1. Introduction
Hepatitis A is an acute liver disease caused by hepatitis A virus (HAV) infection. The prevalence of hepatitis A is closely associated with socioeconomic development and sanitation policies that ensure access to clean water, and adequate conditions for personal hygiene [
1]. Although HAV transmission occurs primarily via exposure to contaminated food and water, many outbreaks of HAV infection have been associated with drug abuse and sexual behaviors, including men having sex with men (MSM) [
2,
3]. The clinical manifestations of hepatitis A are age-related, with less than 30% of patients under 6 years of age presenting with symptoms, while in adults more than 70% manifest symptoms such as fever, malaise, abdominal discomfort, nausea, vomiting, and jaundice [
4]. HAV infection is usually self-limiting, however, 1% of cases evolve to acute liver failure, with the highest rates observed in older adults (>40 years old) or in patients with underlying chronic liver disease [
5].
Between 1999 and 2015, HAV infection comprised 31% of all viral hepatitis reported in Brazil, with the North and Northeast regions accounting for 57% of all confirmed cases of hepatitis A and presenting the highest age-standardized mortality rate [
6,
7]. Since 2006, the overall incidence rate of HAV infection in Brazil has shown a downward trend, from 9.1/1,000,000 inhabitants to 3.1/1,000,000 in 2013 [
7]. This considerable reduction is likely to be closely associated with improvements in water supply and sanitation. It is also important to note that a national serological survey conducted between 2004 and 2009 demonstrated that the country was in epidemiological transition, presenting two distinct patterns across the Brazilian regions. The North, Northeast and Midwest regions showed an intermediate endemicity pattern, in which 56.0–67.5% of children and adolescents aged 5–19 years were seropositive, compared to only 34.5–37.7% in the South and Southeast regions [
8,
9]. Increased outbreaks were reported across the country, most of them affecting the children and adolescents in this age group. In this situation, the World Health Organization (WHO) recommends integration of universal HAV immunization schedule for children ≥ 1 year old to reduce the number of overall hepatitis A and control outbreaks [
10].
Most hepatitis A immunization schedules traditionally involve two doses of an inactivated hepatitis A vaccine, given 6-18 months apart for complete and life-long immunization [
11]. Alternatively, a single-dose inactivated hepatitis A vaccine immunization schedule can be put into practice, offering seemingly comparable effectiveness, and easier implementation than the classic two-dose schedule. A universal single-dose childhood vaccination program has been adopted in some Latin American countries due to a competitive National Immunization Program (NIP) fund allocation. In July 2014, an inactivated hepatitis A vaccination program with a single-dose scheme targeting children between 12 and 24 months old was included in the Brazilian NIP, and expanded to cover children under 5 years old in 2017. This was based on experience in Argentina, where a decrease in mean incidence rate from 66.5/100,000 in 2000–2002 to 7.9/100,000 in 2006–2011 was reported after a single-dose program implementation in 2005, as well as through further endorsement in the 2012 WHO position paper on hepatitis A vaccines [
10].
Previous data on the impact of universal hepatitis A vaccination in Brazil have demonstrated a cumulative 85.5% reduction in the total number of hepatitis A cases reported between 2014 and 2016 with vaccination coverage ranging from 60.1% to 97.1% [
12,
13]. The reduction was more prominent among children under 5 years old suggesting a direct vaccination effect. Additionally, the sharp decline in hepatitis A cases in children between 5 and 14 years old indicated the herd immunity phenomenon. Despite the importance of these data, only a descriptive analysis was performed, and the reduction of hepatitis A cases did not account for the baseline downward trend observed in the pre-vaccination period. It is, therefore, unknown whether the impact of the NIP on prevention of hepatitis A persists when pre-vaccination period effects are offset. It would also be useful to explore if the reduction in hepatitis A cases was consistent across different age groups and geographic locations after the universal vaccine introduction in order to identify potential outbreak triggers. Finally, it is important to measure the direct effect of the vaccination program by estimating the averted hepatitis A cases after the vaccine introduction.
The aim of the current study was to assess the effect of universal childhood vaccination on hepatitis A incidence across age groups by conducting an interrupted time-series analysis. Additionally, we assessed the hepatitis A distribution throughout Brazilian geographic regions before and after the vaccination program implementation.
2. Materials and Methods
2.1. Study Design and Population
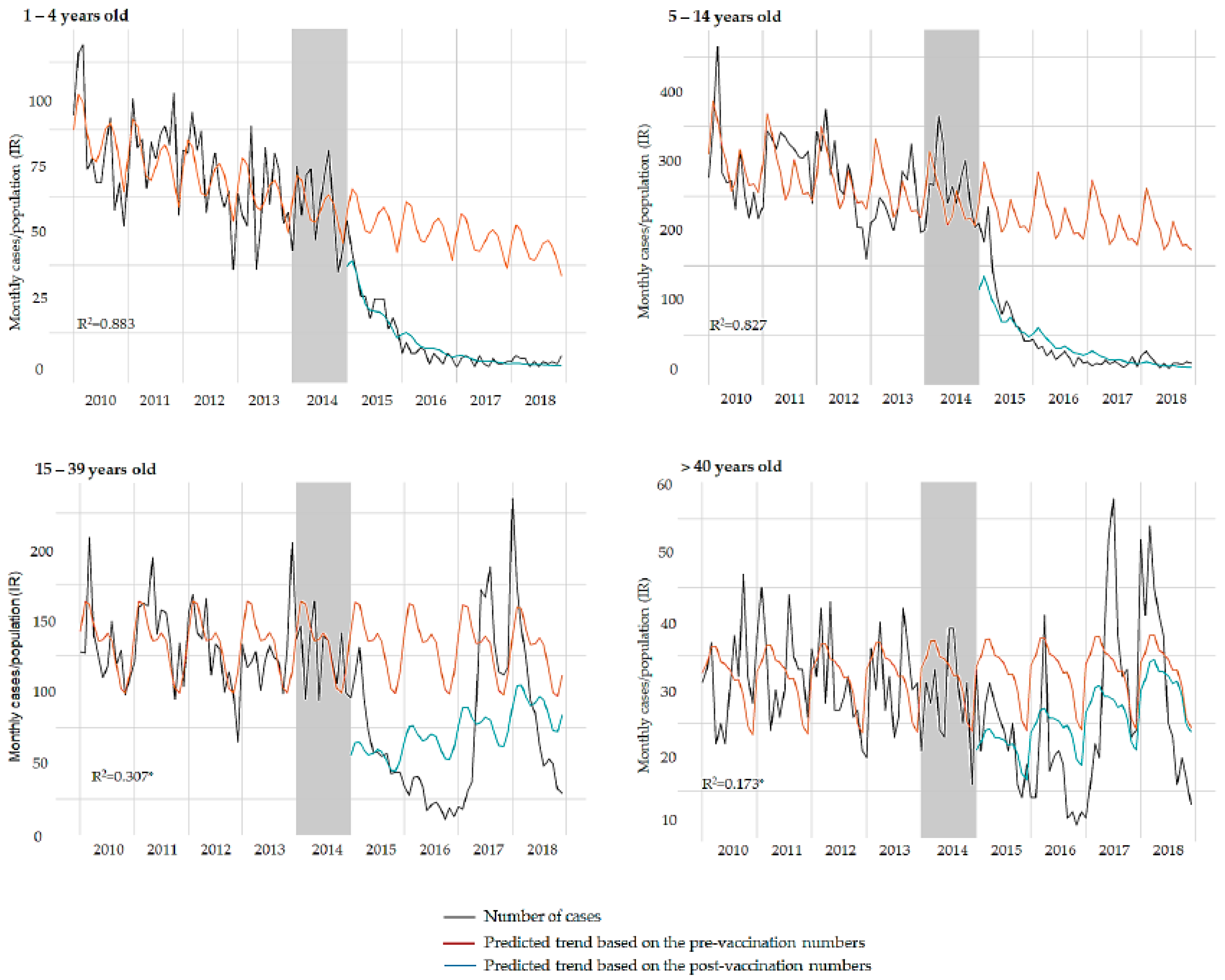
An interrupted time-series analysis was performed to assess changes in hepatitis A incidence rate in Brazil from 2010 to 2018. An inactivated hepatitis A vaccine (Vaqta™ Ped/Adol vaccine, 25U of inactivated HAV antigen—Merck & Co., Inc., Kenilworth, NJ, USA) was incorporated in the Brazilian NIP in July 2014. We analyzed the period before (2010–2013) and after (2015–2018) the introduction of hepatitis A vaccine in the NIP, excluding the year 2014, considered as a transition period. The time-series analysis was conducted for the following age groups: 1–4 years old (target immunization population); 5–14 years old; 15–39 years old; over 40 years old. A secondary time-series analysis was performed to account for the outbreak among young adults in the Southeast region between 2017 and 2018 [
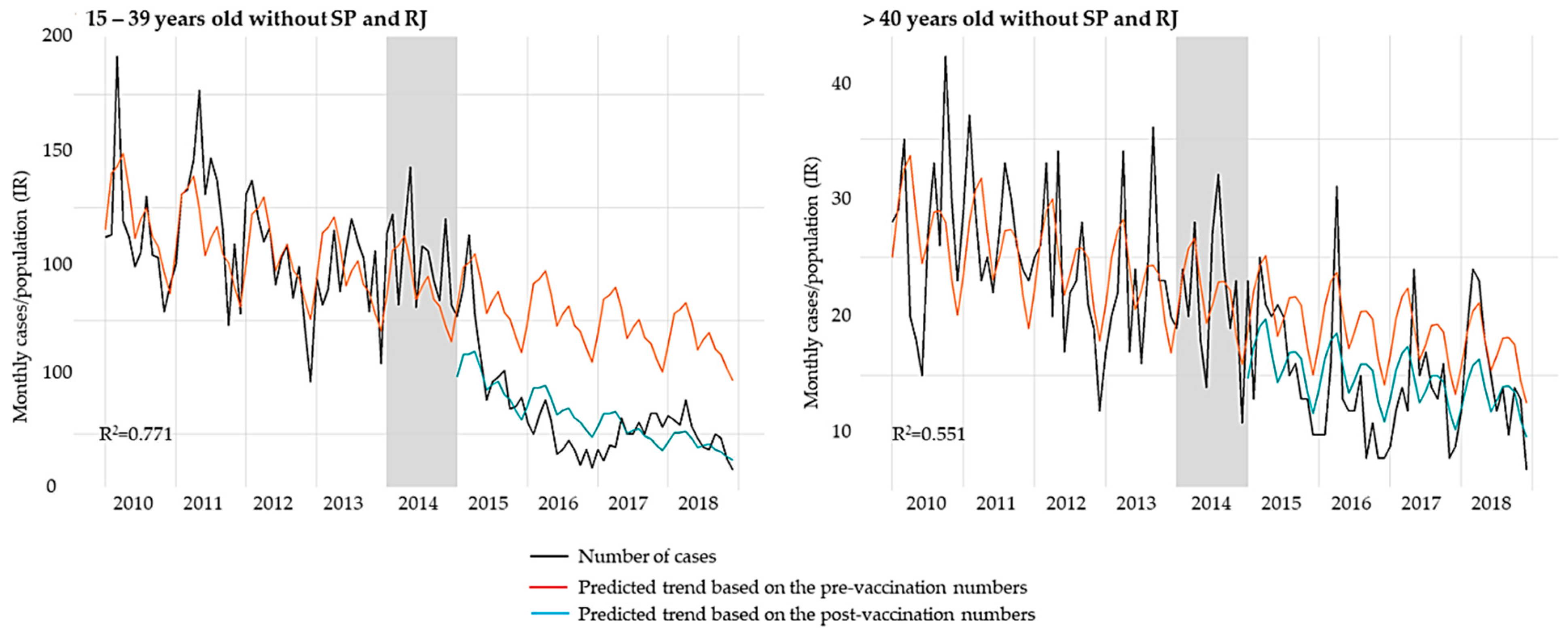
14]. To project an outbreak-free scenario, this analysis considered the age groups of 15–39 years and over 40 years old, in addition to the overall population, and excluded data from the main affected states, São Paulo and Rio de Janeiro. Additionally, the hepatitis A incidence rate was analyzed for the five geographic regions of Brazil: North, Northeast, Center-West, Southeast, and South. The total number of fulminant hepatitis cases was also assessed in the pre- and post-vaccination period.
2.2. Data Sources
Data were extracted from the Brazilian National Epidemiologic Surveillance System (SINAN), made available by the Brazilian IT Department of Public Healthcare System (DATASUS). Since 1996, all viral hepatitis cases (suspicious and confirmed) are classified as diseases of compulsory notification, and data are publicly available in the SINAN database. We extracted all confirmed hepatitis A cases reported between January 2010 and December 2018 in Brazil, defined as those with positive IgM anti-HAV or those that have detected HAV RNA or those that meet the clinical criteria and had contact with a laboratory-confirmed hepatitis A prior to onset of symptoms (e.g., household or sexual) or those that have died due to hepatitis A, as registered in the national mortality information system. Data were stratified according to age group and geographic region. Additionally, all cases classified in SINAN as fulminant hepatitis were extracted.
Data on vaccination coverage were extracted from the NIP Information System (SI-PNI), also made available by DATASUS. The estimates of vaccination coverage in Brazil are mainly obtained through administrative method, where the numerator is defined by the number of vaccine doses administered that are registered in the public health units, and the denominator is defined by the population census estimates. For both vaccination coverage and incidence rate calculations, the yearly population estimate was obtained from the census available in the Brazilian Institute of Geography and Statistics (IBGE) database.
2.3. Data Analysis
Vaccination coverage was defined as the total number of immunized in the target-population per total number of target-population, within the region and period of analysis. Incidence rate was the sum of all new cases of hepatitis A in the period of analysis per 100,000 inhabitants, using total population for each age group and geographic region according to the year of analysis.
A univariate Poisson regression model was used to compare the mean hepatitis A incidence rate in the pre-vaccination (from January 2010 to December 2013) and post-vaccination periods (from January 2015 to December 2018) across Brazilian regions. The overall mean incidence of fulminant hepatitis was also compared between pre- and post-vaccination periods.
For the interrupted time-series analysis, a generalized negative binomial linear model with linked logarithmic function was used to predict counterfactual hepatitis A cases that would have been expected in the absence of vaccination for the post-vaccination period. To convert the monthly cases of hepatitis A into a rate, the logarithmic function of the population divided by 100,000 was included as an offset variable, adjusting for any potential changes in the population over time. Data from the transition period (2014) were excluded. The vaccination effect on hepatitis A incidence rates was calculated per year after exponentiation of model coefficients (slope change) of both pre-vaccination (trend without vaccination effect) and post-vaccination (trend with vaccination effect) period. The immediate effect was the level change observed immediately after the vaccine introduction. The vaccine impact was assessed as the level change and as the counterfactual comparison with the post-vaccination trend. A simulation bootstrap with 1000 replications was used to estimate the total number of averted hepatitis A cases, represented as median and percentiles 2.5% and 97.5%.
4. Discussion
To our knowledge, this is the first study using interrupted time-series analysis to evaluate the impact of introducing a hepatitis A vaccine into the NIP on hepatitis A incidence rates, in the Brazilian population. Previous studies have demonstrated important reductions of hepatitis A incidence in all regions of Brazil after the vaccine introduction using other methodologies [
9,
13,
14,
15]. We found a significant immediate reduction (level change) of hepatitis A incidence rates in the overall population as well as in the target population for vaccination. The reduction of incidence rates per year (slope) was accentuated in the post-vaccination period compared to pre-vaccination period among children under 14 years of age. Over the period of 2015–2018, we estimated that 14,468 hepatitis A cases were prevented in Brazil after the vaccine introduction.
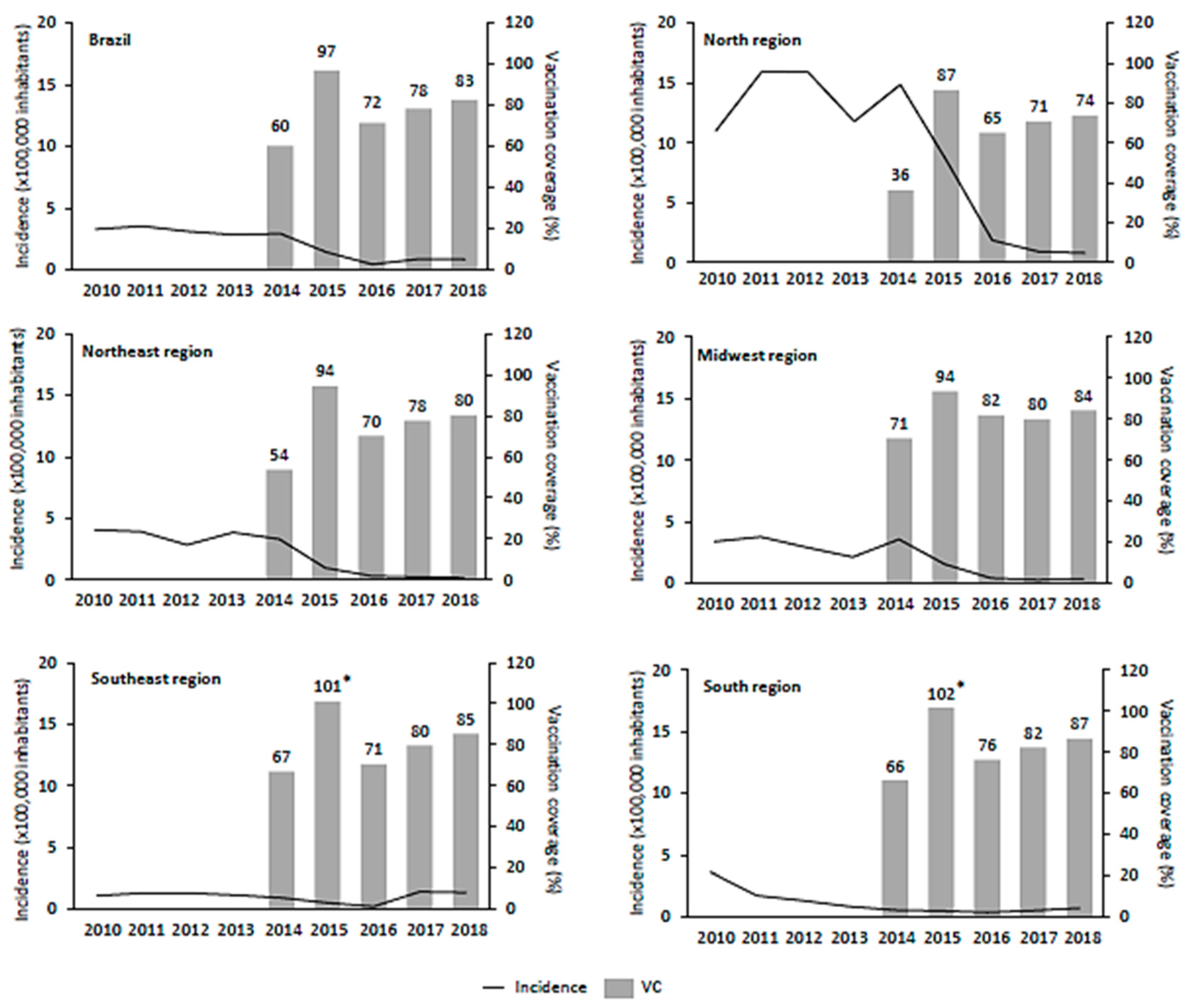
In Brazil, the inactivated hepatitis A vaccine was made universally available in mid-2014 as a single-dose vaccine for children aged 12–24 months and the vaccination coverage goal was set at 95% by the Ministry of Health. Since then, the national coverage goal has been achieved only once, in 2015, followed by a marked reduction in 2016 (
Figure 1). Nevertheless, a sustained vaccination coverage from 65% to 85% was reported between 2017 and 2019 with a slightly increasing trend over the years in all national territories. The drop in hepatitis A vaccination coverage in 2016 was consistent throughout all vaccines included in the childhood immunization schedule, probably due to multiple factors including lack of health education promotion on the benefits of vaccination and the change of the NIP information system from consolidated doses applied to nominal register [
13]. From 1994 until 2013, information on vaccine doses administered was provided by the municipalities administrators as aggregated data. Since 2014, the SI-PNI has gradually implemented an electronic national vaccination registry module with patient-level data, which depends on an adequate infrastructure and trained personal within the vaccination rooms of the municipalities to report the administered doses.
In the North region, despite the low baseline vaccination coverage (
Figure 1), we observed the greatest incidence decline within all regions. It represents the region with the lowest Human Development Index (HDI) in Brazil, with less access to, or availability of, education, health, water, and sanitation services. Only 55.4% of residents in the North region has access to water supply and 10.5% to sanitation services, contributing to a favorable environment for HAV transmission [
16]. In this region, it was very clear how vaccination policy can be used as a tool for closing health disparities between populations. Conversely, in the Southeast region, which has the highest HDI with better access to water and sanitation services [
16], the incidence rate in 2018 was higher than in 2010, even with sustained vaccination coverage >67% between 2014 and 2019. According to epidemiological reports [
17], this increase was mainly observed as a temporal and geographical cluster of cases in São Paulo and Rio de Janeiro states among young male adults [
14]. A secondary time-series analysis excluding the population affected by the outbreak demonstrated that the universal vaccination, paired with proper protection of adults with risk factors, could have reduced hepatitis A infection at a larger scale and a faster pace.
Since February 2016, hepatitis A outbreaks in MSM populations have been reported in many parts of the world including the major cities of Latin America [
3,
18,
19,
20]. Molecular epidemiology shows similar HAV strains circulating among HAV-infected MSM, suggesting a distinct route of transmission through sexual contact [
11]. Unlike Argentina, where vaccination is offered to the MSM population within the NIP, Brazil does not include this population among the individuals eligible to receive the vaccination. For this population, as well as for other individuals at substantial risk of contracting hepatitis A, the preferred regimen is the traditional two-dose schedule given 6–18 months apart [
13]. It is expected that a greater reduction in hepatitis A cases will occur when those immunized via the current NIP eventually become young adults. However, an immediate inclusion of the MSM population in the Brazilian NIP would be more effective in preventing hepatitis A outbreaks and HAV transmission [
21].
Compared to the results shown by Souto et al. [
10], our methodology discounted the effect of the decreasing pre-vaccination trends and, as expected, showed somewhat smaller population impact. Our results complement findings from studies in Argentina of the impact of a single-dose vaccine in reducing HAV circulation and symptomatic hepatitis A cases. In Argentina, fulminant hepatitis and liver transplantation also reduced drastically in a short period of time [
22,
23,
24]. In Brazil, although the overall fulminant hepatitis cases halved after the vaccine introduction, there was no statistical difference in the overall fulminant hepatitis incidence rate, likely due to low number of cases observed between 2010 and 2018. This difference between Argentina and Brazil was likely due to the seriousness of the baseline incidence in the former country.
Traditionally, the two-dose vaccine is recommended for complete immunization, offering approximately 99% effectiveness and up to 20 years long-term immunogenicity in real-world studies and ≥30 years in modeling studies [
25,
26,
27,
28,
29]. However, the 2012 WHO position paper on hepatitis A vaccines stated that national immunization programs may consider inclusion of single-dose inactivated hepatitis A vaccines in childhood immunization schedules [
10] based on experience in Argentina [
30]. This recommendation was followed by other low and middle income countries of Latin America as Brazil, Chile and Colombia introduced hepatitis A vaccination in their childhood immunization schedules [
31]. Other countries outside Latin America have shown similar positive effects after the use of a single-dose hepatitis A vaccine, such as Russia [
32]. Our study results mirror high immunogenicity acquired after the first dose of hepatitis A vaccine. Clinical trials conducted in the United States with inactivated hepatitis A vaccine showed protective antibody concentration in 92% of toddlers after a single dose and 100% after two doses [
33]. Longer term studies from Argentina have shown protective antibodies against HAV in 97.0% and 87.6% of Argentinean children after 9 and 11 years of the introduction, respectively [
34]. In Brazil, a preliminary study demonstrated that 93.6% of children seroconverted 30 days after the immunization [
15]. Further long-term assessments in the Brazilian population are required to confirm the seroprotective effect of a single-dose HAV vaccine.
The Global Burden of Disease (GBD) project estimates that hepatitis A resulted in 2.35 million (95% UI 1.70–3.09) global disability-adjusted life year (DALYs) in 2019 and was responsible for 53.9% (42.9–63.6) of acute hepatitis DALYs [
35]. In Americas WHO region, Latin America concentrated the highest burden of the disease. The findings of this study can provide useful information for policy makers in Latin America, a region characterized by middle-income countries with a mix of subpopulations with intermediate and low seroprevalences [
36], leaving a large proportion of adolescents and adults susceptible. Our results reassure the effectiveness of a single dose schedule and how hepatitis A national childhood immunization may be a proper disease prevention strategy in Latin America and other countries with similar epidemiological profile.
This study has some limitations innate to the database used to source epidemiological data. The hepatitis A incidence rate considered only the cases that were reported through SINAN database, either those symptomatic or those identified through routine assessments, considering both the public and private healthcare systems. Therefore, the number of hepatitis A cases could be underestimated. It is also important to emphasize that the vaccination coverage reported here was based on aggregated data provided by municipal administrators regarding total doses administrated annually and population census estimates. Thus, some variations in the values are expected due to the inherent biases in the methodology applied to estimate vaccination coverage. Finally, as this is a retrospective study based solely on data from government databases, the validity of data enclosed could not be verified through medical records. However, data is assumed to be both sensitive and specific, as collected as part of notifiable disease reporting and requiring a combination of laboratory and clinical criteria. Therefore, it is expected that this study represents a real-world scenario in Brazil.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}



