
BNT162b2 COVID-19 Vaccine Hesitancy among Parents of 4023 Young Adolescents (12–15 Years) in Qatar

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
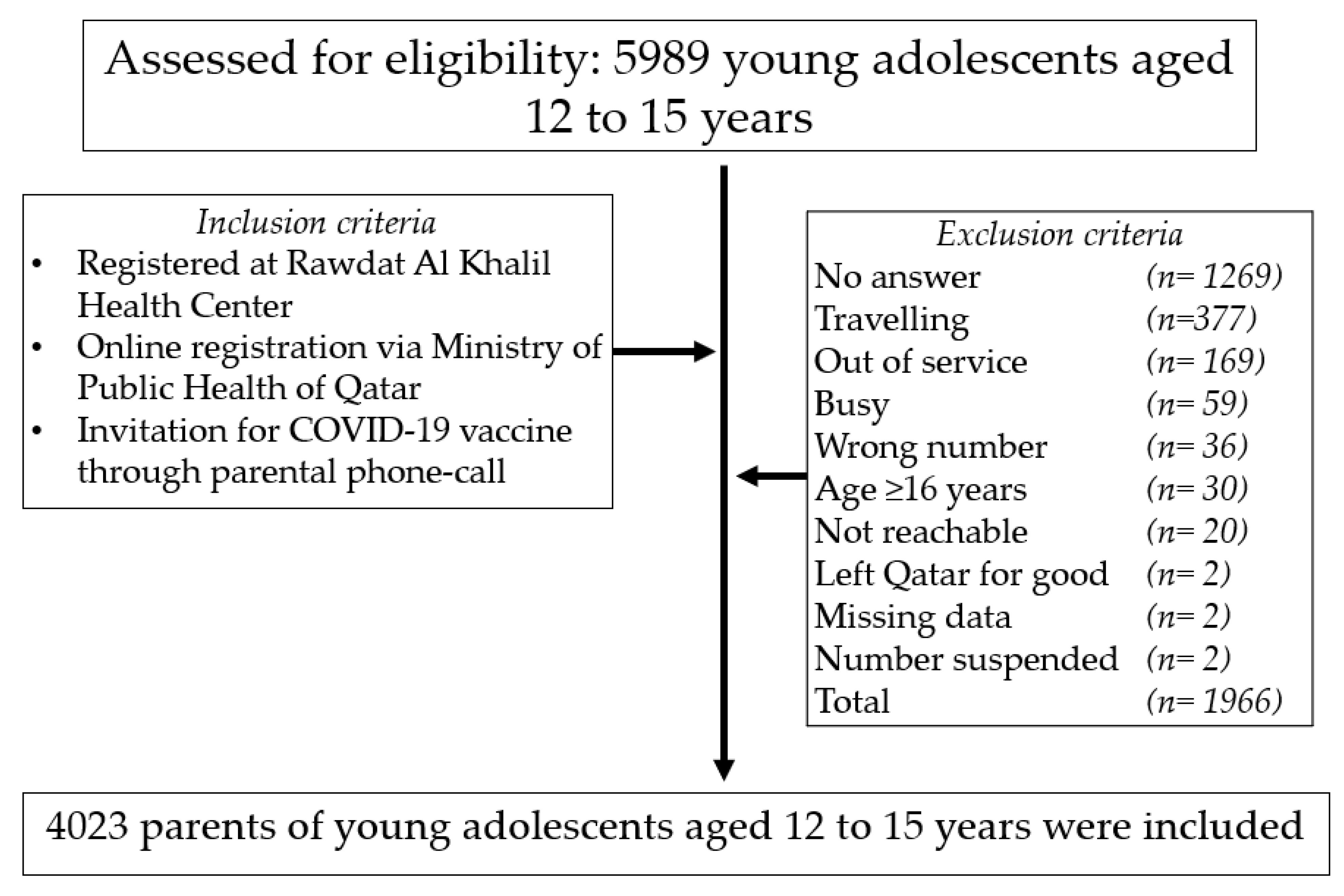
2.1. Study Design and Participants
2.2. Vaccination Campaign in Qatar
- Phase 1 (from 23 December 2020 to 31 March 2021) encompassed people who are aged 70 years and above, long-term care and home care patients, people with severe or multiple conditions including age group from 16 years and older, key personnel and first responders including health care providers, ambulance teams, Ministry of Interior, Ministry of Defence, oil and gas sector, Hamad International Airport and Qatar Airways, and 50% of teachers.
- Phase 2 (from 1 April to 30 June 2021) encompassed people aged 40 years and above, those with moderate health conditions, workers in industries including food, housekeeping, hairdressing and transportation, all remaining teachers, all health care personnel not included in the first stage, people in group accommodation facilities for persons with physical disabilities or psychological problems or in the recovery phase and persons in detention facilities. Throughout phase 2, young adolescents aged 12–15 years old were added on 12 May 2021, two days following the U.S.A. FDA approval and authorization of Pfizer-BioNTech COVID-19. Adolescents aged 16–17 who were not vaccinated in phases 1 and 2 were included as well.
- Phase 3 (from 1 June to 31 July 2021) included workers in industries essential to the functioning of society who are at increased risk of disease and eligible people who were not included in the first and second phases.
- Phase 4 (from 1 August to 31 October 2021) intends to include all the residents of Qatar aged 12 years and more, who did not receive the vaccine in the previous stages.
2.3. Sample Size
2.4. Vaccine Acceptance and Hesitancy
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Parents and Young Adolescents’ Characteristics
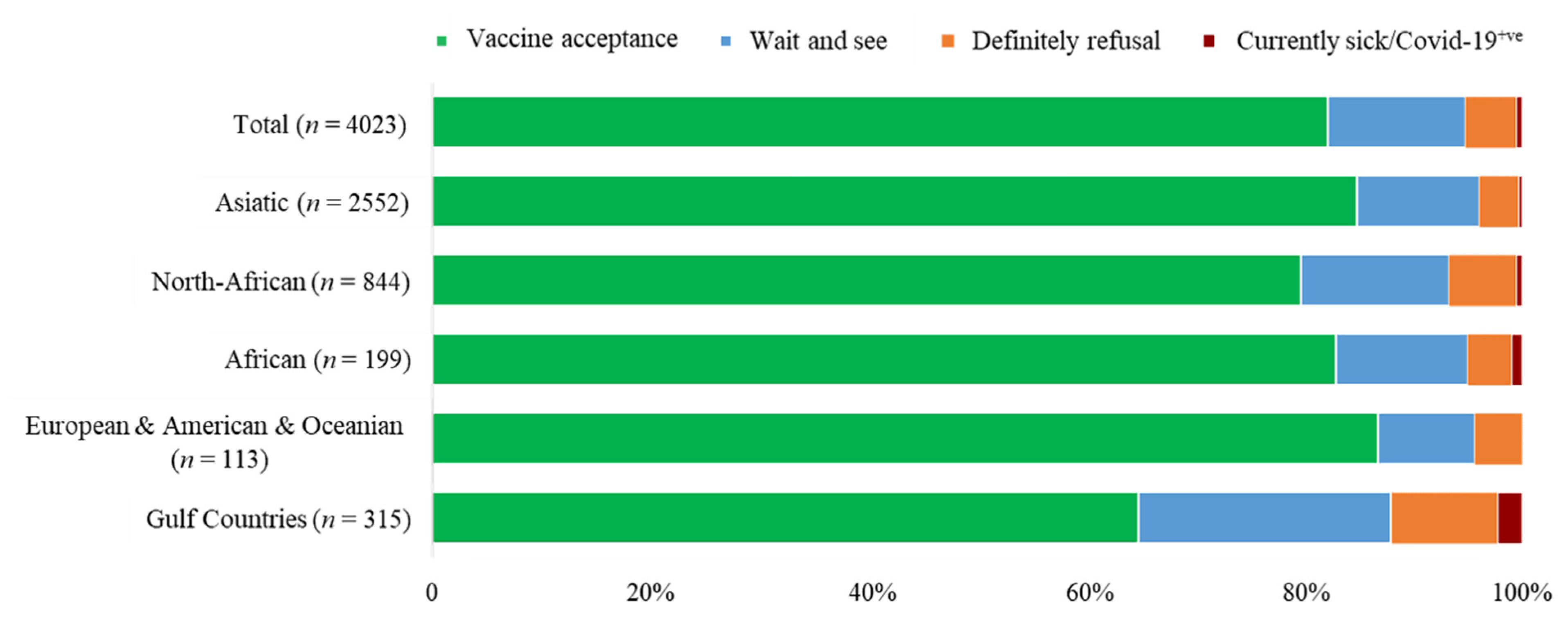
3.2. Influencing Factors of Vaccine Acceptance and Hesitancy Rates
- (i).
- The 12 years group compared to the 13- and 15-years groups,
- (ii).
- North-African nationalities compared to Asiatic nationalities,
- (iii).
- Gulf Countries nationalities compared to the four remaining groups of nationalities,
- (iv).
- Young adolescents with the chronic disease compared to those free from chronic disease, and in
- (v).
- Young adolescents having been previously COVID-19 infected as compared to their COVID-19 negative-history counterparts.
3.3. Reasons for Parental VH
3.4. Vaccine Acceptance among Previously Vaccine Hesitant Parents
4. Discussion
4.1. VH amongst Parents of Young Adolescents According to Age Groups and Sex
4.2. VH amongst Parents of Young Adolescents According to Nationalities
4.3. VH amongst Parents of Young Adolescents Living with a Chronic Disease
4.4. VH amongst Parents of Young Adolescents Previously Infected by COVID-19
5. Hesitancy Reasons of the BNT162b2 COVID-19 Vaccine amongst Parents of Young Adolescents
6. Vaccine Acceptance among Previously Hesitant Parents
7. Extension
8. Strengths and Limitations
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics and Consent
References
- Worldometer COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 18 August 2021).
- Dergaa, I.; Varma, A.; Tabben, M.; Malik, R.A.; Sheik, S.; Vedasalam, S.; Abbassi, A.K.; Almulla, J.; Chaabane, M.; Chamari, K. Organising football matches with spectators during the COVID-19 pandemic: What can we learn from the Amir Cup Football Final of Qatar 2020? A call for action. Biol. Sport 2021, 38, 677–681. [Google Scholar] [CrossRef]
- Varma, A.; Dergaa, I.; Mohammed, A.R.; Abubaker, M.; Al Naama, A.; Mohammed, S.; Rafique, M.A.; Manu, L.; Vedasalam, S.; Parveze, P.; et al. COVID-19 and diabetes in primary care—How do hematological parameters present in this cohort? Expert Rev. Endocrinol. Metab. 2021, 16, 147–153. [Google Scholar] [CrossRef]
- Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. On Behalf of the Eclb-Covid Consortium. Sleep Quality and Physical Activity as Predictors of Mental Wellbeing Variance in Older Adults during COVID-19 Lockdown: ECLB COVID-19 International Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 4329. [Google Scholar] [CrossRef]
- Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. Globally altered sleep patterns and physical activity levels by confinement in 5056 individuals: ECLB COVID-19 international online survey. Biol. Sport 2021, 38, 495–506. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Ferris, A.; Kernan, K.F.; Schulert, G.S.; et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 2. Arthritis Rheumatol. 2021, 73, e13–e29. [Google Scholar] [CrossRef] [PubMed]
- Havers, F.P.; Whitaker, M.; Self, J.L.; Chai, S.J.; Kirley, P.D.; Alden, N.B.; Kawasaki, B.; Meek, J.; Yousey-Hindes, K.; Anderson, E.J.; et al. COVID-NET Surveillance Team. Hospitalization of Adolescents Aged 12–17 Years with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, March 1, 2020-April 24, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 851–857. [Google Scholar] [CrossRef]
- Rubens, J.H.; Akindele, N.P.; Tschudy, M.M.; Sick-Samuels, A.C. Acute COVID-19 and multisystem inflammatory syndrome in children. BMJ 2021, 372, n385. [Google Scholar] [CrossRef]
- WHO. International Travel and Health. Chapter 6: Vaccine-Preventable Diseases and Vaccines. Available online: https://www.who.int/ith/ITH-Chapter6.pdf (accessed on 26 June 2021).
- Hacisuleyman, E.; Hale, C.; Saito, Y.; Blachere, N.E.; Bergh, M.; Conlon, E.G.; Schaefer-Babajew, D.J.; DaSilva, J.; Muecksch, F.; Gaebler, C.; et al. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N. Engl. J. Med. 2021, 384, 2212–2218. [Google Scholar] [CrossRef]
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. C4591001 Clinical Trial Group. Safety, Immunogenicity, and Efficacy of the BNT162b2 COVID-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef]
- Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight against Pandemic. 10 May 2021. Available online: www.fda.gov/news-events/press-announcements/coronavirus-COVID-19-update-fda-authorizes-pfizer-biontech-COVID-19-vaccine-emergency (accessed on 26 June 2021).
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Montalti, M.; Rallo, F.; Guaraldi, F.; Bartoli, L.; Po, G.; Stillo, M.; Perrone, P.; Squillace, L.; Dallolio, L.; Pandolfi, P.; et al. Would Parents Get Their Children Vaccinated Against SARS-CoV-2? Rate and Predictors of Vaccine Hesitancy According to a Survey over 5000 Families from Bologna, Italy. Vaccines 2021, 9, 366. [Google Scholar] [CrossRef]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health of Qatar: National COVID-19 Vaccination Program Data. Available online: https://covid19.moph.gov.qa/EN/Pages/Vaccination-Program-Data.aspx (accessed on 26 June 2021).
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- Simonson, M.; Baum, M.; Lazer, D.; Ognyanova, K.; Gitomer, A.; Perlis, R.H.; Lin, J. The COVID States Project# 45: Vaccine hesitancy and resistance among parents. OSF Prepr. 2021. [Google Scholar] [CrossRef]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental Acceptability of COVID-19 Vaccination for Children Under the Age of 18 Years: Cross-Sectional Online Survey. JMIR Pediatrics Parent. 2020, 3, e24827. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Hoq, M.; Measey, M.A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020, 21, e110. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Alabdulla, M.; Reagu, S.M.; Al-Khal, A.; Elzain, M.; Jones, R.M. COVID-19 vaccine hesitancy and attitudes in Qatar: A national cross-sectional survey of a migrant-majority population. Influenza Other Respir. Viruses 2021, 15, 361–370. [Google Scholar] [CrossRef]
- Magadmi, R.M.; Kamel, F.O. Beliefs and Barriers Associated with COVID-19 Vaccination among the General Population in Saudi Arabia. BMC Public Health 2020, 21, 1438. [Google Scholar] [CrossRef]
- El-Elimat, T.; AbuAlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and attitudes toward COVID-19 vaccines: A cross-sectional study from Jordan. PLoS ONE 2021, 16, e0250555. [Google Scholar] [CrossRef] [PubMed]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 Vaccine Acceptance in Saudi Arabia: A Web-Based National Survey. (JMDH) J. Multi. Discip. Healthc. 2020, 13, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Qunaibi, E.A.; Helmy, M.; Basheti, I.; Sultan, I. A high rate of COVID-19 vaccine hesitancy in a large-scale survey on Arabs. eLife 2021, 10, e68038. [Google Scholar] [CrossRef]
- Qunaibi, E.; Basheti, I.; Soudy, M.; Sultan, I. Hesitancy of Arab Healthcare Workers towards COVID-19 Vaccination: A Large-Scale Multinational Study. Vaccines 2021, 9, 446. [Google Scholar] [CrossRef]
- Ventola, C.L. Social media and health care professionals: Benefits, risks, and best practices. Pharm. Ther. 2014, 39, 491–520. [Google Scholar]
- Reno, C.; Maietti, E.; Fantini, M.P.; Savoia, E.; Manzoli, L.; Montalti, M.; Gori, D. Enhancing COVID-19 Vaccines Acceptance: Results from a Survey on Vaccine Hesitancy in Northern Italy. Vaccines 2021, 9, 378. [Google Scholar] [CrossRef]
- Tsabouri, S.; Makis, A.; Kosmeri, C.; Siomou, E. Risk Factors for Severity in Children with Coronavirus Disease 2019: A Comprehensive Literature Review. Pediatr. Clin. N. Am. 2021, 68, 321–338. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Centre for Diseases Control and Prevention (CDC) COVID-19: Medical Condition, Updated on 13 May 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 16 August 2021).
- Stafstrom, C.E.; Jantzie, L.L. COVID-19: Neurological Considerations in Neonates and Children. Children 2020, 7, 133. [Google Scholar] [CrossRef] [PubMed]
- Gerussi, V.; Peghin, M.; Palese, A.; Bressan, V.; Visintini, E.; Bontempo, G.; Graziano, E.; De Martino, M.; Isola, M.; Tascini, C. Vaccine Hesitancy among Italian Patients Recovered from COVID-19 Infection towards Influenza and Sars-Cov-2 Vaccination. Vaccines 2021, 9, 172. [Google Scholar] [CrossRef]
- Millner, V.S.; Eichold, B.H., 2nd; Franks, R.D.; Johnson, G.D. Influenza vaccination acceptance and refusal rates among health care personnel. South. Med. J. 2010, 103, 993–998. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- British Society of Immunology. Immunity and COVID-19. 3 February 2021. Available online: https://www.immunology.org/sites/default/files/BSI_Briefing_Note_2021_immunity_COVID19.pdf (accessed on 26 June 2021).
- Yılmaz, M.; Sahin, M.K. Parents’ willingness and attitudes concerning the COVID-19 vaccine: A cross-sectional study. Int. J. Clin. Pract. 2021, e14364. [Google Scholar] [CrossRef]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. (JECH) J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Marquez, R.R.; Gosnell, E.S.; Thikkurissy, S.; Schwartz, S.B.; Cully, J.L. Caregiver acceptance of an anticipated COVID-19 vaccination. J. Am. Dent. Assoc. 2021, 152, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Aknin, L.B.; Barrington-Leigh, C.P.; Dunn, E.W.; Helliwell, J.F.; Burns, J.; Biswas-Diener, R.; Kemeza, I.; Nyende, P.; Ashton-James, C.E.; Norton, M.I. Prosocial spending and well-being: Cross-cultural evidence for a psychological universal. J. Pers. Soc. Psychol. 2013, 104, 635–652. [Google Scholar] [CrossRef] [Green Version]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; van der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared with Adults: A Systematic Review and Meta-analysis. JAMA Pediatrics 2021, 175, 143–156. [Google Scholar] [CrossRef]
- Paterson, P.; Chantler, T.; Larson, H.J. Reasons for non-vaccination: Parental vaccine hesitancy and the childhood influenza vaccination school pilot programme in England. Vaccine 2018, 36, 5397–5401. [Google Scholar] [CrossRef]
- Dergaa, I.; Abdelrahman, H.; Varma, A.; Yousfi, N.; Souissi, A.; Ghram, A.; Hammad, A.S.; Musa, E.R.; Taher, M.; Irandoust, K.; et al. COVID-19 Vaccination, Herd Immunity and The Transition Toward Normalcy: Challenges with The Upcoming Sports Events. Ann. Appl. Sport Sci. 2021, 9. [Google Scholar] [CrossRef]
- WHO. Call to Action: Vaccine Equity. 18 January 2021. Available online: https://www.who.int/campaigns/annual-theme/year-of-health-and-care-workers-2021/vaccine-equity-declaration (accessed on 26 June 2021).
- Musa, S.; Al Baker, W.; Al Muraikhi, H.; Nazareno, D.; Al Naama, A.; Dergaa, I. Wellness Program Within Primary Health Care: How to Avoid “No Show” to Planned Appointments?—A Patient-Centred Care Perspective. Phys. Act. Health 2021, 5. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total n = 4023 (100%) | Vaccine Booking Status | Multivariate Analysis (Binary Logistic Regression) | |||
|---|---|---|---|---|---|---|
| Acceptance n = 3303 (82.10%) | Hesitancy n = 720 (17.90%) | OR | 95% CI | p-Value | ||
| Adolescents’ Age Groups | ||||||
| 12 years | 1100 (27.34) | 78.36 | 21.64 | 1.38 | 1.12–1.70 | 0.002 |
| 13 years | 1100 (27.34) | 84.00 a | 16.00 | 1.04 | 0.85–1.28 | 0.718 |
| 14 years | 959 (23.84) | 81.75 | 18.25 | 1.14 | 0.92–1.41 | 0.231 |
| 15 years | 864 (21.48) | 84.84 b | 15.16 | REF | ||
| Chi-2 test: p-value | 0.0001 * | |||||
| Sex | ||||||
| Boys | 1983 (49.29) | 82.25 | 17.75 | 0.98 | 0.85–1.13 | 0.775 |
| Girls | 2040 (50.71) | 81.96 | 18.04 | REF | ||
| Chi-2 test: p-value | 0.8104 | |||||
| Nationalities | ||||||
| Asiatic | 2552 (63.44) | 84.80 | 15.20 | 0.38 | 0.29–0.50 | 0.000 |
| North-African | 844 (20.98) | 79.62 a | 20.38 | 0.48 | 0.36–0.65 | 0.000 |
| African | 199 (4.95) | 82.91 | 17.09 | 0.41 | 0.27–0.62 | 0.000 |
| E & A & O | 113 (2.81) | 86.73 | 13.27 | 0.34 | 0.21–0.56 | 0.000 |
| GC (97% Qatari) | 315 (7.83) | 64.76 b–e | 35.24 | REF | ||
| Chi-2 test: p-value | 0.0001 * | |||||
| Chronic Disease | ||||||
| Yes | 503 (12.50) | 78.73 | 21.27 | 1.13 | 0.91–1.40 | 0.290 |
| No | 3520 (87.50) | 82.59 | 17.41 | REF | ||
| Chi-2 test: p-value | 0.0346 * | |||||
| COVID-19+ve | ||||||
| Yes | 253 (6.29) | 75.89 | 24.11 | 1.37 | 1.02–1.84 | 0.036 |
| No | 3770 (93.71) | 82.52 | 17.48 | REF | ||
| Chi-2 test: p-value | 0.0077 * | |||||
| Characteristics | Wait and See n = 509 (70.69%) | Definitely Refusal n = 187 (25.97%) | Currently Sick/COVID-19+ve n = 24 (3.34%) |
|---|---|---|---|
| Adolescents’ Age Groups | |||
| 12 years (n = 238) | 176 (73.95) | 59 (24.79) | 3 (1.26) |
| 13 years (n = 176) | 117 (66.48) | 50 (28.41) | 9 (5.11) |
| 14 years (n = 175) | 129 (73.71) | 40 (22.86) | 6 (3.43) |
| 15 years (n = 131) | 87 (66.41) | 38 (29.01) | 6 (4.58) |
| Chi-2 test: p-value | 0.21 | ||
| Sex | |||
| Boys (n = 352) | 248 (70.45) | 89 (25.28) | 15 (4.27) |
| Girls (n = 368) | 261 (70.92) | 98 (26.63) | 9 (2.45) |
| Chi-2 test: p-value | 0.38 | ||
| Nationalities | |||
| Asiatic (n = 388) | 287 (73.97) | 91 (23.45) | 10 (2.58) |
| North-African (n = 172) | 115 (66.86) | 52 (30.23) | 5 (2.91) |
| African (n = 34) | 24 (70.59) | 8 (23.53) | 2 (5.88) |
| E & A & O (n = 15) | 10 (66.67) | 5 (33.33) | 0 (0.00) |
| GC (n = 111; 91% Qatari) | 73 (65.77) | 31 (27.93) | 7 (6.30) |
| Chi-2 test: p-value | 0.34 | ||
| Chronic Disease | |||
| Yes (n = 107) | 61 (57.01) | 33 (30.84) | 13 (12.15) |
| No (n = 613) | 448 (73.08) | 154 (25.12) | 11 (1.80) |
| Chi-2 test: p-value | 0.03 *,a,b | ||
| COVID-19+ve | |||
| Yes (n = 61) | 39 (63.93) | 6 (9.84) | 16 (26.23) |
| No (n = 659) | 470 (71.32) | 181 (27.47) | 8 (1.21) |
| Chi-2 test: p-value | 0.02 *,a,b | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musa, S.; Dergaa, I.; Abdulmalik, M.A.; Ammar, A.; Chamari, K.; Saad, H.B. BNT162b2 COVID-19 Vaccine Hesitancy among Parents of 4023 Young Adolescents (12–15 Years) in Qatar. Vaccines 2021, 9, 981. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9090981
Musa S, Dergaa I, Abdulmalik MA, Ammar A, Chamari K, Saad HB. BNT162b2 COVID-19 Vaccine Hesitancy among Parents of 4023 Young Adolescents (12–15 Years) in Qatar. Vaccines. 2021; 9(9):981. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9090981
Chicago/Turabian StyleMusa, Sarah, Ismail Dergaa, Mariam Ali Abdulmalik, Achraf Ammar, Karim Chamari, and Helmi Ben Saad. 2021. "BNT162b2 COVID-19 Vaccine Hesitancy among Parents of 4023 Young Adolescents (12–15 Years) in Qatar" Vaccines 9, no. 9: 981. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9090981