
The Association between Influenza Vaccination and COVID-19 and Its Outcomes: A Systematic Review and Meta-Analysis of Observational Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Data Sources and Search Strategy
2.3. Quality Assessment
2.4. Data Extraction
2.5. Data Synthesis and Statistical Analysis
3. Results
3.1. Study Selection and Study Characteristics
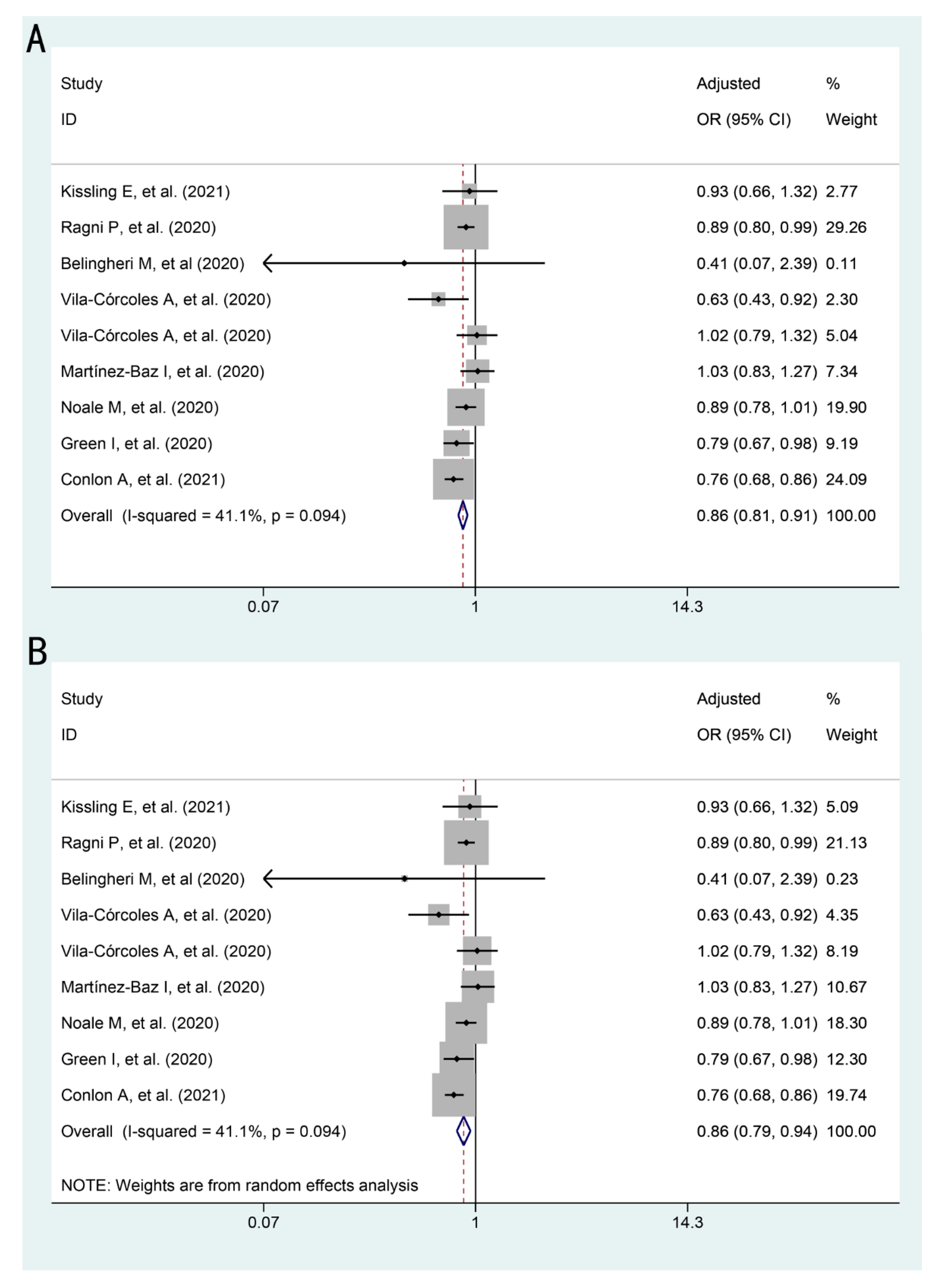
3.2. The Association between Influenza Vaccination and COVID-19 and Its Outcomes
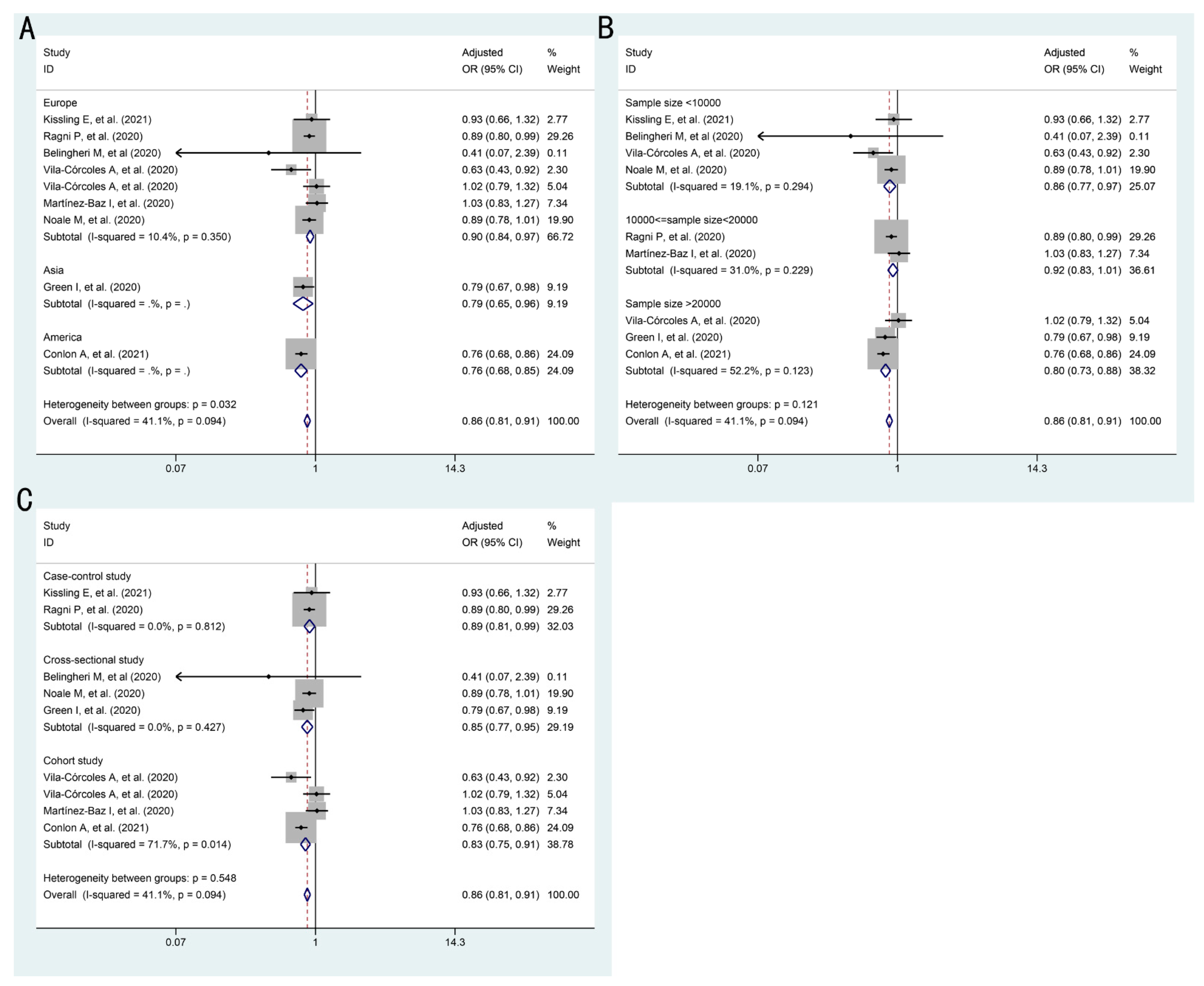
3.3. Subgroup Analysis
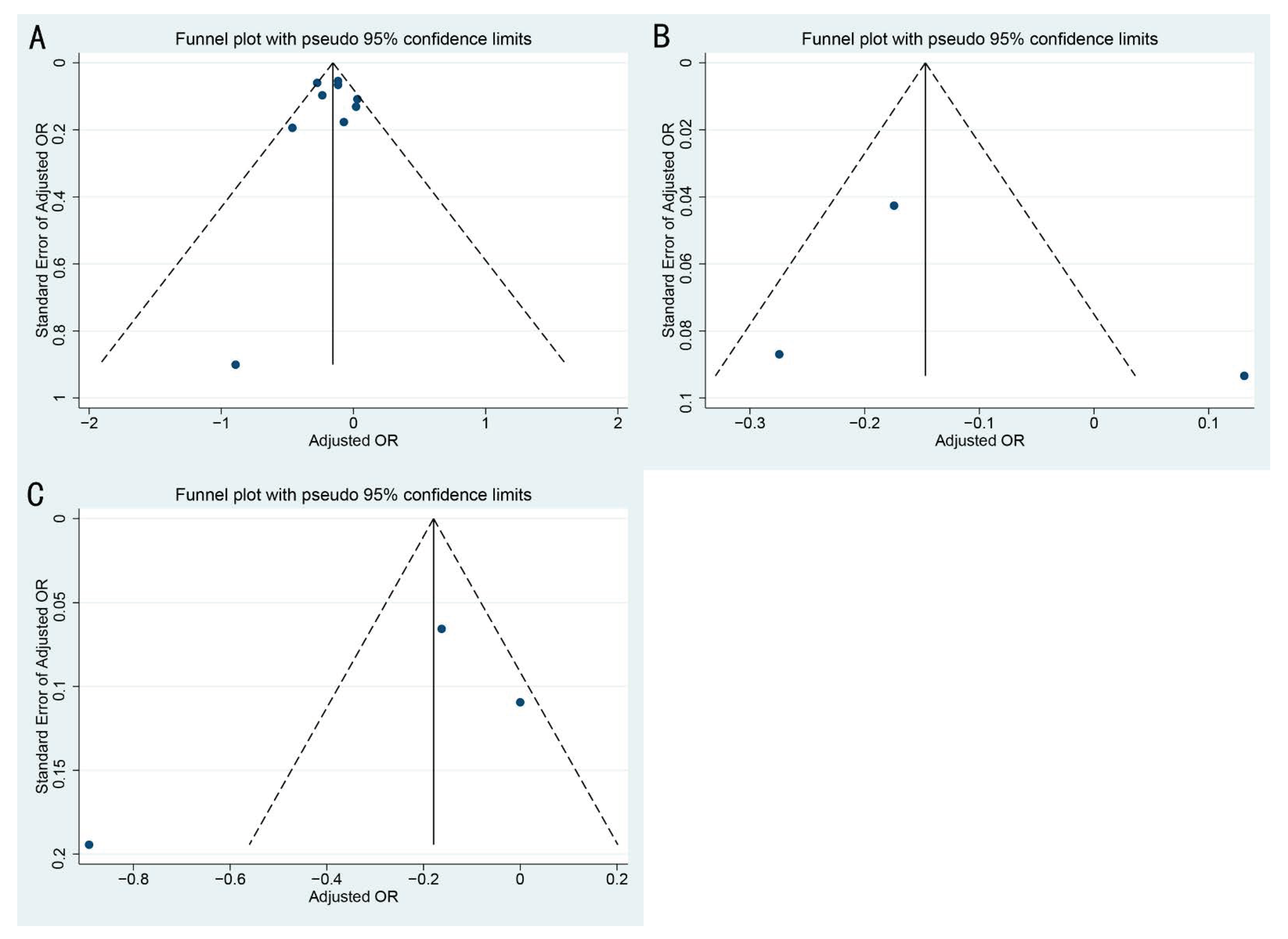
3.4. Publication Bias and Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update on COVID-19. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19 (accessed on 10 April 2021).
- Nelson, M.I.; Tan, Y.; Ghedin, E.; Wentworth, D.E.; St George, K.; Edelman, L.; Beck, E.T.; Fan, J.; Lam, T.T.-Y.; Kumar, S.; et al. Phylogeography of the spring and fall waves of the H1N1/09 pandemic influenza virus in the United States. J. Virol. 2011, 85, 828–834. [Google Scholar] [CrossRef] [Green Version]
- Bai, L.; Zhao, Y.; Dong, J.; Liang, S.; Guo, M.; Liu, X.; Wang, X.; Huang, Z.; Sun, X.; Zhang, Z.; et al. Coinfection with influenza A virus enhances SARS-CoV-2 infectivity. Cell. Res. 2021, 31, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Xiang, X.; Wang, Z.H.; Ye, L.L.; He, X.L.; Wei, X.S.; Ma, Y.L.; Li, H.; Chen, L.; Wang, X.R.; Zhou, Q. Co-infection of SARS-COV-2 and Influenza A Virus: A Case Series and Fast Review. Curr. Med. Sci. 2021, 41, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Konala, V.M.; Adapa, S.; Gayam, V.; Naramala, S.; Daggubati, S.R.; Kammari, C.B.; Chenna, A. Co-infection with Influenza A and COVID-19. Eur. J. Case. Rep. Intern. Med. 2020, 7, 001656. [Google Scholar] [PubMed]
- Buchy, P.; Badur, S. Who and when to vaccinate against influenza. Int. J. Infect. Dis. 2020, 93, 375–387. [Google Scholar] [CrossRef]
- Liu, Y.; Morgenstern, C.; Kelly, J.; Lowe, R.; Jit, M. The impact of non-pharmaceutical interventions on SARS-CoV-2 transmission across 130 countries and territories. BMC Med. 2021, 19, 40. [Google Scholar] [CrossRef]
- Moore, J.P.; Klasse, P.J. COVID-19 Vaccines: “Warp Speed” Needs Mind Melds, Not Warped Minds. J. Virol. 2020, 94, e01083-20. [Google Scholar] [CrossRef]
- Wolff, G.G. Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017–2018 influenza season. Vaccine 2020, 38, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.; Orlova-Fink, N.; Schindler, T.; Grisi, S.; Ferrer, A.P.S.; Daubenberger, C.; Brentani, A. Inactivated trivalent influenza vaccination is associated with lower mortality among patients with COVID-19 in Brazil. BMJ Evid. Based Med. 2020, in press. [Google Scholar] [CrossRef]
- Del Riccio, M.; Lorini, C.; Bonaccorsi, G.; Paget, J.; Caini, S. The Association between Influenza Vaccination and the Risk of SARS-CoV-2 Infection, Severe Illness, and Death: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2020, 17, 7870. [Google Scholar] [CrossRef]
- Cocco, P.; Meloni, F.; Coratza, A.; Schirru, D.; Campagna, M.; De Matteis, S. Vaccination against seasonal influenza and socio-economic and environmental factors as determinants of the geographic variation of COVID-19 incidence and mortality in the Italian elderly. Prev. Med. 2021, 143, 106351. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; Werba, J.P.; Frigerio, B.; Coggi, D.; Sansaro, D.; Ravani, A.; Ferrante, P.; Veglia, F.; Tremoli, E.; Baldassarre, D. Relationship between Influenza Vaccination Coverage Rate and COVID-19 Outbreak: An Italian Ecological Study. Vaccines 2020, 8, 535. [Google Scholar] [CrossRef] [PubMed]
- Arokiaraj, M.C. Considering Interim Interventions to Control COVID-19 Associated Morbidity and Mortality-Perspectives. Front. Public Health 2020, 8, 444. [Google Scholar] [CrossRef] [PubMed]
- Marín-Hernández, D.; Schwartz, R.E.; Nixon, D.F. Epidemiological evidence for association between higher influenza vaccine uptake in the elderly and lower COVID-19 deaths in Italy. J. Med. Virol. 2021, 93, 64–65. [Google Scholar] [CrossRef]
- Martínez-Baz, I.; Trobajo-Sanmartín, C.; Arregui, I.; Navascués, A.; Adelantado, M.; Indurain, J.; Fresán, U.; Ezpeleta, C.; Castilla, J. Influenza Vaccination and Risk of SARS-CoV-2 Infection in a Cohort of Health Workers. Vaccines 2020, 8, 611. [Google Scholar] [CrossRef]
- De la Cruz Conty, M.L.; Encinas Pardilla, M.B.; Garcia Sanchez, M.; Gonzalez Rodriguez, L.; Muner-Hernando, M.L.; Royuela Vicente, A.; Pintado Recarte, P.; Martinez Varea, A.; Martinez Diago, C.; Cruz Melguizo, S.; et al. Impact of Recommended Maternal Vaccination Programs on the Clinical Presentation of SARS-CoV-2 Infection: A Prospective Observational Study. Vaccines 2021, 9, 31. [Google Scholar] [CrossRef]
- Kissling, E.; Hooiveld, M.; Brytting, M.; Vilcu, A.M.; de Lange, M.; Martínez-Baz, I.; Sigerson, D.; Enkirch, T.; Belhillil, S.; Meijer, A.; et al. Absence of association between 2019-20 influenza vaccination and COVID-19: Results of the European I-MOVE-COVID-19 primary care project, March-August 2020. Influenza Other Respir. Viruses. in press.
- Wells, G.A.; Shea, B.; O’Connell, D.a.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 April 2021).
- Rostom, A.; Dube, C.; Cranney, A. Rockville (MD): Agency for Healthcare Research and Quality (US). Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK35156/ (accessed on 1 April 2021).
- Massoudi, N.; Mohit, B. A Case–Control Study of the 2019 Influenza Vaccine and Incidence of COVID-19 among Healthcare Workers. J. Clin. Immunol. 2021, 41, 324–334. [Google Scholar] [CrossRef]
- Ragni, P.; Marino, M.; Formisano, D.; Bisaccia, E.; Scaltriti, S.; Bedeschi, E.; Grilli, R. Association between Exposure to Influenza Vaccination and COVID-19 Diagnosis and Outcomes. Vaccines 2020, 8, 675. [Google Scholar] [CrossRef]
- Belingheri, M.; Paladino, M.E.; Latocca, R.; De Vito, G.; Riva, M.A. Association between seasonal flu vaccination and COVID-19 among healthcare workers. Occup. Med. 2020, 70, 665–671. [Google Scholar] [CrossRef]
- Vila-Córcoles, Á.; Ochoa-Gondar, O.; Torrente-Fraga, C.; Vila-Rovira, Á.; Satué-Gracia, E.; Hospital-Guardiola, I.; de Diego-Cabanes, C.; Gómez-Bertomeu, F.; Basora-Gallisà, J. Evaluation of incidence and risk profile for suffering Covid-19 infection by underlying conditions among middle-aged and older adults in Tarragona. Rev. Esp. Salud. Publica 2020, 94, e202006065. [Google Scholar]
- Vila-Córcoles, A.; Ochoa-Gondar, O.; Satué-Gracia, E.M.; Torrente-Fraga, C.; Gomez-Bertomeu, F.; Vila-Rovira, A.; Hospital-Guardiola, I.; de Diego-Cabanes, C.; Bejarano-Romero, F.; Basora-Gallisà, J. Influence of prior comorbidities and chronic medications use on the risk of COVID-19 in adults: A population-based cohort study in Tarragona, Spain. BMJ Open 2020, 10, e041577. [Google Scholar] [CrossRef]
- Pawlowski, C.; Puranik, A.; Bandi, H.; Venkatakrishnan, A.J.; Agarwal, V.; Kennedy, R.; O’Horo, J.C.; Gores, G.J.; Williams, A.W.; Halamka, J.; et al. Exploratory analysis of immunization records highlights decreased SARS-CoV-2 rates in individuals with recent non-COVID-19 vaccinations. Sci. Rep. 2021, 11, 4741. [Google Scholar] [CrossRef] [PubMed]
- Jehi, L.; Ji, X.; Milinovich, A.; Erzurum, S.; Rubin, B.P.; Gordon, S.; Young, J.B.; Kattan, M.W. Individualizing Risk Prediction for Positive Coronavirus Disease 2019 Testing: Results From 11,672 Patients. Chest 2020, 158, 1364–1375. [Google Scholar] [CrossRef] [PubMed]
- Noale, M.; Trevisan, C.; Maggi, S.; Antonelli Incalzi, R.; Pedone, C.; Di Bari, M.; Adorni, F.; Jesuthasan, N.; Sojic, A.; Galli, M.; et al. The Association between Influenza and Pneumococcal Vaccinations and SARS-Cov-2 Infection: Data from the EPICOVID19 Web-Based Survey. Vaccines 2020, 8, 471. [Google Scholar] [CrossRef] [PubMed]
- Green, I.; Ashkenazi, S.; Merzon, E.; Vinker, S.; Golan-Cohen, A. The association of previous influenza vaccination and coronavirus disease-2019. Hum. Vaccines Immunother. in press.
- Conlon, A.; Ashur, C.; Washer, L.; Eagle, K.A.; Hofmann Bowman, M.A. Impact of the influenza vaccine on COVID-19 infection rates and severity. Am. J. Infect. Control 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.R.; Islam, N.; Dambha-Miller, H. Association between influenza vaccination and hospitalisation or all-cause mortality in people with COVID-19: A retrospective cohort study. BMJ Open. Respir. Res. 2021, 8, e000857. [Google Scholar] [CrossRef]
- Yang, M.J.; Rooks, B.J.; Le, T.T.; Santiago, I.O., 3rd; Diamond, J.; Dorsey, N.L.; Mainous, A.G., 3rd. Influenza Vaccination and Hospitalizations among COVID-19 Infected Adults. J. Am. Board Fam. Med. 2021, 34, S179–S182. [Google Scholar] [CrossRef]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Deployment of COVID-19 Vaccines. Available online: https://en.wikipedia.org/wiki/Deployment_of_COVID-19_vaccines#cite_note-world-total-18 (accessed on 10 April 2021).
- Grubaugh, N.D.; Hanage, W.P.; Rasmussen, A.L. Making Sense of Mutation: What D614G Means for the COVID-19 Pandemic Remains Unclear. Cell 2020, 182, 794–795. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Yue, N.; Zheng, M.; Wang, D.; Duan, C.; Yu, X.; Zhang, X.; Bao, C.; Jin, H. Influenza vaccination coverage of population and the factors influencing influenza vaccination in mainland China: A meta-analysis. Vaccine 2018, 36, 7262–7269. [Google Scholar] [CrossRef]
- Quach, T.H.T.; Mallis, N.A.; Cordero, J.F. Influenza Vaccine Efficacy and Effectiveness in Pregnant Women: Systematic Review and Meta-analysis. Matern. Child Health J. 2020, 24, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, K.; Wei, Y.; Szwajcer, A.; Rabbani, R.; Zarychanski, R.; Abou-Setta, A.M.; Mahmud, S.M. Efficacy and safety of high-dose influenza vaccine in elderly adults: A systematic review and meta-analysis. Vaccine 2017, 35, 2775–2780. [Google Scholar] [CrossRef]
- Restivo, V.; Costantino, C.; Bono, S.; Maniglia, M.; Marchese, V.; Ventura, G.; Casuccio, A.; Tramuto, F.; Vitale, F. Influenza vaccine effectiveness among high-risk groups: A systematic literature review and meta-analysis of case-control and cohort studies. Hum. Vaccines Immunother. 2018, 14, 724–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Cao, X.; Cao, Z.; Xu, C.; Sun, L.; Gao, Y.; Wang, Y.; Li, S.; Wu, C.; Li, X.; et al. Effects of influenza vaccination on the risk of cardiovascular and respiratory diseases and all-cause mortality. Ageing Res. Rev. 2020, 62, 101124. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Huedo, M.A.; Lopez-De-Andrés, A.; Mora-Zamorano, E.; Hernández-Barrera, V.; Jiménez-Trujillo, I.; Zamorano-Leon, J.J.; Jiménez-García, R. Decreasing influenza vaccine coverage among adults with high-risk chronic diseases in Spain from 2014 to 2017. Hum. Vaccines Immunother. 2020, 16, 95–99. [Google Scholar] [CrossRef]
- Tian, C.; Wang, H.; Wang, W.; Luo, X. Influenza vaccination coverage among US children from 2004/2005 to 2015/2016. J. Public Health 2018, 41, e62–e69. [Google Scholar] [CrossRef]
- Descamps, A.; Launay, O.; Bonnet, C.; Blondel, B. Seasonal influenza vaccine uptake and vaccine refusal among pregnant women in France: Results from a national survey. Hum. Vaccines Immunother. 2020, 16, 1093–1100. [Google Scholar] [CrossRef]
- Paget, J.; Caini, S.; Cowling, B.; Esposito, S.; Falsey, A.R.; Gentile, A.; Kyncl, J.; MacIntyre, C.; Pitman, R.; Lina, B. The impact of influenza vaccination on the COVID-19 pandemic? Evidence and lessons for public health policies. Vaccine 2020, 38, 6485–6486. [Google Scholar] [CrossRef]
- Thindwa, D.; Garcia Quesada, M.; Liu, Y.; Bennett, J.; Cohen, C.; Knoll, M.D.; von Gottberg, A.; Hayford, K.; Flasche, S. Use of seasonal influenza and pneumococcal polysaccharide vaccines in older adults to reduce COVID-19 mortality. Vaccine 2020, 38, 5398–5401. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; Domínguez-Andrés, J.; Barreiro, L.B.; Chavakis, T.; Divangahi, M.; Fuchs, E.; Joosten, L.A.B.; van der Meer, J.W.M.; Mhlanga, M.M.; Mulder, W.J.M.; et al. Defining trained immunity and its role in health and disease. Nat. Rev. Immunol. 2020, 20, 375–388. [Google Scholar] [CrossRef] [Green Version]
- Kleinnijenhuis, J.; Quintin, J.; Preijers, F.; Joosten, L.A.; Jacobs, C.; Xavier, R.J.; van der Meer, J.W.; van Crevel, R.; Netea, M.G. BCG-induced trained immunity in NK cells: Role for non-specific protection to infection. Clin. Immunol. 2014, 155, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walk, J.; de Bree, L.C.J.; Graumans, W.; Stoter, R.; van Gemert, G.J.; van de Vegte-Bolmer, M.; Teelen, K.; Hermsen, C.C.; Arts, R.J.W.; Behet, M.C.; et al. Outcomes of controlled human malaria infection after BCG vaccination. Nat. Commun. 2019, 10, 874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, K.P.Y.; Cheung, M.C.; Perera, R.; Ng, K.C.; Bui, C.H.T.; Ho, J.C.W.; Ng, M.M.T.; Kuok, D.I.T.; Shih, K.C.; Tsao, S.W.; et al. Tropism, replication competence, and innate immune responses of the coronavirus SARS-CoV-2 in human respiratory tract and conjunctiva: An analysis in ex-vivo and in-vitro cultures. Lancet Respir. Med. 2020, 8, 687–695. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Vaccination Season | Identification of COVID-19 | Country | Sample Size | Infected (n)/Vaccinated(n) | Infected (n)/Unvaccinated (n) | Adjusted Estimate (95%CI) | Quality Score and Risk of Bias Assessment | Adjusted Factors |
|---|---|---|---|---|---|---|---|---|---|---|
| Massoudi et al., (2021) [21] | Case-control study | 2019–2020 | pulmonologist-confirmed | Iran | 261 | 3/90 | 77/171 | - | 6(moderate) | - |
| Kissling et al., (2021) [18] | Case-control study | 2019–2020 | rt-PCR | Europe a | 1701 | 68/429 | 157/1272 | 0.93 (0.66–1.32) | 8 (low) | Study site, time, age, sex, and chronic condition |
| Ragni et al., (2020) [22] | Case-control study | 2019–2020 | rt-PCR | Italy | 17,608 | 1676/5427 | 3209/12,181 | 0.89 (0.80–0.99) | 9 (low) | Age, sex, Charlson index, and time of the swab test |
| Belingheri et al., (2020) [23] | Cross-sectional study | 2019–2020 | rt-PCR | Italy | 3520 | 28/817 | 100/2703 | 0.41 (0.07–2.39) | 7 (low) | Age, sex, and an interaction term between age and the vaccination intake in 2019/3020 |
| Vila-Córcoles et al., (2020) [24] | Retrospective cohort study | 2019–2020 | rt-PCR | Spain | 1547 | 189/705 | 160/842 | 0.63 (0.43–0.92) b | 8 (low) | Age, sex, and comorbidities |
| Pawlowski et al., (2021) [26] | Retrospective cohort study | 2019–2020 | rt-PCR | America | 25,582 | 442/12,791 | 521/12,791 | - | 8 (low) | - |
| Jehi et al., (2020) [27] | Prospective cohort study | -c | rt-PCR | America | 11,672 | 384/6324 | 434/5348 | - | 7 (low) | - |
| Vila-Córcoles et al., (2020) d [25] | Retrospective cohort study | 2019–2020 | rt-PCR | Spain | 78,883 | 205/22,606 | 175/56,277 | 1.02 (0.79–1.32) b | 7 (low) | Age, sex, comorbidities, and medications use. |
| Martínez-Baz et al., (2020) e [16] | Prospective cohort study | 2019–2020 | rt-PCR | Spain | 10,714 | 155/3677 | 248/7037 | 1.03 (0.83–1.27) | 7 (low) | Age groups, sex, major chronic conditions, profession, and any ILI diagnosis in the previous five years |
| Noale et al., (2020) [28] | Cross-sectional study | 2019–2020 | rt-PCR | Italy | 6680 | 562/2246 | 1114/4434 | 0.89 (0.78–1.01) | 8 (low) | Age, sex, education, area of residence, self-reported comorbidities, and smoking status |
| Green et al., (2020) [29] | Cross-sectional study | 2019–2020 | rt-PCR | Israel | 22,563 | 244/4711 | 1580/17,852 | 0.79 (0.67–0.98) | 9 (low) | Age, ethnic, smoking status, socioeconomic status, and comorbidities |
| Conlon et al., (2021) [30] | Retrospective cohort study | 2019–2020 | rt-PCR | America | 27,201 | 525/12,997 | 693/14,204 | 0.76 (0.68–0.86) | 8 (low) | Ethnicity, race, sex, age, BMI, Elixhauser score, smoking status, and comorbidities |
| Study | Study Design | Vaccination Season | Identification of COVID-19 | Country | Sample Size | Events (n)/Vaccinated(n) | Events (n)/Unvaccinated (n) | Adjusted Estimate (95%CI) | Quality Score and Risk of Bias Assessment | Adjusted Factors |
|---|---|---|---|---|---|---|---|---|---|---|
| Intensive Care | ||||||||||
| Pawlowski et al., (2020) [26] | Retrospective cohort study | 2019–2020 | rt-PCR | America | 959 | 15/441 | 16/518 | - | 8 (low) | - |
| de la Cruz Conty et al., (2021) a [17] | Prospective cohort study | - b | rt-PCR | Spain | 1150 | 7/438 | 15/712 | - | 7 (low) | - |
| Fink et al., (2020) [10] | Retrospective cohort study | - b | Clinical diagnosisc | Brazil | 53,752 | - | - | 0.93 (0.87–0.99) | 7 (low) | Age, sex, race, educational level, treatment facility, and comorbidities |
| Yang et al., (2021) [32] | Retrospective cohort study | 2019–2020 | rt-PCR | America | 2005 | 3/214 | 133/1791 | 0.30 (0.07–0.85) | 8 (low) | Age, sex race/ethnicity, hypertension, and comorbidities |
| Hospitalization | ||||||||||
| Pawlowski et al., (2020) [26] | Retrospective cohort study | 2019–2020 | rt-PCR | America | 959 | 74/441 | 78/518 | - | 8 (low) | - |
| Yang et al., (2021) [32] | Retrospective cohort study | 2019–2020 | rt-PCR | America | 2005 | 43/214 | 747/1791 | 0.41 (0.28–0.60) | 8 (low) | Age, sex race/ethnicity, hypertension, and comorbidities |
| Ragni et al., (2020) [22] | retrospective cohort study | 2019–2020 | rt-PCR | Italy | 17,608 | - | - | 0.84 (0.83–1.29) d | 7 (low) | Age, sex, Charlson index, and time of the swab test |
| Wilcox et al., (2021) e [31] | retrospective cohort study | 2019–2020 | rt-PCR | England | 6921 | 1166/2613 | 1584/4308 | 0.85 (0.75–0.97) | 8 (low) | Age, sex, BMI, socioeconomic status, smoking status, frailty score, comorbidities, and the number of prescribed medications |
| Mortality | ||||||||||
| Fink et al., (2020) [10] | Retrospective cohort study | - b | Clinical diagnosis c | Brazil | 53,752 | - | - | 0.84 (0.77–0.91) | 7 (low) | Age, sex, race, educational level, treatment facility, and comorbidities |
| Ragni et al., (2020) [22] | retrospective cohort study | 2019–2020 | rt-PCR | Italy | 17,608 | - | - | 1.14 (0.95–1.37) d | 7 (low) | Age, sex, Charlson index, and time of the swab test |
| Wilcox et al., (2021) [31] | retrospective cohort study | 2019–2020 | rt-PCR | England | 6921 | 372/2613 | 553/4308 | 0.76 (0.64–0.90) | 8 (low) | Age, sex, BMI, socioeconomic status, smoking status, frailty score, comorbidities, and the number of prescribed medications |
| Outcomes | Number of Studies | I2 Value (%) | p Value | Adjusted Estimates a (95%CI) | |
|---|---|---|---|---|---|
| Fixed Effects Model | Random Effects Model | ||||
| SARS-CoV-2 infection | 9 | 41.1 | 0.09 | 0.86 (0.81–0.91) | 0.86 (0.79–0.94) |
| Intensive care | 2 | 68.2 | 0.08 | 0.93 (0.87–0.99) | 0.63 (0.22–1.81) |
| Hospitalization | 3 | 87.6 | <0.01 | 0.84 (0.75–0.93) | 0.74 (0.51–1.06) |
| Mortality | 3 | 82.5 | <0.01 | 0.86 (0.81–0.93) | 0.89 (0.73–1.09) |
| Grouping Variables | No. of Studies | Random Effects Model | Fixed Effects Model | ||||
|---|---|---|---|---|---|---|---|
| Adjusted Estimate (95%CI) | I2 Value (%) | p Value | Adjusted Estimate (95%CI) | I2 Value (%) | p Value | ||
| Region | 9 | 0.04 a | 0.03 a | ||||
| Europe | 7 | 0.91 (0.84–0.98) | 10.4 | <0.01 b | 0.90 (0.84–0.97) | 10.4 | <0.01 b |
| Asia | 1 | 0.79 (0.65–0.96) | - | - | 0.79 (0.65–0.96) | - | - |
| America | 1 | 0.76 (0.68–0.85) | - | - | 0.76 (0.68–0.85) | - | - |
| Sample size | 9 | 0.34 a | 0.06 a | ||||
| Sample size <20,000 | 6 | 0.89 (0.82–0.97) | 13.3 | 0.33 b | 0.89 (0.83–0.96) | 13.3 | 0.33 b |
| Sample size ≥20,000 | 3 | 0.82 (0.71–0.96) | 52.2 | 0.12 b | 0.80 (0.73–0.88) | 52.2 | 0.12 b |
| Study design | 9 | 0.83 a | 0.55 a | ||||
| Case-control study | 2 | 0.89 (0.81–0.99) | 0.0 | 0.81 b | 0.89 (0.81–0.99) | 0.0 | 0.81 b |
| Cross-sectional study | 3 | 0.85 (0.77–0.95) | 0.0 | 0.43 b | 0.85 (0.77–0.95) | 0.0 | 0.43 b |
| Cohort study | 4 | 0.86 (0.70–1.05) | 71.7 | 0.01 b | 0.83 (0.75–0.91) | 71.7 | 0.01 b |
| Outcomes | t Value | p Value |
|---|---|---|
| SARS-CoV-2 infection | −0.19 | 0.85 |
| Mortality | 0.46 | 0.73 |
| Hospitalization | −0.87 | 0.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, R.; Liu, M.; Liu, J. The Association between Influenza Vaccination and COVID-19 and Its Outcomes: A Systematic Review and Meta-Analysis of Observational Studies. Vaccines 2021, 9, 529. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9050529
Wang R, Liu M, Liu J. The Association between Influenza Vaccination and COVID-19 and Its Outcomes: A Systematic Review and Meta-Analysis of Observational Studies. Vaccines. 2021; 9(5):529. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9050529
Chicago/Turabian StyleWang, Ruitong, Min Liu, and Jue Liu. 2021. "The Association between Influenza Vaccination and COVID-19 and Its Outcomes: A Systematic Review and Meta-Analysis of Observational Studies" Vaccines 9, no. 5: 529. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9050529