
Sharing Mechanical Ventilator: In Vitro Evaluation of Circuit Cross-Flows and Patient Interactions

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
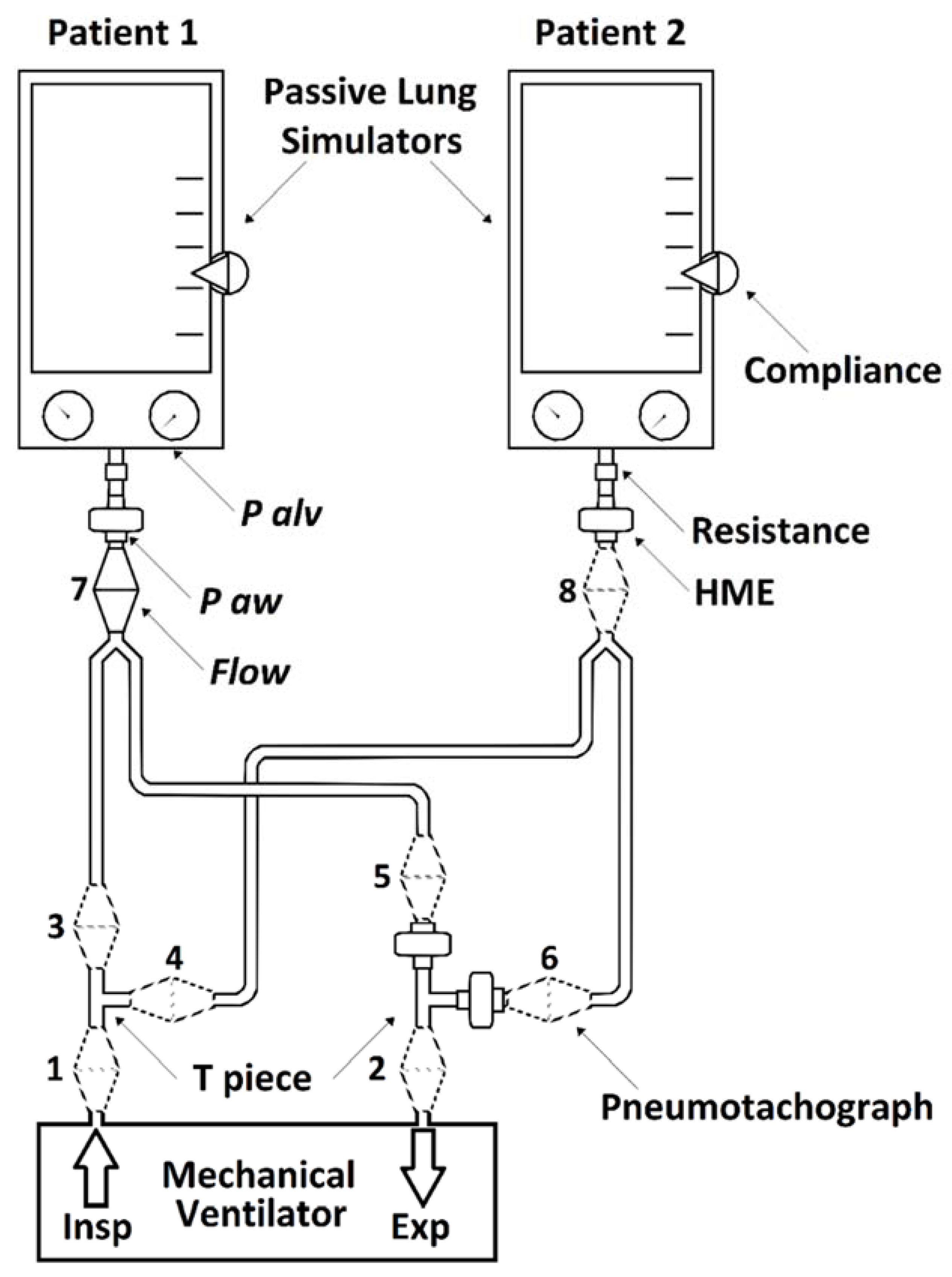
2.1. Laboratory Setting
- Inspiratory branch of ventilator (before T-piece);
- Expiratory branch of ventilator (after T-piece);
- Inspiratory branch of simulated patient 1 (after T-piece);
- Inspiratory branch of simulated patient 2 (after T-piece);
- Expiratory branch of simulated patient 1 (before T-piece and HME);
- Expiratory branches of simulated patient 2 (before T-piece and HME);
- Y-connector of simulated patient 1 (before HME);
- Y-connector of simulated patient 2 (before HME);
2.2. Graphical Representation and Statistical Analysis
3. Results
3.1. Relationships between Pressures, Volumes and Patients’ Mechanical Characteristics
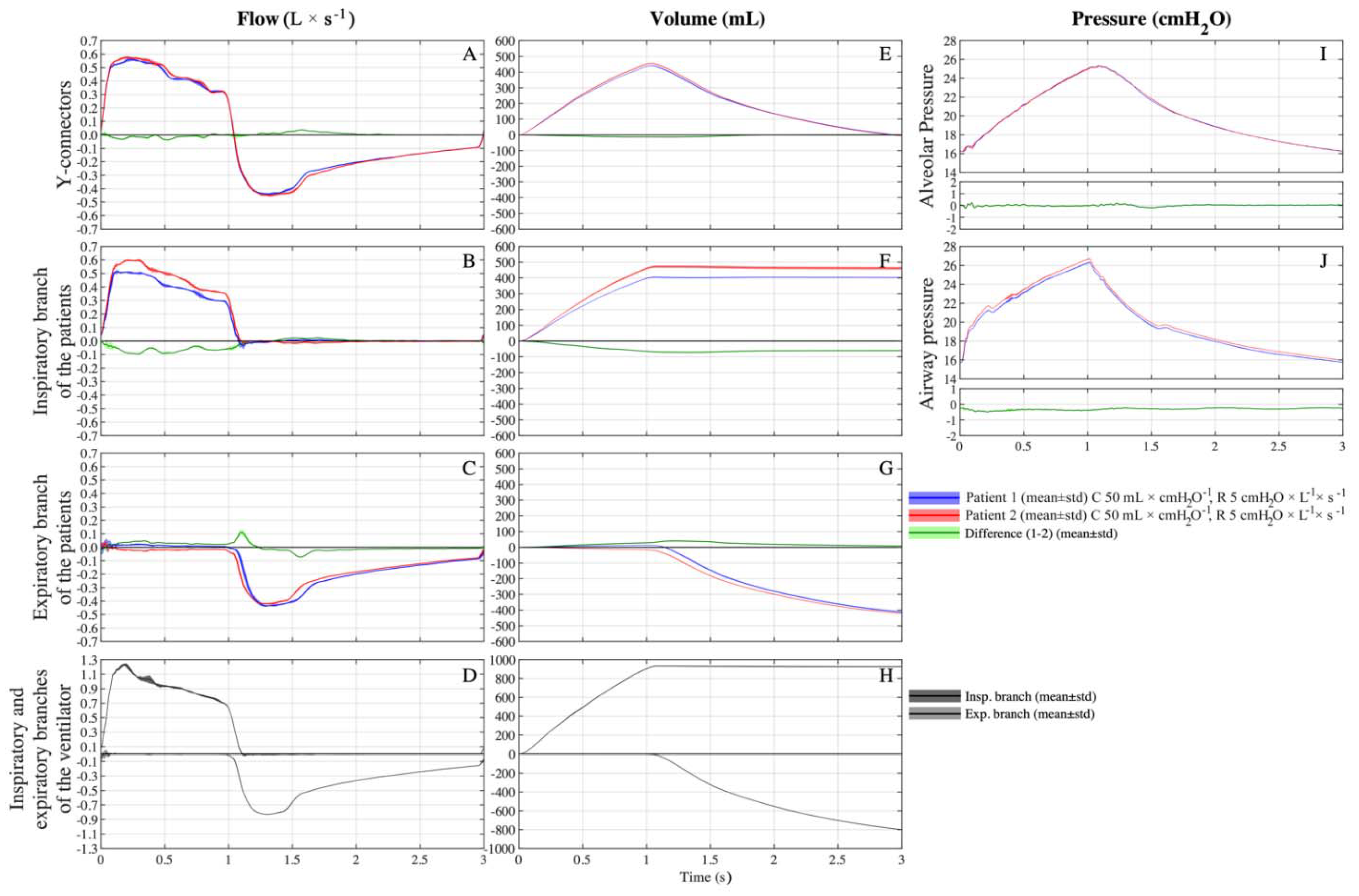
3.2. Setting C 50-50/R 5-5
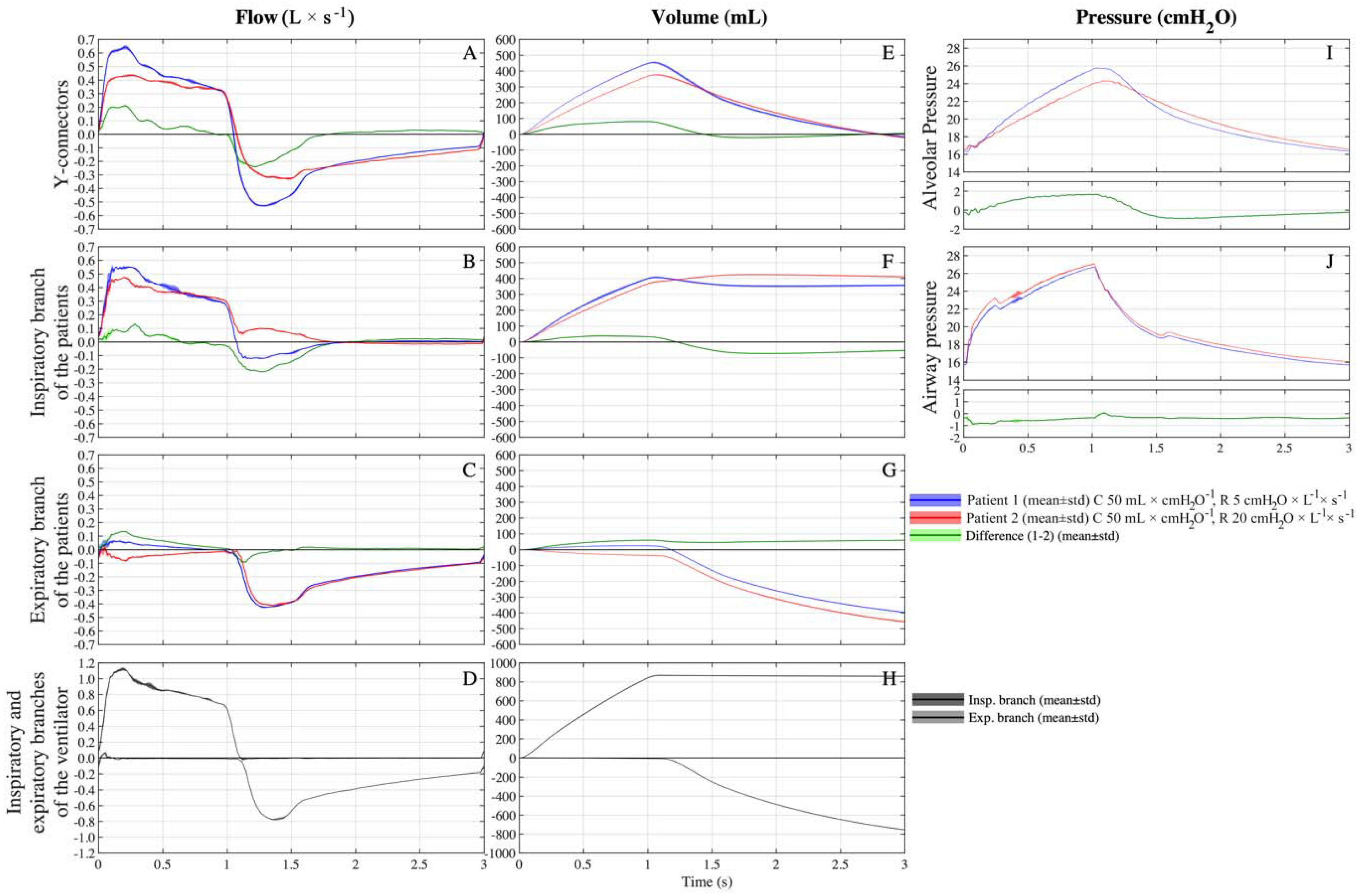
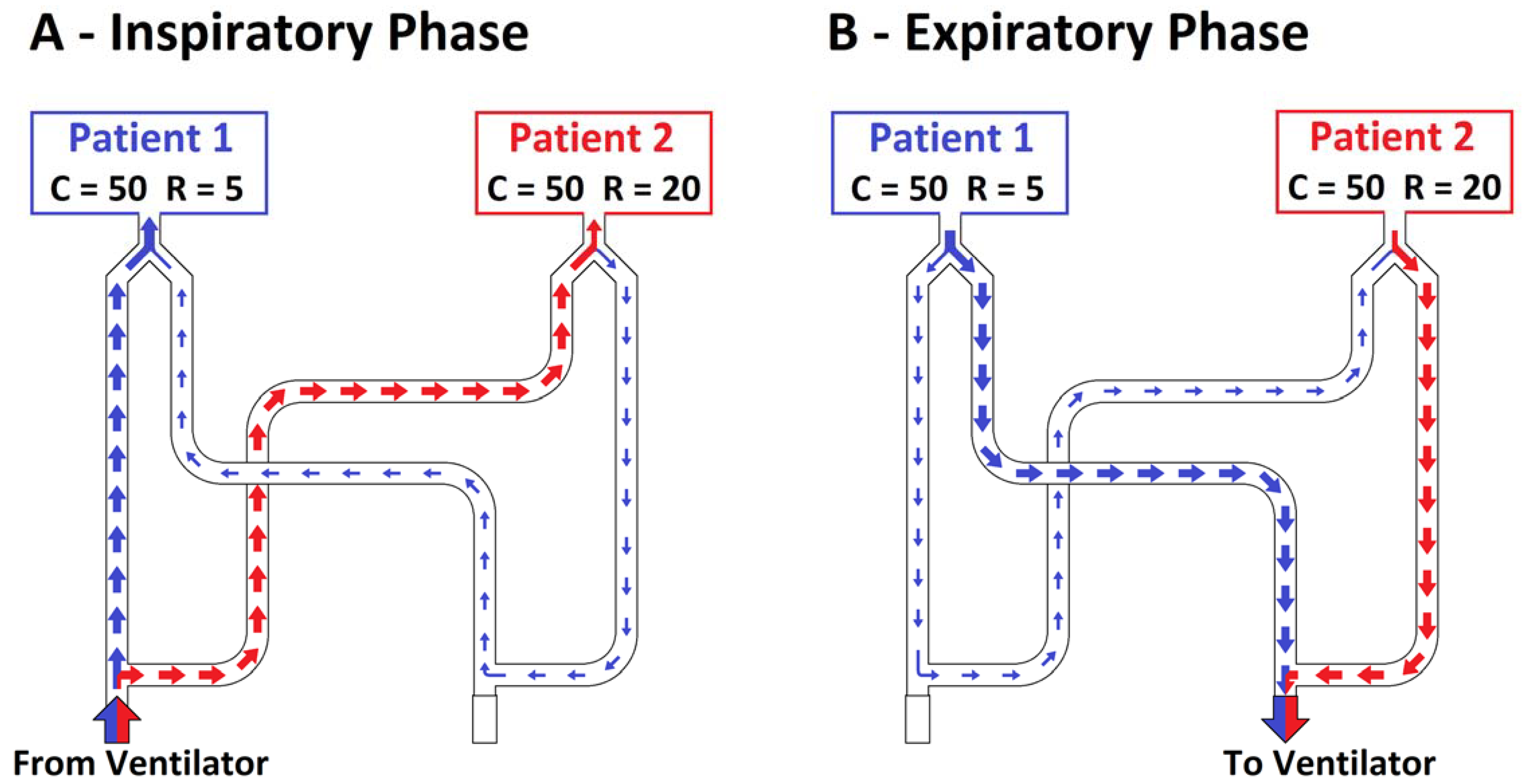
3.3. Setting C 50-50/R 5-20
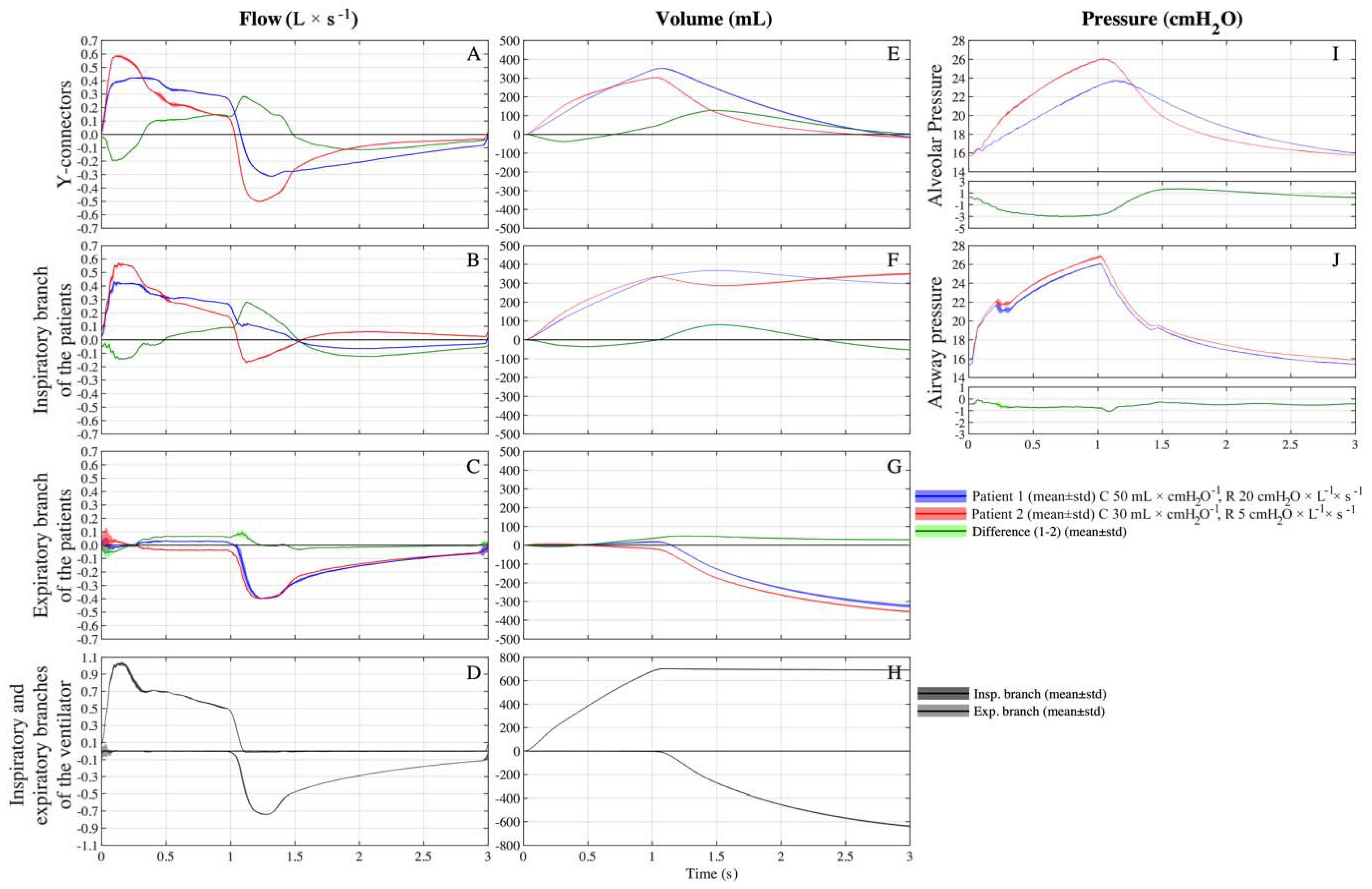
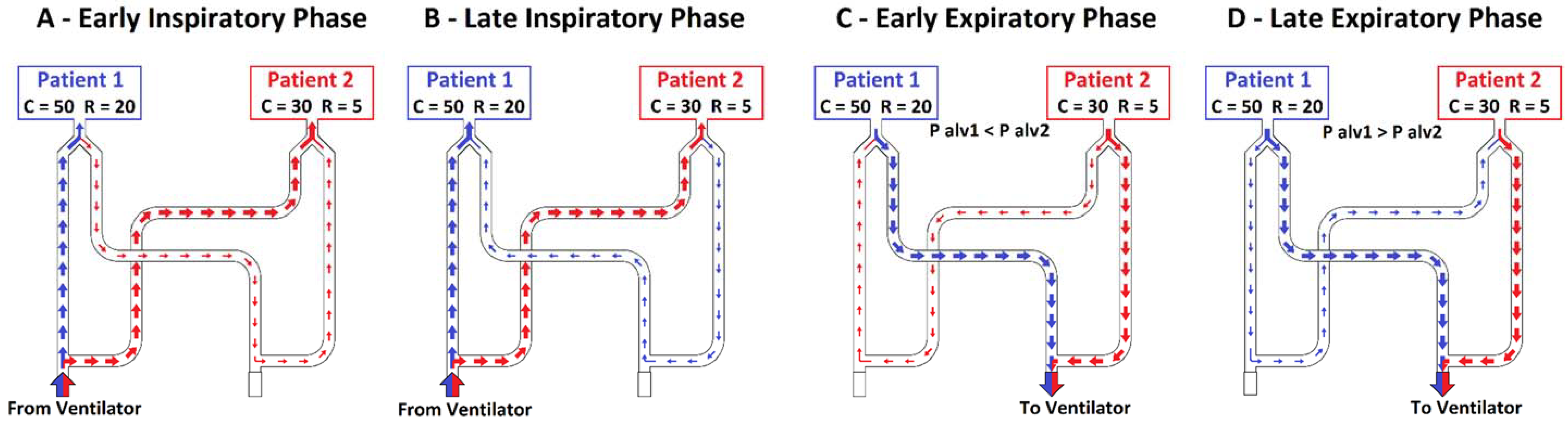
3.4. Setting C 50-30/R 20-5
3.5. Settings C 50-30/R 20-20 and C 50-30/R 5-20
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| C | compliance |
| CO2 | carbon dioxide |
| HME | heat and moisture exchanger |
| ICU | intensive care unit |
| PCV | pressure-controlled ventilation |
| P alv | alveolar pressure |
| P aw | airway pressure |
| PEEP | positive end expiratory pressure |
| Pt | patient |
| R | resistance |
| RR | respiratory rate |
| τ | time constant |
| VT | tidal volume |
References
- Aziz, S.; Arabi, Y.M.; Alhazzani, W.; Evans, L.; Citerio, G.; Fischkoff, K.; Salluh, J.; Meyfroidt, G.; Alshamsi, F.; Oczkowski, S.; et al. Managing ICU surge during the COVID-19 crisis: Rapid guidelines. Intensiv. Care Med. 2020, 46, 1303–1325. [Google Scholar] [CrossRef]
- Truog, R.D.; Mitchell, C.; Daley, G.Q. The Toughest Triage—Allocating Ventilators in a Pandemic. N. Engl. J. Med. 2020, 382, 1973–1975. [Google Scholar] [CrossRef]
- Ricard, J.-D. Manual ventilation and risk of barotrauma: Primum non nocere. Respir. Care 2005, 50, 338–339. [Google Scholar]
- Tonetti, T.; Zanella, A.; Pizzilli, G.; Babcock, C.I.; Venturi, S.; Nava, S.; Pesenti, A.; Ranieri, V.M. One ventilator for two patients: Feasibility and considerations of a last resort solution in case of equipment shortage. Thorax 2020, 75, 517–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turki, M.; Young, M.P.; Wagers, S.S.; Bates, J.H.T. Peak pressures during manual ventilation. Respir. Care 2005, 50, 340–344. [Google Scholar]
- Neyman, G.; Irvin, C.B. A single ventilator for multiple simulated patients to meet disaster surge. Acad. Emerg. Med. 2006, 13, 1246–1249. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonetti, T.; Grasselli, G.; Zanella, A.; Pizzilli, G.; Fumagalli, R.; Piva, S.; Lorini, L.; Iotti, G.; Foti, G.; Colombo, S.; et al. Use of critical care resources during the first 2 weeks (February 24–March 8, 2020) of the COVID-19 outbreak in Italy. Ann. Intensiv. Care 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Beitler, J.R.; Mittel, A.M.; Kallet, R.; Kacmarek, R.; Hess, D.; Branson, R.; Olson, M.; Garcia, I.; Powell, B.; Wang, D.S.; et al. Ventilator Sharing during an Acute Shortage Caused by the COVID-19 Pandemic. Am. J. Respir. Crit. Care Med. 2020, 202, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Branson, R.D.; Blakeman, T.C.; Robinson, B.R.; Johannigman, J.A. Use of a Single Ventilator to Support 4 Patients: Laboratory Evaluation of a Limited Concept. Respir. Care 2012, 57, 399–403. [Google Scholar] [CrossRef] [Green Version]
- Paladino, L.; Silverberg, M.; Charchaflieh, J.G.; Eason, J.K.; Wright, B.J.; Palamidessi, N.; Arquilla, B.; Sinert, R.; Manoach, S. Increasing ventilator surge capacity in disasters: Ventilation of four adult-human-sized sheep on a single ventilator with a modified circuit. Resuscitation 2008, 77, 121–126. [Google Scholar] [CrossRef] [PubMed]
- The Anesthesia Patient Safety Foundation (ASPF); Society of Critical Care Medicine (SCCM); American Association for Respiratory Care (AARC); American Society of Anesthesiologists (ASA); American Association of Critical-Care Nurses (AACN); American College of Chest Physicians (CHEST). Joint Statement on Multiple Patients Per Ventilator. 2020. Available online: https://www.apsf.org/news-updates/joint-statement-on-multiple-patients-per-ventilator/ (accessed on 15 July 2021).
- Eijo, P.M.G.; D’Adamo, J.; Bianchetti, A.; Duriez, T.; Cabaleiro, J.M.; Irrazabal, C.; Otero, P.; Artana, G. Exhalatory dynamic interactions between patients connected to a shared ventilation device. PLoS ONE 2021, 16, e0250672. [Google Scholar] [CrossRef]
- VanKoevering, K.K.; Yalamanchi, P.; Haring, C.T.; Phillips, A.G.; Harvey, S.L.; Rojas-Pena, A.; Zopf, D.A.; Green, G.E. Delivery system can vary ventilatory parameters across multiple patients from a single source of mechanical ventilation. PLoS ONE 2020, 15, e0243601. [Google Scholar] [CrossRef]
- Korsós, A.; Peták, F.; Südy, R.; Schranc, Á.; Fodor, G.H.; Babik, B. Use of capnography to verify emergency ventilator sharing in the COVID-19 era. Respir. Physiol. Neurobiol. 2021, 285, 103611. [Google Scholar] [CrossRef] [PubMed]
- Wankum, B.P.; Reynolds, R.E.; McCain, A.R.; Zollinger, N.T.; Buesing, K.L.; Sindelar, R.D.; Freihaut, F.M.; Fekadu, T.; Terry, B.S. Development of a multi-patient ventilator circuit with validation in an ARDS porcine model. J. Anesth. 2021, 16, 1–12. [Google Scholar] [CrossRef]
- Petersen, L.G.; Friend, J.; Merritt, S. Single ventilator for multiple patients during COVID19 surge: Matching and balancing patients. Crit. Care 2020, 24, 357. [Google Scholar] [CrossRef]
- Cook, D.C. Implementing shared ventilation must be scientific and ethical, or it risks harm. Br. J. Anaesth. 2020, 125, e181–e183. [Google Scholar] [CrossRef]
- Laffey, J.G.; Chikhani, M.; Bates, D.G.; Hardman, J.G. Supporting more than one patient with a single mechanical ventilator: Useful last resort or unjustifiable risk? Br. J. Anaesth. 2020, 125, 247–250. [Google Scholar] [CrossRef]
- Bhatt, H.; Singh, S. The ethical dilemma of ventilator sharing during the COVID-19 pandemic. J. Glob. Health 2020, 10, 020392. [Google Scholar] [CrossRef]
- Chase, J.G.; Chiew, Y.-S.; Lambermont, B.; Morimont, P.; Shaw, G.M.; Desaive, T. In-Parallel Ventilator Sharing during an Acute Shortage: Too Much Risk for a Wider Uptake. Am. J. Respir. Crit. Care Med. 2020, 202, 1316–1317. [Google Scholar] [CrossRef]
- Carenzo, L.; Costantini, E.; Greco, M.; Barra, F.L.; Rendiniello, V.; Mainetti, M.; Bui, R.; Zanella, A.; Grasselli, G.; Lagioia, M.; et al. Hospital surge capacity in a tertiary emergency referral centre during the COVID-19 outbreak in Italy. Anaesthesia 2020, 75, 928–934. [Google Scholar] [CrossRef]
- Chiumello, D.A.; Carlesso, E.; Cadringher, P.; Caironi, P.; Valenza, F.; Polli, F.; Tallarini, F.; Cozzi, P.; Cressoni, M.; Colombo, A.; et al. Lung Stress and Strain during Mechanical Ventilation for Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2008, 178, 346–355. [Google Scholar] [CrossRef] [Green Version]
- Darowski, M.; Englisz, M. Artificial ventilation of the lungs for emergencies. Front. Med Biol. Eng. 2000, 10, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Chase, J.G.; Chiew, Y.S.; Lambermont, B.; Morimont, P.; Shaw, G.M.; Desaive, T. Safe doubling of ventilator capacity: A last resort proposal for last resorts. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Chatburn, R.L.; Branson, R.D.; Hatipoğlu, U. Multiplex Ventilation: A Simulation-Based Study of Ventilating 2 Patients with a Single Ventilator. Respir. Care 2020, 65, 920–931. [Google Scholar] [CrossRef] [PubMed]
- Clarke, A.L.; Stephens, A.F.; Liao, S.; Byrne, T.J.; Gregory, S.D. Coping with COVID-19: Ventilator splitting with differential driving pressures using standard hospital equipment. Anaesthesia 2020, 75, 872–880. [Google Scholar] [CrossRef]
- Han, J.S.; Mashari, A.; Singh, D.; Dianti, J.; Goligher, E.; Long, M.; Ng, W.; Wasowicz, M.; Preiss, D.; Vesely, A.; et al. Personalized Ventilation to Multiple Patients Using a Single Ventilator: Description and Proof of Concept. Crit. Care Explor. 2020, 2, e0118. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J.; Da Cruz, A.F.; Hawley, M.L.; Branson, R.D.; Kaczka, D.W. Shared Ventilation in the Era of COVID-19: A Theoretical Consideration of the Dangers and Potential Solutions. Respir. Care 2020, 65, 932–945. [Google Scholar] [CrossRef] [PubMed]
- Kheyfets, V.O.; Lammers, S.R.; Wagner, J.; Bartels, K.; Piccoli, J.; Smith, B.J. PEEP/FIO2 ARDSNet Scale Grouping of a Single Ventilator for Two Patients: Modeling Tidal Volume Response. Respir. Care 2020, 65, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; Siner, J.M.; Balcezak, T.; Fajardo, E. Ventilator Sharing Using Volume-controlled Ventilation during the COVID-19 Pandemic. Am. J. Respir. Crit. Care Med. 2020, 202, 1317–1319. [Google Scholar] [CrossRef]
- Levin, M.; Shah, A.; Shah, R.; Kane, E.; Zhou, G.; Eisenkraft, J.B.; Chen, M.D. Mount Sinai HELPS Innovate Group; Differential Ventilation Using Flow Control Valves as a Potential Bridge to Full Ventilatory Support during the COVID-19 Crisis. Anesthesiology 2020, 133, 892–904. [Google Scholar] [CrossRef]
- Doukas, D.J.; Paladino, L.; Hanuscin, C.; McMahon, J.; Quale, J.; Bhatt, I.; Eason, J.; Silverberg, M. Evaluating cross contamination on a shared ventilator. Emerg. Med. J. 2021, 38, 220–223. [Google Scholar] [CrossRef] [PubMed]
- King, W.P.; Amos, J.; Azer, M.; Baker, D.; Bashir, R.; Best, C.; Bethke, E.; Boppart, S.A.; Bralts, E.; Corey, R.M.; et al. Emergency ventilator for COVID-19. PLoS ONE 2020, 15, e0244963. [Google Scholar] [CrossRef]
- Stiers, M.; Mergeay, M.; Pinson, H.; Janssen, L.; Voets, E.; De Cauwer, H.; Schepens, T. Individualized mechanical ventilation in a shared ventilator setting: Limits, safety and technical details. J. Clin. Monit. 2020, 1–11. [Google Scholar] [CrossRef]
- Chen, G.H.; Hellman, S.; Irie, T.; Downey, R.J.; Fischer, G.W. Regulating inspiratory pressure to individualise tidal volumes in a simulated two-patient, one-ventilator system. Br. J. Anaesth. 2020, 125, e366–e368. [Google Scholar] [CrossRef]
- Webb, J.B.; Bray, A.; Asare, P.K.; Clipp, R.B.; Mehta, Y.B.; Penupolu, S.; Patel, A.A.; Poler, S.M. Computational simulation to assess patient safety of uncompensated COVID-19 two-patient ventilator sharing using the Pulse Physiology Engine. PLoS ONE 2020, 15, e0242532. [Google Scholar] [CrossRef]
- Solís-Lemus, J.A.; Costar, E.; Doorly, D.; Kerrigan, E.C.; Kennedy, C.H.; Tait, F.; Niederer, S.; Vincent, P.E.; Williams, S.E. A simulated single ventilator/dual patient ventilation strategy for acute respiratory distress syndrome during the COVID-19 pandemic. R. Soc. Open Sci. 2020, 7, 200585. [Google Scholar] [CrossRef] [PubMed]
- Stiers, M.; Bleeser, T.; Mergeay, M.; Pinson, H.; Janssen, L.; Schepens, T. Successful ventilation of two animals with a single ventilator: Individualized shared ventilator setup in an in vivo model. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Branson, R.; Dichter, J.R.; Feldman, H.; Devereaux, A.; Dries, D.; Benditt, J.; Hossain, T.; Ghazipura, M.; King, M.; Baldisseri, M.; et al. The US Strategic National Stockpile Ventilators in Coronavirus Disease 2019: A Comparison of Functionality and Analysis Regarding the Emergency Purchase of 200,000 Devices. Chest 2021, 159, 634–652. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Setting | C 50-50/R 5-5 | C 50-50/R 5-20 | C 50-30/R 20-20 | C 50-30/R 5-20 | C 50-30/R 20-5 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C | R | τ | C | R | τ | C | R | τ | C | R | τ | C | R | τ | |
| Patient 1 | 50 | 5 | 0.25 | 50 | 5 | 0.25 | 50 | 20 | 1.00 | 50 | 5 | 0.25 | 50 | 20 | 1.00 |
| Patient 2 | 50 | 5 | 0.25 | 50 | 20 | 1.00 | 30 | 20 | 0.60 | 30 | 20 | 0.60 | 30 | 5 | 0.15 |
| Setting | Pt | Tidal Volume at Y-Connectors (mL) | p | Min. Alveolar Pressure (cmH2O) | p | Max. Alveolar Pressure (cmH2O) | p | Inspiratory Time Cross-Volumes (mL) | Expiratory Time Cross-Volumes (mL) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| C 50-50/ R 5-5 | 1 | 441 ± 2 | <0.001 | 16.26 ± 0.01 | 0.286 | 25.33 ± 0.01 | 0.673 | ||||
| 2 | 455 ± 2 | 16.24 ± 0.03 | 25.32 ± 0.05 | ||||||||
| C 50-50/ R 5-20 | 1 | 455 ± 5 | <0.001 | 16.32 ± 0.03 | <0.001 | 25.78 ± 0.02 | <0.001 | 23.8 mL from Pt 2 to Pt 1 | 50.4 mL from Pt 1 to Pt 2 | ||
| 2 | 377 ± 3 | 16.57 ± 0.04 | 24.33 ± 0.03 | ||||||||
| C 50-30/ R 20-20 | 1 | 372 ± 2 | <0.001 | 15.88 ± 0.03 | <0.001 | 23.52 ± 0.05 | <0.001 | 26.6 mL from Pt 2 to Pt 1 | 7.5 mL from Pt 2 to Pt 1 E1 | 54.9 mL from Pt 1 to Pt 2 L1 | |
| 2 | 283 ± 2 | 15.5 ± 0.04 | 25.05 ± 0.07 | ||||||||
| C 50-30/ R 5-20 | 1 | 473 ± 4 | <0.001 | 15.73 ± 0.03 | <0.001 | 24.84 ± 0.02 | <0.001 | 33.6 mL from Pt 2 to Pt 1 | 92.9 mL from Pt 1 to Pt 2 | ||
| 2 | 269 ± 3 | 15.5 ± 0.04 | 25.05 ± 0.04 | ||||||||
| C 50-30/ R 20-5 | 1 | 352 ± 3 | <0.001 | 15.94 ± 0.02 | <0.001 | 23.75 ± 0.04 | <0.001 | 6.1 mL from Pt 1 to Pt 2 E2 | 18 mL from Pt 2 to Pt 1 L2 | 30.4 mL from Pt 2 to Pt 1 E3 | 70.9 mL from Pt 1 to Pt 2 L3 |
| 2 | 303 ± 2 | 15.7 ± 0.03 | 26.05 ± 0.07 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombo, S.M.; Battistin, M.; Carlesso, E.; Vivona, L.; Carfagna, F.; Valsecchi, C.; Florio, G.; Carenzo, L.; Tonetti, T.; Ranieri, V.M.; et al. Sharing Mechanical Ventilator: In Vitro Evaluation of Circuit Cross-Flows and Patient Interactions. Membranes 2021, 11, 547. https://0-doi-org.brum.beds.ac.uk/10.3390/membranes11070547
Colombo SM, Battistin M, Carlesso E, Vivona L, Carfagna F, Valsecchi C, Florio G, Carenzo L, Tonetti T, Ranieri VM, et al. Sharing Mechanical Ventilator: In Vitro Evaluation of Circuit Cross-Flows and Patient Interactions. Membranes. 2021; 11(7):547. https://0-doi-org.brum.beds.ac.uk/10.3390/membranes11070547
Chicago/Turabian StyleColombo, Sebastiano Maria, Michele Battistin, Eleonora Carlesso, Luigi Vivona, Fabio Carfagna, Carlo Valsecchi, Gaetano Florio, Luca Carenzo, Tommaso Tonetti, Vito Marco Ranieri, and et al. 2021. "Sharing Mechanical Ventilator: In Vitro Evaluation of Circuit Cross-Flows and Patient Interactions" Membranes 11, no. 7: 547. https://0-doi-org.brum.beds.ac.uk/10.3390/membranes11070547