TX, USA, 2019. [Google Scholar]
- Petrova, E.V.; Franklin, B.A.; Woc-Colburn, L.E.; Anandasabapathy, S. COVID-19/Coronavirus Outbreak: Donning and Doffing Personal Protective Equipment (PPE) for Healthcare Providers. J. Vis. Exp. 2020, 2, e6425. [Google Scholar]
- Petrova, E.V.; Xu, H.; Franklin, B.A.; Woc-Colburn, L.E.; Anandasabapathy, S. COVID-19/Coronavirus Outbreak: Guidance for Hand Hygiene for Healthcare Providers to Ensure a Safe and Healthy Environment. J. Vis. Exp. 2020, e6424. [Google Scholar] [CrossRef]
- SmartPod Facility to Expand Healthcare Access in Pasadena. Available online: https://www.houstonchronicle.com/neighborhood/pasadena/news/article/SmartPod-facility-to-expand-healthcare-access-in-15944100.php (accessed on 3 August 2021).
- Rodriguez, N.; Goebel, M.; Bhushan, S.; Anandasabapathy, S.; Patel, S.M. Utilization of Project ECHO for COVID-19 Medical Knowledge and Best Practices for Health Professionals serving an Underserved Population. In Proceedings of the IDWEEK Virtual 2021, Washington, DC, USA, 29 September–3 October 2021. (Virtual poster #973; 29 September 2021). [Google Scholar]
- Rutala, W.A.; Weber, D.J.; The Healthcare Infection Control Practices Advisory Committee (HICPAC). CDC: Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008 Update: May 2019. Available online: https://www.cdc.gov/infectioncontrol/guidelines/disinfection/ (accessed on 3 August 2021).
- Guidelines for Environmental Infection Control in Health-Care Facilities Background F: Environmental Sampling. Available online: https://www.cdc.gov/infectioncontrol/guidelines/environmental/appendix/air.html (accessed on 3 August 2021).
- Guidelines for Environmental Infection Control in Health-Care Facilities Appendix B: Air. Available online: https://www.cdc.gov/infectioncontrol/guidelines/environmental/background/sampling.html (accessed on 3 August 2021).
- Morawska, L.; Tang, J.W.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F.; et al. How can airborne transmission of COVID-19 indoors be minimised? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef]
- Schweizer, M.; Graham, M.; Ohl, M.; Heilmann, K.; Boyken, L.; Diekema, D. Novel Hospital Curtains with Antimicrobial Properties: A Randomized, Controlled Trial. Infection control and hospital epidemiology. Infect. Control. Hosp. Epidemiol. 2021, 33, 1081–1085. [Google Scholar] [CrossRef]
- Wilson, G.; Jackson, V.; Boyken, L.; Puig-Asensio, M.; Marra, A.R.; Perencevich, E.; Schweizer, M.L.; Diekema, D.; Breheny, P.; Petersen, C. A randomized control trial evaluating efficacy of antimicrobial impregnated hospital privacy curtains in an intensive care setting. Am. J. Infect. Control. 2020, 48, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Interim Infection Prevention and Control Recommendations for Healthcare Personnel during the Coronavirus Disease 2019 (COVID-19) Pandemic. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html (accessed on 3 August 2021).
- Burke, J.P. Infection Control—A Problem for Patient Safety. NEJM 2003, 348, 651. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Tian, J.; Li, G.; Li, G. Initiation of a new infection control system for the COVID-19 outbreak. Lancet Infect. Dis. 2020, 20, 397–398. [Google Scholar] [CrossRef]
- Thies, K.M.; Gonzalez, M.; Porto, A.; Ashley, K.L.; Korman, S.; Lamb, M. Project ECHO COVID-19: Vulnerable Populations and Telehealth Early in the Pandemic. J. Prim. Care Community Health 2021, 12, 21501327211019286. [Google Scholar] [CrossRef]
- Katzman, J.G.; Tomedi, L.E.; Everly, G.; Greenwood-Ericksen, M.; Romero, E.; Rosenbaum, N.; Medrano, J.; Menking, P.; Archer, G.R.D.; Martin, C.; et al. First Responder Resiliency ECHO: Innovative Telementoring during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4900. [Google Scholar] [CrossRef] [PubMed]
- Lyu, H.; Wang, J.; Wu, W.; Duong, V.; Zhang, X.; Dye, T.D.; Luo, J. Social media study of public opinions on potential COVID-19 vaccines: Informing dissent, disparities and dissemination. Intell. Med. 2021, in press. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Time | COVID-19 Detection (N1 Ct) | General Bacterial Culture * (CFUs/cm2) | MRSA (CFUs/cm2) | VRE (CFUs/cm2) |
|---|---|---|---|---|---|
| Positive Control | 33.8 | 8 | 11 | 6 | |
| Negative Control | N.D. | 0 | 0 | 0 | |
| Surface Samples (10 sampling spots) | 7 AM | N.D. | 2 | 0 | 0 |
| 5 PM | N.D. | 4 | 0 | 0 | |
| 7 PM | N.D. | 0 | 0 | 0 | |
| Air Distribution System (6 sampling spots) | 7 AM | N.D. | 3 | 0 | 0 |
| 5 PM | N.D. | 6 | 0 | 0 | |
| 7 PM | N.D. | 2 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrova, E.; Farinholt, T.; Joshi, T.P.; Moreno, H.; Al Mohajer, M.; Patel, S.M.; Petrosino, J.; Anandasabapathy, S. A Community-Based Management of COVID-19 in a Mobile Container Unit. Vaccines 2021, 9, 1362. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111362
Petrova E, Farinholt T, Joshi TP, Moreno H, Al Mohajer M, Patel SM, Petrosino J, Anandasabapathy S. A Community-Based Management of COVID-19 in a Mobile Container Unit. Vaccines. 2021; 9(11):1362. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111362
Chicago/Turabian StylePetrova, Elena, Timothy Farinholt, Tejas P. Joshi, Hannah Moreno, Mayar Al Mohajer, Shital M. Patel, Joseph Petrosino, and Sharmila Anandasabapathy. 2021. "A Community-Based Management of COVID-19 in a Mobile Container Unit" Vaccines 9, no. 11: 1362. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111362