
Using Household Surveys to Assess Missed Opportunities for Simultaneous Vaccination: Longitudinal Examples from Colombia and Nigeria

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Sources of Data
2.2. Data Analysis
3. Definitions
3.1. Visit-Based Analyses
3.2. Child-Based Analyses
4. Results
4.1. Background Information on the Survey Populations
4.2. MOSV, Visit-Based Analyses
4.3. MOSV, Child-Based Analyses
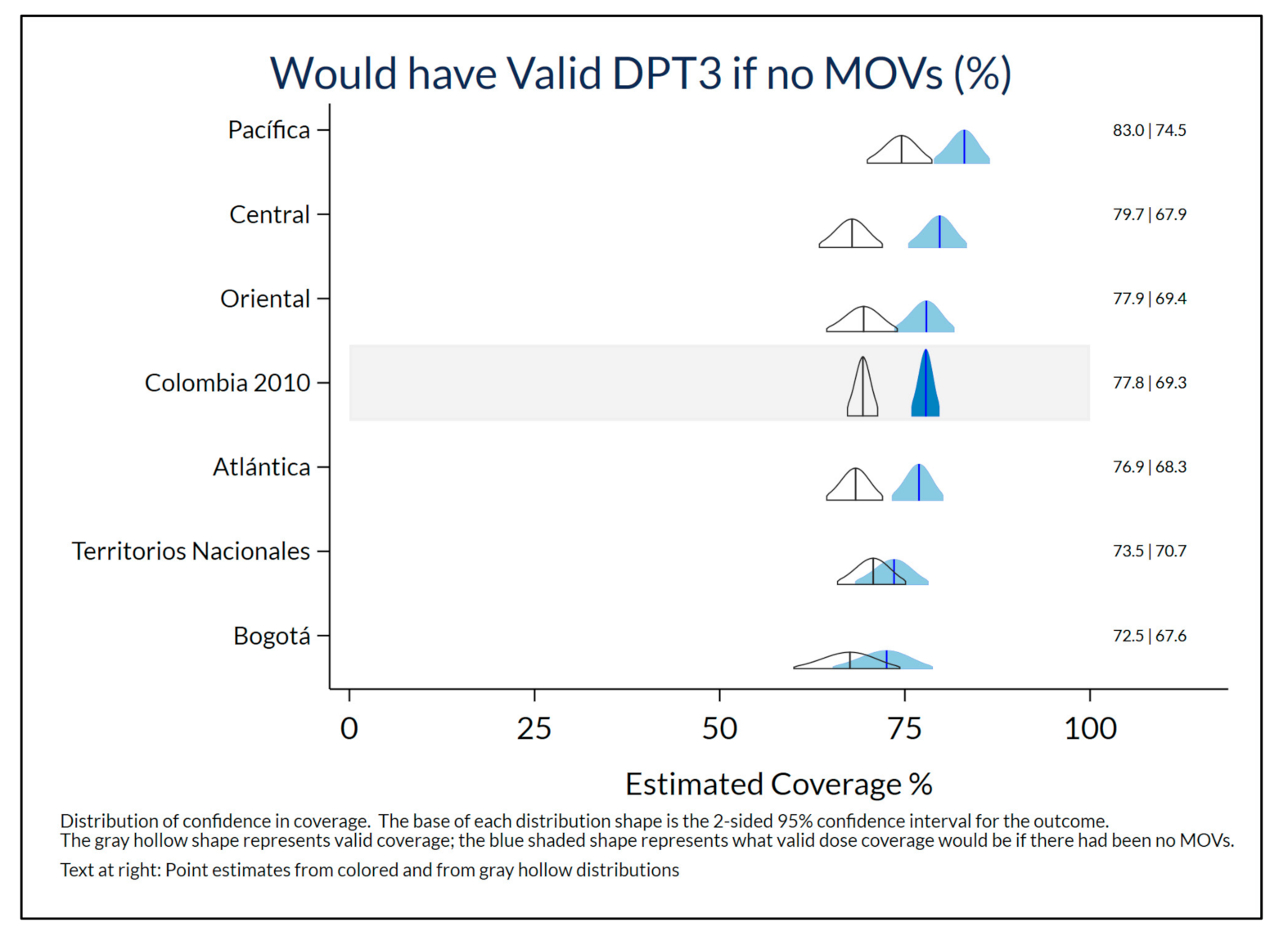
4.4. Potential Consequences
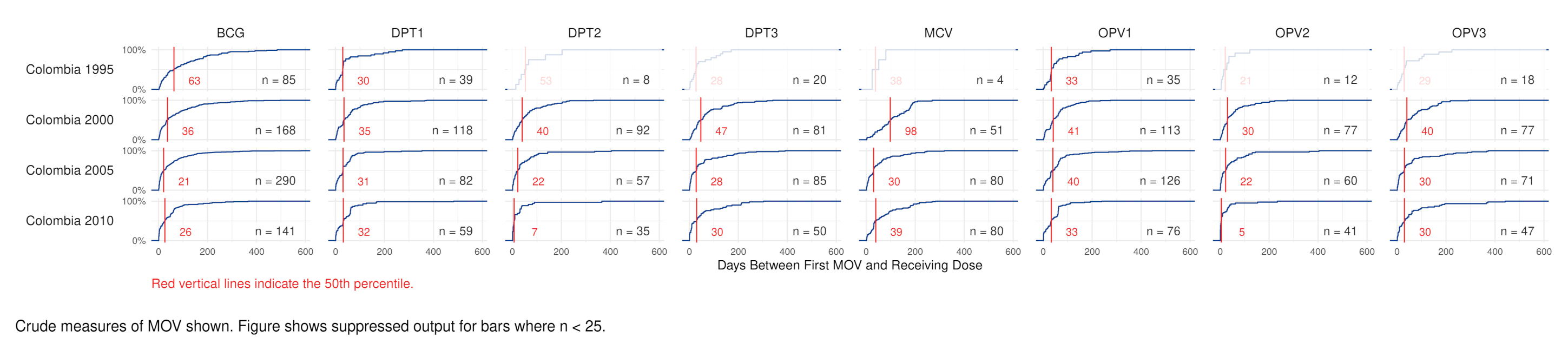
4.5. Delay to Receipt of Missed Doses
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hutchins, S.S.; Jansen, H.A.; Robertson, S.E.; Evans, P.; Kim-Farley, R.J. Studies of missed opportunities for immunization in developing and industrialized countries. Bull. World Health Organ. 1993, 71, 549–560. [Google Scholar] [PubMed]
- WHO. Missed Opportunities for Vaccination (MOV) Strategy. Missed Opportunities for Vaccination (MOV) Strategy 2020. Available online: https://www.who.int/immunization/programmes_systems/policies_strategies/MOV/en/ (accessed on 17 April 2020).
- World Health Organization. Leave No One Behind: Guidance for Planning and Implementing Catch-up Vaccination; Working Draft; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Mandomando, I.; Mumba, M.; Biey, J.N.-M.; Paluku, G.K.; Weldegebriel, G.; Mwenda, J.M. Implementation of the World Health Organization recommendation on the use of rotavirus vaccine without age restriction by African countries. Vaccine 2021, 39, 3111–3119. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Vaccine Position Papers 2020. Available online: https://www.who.int/immunization/documents/positionpapers/en/ (accessed on 31 May 2021).
- Galazka, A.M.; Lauer, B.A.; Henderson, R.H.; Keja, J. Indications and contraindications for vaccines used in the Expanded Programme on Immunization. Bull. World Health Organ. 1984, 62, 357–366. [Google Scholar] [PubMed]
- WHO. EPI Missed Immunization Opportunities. Wkly. Epidemiol. Rec. 1984, 59, 341. [Google Scholar]
- World Health Organization. Immunization Agenda 2030—A Global Strategy to Leave No One Behind. World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Lancet, T. 2021: The beginning of a new era of immunisations? Lancet 2021, 397, 1519. [Google Scholar] [CrossRef]
- Sato, P. Protocol for the Assessment of Missed Opportunities for Immunization; World Health Organization: Geneva, Switzerland, 1988. [Google Scholar]
- Pan American Health Organization. Methodology for the Evaluation of Missed Opportunities for Vaccination; Pan American Health Organization (PAHO): Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. Methodology for the Assessment of Missed Opportunities for Vaccination; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Sridhar, S.; Maleq, N.; Guillermet, E.; Colombini, A.; Gessner, B.D. A systematic literature review of missed opportunities for immunization in low- and middle-income countries. Vaccine 2014, 32, 6870–6879. [Google Scholar] [CrossRef]
- Cutts, F.; Soares, A.; Jecque, A.V.; Cliff, J.; Kortbeek, S.; Colombo, S. The use of evaluation to improve the Expanded Programme on Immunization in Mozambique. Bull. World Health Organ. 1990, 68, 199–208. [Google Scholar] [PubMed]
- Cutts, F.T.; Diallo, S.; Zell, E.R.; Rhodes, P. Determinants of Vaccination in an Urban Population in Conakry, Guinea. Int. J. Epidemiology 1991, 20, 1099–1106. [Google Scholar] [CrossRef]
- Cutts, F.T.; Zell, E.R.; Soares, A.C.; Diallo, S. Obstacles to Achieving Immunization for all 2000: Missed Immunization Opportunities and Inappropriately Timed Immunization. J. Trop. Pediatr. 1991, 37, 153–158. [Google Scholar] [CrossRef]
- Gindler, J.S.; Cutts, F.T.; Barnett-Antinori, M.E.; Zell, E.R.; Swint, E.B.; Hadler, S.C.; Rullán, J.V. Successes and failures in vaccine delivery: Evaluation of the immunization delivery system in Puerto Rico. Pediatrics 1993, 91, 315–320. [Google Scholar]
- Kahn, J.G.; Mokdad, A.H.; Deming, M.S.; Roungou, J.B.; Boby, A.M.; Excler, J.L.; Waldman, R.J. Avoiding missed opportunities for immunization in the Central African Republic: Potential impact on vaccination coverage. Bull. World Health Organ. 1995, 73, 47–55. [Google Scholar]
- Dammann, D.F.; Solarsh, G.C. The use of COSAS in the analysis of vaccination coverage in urban, peri-urban and rural populations in the Edendale/Vulindlela district of KwaZulu. South Afr. Med. J. 1992, 82, 118–123. [Google Scholar]
- Wagai, J.N.; Rhoda, D.; Prier, M.; Trimmer, M.K.; Clary, C.B.; Oteri, J.; Okposen, B.; Adeniran, A.; Danovaro-Holliday, C.; Cutts, F. Implementing WHO guidance on conducting and analysing vaccination coverage cluster surveys: Two examples from Nigeria. PLoS ONE 2021, 16, e0247415. [Google Scholar] [CrossRef]
- World Health Organization. Immunization and Vaccine-related Implementation Research Advisory Committee (IVIR-AC): Summary of conclusions and recommendations, 9–11 June 2015 meeting. Wkly. Epidemiol. Rec. 2015, 90, 477–488. [Google Scholar]
- Biostat Global Consulting. Vaccination Coverage Quality Indicators (VCQI) Resources 2017. Available online: http://www.biostatglobal.com/VCQI_resources.html (accessed on 12 July 2021).
- Rhoda, D.A. VCQI Indicator List with Specifications, Draft Version 2.2; Biostat Global Consulting: Worthington, OH, USA, 2021. [Google Scholar]
- ICF. DHS Program 2020. Available online: https://dhsprogram.com (accessed on 26 May 2021).
- National Population Commission—NPC/Nigeria. Nigeria Demographic and Health Survey 1999; NPC/Nigeria and ORC Macro: Calverton, MD, USA, 2000. [Google Scholar]
- National Population Commission—NPC/Nigeria, ORC Macro. Nigeria Demographic and Health Survey 2003; NPC and ORC Macro: Calverton, MD, USA, 2004. [Google Scholar]
- Federal Office of Statistics/Nigeria, Institute for Resource Development—IRD/Macro International. Nigeria Demographic and Health Survey 1990; Federal Office of Statistics/Nigeria and IRD/Macro International: Columbia, MD, USA, 1992. [Google Scholar]
- National Population Commission—NPC/Nigeria, ICF Macro. Nigeria Demographic and Health Survey 2008; NPC/Nigeria and ICF Macro: Abuja, Nigeria, 2009. [Google Scholar]
- National Population Commission—NPC/Nigeria, ICF International. Nigeria Demographic and Health Survey 2013; NPC/Nigeria and ICF International: Abuja, Nigeria, 2014. [Google Scholar]
- National Population Commission—NPC, ICF. Nigeria Demographic and Health Survey 2018—Final Report; NPC and ICF: Abuja, Nigeria, 2019. [Google Scholar]
- Boyle, E.H.; King, M.; Sobek, M. IPUMS Demographic and Health Surveys Version 8 [Dataset] Minneapolis; IPUMS and ICF2020: Minnesota Population Center, University of Minnesota: Minneapolis, MN, USA, 2020. [Google Scholar] [CrossRef]
- Profamilia, Macro International. Colombia Encuesta Nacional de Demografía y Salud 1995; Profamilia/Colombia: Bogotá, Colombia, 1995. [Google Scholar]
- Profamilia. Colombia Salud Sexual y Reproductiva. In Resultados Encuesta Nacional de Demografía y Salud 2000; Profamilia/Colombia: Bogotá, Colombia, 2000. [Google Scholar]
- Ojeda, G.; Ordóñez, M.; Ochoa, L.H. Colombia Salud Sexual y Reproductiva. In Resultados Encuesta Nacional de Demografía y Salud 2005; Profamilia/Colombia: Bogotá, Colombia, 2005. [Google Scholar]
- Ojeda, G.; Ordóñez, M.; Ochoa, L.H. Colombia Encuesta Nacional de Demografía y Salud 2010; Profamilia/Colombia: Bogotá, Colombia, 2011. [Google Scholar]
- Rhoda, D.A.; Prier, M.L.; Trimner, M.K. VCQI Forms and Variable List (FVL) Document; Draft Version 1.7; Biostat Global Consulting: Worthington, OH, USA, 2021. [Google Scholar]
- Rhoda, D.A.; Trimner, M.K.; Prier, M.L.; Clary, C.B. VCQI User’s Guide; Draft Version 2.9; Biostat Global Consulting: Worthington, OH, USA, 2021. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC.: College Station, TX, USA, 2019. [Google Scholar]
- Clary, C.B.; Rhoda, D.A. Missed Opportunities for Vaccination—VCQI—R Shiny Tool 2020. Available online: https://biostat-global-consulting.shinyapps.io/MOV_Tool_Public/ (accessed on 25 September 2020).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Chang, W.; Cheng, J.; Allaire, J.; Sievert, C.; Schloerke, B.; Xie, Y.; Allen, J.; McPherson, J.; Dipert, A.; Borges, B.; et al. Shiny: Web Application Framework for R. 2021. Available online: https://cran.r-project.org/web/packages/shiny/index.html (accessed on 16 July 2021).
- World Health Organization. Vaccination Coverage Cluster Surveys: Reference Manual; (No. WHO/IVB/18.09); World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/handle/10665/272820.License:CCBY-NC-SA3.0IGO (accessed on 16 July 2021).
- World Health Organization. Summary of WHO Position Papers—Recommendations for Routine Immunization 2020. Available online: http://www.who.int/immunization/policy/Immunization_routine_table1.pdf (accessed on 31 May 2021).
- World Health Organization. Summary of WHO Position Papers—Recommended Routine Immunizations for Children 2020. Available online: http://www.who.int/immunization/policy/Immunization_routine_table2.pdf (accessed on 31 May 2021).
- Desvé, G.; Havreng, J.-F.; Brenner, E. Coverage Survey Analysis System (COSAS) 4.3—Software for EPI 30 Cluster Coverage Surveys; EPICENTRE: Geneva, Switzerland, 1991. [Google Scholar]
- Pan American Health Organization. Tools for monitoring the coverage of integrated public health interventions. In Vaccination and Deworming of Soil-Transmitted Helminthiasis. Vol. Module 6. Analysis of Data from Surveys and Nominal Registries; Pan American Health Organization: Washington, DC, USA, 2017. [Google Scholar]
- Garib, Z.; Vargas, A.L.; Trumbo, S.P.; Anthony, K.; Diaz-Ortega, J.-L.; Bravo-Alcántara, P.; Leal, I.; Danovaro-Holliday, M.C.; Velandia-González, M. Missed Opportunities for Vaccination in the Dominican Republic: Results of an Operational Investigation. BioMed Res. Int. 2016, 2016, 4721836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutts, F.T.; Rodrigues, L.C.; Colombo, S.; Bennett, S. Evaluation of Factors Influencing Vaccine Uptake in Mozambique. Int. J. Epidemiol. 1989, 18, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Baptiste, A.E.J.; Masresha, B.; Wagai, J.; Luce, R.; Oteri, J.; Dieng, B.; Bawa, S.; Ikeonu, O.C.; Chukwuji, M.; Braka, F.; et al. Trends in measles incidence and measles vaccination coverage in Nigeria, 2008–2018. Vaccine 2021. [Google Scholar] [CrossRef]
- Chard, A.N.; Gacic-Dobo, M.; Diallo, M.S.; Sodha, S.V.; Wallace, A.S. Routine Vaccination Coverage—Worldwide, 2019. MMWR. Morb. Mortal. Wkly. Rep. 2000, 69, 1706–1710. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.K.; Goodson, J.L.; Alexander, J.P.; Kretsinger, K.; Sodha, S.V.; Steulet, C.; Gacic-Dobo, M.; Rota, P.A.; McFarland, J.; Menning, L.; et al. Progress Toward Regional Measles Elimination—Worldwide, 2000–2019. Morb. Mortal. Wkly. Rep. 2020, 69, 1700–1705. [Google Scholar] [CrossRef]
- Adamu, A.A.; Uthman, O.A.; Gadanya, M.A.; Adetokunboh, O.O.; Wiysonge, C.S. A multilevel analysis of the determinants of missed opportunities for vaccination among children attending primary healthcare facilities in Kano, Nigeria: Findings from the pre-implementation phase of a collaborative quality improvement programme. PLoS ONE 2019, 14, e0218572. [Google Scholar] [CrossRef] [Green Version]
- Giuffrida, A.; Flórez, C.E.; Giedion, Ú.; Cueto, E.; López, J.G.; Glassman, A.; Castaño, R.A.; Pinto, D.M.; Pardo, R.; Tono, T.M.; et al. From Few to Many: Ten Years of Health Insurance Expansion in Colombia; Inter-American Development Bank: Washington, DC, USA, 2009. [Google Scholar]
- World Bank. Colombia Decentralization Options and Incentives for Efficiency—Main Report; World Bank: Washington, DC, USA, 2009. [Google Scholar]
- EPI in the Americas. Expanded Program on Immunization in the Americas. Missed opportunities for vaccination in the Americas: Diagnosis and interventions, 1988–1990. EPI Newsl. 1991, 13, 3–6. [Google Scholar]
- World Health Organization. Immunization Coverage Cluster Survey: Reference Manual; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- UNICEF. New Partnership with IPUMS 2018. Available online: https://mics.unicef.org/news_entries/104/NEW-PARTNERSHIP-WITH-IPUMS (accessed on 2 June 2021).
- Hanson, C.M.; Mirza, I.; Kumapley, R.; Ogbuanu, I.; Kezaala, R.; Nandy, R. Enhancing immunization during second year of life by reducing missed opportunities for vaccinations in 46 countries. Vaccine 2018, 36, 3260–3268. [Google Scholar] [CrossRef]
- Clark, A.; Sanderson, C. Timing of children’s vaccinations in 45 low-income and middle-income countries: An analysis of survey data. Lancet 2009, 373, 1543–1549. [Google Scholar] [CrossRef]
- Ndwandwe, D.; Nnaji, C.A.; Wiysonge, C.S. The Magnitude and Determinants of Missed Opportunities for Childhood Vaccination in South Africa. Vaccines 2020, 8, 705. [Google Scholar] [CrossRef]
- Acharya, K.; Lacoul, M.; Bietsch, K. Factors Affecting Vaccination Coverage and Retention of Vaccination Cards in Nepal; ICF: Rockville, MD, USA, 2019. [Google Scholar]
- National Department of Health, ICF. South Africa Demographic and Health Survey 2016, Table 10.3; National Department of Health—NDoH—ICF: Pretoria, South Africa, 2019. [Google Scholar]
- Kaboré, L.; Meda, B.; Médah, I.; Shendale, S.; Lochlainn, L.N.; Sanderson, C.; Ouattara, M.; Kaboré, W.M.; Betsem, E.; Ogbuanu, I.U. Assessment of missed opportunities for vaccination (MOV) in Burkina Faso using the World Health Organization’s revised MOV strategy: Findings and strategic considerations to improve routine childhood immunization coverage. Vaccine 2020, 38, 7603–7611. [Google Scholar] [CrossRef]
- Li, A.J.; Tabu, C.; Shendale, S.; Okoth, P.O.; Sergon, K.; Maree, E.; Mugoya, I.K.; Machekanyanga, Z.; Onuekwusi, I.U.; Ogbuanu, I.U. Qualitative insights into reasons for missed opportunities for vaccination in Kenyan health facilities. PLoS ONE 2020, 15, e0230783. [Google Scholar] [CrossRef] [Green Version]
- Li, A.J.; Tabu, C.; Shendale, S.; Sergon, K.; Okoth, P.O.; Mugoya, I.K.; Machekanyanga, Z.; Onuekwusi, I.U.; Sanderson, C.; Ogbuanu, I.U. Assessment of missed opportunities for vaccination in Kenyan health facilities, 2016. PLoS ONE 2020, 15, e0237913. [Google Scholar] [CrossRef] [PubMed]
- Li, A.J.; Peiris, T.S.R.; Sanderson, C.; Nic Lochlainn, L.; Mausiry, M.; da Silva, R.B.J.B.M.; Ogbuanu, I.U. Opportunities to improve vaccination coverage in a country with a fledgling health system: Findings from an assessment of missed opportunities for vaccination among health center attendees—Timor Leste, 2016. Vaccine 2019, 37, 4281–4290. [Google Scholar] [CrossRef]
- Ogbuanu, I.U.; Li, A.J.; Anya, B.-P.M.; Tamadji, M.; Chirwa, G.; Chiwaya, K.W.; Djalal, M.E.-H.; Cheikh, D.; Machekanyanga, Z.; Okeibunor, J.; et al. Can vaccination coverage be improved by reducing missed opportunities for vaccination? Findings from assessments in Chad and Malawi using the new WHO methodology. PLoS ONE 2019, 14, e0210648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamu, A.A. Using Quality Improvement Approach to Addressed Missed Opportunities for Vaccination in Kano Metropolis, Nigeria; Stellenbosch University: Stellenbosch, South Africa, 2019. [Google Scholar]
- World Health Organization. Planning Guide to Reduce Missed Opportunities for Vaccination; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Intervention Guidebook for Implementing and Monitoring Activities to Reduce Missed Opportunities for Vaccination; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Mansour, Z.; Brandt, L.; Said, R.; Fahmy, K.; Riedner, G.; Danovaro-Holliday, M.C. Home-based records’ quality and validity of caregivers’ recall of children’s vaccination in Lebanon. Vaccine 2019, 37, 4177–4183. [Google Scholar] [CrossRef]
- Kaboré, L.; Méda, C.Z.; Sawadogo, F.; Bengue, M.M.; Kaboré, W.M.; Essoh, A.T.; Gervaix, A.; Galetto-Lacour, A.; Médah, I.; Betsem, E. Quality and reliability of vaccination documentation in the routine childhood immunization program in Burkina Faso: Results from a cross-sectional survey. Vaccine 2020, 38, 2808–2815. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Year | Vaccines Included in DHS Report | Age 12–23 m in DHS Dataset N | Card Seen N (%) | Included in MOSV Analysis * N (%) |
|---|---|---|---|---|---|
| Colombia | 1995 | BCG from birth DPT doses 1–3 OPV doses 1–3 MCV/Measles dose 1 | 1031 | 630 (61.1%) | 615 (59.7%) |
| 2000 | BCG from birth DPT doses 1–3 OPV doses 1–3 MCV/MMR dose 1 | 914 | 686 (75.1%) | 683 (74.7%) | |
| 2005 | 2919 | 2208 (75.6%) | 2201 (75.4%) | ||
| 2010 | BCG from birth Penta/DPT doses 1–3 OPV doses 1–3 MMR dose 1 | 3435 | 2895 (84.3%) | 2891 (84.2%) | |
| Nigeria | 1999 | BCG from birth DPT doses 1–3 OPV birth dose OPV doses 1–3 MCV/Measles dose 1 | 1042 | 217 (20.8%) | 210 (20.2%) |
| 2003 | 987 | 232 (23.5%) | 225 (22.8%) | ||
| 2008 | 5022 | 1269 (25.3%) | 1243 (24.8%) | ||
| 2013 | 5834 | 1764 (30.2%) | 1707 (29.3%) | ||
| 2018 | BCG from birth HepB birth dose Penta doses 1–3 OPV birth dose OPV doses 1–3 IPV dose 1 PCV doses 1–3 MCV/Measles dose 1 | 6057 | 2426 (40.1%) | 2271 (37.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rhoda, D.A.; Prier, M.L.; Clary, C.B.; Trimner, M.K.; Velandia-Gonzalez, M.; Danovaro-Holliday, M.C.; Cutts, F.T. Using Household Surveys to Assess Missed Opportunities for Simultaneous Vaccination: Longitudinal Examples from Colombia and Nigeria. Vaccines 2021, 9, 795. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070795
Rhoda DA, Prier ML, Clary CB, Trimner MK, Velandia-Gonzalez M, Danovaro-Holliday MC, Cutts FT. Using Household Surveys to Assess Missed Opportunities for Simultaneous Vaccination: Longitudinal Examples from Colombia and Nigeria. Vaccines. 2021; 9(7):795. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070795
Chicago/Turabian StyleRhoda, Dale A., Mary L. Prier, Caitlin B. Clary, Mary Kay Trimner, Martha Velandia-Gonzalez, M. Carolina Danovaro-Holliday, and Felicity T. Cutts. 2021. "Using Household Surveys to Assess Missed Opportunities for Simultaneous Vaccination: Longitudinal Examples from Colombia and Nigeria" Vaccines 9, no. 7: 795. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070795