
Usefulness of IVD Kits for the Assessment of SARS-CoV-2 Antibodies to Evaluate the Humoral Response to Vaccination

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Policy
2.2. Participants
2.3. Assays Characteristics
2.4. Statistical Analysis
3. Results
3.1. Assay Precision and Accuracy
3.2. Detection of SARS-CoV-2 Antibody within the Whole Study Group
3.3. Detection of SARS-CoV-2 Antibody within the SCV2-Positive Group
3.4. Detection of SARS-CoV-2 Antibody within SCV2-Negative Group Prior to Second Vaccine Dose
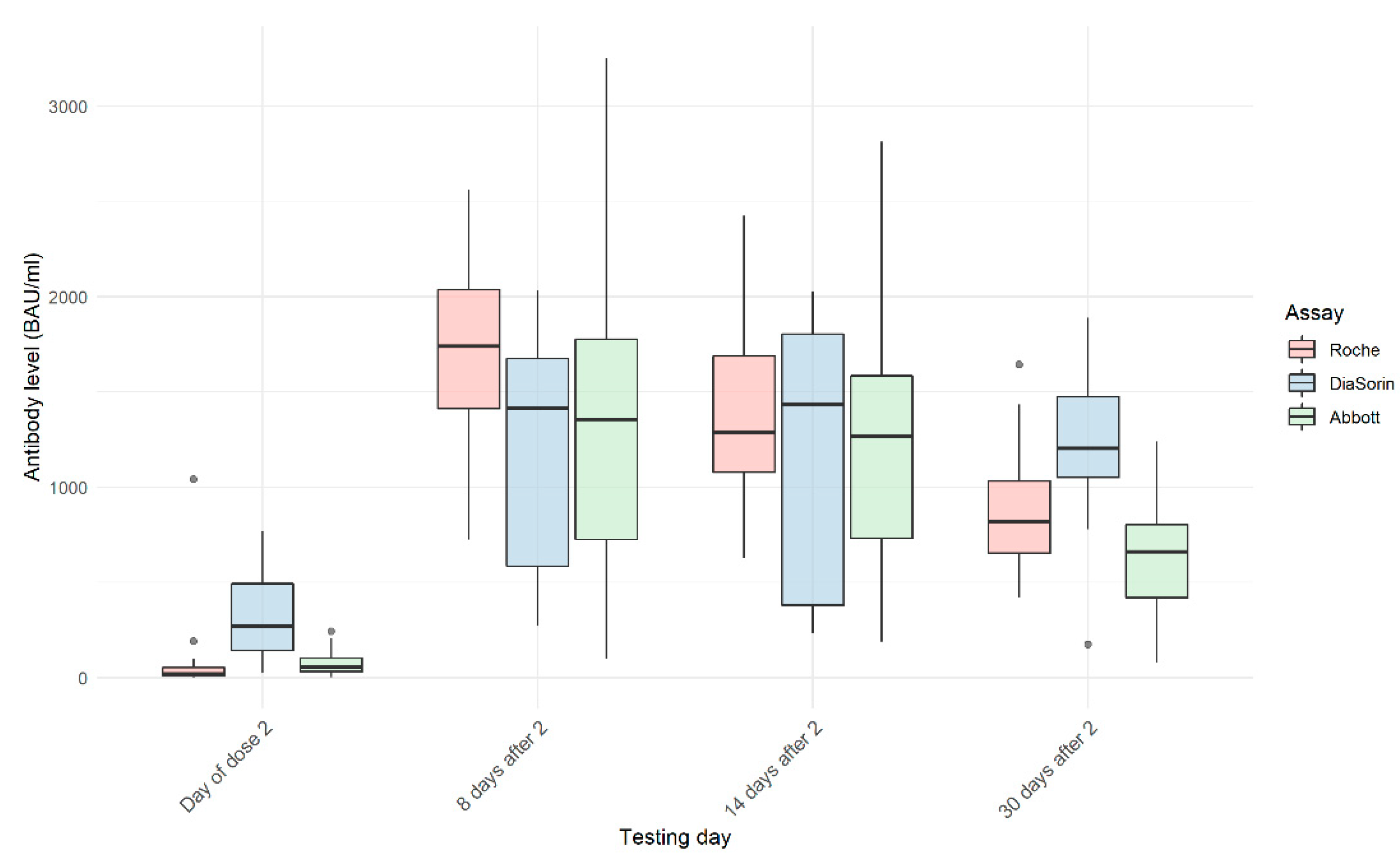
3.5. Detection of SARS-CoV-2 Antibody within SCV2-Negative Group on Day 8, 14, and 30 after the Second Dose
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weissleder, R.; Lee, H.; Ko, J.; Pittet, M.J. COVID-19 diagnostics in context. Sci. Transl. Med. 2020, 12, 1931. [Google Scholar] [CrossRef]
- Theel, E.S.; Slev, P.; Wheeler, S.; Couturier, M.R.; Wong, S.J.; Kadkhoda, K. The role of antibody testing for sars-cov-2: Is there one? J. Clin. Microbiol. 2020, 58, e00797-20. [Google Scholar] [CrossRef]
- Føns, S.; Krogfelt, K.A. How can we interpret SARS-CoV-2 antibody test results? Pathog. Dis. 2021, 79, 69. [Google Scholar] [CrossRef]
- Paiva, K.J.; Grisson, R.D.; Chan, P.A.; Huard, R.C.; Caliendo, A.M.; Lonks, J.R.; King, E.; Tang, E.W.; Pytel-Parenteau, D.L.; Nam, G.H.; et al. Validation and performance comparison of three SARS-CoV-2 antibody assays. J. Med. Virol. 2021, 93, 916–923. [Google Scholar] [CrossRef]
- Grzelak, L.; Temmam, S.; Planchais, C.; Demeret, C.; Tondeur, L.; Huon, C.; Guivel-Benhassine, F.; Staropoli, I.; Chazal, M.; Dufloo, P.; et al. A comparison of four serological assays for detecting anti–SARS-CoV-2 antibodies in human serum samples from different populations. Sci. Transl. Med. 2020, 12, 3103. [Google Scholar] [CrossRef]
- Krüttgen, A.; Cornelissen, C.G.; Dreher, M.; Hornef, M.; Imöhl, M.; Kleines, M. Comparison of four new commercial serologic assays for determination of SARS-CoV-2 IgG. J. Clin. Virol. 2020, 128, 104394. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, A.C.; Holm, D.K.; Justesen, U.S.; Gorm-Jensen, T.; Andersen, N.S.; Øvrehus, A.; Michelsen, J.; Sprogøea, U.; Lillevang, T. Comparison of six commercially available SARS-CoV-2 antibody assays—Choice of assay depends on intended use. Int. J. Infect. Dis. 2021, 103, 381–388. [Google Scholar] [CrossRef]
- Egger, M.; Bundschuh, C.; Wiesinger, K.; Gabriel, C.; Clodi, M.; Mueller, T.; Dieplinger, B. Comparison of the Elecsys® Anti-SARS-CoV-2 immunoassay with the EDITM enzyme linked immunosorbent assays for the detection of SARS-CoV-2 antibodies in human plasma. Clin. Chim. Acta 2020, 509, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Verkerke, H.; Horwath, M.; Saeedi, B.; Boyer, D.; Allen, J.W.; Owens, J.; Arthur, C.M.; Nakahara, H.; Rha, J.; Patel, K.; et al. Comparison of Antibody Class-Specific SARS-CoV-2 Serologies for the Diagnosis of Acute COVID-19. J. Clin. Microbiol. 2021, 59. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, M.; Andersson, M.; Auckland, K.; Baillie, J.K.; Barnes, E.; Beer, S.; Beveridge, A.; Bibi, S.; Blackwell, L.; Borak, M.; et al. Performance characteristics of five immunoassays for SARS-CoV-2: A head-to-head benchmark comparison. Lancet Infect. Dis. 2020, 20, 1390–1400. [Google Scholar] [CrossRef]
- James, J.; Rhodes, S.; Ross, C.S.; Skinner, P.; Smith, S.P.; Shipley, R.; Warren, C.J.; Goharriz, H.; McElhinney, L.M.; Temperton, N.; et al. Comparison of Serological Assays for the Detection of SARS-CoV-2 Antibodies. Viruses 2021, 13, 713. [Google Scholar] [CrossRef] [PubMed]
- Krüttgen, A.; Cornelissen, C.G.; Dreher, M.; Hornef, M.W.; Imöhl, M.; Kleines, M. Determination of SARS-CoV-2 antibodies with assays from Diasorin, Roche and IDvet. J. Virol. Methods 2021, 287, 113978. [Google Scholar] [CrossRef]
- Weidner, L.; Gänsdorfer, S.; Unterweger, S.; Weseslindtner, L.; Drexler, C.; Farcet, M.; Witt, V.; Schistal, E.; Schlenke, P.; Kreil, T.R.; et al. Quantification of SARS-CoV-2 antibodies with eight commercially available immunoassays. J. Clin. Virol. 2020, 129, 104540. [Google Scholar] [CrossRef]
- Wakita, M.; Idei, M.; Saito, K.; Horiuchi, Y.; Yamatani, K.; Ishikawa, S.; Yamamoto, T.; Igawa, G.; Hinata, M.; Kadota, K.; et al. Comparison of the clinical performance and usefulness of five SARS-CoV-2 antibody tests. PLoS ONE 2021, 16, e0246536. [Google Scholar] [CrossRef] [PubMed]
- Jahrsdörfer, B.; Kroschel, J.; Ludwig, C.; Corman, V.M.; Schwarz, T.; Körper, S.; Rojewski, M.; Lotfi, R.; Weinstock, C.; Drosten, C.; et al. Independent Side-by-Side Validation and Comparison of 4 Serological Platforms for SARS-CoV-2 Antibody Testing. J. Infect. Dis. 2021, 223, 796–801. [Google Scholar] [CrossRef]
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; Ferrante di Ruffano, L.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef]
- Kontou, P.I.; Braliou, G.G.; Dimou, N.L.; Nikolopoulos, G.; Bagos, P.G. Antibody tests in detecting SARS-CoV-2 infection: A meta-analysis. Diagnostics 2020, 10, 319. [Google Scholar] [CrossRef]
- Mueller, T. Antibodies against severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) in individuals with and without COVID-19 vaccination: A method comparison of two different commercially available serological assays from the same manufacturer. Clin. Chim. Acta 2021, 518, 9–16. [Google Scholar] [CrossRef]
- Trabaud, M.-A.; Icard, V.; Milon, M.-P.; Bal, A.; Lina, B.; Escuret, V. Comparison of eight commercial, high-throughput, automated or ELISA assays detecting SARS-CoV-2 IgG or total antibody. J. Clin. Virol. 2020, 132, 104613. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Hunt, K.; Pesukova, J.; Haljasmagi, L.; Rumm, P.; Peterson, P.; Hololejenko, J.; Eero, I.; Jõgi, P.; Toompere, K.; et al. Evaluation of SARS-CoV-2 IgG antibody response in PCR positive patients: Comparison of nine tests in relation to clinical data. PLoS ONE 2020, 15, e0237548. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Breyer, M.K.; Breyer-Kohansal, R.; Burghuber, O.C.; Hartl, S.; Aletaha, D.; Sieghart, D.; Quehenberger, P.; Marculescu, R.; et al. Side-by-Side Comparison of Three Fully Automated SARS-CoV-2 Antibody Assays with a Focus on Specificity. Clin. Chem. 2020, 66, 1405–1413. [Google Scholar] [CrossRef]
- Mattiuzzo, G.; Bentley, E.M.; Hassall, M.; Routley, S. Establishment of the WHO International Standard and Reference Panel for anti-SARS-CoV-2 antibody. 2020, pp. 9–10. Available online: https://www.who.int/publications/m/item/WHO-BS-2020.2403 (accessed on 20 May 2021).
- NIBSC. WHO International Standard First WHO International Standard for Anti-SARS-CoV-2 Immunoglobulin (Human); NIBSC: Potters Bar, UK, 2020. [Google Scholar]
- R Core Team. R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 24 May 2021).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Manuilova, E.; Schuetzenmeister, A.; Model, F. CRAN—Package mcr. Available online: https://cran.r-project.org/web/packages/mcr/index.html (accessed on 24 May 2021).
- Wang, Z.; Schmidt, F.; Weisblum, Y.; Muecksch, F.; Barnes, C.O.; Finkin, S.; Schaefer-Babajew, D.; Cipolla, M.; Gaebler, C.; Lieberman, J.A.; et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. Nat. Cell Biol. 2021, 592, 616–622. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-Spike Protein Assays to Determine Post-Vaccination Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. MedRxiv 2021. [Google Scholar] [CrossRef]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA J. Am. Med Assoc. 2020, 323, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, P.A.; Page, M.; Bernasconi, V.; Mattiuzzo, G.; Dull, P.; Makar, K.; Plotkin, S.; Knezevic, I. WHO International Standard for anti-SARS-CoV-2 immunoglobulin. Lancet 2021, 397, 1347–1348. [Google Scholar] [CrossRef]
- Poland, G.A.; Ovsyannikova, I.G.; Kennedy, R.B. SARS-CoV-2 Immunity: Review and Applications to Phase 3 Vaccine Can-didates. Lancet 2020, 396, 1595–1606. [Google Scholar] [CrossRef]
- Padoan, A.; Sciacovelli, L.; Basso, D.; Negrini, D.; Zuin, S.; Cosma, C.; Faggian, D.; Matricardi, P.; Plebani, M. IgA-Ab response to spike glycoprotein of SARS-CoV-2 in patients with COVID-19: A longitudinal study. Clinica Chimica Acta 2020, 507, 164–166. [Google Scholar] [CrossRef]
- Lou, B.; Li, T.-D.; Zheng, S.-F.; Su, Y.-Y.; Li, Z.-Y.; Liu, W.; Yu, F.; Ge, S.-X.; Zou, Q.-D.; Yuan, Q.; et al. Serology characteristics of SARS-CoV-2 infection after exposure and post-symptom onset. Eur. Respir. J. 2020, 56, 2000763. [Google Scholar] [CrossRef]
- Adams, E.R.; Ainsworth, M.; Anand, R.; Andersson, M.I.; Auckland, K.; Baillie, J.K.; Barnes, E.; Beer, S.; Bell, J.I.; Berry, T.; et al. Antibody testing for COVID-19: A report from the National COVID Scientific Advisory Panel. Wellcome Open Res. 2020, 5, 139. [Google Scholar] [CrossRef]
- Bajaj, V.; Gadi, N.; Spihlman, A.P.; Wu, S.C.; Choi, C.H.; Moulton, V.R. Aging, Immunity, and COVID-19: How Age Influences the Host Immune Response to Coronavirus Infections? Front. Physiol. 2021, 11, 571416. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Elecsys Anti-SARS-CoV-2 S | LIAISON® SARS-CoV-2 TrimericS IgG | SARS-CoV-2 IgG II Quant |
|---|---|---|---|
| Specified by manufacturer: | |||
| Assay type | Automated | ||
| Dilution method | Automated, 10× | Manual, 10× | Automated, 2× |
| Testing time | 18 min | 35 min | 29 min |
| Test principle | Double-antigen sandwich principle. Electrochemiluminescence detection (ECLIA) | Indirect immunoassay. Chemiluminescence detection (CLIA) | Chemiluminescence microparticle immunoassay (CMIA) |
| Calibration | 2 points | 6 points | |
| Calibrators frequency | Started with new reagent lot/quality control findings outside the defined limits | ||
| Traceability | Standardized against the internal Roche standard for anti-SARS-CoV-2 S/from date 12.01.2021. Standardized against the WHO IS: NIBSC 20-136 | Correlation with Microneutralization Test (MNT)/from date 02.02.2021. Standardized against the WHO IS: NIBSC 20-136 | Standardized against the internal Abbott standard for anti-SARS-CoV-2 S/correlation with Microneutralization Test (MNT)/from date 02.2021. Standardized against the WHO IS: NIBSC 20-136 |
| Sample material | Serum | ||
| Sample volume | 12 uL | 10 uL | 25 uL |
| Limit of detection (LoD) | 0.35 U/mL | 0.712 AU/mL | 6.8 AU/mL |
| Limit of quantification (LoQ) | 0.40 U/mL | 1.63 AU/mL | 21.0 AU/mL |
| Measuring range | 0.40–250 U/mL | 1.85–800 AU/mL | 21.0–40,000.0 AU/mL |
| BAU conversion | U/mL × 1.029 | AU/mL × 2.6 | AU/mL × 0.142 |
| Laboratory specific: | |||
| Controls frequency | Daily | ||
| Control Sample | Roche (U/mL) | DiaSorin (AU/mL) | Abbott (AU/mL) | ||||
|---|---|---|---|---|---|---|---|
| PreciControl Anti-SARS-CoV-2 S p1 | PreciControl Anti-SARS-CoV-2 S p2 | SARS-CoV-2 TG Control Set p1 | SARS-CoV-2 TG Control Set p2 | SARS-CoV-2 IgG II Quant Control | SARS-CoV-2 IgG II Quant Control +1 | SARS-CoV-2 IgG II Quant Control +2 | |
| LOT | 526346 | 526347 | 311031 | 212031 | 23268FN00 | ||
| Nominal value | n/a | 8.41 | n/a | 37.5 | 2.3 | 166 | 602.5 |
| Range | 0.000–0.399 | 5.887–10.933 | 0.0–6.0 | 26.38–48.8 | 0.0–18.0 | 91.3–240.7 | 331.4–873.6 |
| Average | <0.400 | 7.86 | <1.85 | 38.29 | 3.075 | 172.5 | 650.84 |
| SD | n/a | 0.193 | n/a | 1.323 | n/a | 5.81 | 14.47 |
| I (%) | n/a | 2.5 | n/a | 3.46 | n/a | 4.4 | 3.3 |
| B (%) | n/a | −6.6 | n/a | 2.1 | n/a | 3.9 | 8.0 |
| All Samples | SCV2-Positive | SCV2-Negative | ||||
|---|---|---|---|---|---|---|
| Before Dose 1 | Before Dose 2 | 8 d after Dose 2 | 14 d after Dose 2 | 30 d after Dose 2 | ||
| ■ Pair of tests | ρ | ρ | ρ | ρ | ρ | ρ |
| ■ Roche ■ /DiaSorin | 0.684 * | 0.514 * | 0.775 * | 0.062 | 0.154 | 0.506 * |
| ■ Roche ■ /Abbott | 0.902 * | 0.554 * | 0.817 * | 0.693 * | 0.603 * | 0.314 |
| ■ DiaSorin ■ /Abbott | 0.663 * | 0.821 * | 0.825 * | −0.131 | −0.247 | 0.624 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lukaszuk, K.; Kiewisz, J.; Rozanska, K.; Dabrowska, M.; Podolak, A.; Jakiel, G.; Woclawek-Potocka, I.; Lukaszuk, A.; Rabalski, L. Usefulness of IVD Kits for the Assessment of SARS-CoV-2 Antibodies to Evaluate the Humoral Response to Vaccination. Vaccines 2021, 9, 840. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9080840
Lukaszuk K, Kiewisz J, Rozanska K, Dabrowska M, Podolak A, Jakiel G, Woclawek-Potocka I, Lukaszuk A, Rabalski L. Usefulness of IVD Kits for the Assessment of SARS-CoV-2 Antibodies to Evaluate the Humoral Response to Vaccination. Vaccines. 2021; 9(8):840. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9080840
Chicago/Turabian StyleLukaszuk, Krzysztof, Jolanta Kiewisz, Karolina Rozanska, Malgorzata Dabrowska, Amira Podolak, Grzegorz Jakiel, Izabela Woclawek-Potocka, Aron Lukaszuk, and Lukasz Rabalski. 2021. "Usefulness of IVD Kits for the Assessment of SARS-CoV-2 Antibodies to Evaluate the Humoral Response to Vaccination" Vaccines 9, no. 8: 840. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9080840