Risk of Contracting COVID-19, Personal Resources and Subjective Well-Being among Healthcare Workers: The Mediating Role of Stress and Meaning-Making



Abstract
:1. Introduction
1.1. Risk of Contracting COVID-19, Personal Resources, and Subjective Well-Being
1.2. Meaning-Making and Stress as Potential Mediators
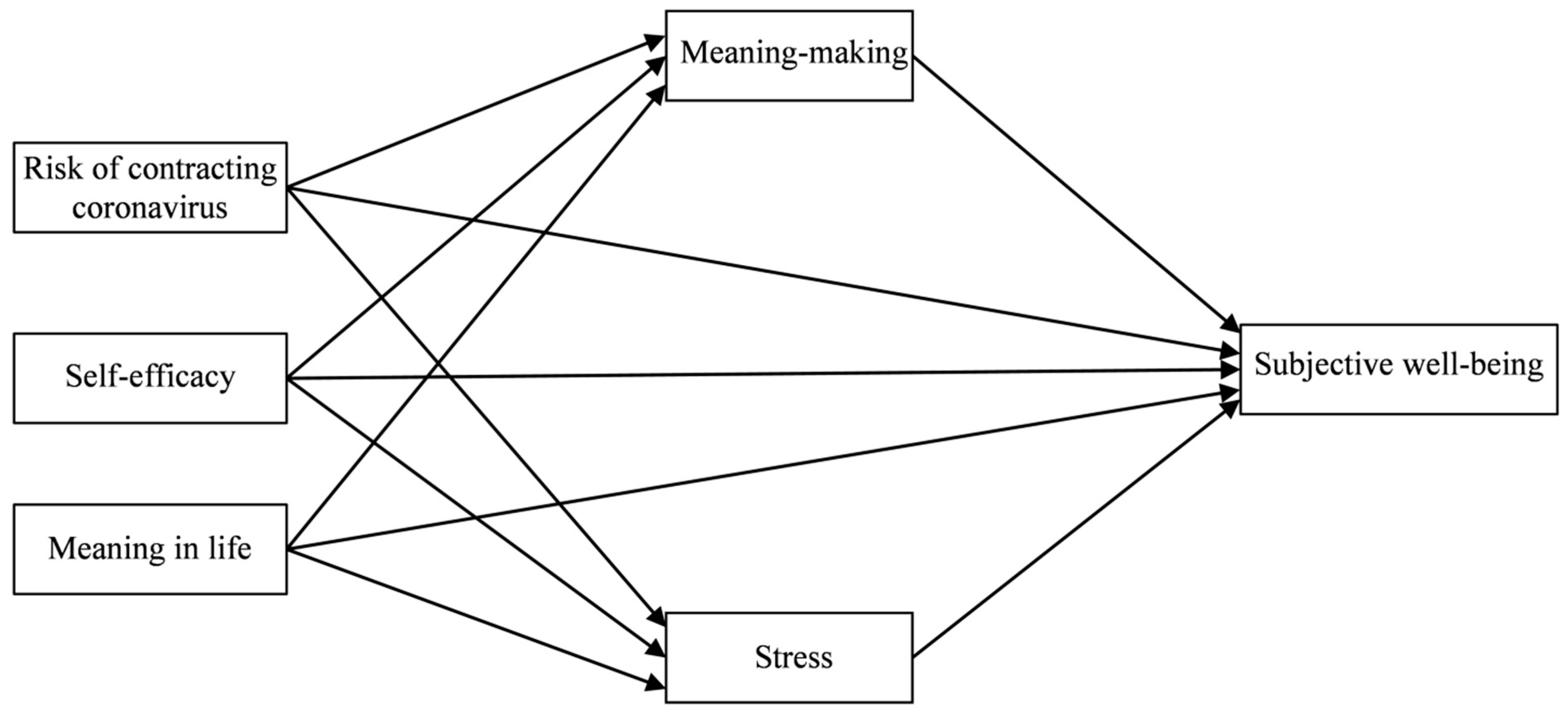
1.3. The Current Study
2. Method
2.1. Participants and Procedure
2.2. Measures
2.2.1. Risk of Contracting COVID-19
2.2.2. Self-Efficacy
2.2.3. Meaning in Life
2.2.4. Meaning-Making
2.2.5. Stress
2.2.6. Subjective Well-Being
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics and Initial Correlations
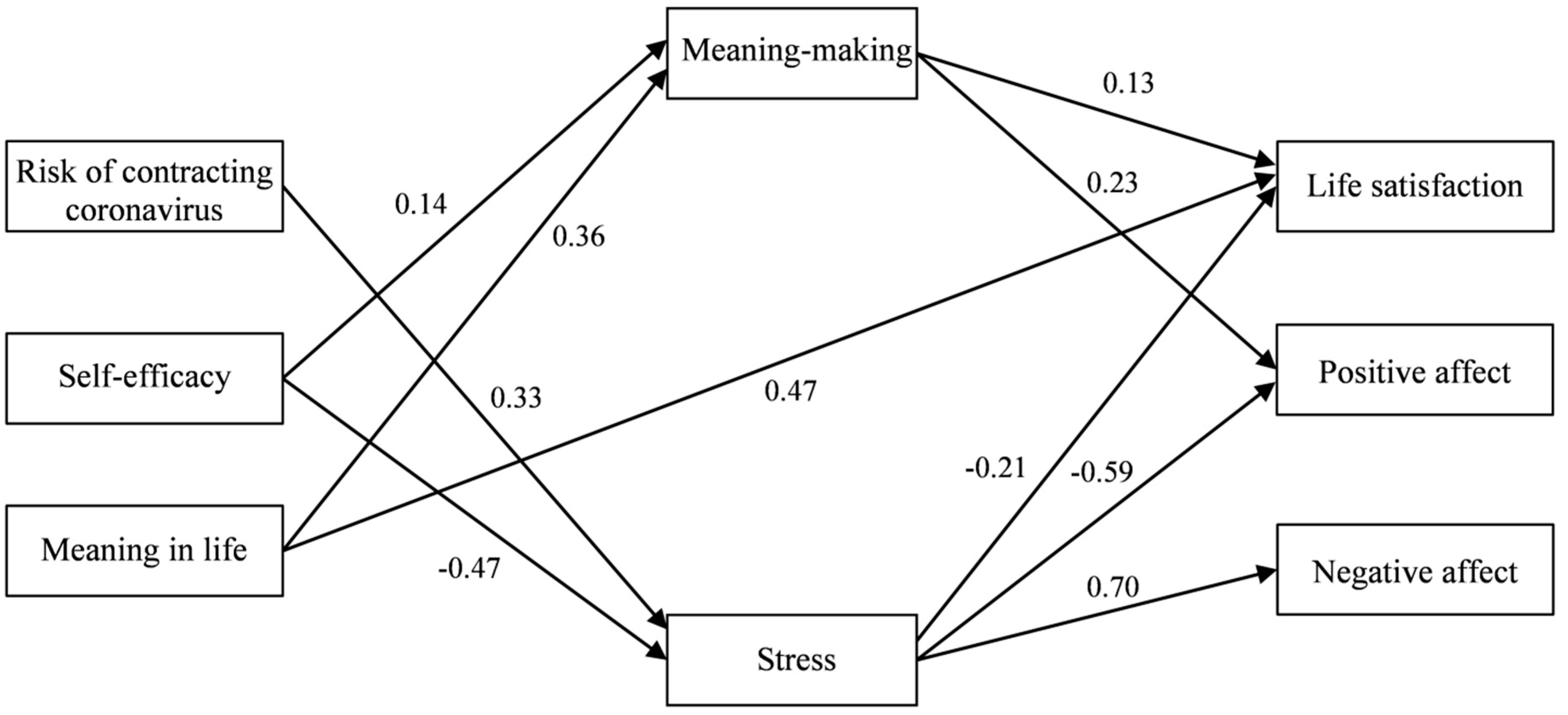
3.2. Testing Mediational Relations Using Path Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neto, M.L.R.; Almeida, H.G.; Esmeraldo, J.D.; Nobre, C.B.; Pinheiro, W.R.; de Oliveira, C.R.T.; da Costa Sousa, I.; Lima, O.M.M.L.; Lima, N.N.R.; Moreira, M.M.; et al. When health professionals look death in the eye: The mental health of professionals who deal daily with the 2019 coronavirus outbreak. Psychiatry Res. 2020, 288, 112972. [Google Scholar] [CrossRef]
- Krok, D.; Zarzycka, B. Risk Perception of COVID-19, Meaning-Based Resources and Psychological Well-Being amongst Healthcare Personnel: The Mediating Role of Coping. J. Clin. Med. 2020, 9, 3225. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.M.Y.; Kwong-Lo, R.S.Y.; Mak, C.W.Y.; Wong, J.S. Fear of severe acute respiratory syndrome (SARS) among health care workers. J. Consult. Clin. Psychol. 2005, 73, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Maunder, R.G.; Lancee, W.J.; Rourke, S.; Hunter, J.J.; Goldbloom, D.; Balderson, K.; Petryshen, P.; Steinberg, R.; Wasylenki, D.; Koh, D.; et al. Factors Associated With the Psychological Impact of Severe Acute Respiratory Syndrome on Nurses and Other Hospital Workers in Toronto. Psychosom. Med. 2004, 66, 938–942. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.W.C.; Pang, E.P.F.; Lam, L.C.W.; Chiu, H.F.K. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: Stress and psychological impact among frontline healthcare workers. Psychol. Med. 2004, 34, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- de Pablo, G.S.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Shacham, M.; Hamama-Raz, Y.; Kolerman, R.; Mijiritsky, O.; Ben-Ezra, M.; Mijiritsky, E. COVID-19 Factors and Psychological Factors Associated with Elevated Psychological Distress among Dentists and Dental Hygienists in Israel. Int. J. Environ. Res. 2020, 17, 2900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.K.W.; Chong, G.H.C.; Chang, S.S.Y.; Wong, C.W.; Wong, C.S.Y.; Wong, M.T.P.; Wong, K.C. Adjustment to severe acute respiratory syndrome (SARS): Roles of appraisal and post-traumatic growth. Psychol. Health 2006, 21, 301–317. [Google Scholar] [CrossRef]
- Li, J.B.; Yang, A.; Dou, K.; Wang, L.-X.; Zhang, M.-C.; Lin, X. Chinese public’s knowledge, perceived severity, and perceived controllability of the COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: A national survey. BMC Public Health 2020. [Google Scholar] [CrossRef]
- Li, J.B.; Yang, A.; Dou, K.; Cheung, R.Y.M. Self-control moderates the association between perceived severity of the coronavirus disease 2019 (COVID-19) and mental health problems among the Chinese public. Int. J. Environ. Res. Public Health 2020, 17, 4820. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, K.; Yin, L.; Zhao, W.; Xue, Q.; Peng, M.; Min, B.; Tian, Q.; Leng, H.; Du, J.; et al. Mental Health and Psychosocial Problems of Medical Health Workers during the COVID-19 Epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floyd, D.L.; Prentice-Dunn, S.; Rogers, R.W. A Meta-Analysis of Research on Protection Motivation Theory. J. Appl. Soc. Psychol. 2000, 30, 407–429. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Johnson, R.J.; Ennis, N.; Jackson, A.P. Resource loss, resource gain, and emotional outcomes among inner city women. J. Personal. Soc. Psychol. 2003, 84, 632–643. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Taris, T.W. A critical review of the job demands-resources model: Implications for improving work and health. In Bridging Occupational, Organizational and Public Health; Bauer, G.F., Hämmig, O., Eds.; Springer: Amsterdam, The Netherlands, 2014; p. 4368. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. The Job Demands-Resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef] [Green Version]
- Shiri, S.; Wexler, I.; Marmor, A.; Meiner, Z.; Schwartz, I.; Levzion Korach, O.; Azoulay, D. Hospice Care: Hope and Meaning in Life Mediate Subjective Well-Being of Staff. Am. J. Hosp. Palliat. Care 2020, 37, 785–790. [Google Scholar] [CrossRef]
- Güngör, A.; Uçman, A.G. Depression and hopelessness in Turkish healthcare workers: The moderating and mediating roles of meaning in life. Glob. Public Health 2020, 15, 236–246. [Google Scholar] [CrossRef]
- Reker, G.T.; Wong, P.T. Personal meaning in life and psychosocial adaptation in the later years. In The Human Quest for Meaning: Theories, Research, and Applications; Wong, P.T., Ed.; Routledge: New York, NY, USA; London, UK, 2012; p. 433456. [Google Scholar]
- Park, C.L. Meaning Making in the Context of Disasters: Meaning Making in the Context of Disasters. J. Clin. Psychol. 2016, 72, 1234–1246. [Google Scholar] [CrossRef]
- Miller, K.A.; Wojcik, K.Y.; Ramirez, C.N.; Ritt-Olson, A.; Freyer, D.R.; Hamilton, A.S.; Milam, J.E. Supporting long-term follow-up of young adult survivors of childhood cancer: Correlates of healthcare self-efficacy. Pediatr. Blood Cancer 2017, 64, 358–363. [Google Scholar] [CrossRef] [Green Version]
- Milam, L.A.; Cohen, G.L.; Mueller, C.; Salles, A. The Relationship Between Self-Efficacy and Well-Being Among Surgical Residents. J. Surg. Educ. 2019, 76, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Westcott, R.; Ronan, K.; Bambrick, H.; Taylor, M. Expanding protection motivation theory: Investigating an application to animal owners and emergency responders in bushfire emergencies. BMC Psychol. 2017, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lachnit, I.; Park, C.L.; George, L.S. Processing and Resolving Major Life Stressors: An Examination of Meaning-Making Strategies. Cogn. Ther. Res. 2020, 44, 1015–1024. [Google Scholar] [CrossRef]
- Krok, D.; Zarzycka, B. Self-Efficacy and Psychological Well-Being in Cardiac Patients: Moderated Mediation by Affect and Meaning-Making. J. Psychol. 2020, 154, 411–425. [Google Scholar] [CrossRef] [PubMed]
- Van Seggelen-Damen, I.; van Dam, K. Self-reflection as a mediator between self-efficacy and well-being. J. Manag. Psychol. 2016, 31, 18–33. [Google Scholar] [CrossRef]
- Hooker, S.A.; Masters, K.S.; Park, C.L. A Meaningful Life Is a Healthy Life: A Conceptual Model Linking Meaning and Meaning Salience to Health. Rev. Gen. Psychol. 2018, 22, 11–24. [Google Scholar] [CrossRef] [Green Version]
- Spinelli, M.; Lionetti, F.; Pastore, M.; Fasolo, M. Parents and Children Facing the COVID-19 Outbreak in Italy; Social Science Research Network: Rochester, NY, USA, 2020. [Google Scholar]
- Zhang, M.; Hong, L.; Zhang, T.; Lin, Y.; Zheng, S.; Zhou, X.; Fan, R.; Wang, Z.; Zhang, C.; Zhong, J. Illness perceptions and stress: Mediators between disease severity and psychological well-being and quality of life among patients with Crohn’s disease. Patient Prefer. Adherence 2016, 10, 2387–2396. [Google Scholar] [CrossRef] [Green Version]
- Urquijo, I.; Extremera, N.; Villa, A. Emotional Intelligence, Life Satisfaction, and Psychological Well-Being in Graduates: The Mediating Effect of Perceived Stress. Appl. Res. Qual. Life 2016, 11, 1241–1252. [Google Scholar] [CrossRef]
- Krok, D. The Risk of Contracting COVID-19 Scale; Department of Psychology, University of Opole: Opole, Poland, 2020. [Google Scholar]
- Grothmann, T.; Reusswig, F. People at Risk of Flooding: Why Some Residents Take Precautionary Action While Others Do Not. Nat. Hazards 2006, 38, 101–120. [Google Scholar] [CrossRef]
- Schwarzer, R.; Jerusalem, M. Generalised Self-Efficacy Scale. In Measures in Health Psychology: A user’s Portfolio. Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; Nfer-Nelson: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Steger, M.F.; Frazier, P.; Oishi, S.; Kaler, M. The meaning in life questionnaire: Assessing the presence of and search for meaning in life. J. Couns. Psychol. 2006, 53, 80–93. [Google Scholar] [CrossRef]
- Krok, D. The Meaning-Making Questionnaire (MMQ); Department of Psychology, University of Opole: Opole, Poland, 2018. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health. Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A. The PANAS-X: Manual for the Positive and Negative Affect Schedule-Expanded Form; The University of Iowa: Iowa City, IA, USA, 1999. [Google Scholar]
- Arbuckle, J.L. IBM SPSS Amos 21; Amos Development Corporation: Chicago, IL, USA, 2012. [Google Scholar]
- Fairchild, A.J.; MacKinnon, D.P.; Taborga, M.P.; Taylor, A.B. R2 effect-size measures for mediation analysis. Behav. Res. Methods 2009, 41, 486–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [Green Version]
- Park, C.L. Distinctions to Promote an Integrated Perspective on Meaning: Global Meaning and Meaning-Making Processes. J. Constr. Psychol. 2017, 30, 14–19. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Risk of contracting COVID-19 | 4.18 | 0.63 | − | ||||||
| 2 | Self-efficacy | 3.07 | 0.44 | 0.01 | − | |||||
| 3 | Meaning in life | 5.23 | 1.19 | 0.09 | 0.31 *** | − | ||||
| 4 | Meaning-making | 3.48 | 0.72 | 0.01 | 0.24 *** | 0.40 *** | − | |||
| 5 | Stress | 1.92 | 0.64 | 0.30 *** | −0.45 *** | −0.20 ** | −0.16 * | − | ||
| 6 | Life satisfaction | 4.37 | 0.99 | −0.09 | 0.28 *** | 0.53 *** | 0.28 *** | −0.31 *** | − | |
| 7 | Positive affect | 3.03 | 0.73 | −0.21 ** | 0.41 *** | 0.27 *** | 0.30 *** | −0.61 *** | 0.36 *** | − |
| 8 | Negative affect | 2.23 | 0.77 | 0.29 *** | −0.33 *** | −0.16 * | −0.09 | 0.68 *** | −0.22 *** | −0.47 *** |
| Model Pathways | Estimates | 95% CI | |
|---|---|---|---|
| Lower | Upper | ||
| Risk of contracting COVID-19 → Stress → Life satisfaction | −0.07 | −0.12 | −0.03 |
| Risk of contracting COVID-19 → Stress → Positive affect | −0.20 | −0.27 | −0.13 |
| Risk of contracting COVID-19 → Stress → Negative affect | 0.23 | 0.14 | 0.31 |
| Self-efficacy → Meaning-making/Stress → Life satisfaction | 0.11 | 0.05 | 0.17 |
| Self-efficacy → Meaning-making/Stress → Positive affect | 0.31 | 0.2 | 0.4 |
| Self-efficacy → Stress → Negative affect | −0.32 | −0.42 | −0.22 |
| Meaning in life → Meaning-making → Life satisfaction | 0.07 | 0.01 | 0.12 |
| Meaning in life → Meaning-making → Positive affect | 0.09 | 0.03 | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krok, D.; Zarzycka, B.; Telka, E. Risk of Contracting COVID-19, Personal Resources and Subjective Well-Being among Healthcare Workers: The Mediating Role of Stress and Meaning-Making. J. Clin. Med. 2021, 10, 132. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010132
Krok D, Zarzycka B, Telka E. Risk of Contracting COVID-19, Personal Resources and Subjective Well-Being among Healthcare Workers: The Mediating Role of Stress and Meaning-Making. Journal of Clinical Medicine. 2021; 10(1):132. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010132
Chicago/Turabian StyleKrok, Dariusz, Beata Zarzycka, and Ewa Telka. 2021. "Risk of Contracting COVID-19, Personal Resources and Subjective Well-Being among Healthcare Workers: The Mediating Role of Stress and Meaning-Making" Journal of Clinical Medicine 10, no. 1: 132. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010132