Clinical Value of CT for Differentiation between Ascites and Hemorrhage: An Experimental In-Vitro Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
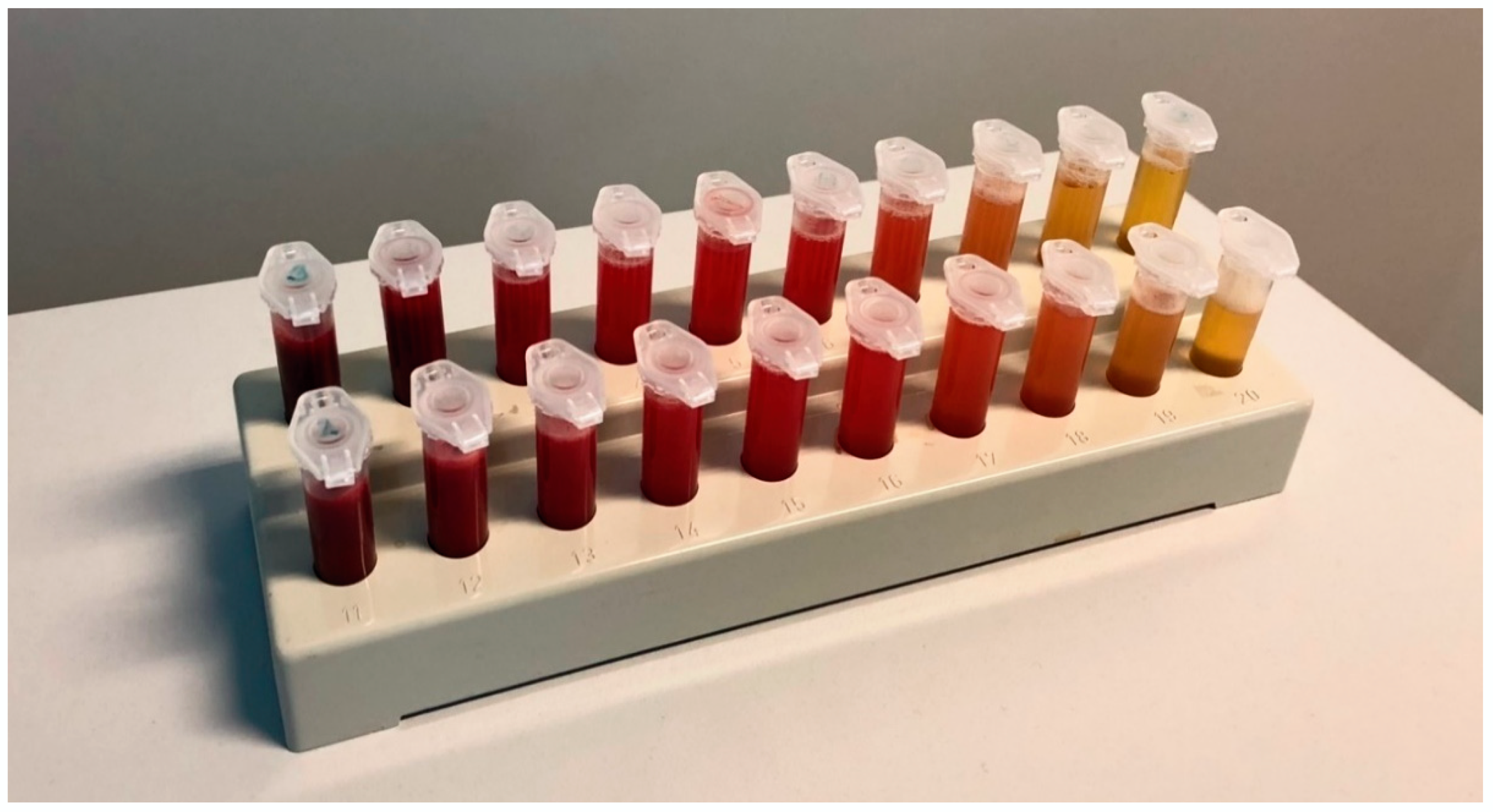
2.2. Sample Processing
2.3. Laboratory-Chemical Analysis
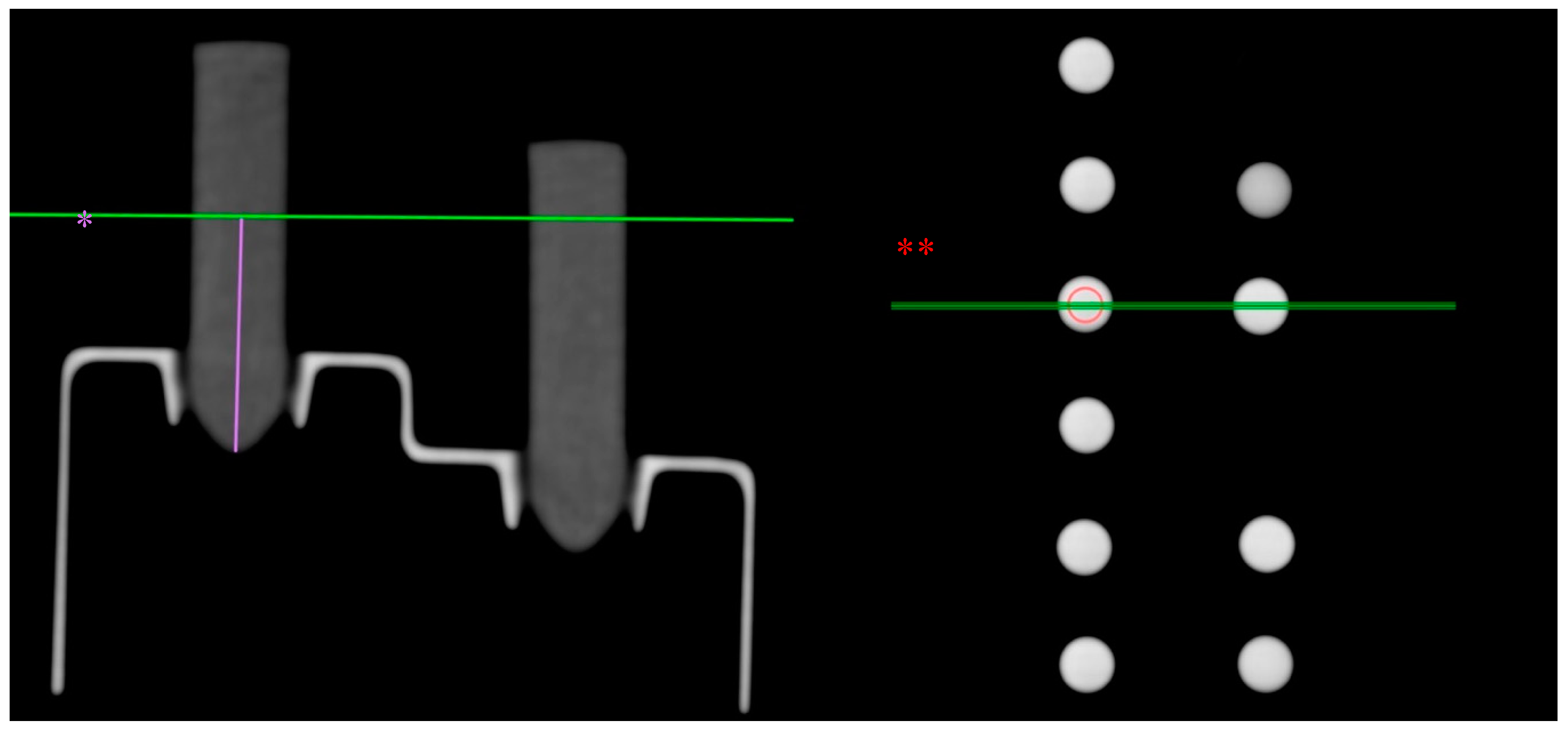
2.4. Radiological Evaluation
2.5. Statistical Evaluation
3. Results
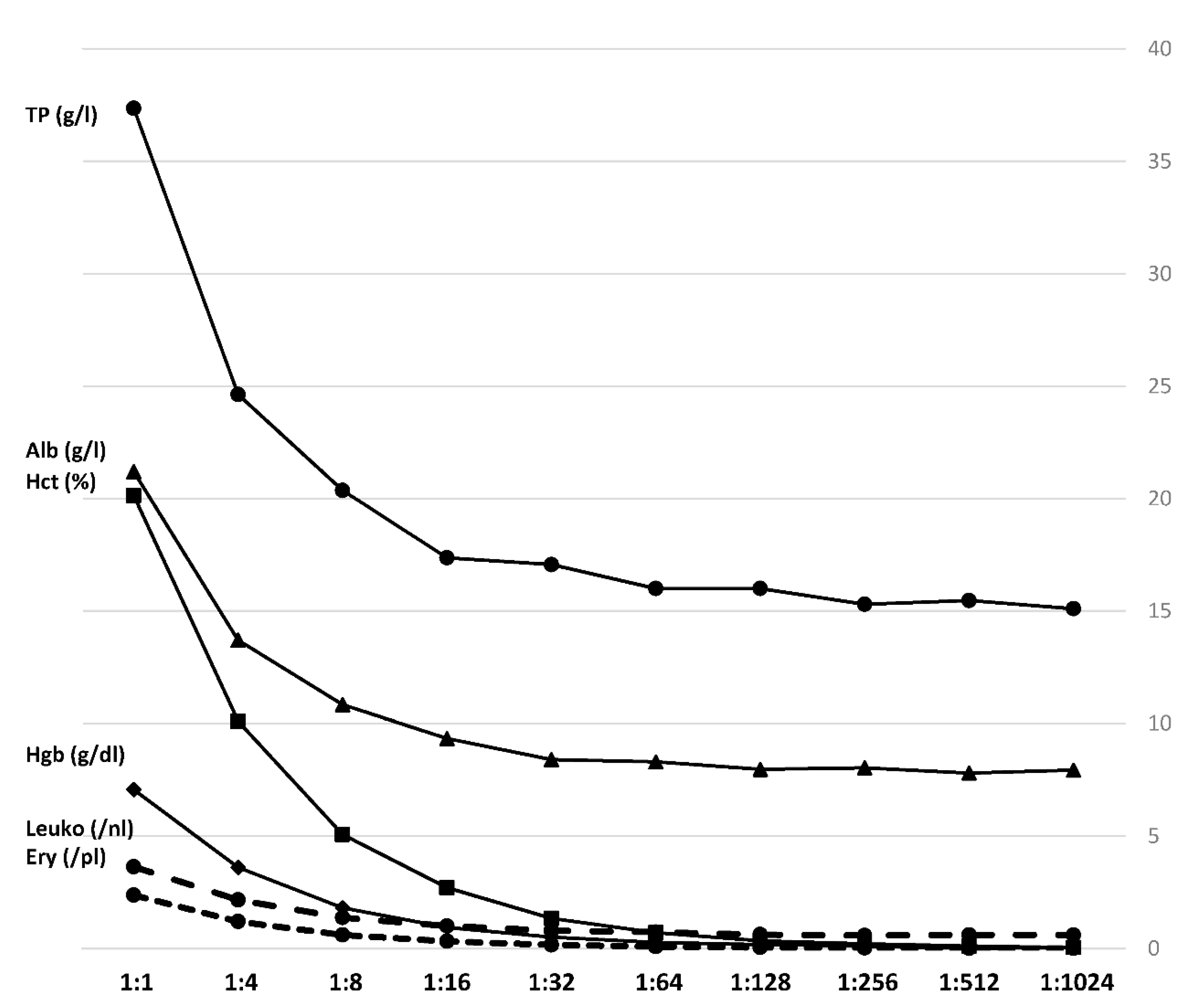
3.1. Laboratory-Chemical Analysis
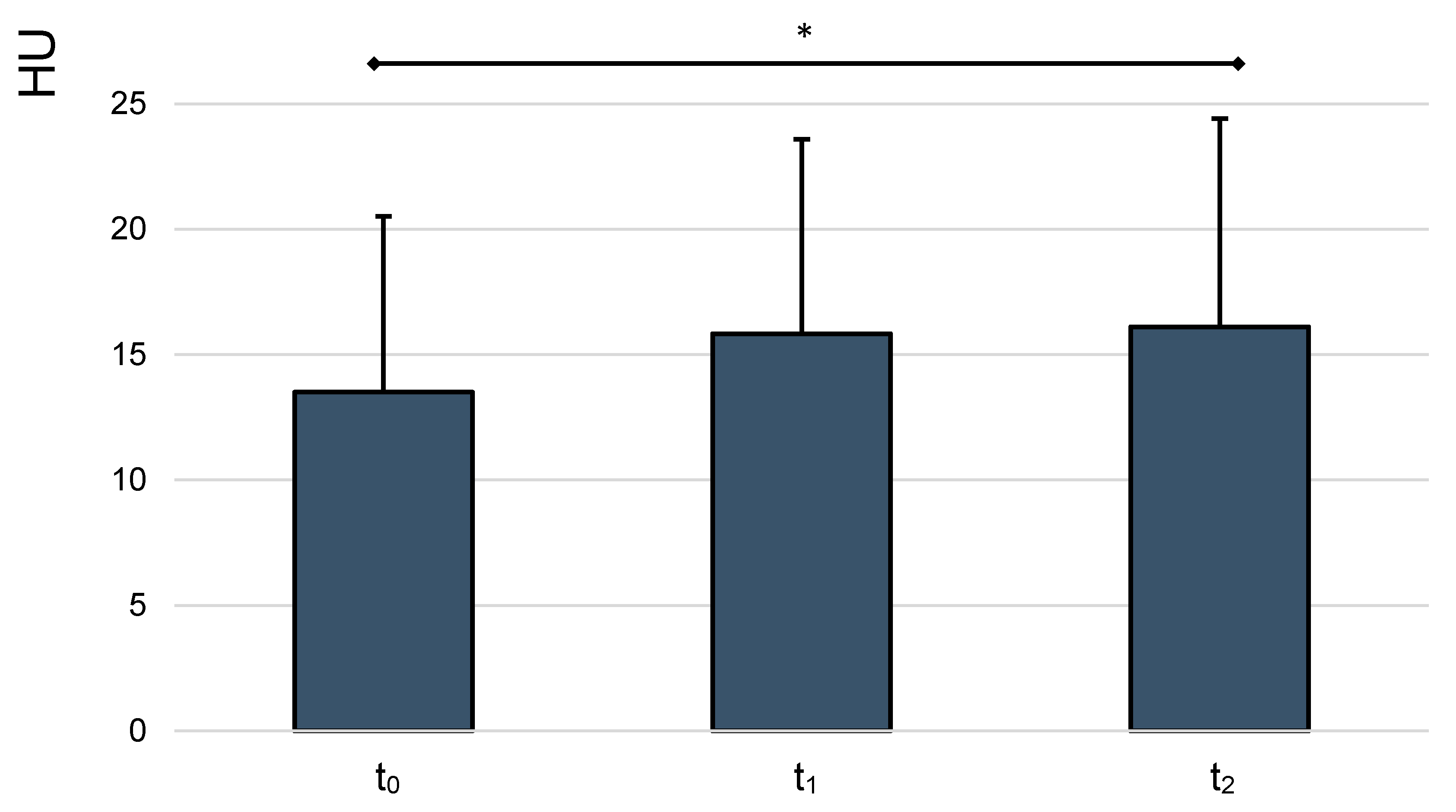
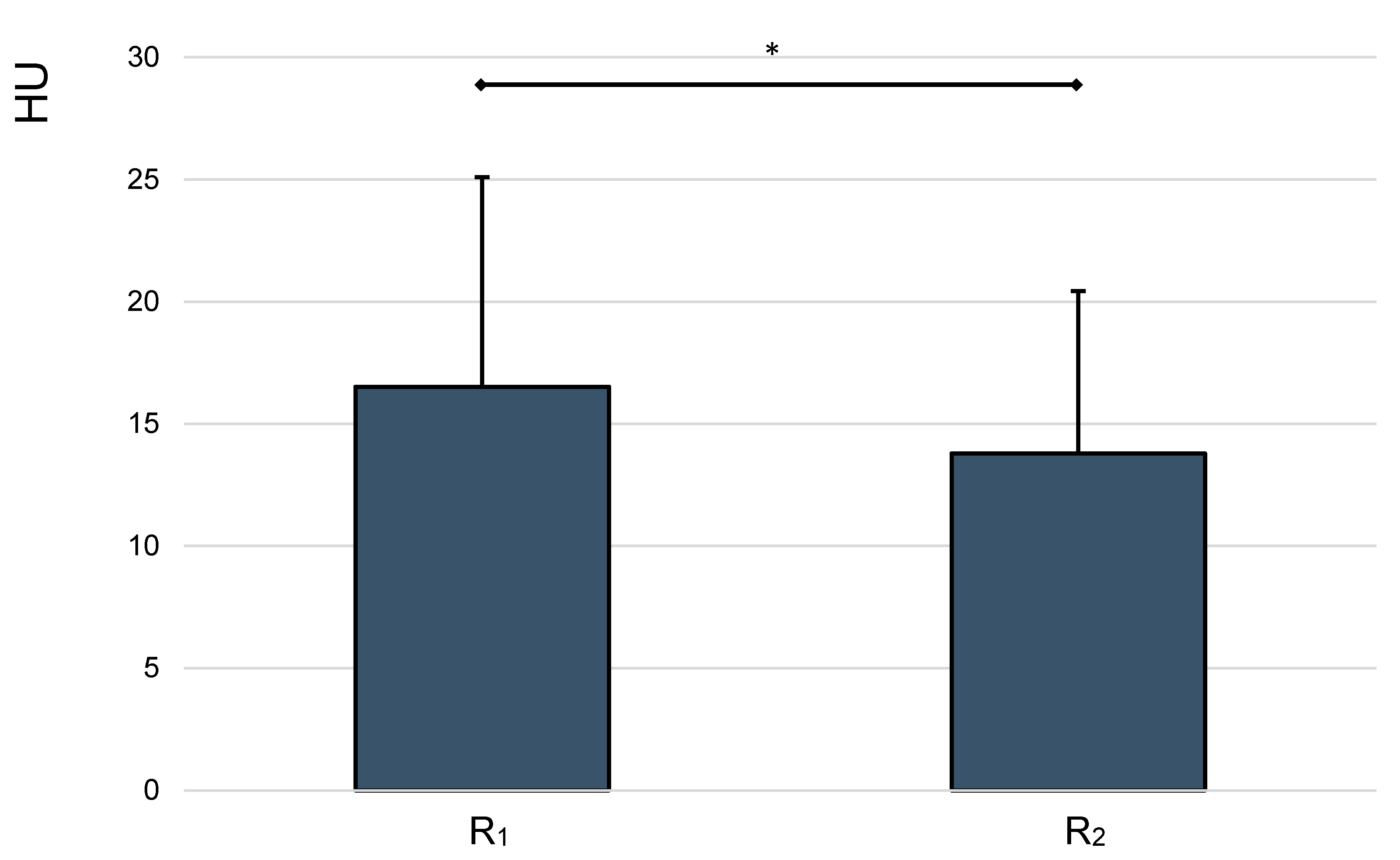
3.2. Radiological Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Costa, G.; Tierno, S.M.; Tomassini, F.; Venturini, L.; Frezza, B.; Cancrini, G.; Stella, F. The epidemiology and clinical evaluation of abdominal trauma. An analysis of a multidisciplinary trauma registry. Annali Italiani di Chirurgia 2010, 81, 95–102. [Google Scholar] [PubMed]
- Ferrah, N.; Cameron, P.; Gabbe, B.; Fitzgerald, M.; Martin, K.; Beck, B. Trends in the Nature and Management of Serious Abdominal Trauma. World J. Surg. 2019, 43, 1216–1225. [Google Scholar] [CrossRef] [PubMed]
- Huber-Wagner, S.; Lefering, R.; Kanz, K.-G.; Biberthaler, P.; Stengel, D. The importance of immediate total-body CT scanning. Lancet 2017, 389, 502–503. [Google Scholar] [CrossRef] [Green Version]
- S3–Leitlinie Polytrauma/Schwerverletzten-Behandlung. 2016. Available online: https://www.awmf.org/uploads/tx_szleitlinien/012-019l_S3_Polytrauma_Schwerverletzten-Behandlung_2017-08.pdf (accessed on 28 December 2020).
- Bydder, G.M.; Kreel, L. Attenuation values of fluid collections within the abdomen. J. Comput. Assist. Tomogr. 1980, 4, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Lucey, B.C.; Varghese, J.C.; Anderson, S.W.; Soto, J.A. Spontaneous hemoperitoneum: A bloody mess. Emerg. Radiol. 2007, 14, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R.A.; Chiro, G.D. Beam hardening in X-ray reconstructive tomography. Phys. Med. Biol. 1976, 21, 390. [Google Scholar] [CrossRef] [PubMed]
- Levine, C.D.; Patel, U.J.; Silverman, P.M.; Wachsberg, R.H. Low attenuation of acute traumatic hemoperitoneum on CT scans. Am. J. Roentgenol. 1996, 166, 1089–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Root, H.; Hauser, C.; McKinley, C.; Lafave, J.; Mendiola, R. Diagnostic peritoneal lavage. Surgery 1965, 57, 633–637. [Google Scholar] [PubMed]
- Liu, M.; Lee, C.H.; P’eng, F.K. Prospective comparison of diagnostic peritoneal lavage, computed tomographic scanning, and ultrasonography for the diagnosis of blunt abdominal trauma. J. Trauma 1993, 35, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Bain, I.M.; Kirby, R.M.; Tiwari, P.; McCaig, J.; Cook, A.L.; Oakley, P.A.; Templeton, J.; Braithwaite, M. Survey of abdominal ultrasound and diagnostic peritoneal lavage for suspected intra-abdominal injury following blunt trauma. Injury 1998, 29, 65–71. [Google Scholar] [CrossRef]
- MoReg, M. Student Course Manual ATLS® Advanced Trauma Life Support. Available online: https://www.academia.edu/36985888/Student_Course_Manual_ATLS_Advanced_Trauma_Life_Support (accessed on 24 October 2020).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hgb (g/dL) | Hct (%) | TP (g/L) | Alb (g/L) | Leuko (/nL) | Ery (/pL) | |
|---|---|---|---|---|---|---|
| Ascites | 0 | 0 | 15 | 7.8 | 0.5 | 0 |
| Blood 1 | 16.2 | 45.1 | 84.7 | 50.4 | 7.62 | 5.21 |
| Blood 2 | 12.8 | 37 | 72.5 | 29.7 | 7.4 | 4.45 |
| Blood 3 | 15.2 | 42.4 | 77.7 | 47.5 | 4.95 | 4.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerschbaum, M.; Schurr, L.A.; Riedl, M.; Mayr, A.; Weiß, I.; Klute, L.; Popp, D.; Pfeifer, C.; Ernstberger, A.; Alt, V.; et al. Clinical Value of CT for Differentiation between Ascites and Hemorrhage: An Experimental In-Vitro Study. J. Clin. Med. 2021, 10, 76. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010076
Kerschbaum M, Schurr LA, Riedl M, Mayr A, Weiß I, Klute L, Popp D, Pfeifer C, Ernstberger A, Alt V, et al. Clinical Value of CT for Differentiation between Ascites and Hemorrhage: An Experimental In-Vitro Study. Journal of Clinical Medicine. 2021; 10(1):76. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010076
Chicago/Turabian StyleKerschbaum, Maximilian, Leonhard Andreas Schurr, Moritz Riedl, Agnes Mayr, Isabella Weiß, Lisa Klute, Daniel Popp, Christian Pfeifer, Antonio Ernstberger, Volker Alt, and et al. 2021. "Clinical Value of CT for Differentiation between Ascites and Hemorrhage: An Experimental In-Vitro Study" Journal of Clinical Medicine 10, no. 1: 76. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010076