
Anti-Phosphatidylserine/Prothrombin Antibodies in Healthy Women with Unexplained Recurrent Pregnancy Loss

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Laboratory Studies
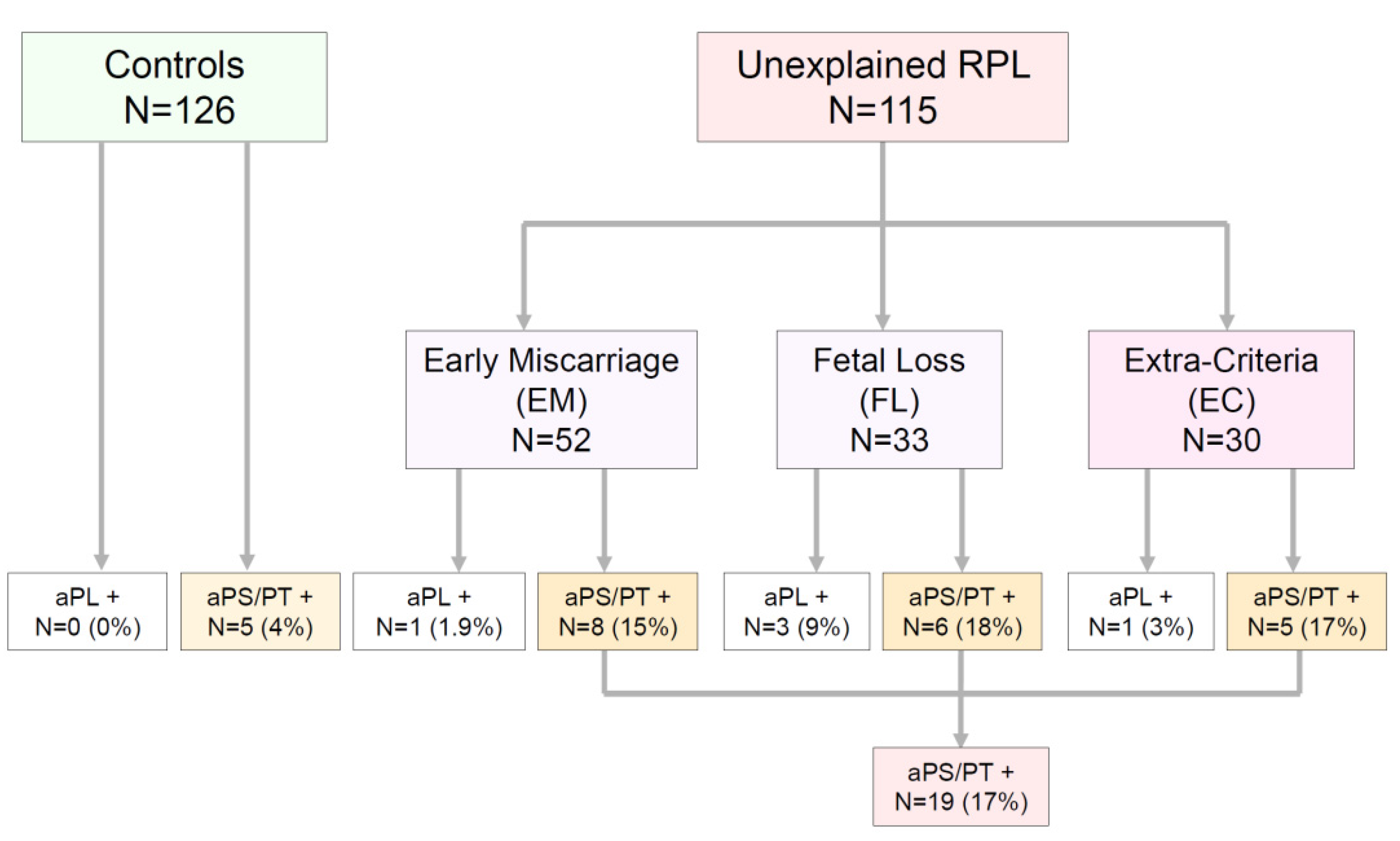
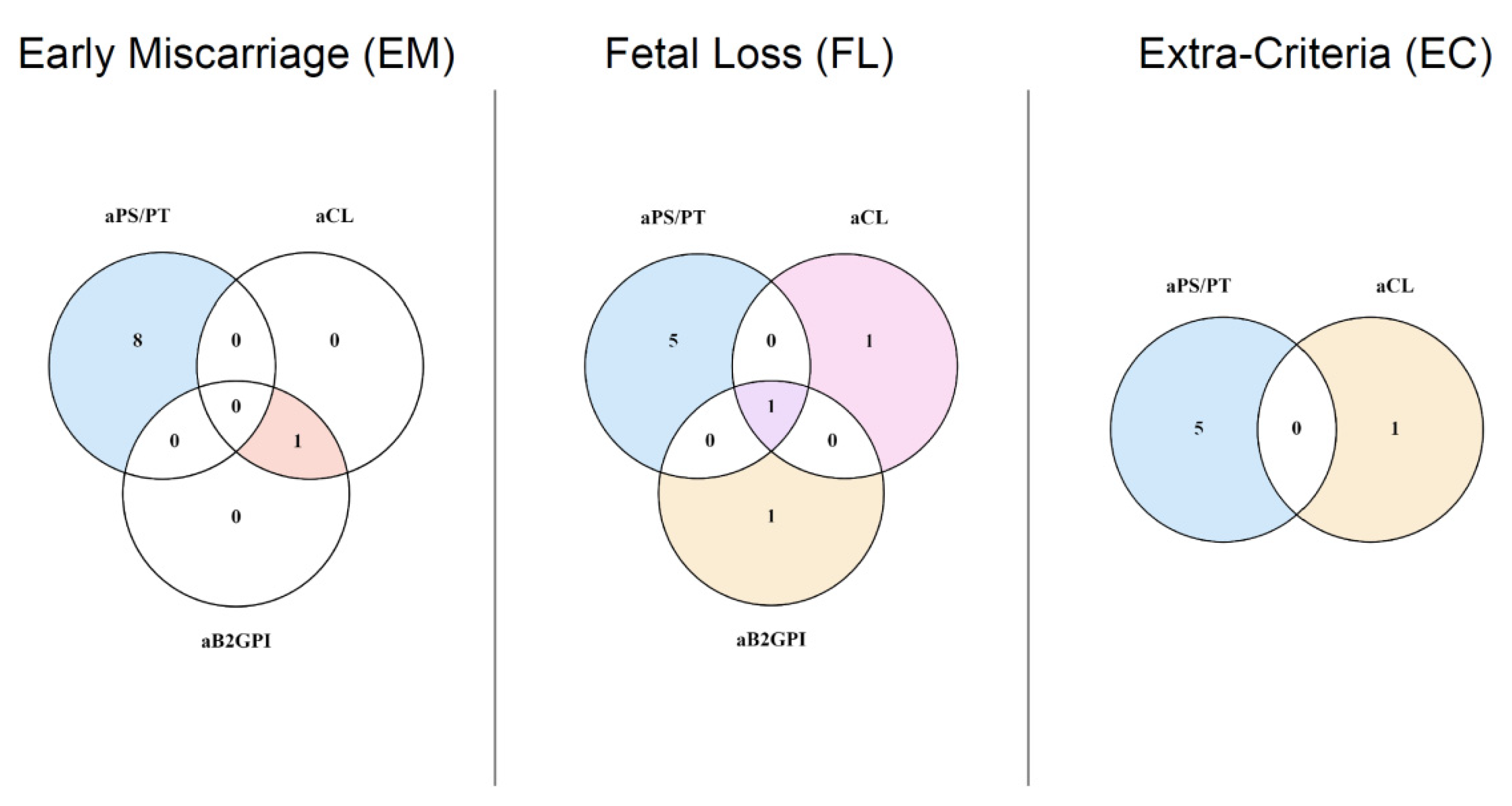
2.2. Patients and Groups
2.3. Follow-Up and Treatment
2.4. Ethics
2.5. Statistics
3. Results
3.1. Demographics
3.2. Levels and Prevalence of aPL in Patients and Controls
3.3. Univariate Analysis of aPS/PT Risk for RPL
3.4. Multivariate Analysis of aPS/PT and Criteria aPL Risk for RPL
3.5. Response to Treatment and Patient Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ford, H.B.; Schust, D.J. Recurrent pregnancy loss: Etiology, diagnosis, and therapy. Rev. Obstet. Gynecol. 2009, 2, 76–83. [Google Scholar] [PubMed]
- Vomstein, K.; Feil, K.; Strobel, L.; Aulitzky, A.; Hofer-Tollinger, S.; Kuon, R.J.; Toth, B. Immunological Risk Factors in Recurrent Pregnancy Loss: Guidelines Versus Current State of the Art. J. Clin. Med. 2021, 10, 869. [Google Scholar] [CrossRef]
- Hennessy, M.; Dennehy, R.; Meaney, S.; Devane, D.; O’Donoghue, K. A protocol for a systematic review of clinical practice guidelines for recurrent miscarriage. HRB Open Res. 2020, 3, 12. [Google Scholar] [CrossRef]
- WHO. Recommended definitions, terminology and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths. Modifications recommended by FIGO as amended October 14, 1976. Acta Obstet. Gynecol. Scand. 1977, 56, 247–253. [Google Scholar]
- RPL, E.G.G.o.; Bender Atik, R.; Christiansen, O.B.; Elson, J.; Kolte, A.M.; Lewis, S.; Middeldorp, S.; Nelen, W.; Peramo, B.; Quenby, S.; et al. ESHRE guideline: Recurrent pregnancy loss. Hum. Reprod Open 2018, 2018, hoy004. [Google Scholar]
- Rai, R.; Regan, L. Recurrent miscarriage. Lancet 2006, 368, 601–611. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: A committee opinion. Fertil. Steril. 2012, 98, 1103–1111. [Google Scholar] [CrossRef]
- Infertility Workup for the Women’s Health Specialist: ACOG Committee Opinion, Number 781. Obstet. Gynecol. 2019, 133, e377–e384. [CrossRef] [PubMed]
- Shetty, S.; Ghosh, K. Anti-phospholipid antibodies and other immunological causes of recurrent foetal loss—A review of literature of various therapeutic protocols. Am. J. Reprod. Immunol. 2009, 62, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Irastorza, G.; Crowther, M.; Branch, W.; Khamashta, M.A. Antiphospholipid syndrome. Lancet 2010, 376, 1498–1509. [Google Scholar] [CrossRef] [Green Version]
- Harris, E.N.; Gharavi, A.E.; Boey, M.L.; Patel, B.M.; Mackworth-Young, C.G.; Loizou, S.; Hughes, G.R. Anticardiolipin antibodies: Detection by radioimmunoassay and association with thrombosis in systemic lupus erythematosus. Lancet 1983, 2, 1211–1214. [Google Scholar] [CrossRef]
- Cervera, R.; Serrano, R.; Pons-Estel, G.J.; Ceberio-Hualde, L.; Shoenfeld, Y.; de Ramon, E.; Buonaiuto, V.; Jacobsen, S.; Zeher, M.M.; Tarr, T.; et al. Morbidity and mortality in the antiphospholipid syndrome during a 10-year period: A multicentre prospective study of 1000 patients. Ann. Rheum. Dis. 2015, 74, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Asherson, R.A. The catastrophic antiphospholipid syndrome, 1998. A review of the clinical features, possible pathogenesis and treatment. Lupus 1998, 7 (Suppl. 2), S55–S62. [Google Scholar] [CrossRef] [PubMed]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.; PG, D.E.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef]
- Gardiner, C.; Hills, J.; Machin, S.J.; Cohen, H. Diagnosis of antiphospholipid syndrome in routine clinical practice. Lupus 2013, 22, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Di Simone, N.; Meroni, P.L.; de Papa, N.; Raschi, E.; Caliandro, D.; De Carolis, C.S.; Khamashta, M.A.; Atsumi, T.; Hughes, G.R.; Balestrieri, G.; et al. Antiphospholipid antibodies affect trophoblast gonadotropin secretion and invasiveness by binding directly and through adhered beta2-glycoprotein I. Arthritis Rheum. 2000, 43, 140–150. [Google Scholar] [CrossRef] [Green Version]
- Di Simone, N.; Castellani, R.; Caliandro, D.; Caruso, A. Monoclonal anti-annexin V antibody inhibits trophoblast gonadotropin secretion and induces syncytiotrophoblast apoptosis. Biol. Reprod. 2001, 65, 1766–1770. [Google Scholar] [CrossRef] [Green Version]
- Atsumi, T.; Ieko, M.; Bertolaccini, M.L.; Ichikawa, K.; Tsutsumi, A.; Matsuura, E.; Koike, T. Association of autoantibodies against the phosphatidylserine-prothrombin complex with manifestations of the antiphospholipid syndrome and with the presence of lupus anticoagulant. Arthritis Rheum. 2000, 43, 1982–1993. [Google Scholar] [CrossRef]
- Sciascia, S.; Amigo, M.C.; Roccatello, D.; Khamashta, M. Diagnosing antiphospholipid syndrome: ‘extra-criteria’ manifestations and technical advances. Nat. Rev. Rheumatol. 2017, 13, 548–560. [Google Scholar] [CrossRef]
- Zigon, P.; Perdan Pirkmajer, K.; Tomsic, M.; Kveder, T.; Bozic, B.; Sodin Semrl, S.; Cucnik, S.; Ambrozic, A. Anti-Phosphatidylserine/Prothrombin Antibodies Are Associated with Adverse Pregnancy Outcomes. J. Immunol. Res. 2015, 2015, 975704. [Google Scholar] [CrossRef] [PubMed]
- Serrano, M.; Espinosa, G.; Lalueza, A.; Bravo-Gallego, L.Y.; Diaz-Simon, R.; Garcinuno, S.; Gil-Etayo, J.; Moises, J.; Naranjo, L.; Prieto-Gonzalez, S.; et al. Beta-2-Glycoprotein-I Deficiency Could Precipitate an Antiphospholipid Syndrome-like Prothrombotic Situation in Patients With Coronavirus Disease 2019. ACR Open Rheumatol. 2021, 3, 267–276. [Google Scholar] [CrossRef]
- Santos, T.D.S.; Ieque, A.L.; de Carvalho, H.C.; Sell, A.M.; Lonardoni, M.V.C.; Demarchi, I.G.; de Lima Neto, Q.A.; Teixeira, J.J.V. Antiphospholipid syndrome and recurrent miscarriage: A systematic review and meta-analysis. J. Reprod. Immunol. 2017, 123, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.A.; Laskin, C.A.; Spitzer, K.A. Anticardiolipin antibodies and recurrent early pregnancy loss: A century of equivocal evidence. Hum. Reprod. Update 2012, 18, 474–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branch, D.W. What’s new in obstetric antiphospholipid syndrome. Hematol. Am. Soc. Hematol. Educ. Program 2019, 2019, 421–425. [Google Scholar] [CrossRef]
- Rai, R.S.; Regan, L.; Clifford, K.; Pickering, W.; Dave, M.; Mackie, I.; McNally, T.; Cohen, H. Antiphospholipid antibodies and beta 2-glycoprotein-I in 500 women with recurrent miscarriage: Results of a comprehensive screening approach. Hum. Reprod. 1995, 10, 2001–2005. [Google Scholar] [CrossRef] [PubMed]
- Bertolaccini, M.L. Antibodies to prothrombin. Lupus 2012, 21, 729–731. [Google Scholar] [CrossRef]
- Serrano, A.; Cabrera-Marante, O.; Naranjo, L.; Diaz-Simon, R.; Pleguezuelo, D.E. Inclusion of anti-B2GPI-IgA and anti-Phosphatidylserine/Prothrombin in the classification criteria would double the diagnoses of APS. Lupus 2019, 28, 30. [Google Scholar]
- Pengo, V. Additional laboratory tests to improve on the diagnosis of antiphospholipid syndrome. J. Thromb. Haemost. 2020, 18, 1846–1848. [Google Scholar] [CrossRef]
- Bertolaccini, M.L.; Sciascia, S.; Murru, V.; Garcia-Fernandez, C.; Sanna, G.; Khamashta, M.A. Prevalence of antibodies to prothrombin in solid phase (aPT) and to phosphatidylserine-prothrombin complex (aPS/PT) in patients with and without lupus anticoagulant. Thromb. Haemost. 2013, 109, 207–213. [Google Scholar]
- Chinnaraj, M.; Planer, W.; Pengo, V.; Pozzi, N. Discovery and characterization of 2 novel subpopulations of aPS/PT antibodies in patients at high risk of thrombosis. Blood Adv. 2019, 3, 1738–1749. [Google Scholar] [CrossRef]
- Radin, M.; Foddai, S.G.; Cecchi, I.; Rubini, E.; Schreiber, K.; Roccatello, D.; Bertolaccini, M.L.; Sciascia, S. Antiphosphatidylserine/Prothrombin Antibodies: An Update on Their Association with Clinical Manifestations of Antiphospholipid Syndrome. Thromb. Haemost. 2020, 120, 592–598. [Google Scholar] [CrossRef]
- Mekinian, A.; Bourrienne, M.C.; Carbillon, L.; Benbara, A.; Noemie, A.; Chollet-Martin, S.; Tigaizin, A.; Montestruc, F.; Fain, O.; Nicaise-Roland, P. Non-conventional antiphospholipid antibodies in patients with clinical obstetrical APS: Prevalence and treatment efficacy in pregnancies. Semin. Arthritis Rheum. 2016, 46, 232–237. [Google Scholar] [CrossRef]
- Yonezawa, M.; Kuwabara, Y.; Ono, S.; Ouchi, N.; Ichikawa, T.; Takeshita, T. Significance of Anti-Phosphatidylethanolamine Antibodies in the Pathogenesis of Recurrent Pregnancy Loss. Reprod. Sci. 2020, 27, 1888–1893. [Google Scholar] [CrossRef]
- Abisror, N.; Nguyen, Y.; Marozio, L.; Esteve Valverde, E.; Udry, S.; Pleguezuelo, D.E.; Billoir, P.; Mayer-Pickel, K.; Urbanski, G.; Zigon, P.; et al. Obstetrical outcome and treatments in seronegative primary APS: Data from European retrospective study. RMD Open 2020, 6, e001340. [Google Scholar] [CrossRef]
- Hamulyak, E.N.; Scheres, L.J.; Marijnen, M.C.; Goddijn, M.; Middeldorp, S. Aspirin or heparin or both for improving pregnancy outcomes in women with persistent antiphospholipid antibodies and recurrent pregnancy loss. Cochrane Database Syst. Rev. 2020, 5, CD012852. [Google Scholar] [PubMed]
- Alijotas-Reig, J.; Esteve-Valverde, E.; Ferrer-Oliveras, R.; Saez-Comet, L.; Lefkou, E.; Mekinian, A.; Belizna, C.; Ruffatti, A.; Tincani, A.; Marozio, L.; et al. The European Registry on Obstetric Antiphospholipid Syndrome (EUROAPS): A survey of 1000 consecutive cases. Autoimmun. Rev. 2019, 18, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Skeith, L.; Carrier, M.; Kaaja, R.; Martinelli, I.; Petroff, D.; Schleussner, E.; Laskin, C.A.; Rodger, M.A. A meta-analysis of low-molecular-weight heparin to prevent pregnancy loss in women with inherited thrombophilia. Blood 2016, 127, 1650–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiber, K.; Radin, M.; Sciascia, S. Current insights in obstetric antiphospholipid syndrome. Curr. Opin. Obstet. Gynecol. 2017, 29, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Bouvier, S.; Cochery-Nouvellon, E.; Lavigne-Lissalde, G.; Mercier, E.; Marchetti, T.; Balducchi, J.P.; Mares, P.; Gris, J.C. Comparative incidence of pregnancy outcomes in treated obstetric antiphospholipid syndrome: The NOH-APS observational study. Blood 2014, 123, 404–413. [Google Scholar] [CrossRef]
- Albert, C.R.; Schlesinger, W.J.; Viall, C.A.; Mulla, M.J.; Brosens, J.J.; Chamley, L.W.; Abrahams, V.M. Effect of hydroxychloroquine on antiphospholipid antibody-induced changes in first trimester trophoblast function. Am. J. Reprod. Immunol. 2014, 71, 154–164. [Google Scholar] [CrossRef]
- Marchetti, T.; Ruffatti, A.; Wuillemin, C.; de Moerloose, P.; Cohen, M. Hydroxychloroquine restores trophoblast fusion affected by antiphospholipid antibodies. J. Thromb. Haemost. 2014, 12, 910–920. [Google Scholar] [CrossRef] [PubMed]
- Meroni, P.L. Prevention & treatment of obstetrical complications in APS: Is hydroxychloroquine the Holy Grail we are looking for? J. Autoimmun. 2016, 75, 1–5. [Google Scholar] [PubMed]
- Mekinian, A.; Lazzaroni, M.G.; Kuzenko, A.; Alijotas-Reig, J.; Ruffatti, A.; Levy, P.; Canti, V.; Bremme, K.; Bezanahary, H.; Bertero, T.; et al. The efficacy of hydroxychloroquine for obstetrical outcome in anti-phospholipid syndrome: Data from a European multicenter retrospective study. Autoimmun. Rev. 2015, 14, 498–502. [Google Scholar] [CrossRef] [PubMed]
- De Carolis, S.; Botta, A.; Salvi, S.; di Pasquo, E.; Del Sordo, G.; Garufi, C.; Lanzone, A.; De Carolis, M.P. Is there any role for the hydroxychloroquine (HCQ) in refractory obstetrical antiphospholipid syndrome (APS) treatment? Autoimmun. Rev. 2015, 14, 760–762. [Google Scholar] [CrossRef] [PubMed]
- Ruffatti, A.; Tonello, M.; Hoxha, A.; Sciascia, S.; Cuadrado, M.J.; Latino, J.O.; Udry, S.; Reshetnyak, T.; Costedoat-Chalumeau, N.; Morel, N.; et al. Effect of Additional Treatments Combined with Conventional Therapies in Pregnant Patients with High-Risk Antiphospholipid Syndrome: A Multicentre Study. Thromb. Haemost. 2018, 118, 639–646. [Google Scholar]
- Ruffatti, A.; Tonello, M.; Favaro, M.; Del Ross, T.; Calligaro, A.; Ruffatti, A.T.; Gervasi, M.T.; Hoxha, A. The efficacy and safety of second-line treatments of refractory and/or high risk pregnant antiphospholipid syndrome patients. A systematic literature review analyzing 313 pregnancies. Semin. Arthritis Rheum. 2021, 51, 28–35. [Google Scholar] [CrossRef]
- Latino, J.O.; Udry, S.; Aranda, F.; Wingeyer, S.P.; Romero, D.S.F.; Belizna, C.; Larranaga, G. Risk factors for early severe preeclampsia in obstetric antiphospholipid syndrome with conventional treatment. The impact of hydroxychloroquine. Lupus 2020, 29, 1736–1742. [Google Scholar] [CrossRef]
- Tian, Y.; Xu, J.; Chen, D.; Yang, C.; Peng, B. The additional use of hydroxychloroquine can improve the live birth rate in pregnant women with persistent positive antiphospholipid antibodies: A systematic review and meta-analysis. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102121. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CONTROLS (126) | EM (52) | FL (33) | EC (30) | All RPL (115) | |
|---|---|---|---|---|---|
| Age and cardiovascular risk factors | |||||
| Median age (IQR) | 36 (35–37) | 37 (34–39) | 36 (29.5–39) | 36 (33–38) | 37 (33–39) |
| Median BMI (IQR) | 27.1 (24.6–31.5) | 24.1 (21.5–27.5) | 25.6 (23.5–28.6) | 24.7 (20.8–27.3) | 24.4 (21.8–27.6) |
| Normal weight (%) | 50 (39.7%) | 39 (75%) | 18 (54.5%) | 19 (63.3%) | 76 (66.1%) |
| Overweight (%) | 50 (39.7%) | 7 (13.4%) | 11 (33%) | 10 (33.3%) | 28 (24.3%) |
| Obesity (%) | 26 (20.6%) | 6 (11.5%) | 4 (12.1%) | 1 (3.3%) | 11 (9.5%) |
| Smoke (%) | 13 (10.3%) | 3 (5.7%) | 2 (6%) | 1 (3.3%) | 6 (5.2%) |
| Alcoholism (%) | 4 (3.1%) | 1 (1.9%) | 0 (0%) | 0 (0%) | 1 (0.8%) |
| Ethnicity: | |||||
| African | 3 (2.3%) | 0 (0%) | 2 (6%) | 0 (0%) | 2 (1.7%) |
| Arabic | 9 (7.1%) | 3 (5.7%) | 2 (6%) | 0 (0%) | 5 (4.3%) |
| Chinese | 11 (8.7%) | 2 (3.8%) | 1 (3%) | 0 (0%) | 3 (2.6%) |
| Caucasic | 61 (48.4%) | 41 (78.8%) | 20 (60.6%) | 27 (90%) | 88 (76.5%) |
| Indian | 2 (1.5%) | 1 (1.9%) | 1 (3%) | 0 (0%) | 2 (1.7%) |
| Hispanic | 35 (27.7%) | 5 (9.6%) | 7 (21.2%) | 3 (10%) | 15 (13%) |
| Romani | 5 (3.9%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Treatments: | |||||
| No previous treatment | - | 50 (96.1%) | 33 (100%) | 27 (90%) | 110 (95.6%) |
| ASA | - | 2 (3.9%) | 0 (0%) | 3 (10%) | 5 (4.4%) |
| LMWH | - | 2 (3.9%) | 0 (0%) | 3 (10%) | 5 (4.4%) |
| HCQ | - | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| aPL Levels (U/mL) | Median (IQR) | ||||
| aCL IgG | 1.9 (1.9–1.9) | 1.6 (1.6–1.6) | 1.6 (1.6–1.6) | 1.6 (1.6–1.6) | 1.6 (1.6–1.6) |
| aCL IgM | 1.9 (1.9–1.9) | 1.4 (0.4–2) | 0.7 (0.2–2.7) | 1.4 (0.6–2.6) | 0.9 (0.4–2.2) |
| aB2GPI IgG | 1.9 (1.9–1.9) | 1.4 (1.4–1.7) | 1.4 (1.4–1.4) | 1.4 (1.4–1.4) | 1.4 (1.4–1.4) |
| aB2GPI IgM | 1.9 (1.9–1.9) | 1.4 (0.7–2.6) | 0.8 (0.4–2.3) | 1.4 (0.5–1.6) | 1.4 (0.5–2.1) |
| aPS/PT IgG | 7.4 (5.8–11.6) | 7.5 (6.7–12.7) | 7.4 (5.9–9.2) | 10.7 (6.7–17.6) | 7.8 (6.5–13) |
| aPS/PT IgM | 12.3 (9.1–17.2) | 19.1 (11.2–30.4) | 16.4 (10.2–20.4) | 14.8 (10.8–20.3) | 17 (10.8–25.4) |
| aPL Prevalence | N (%) | ||||
| LA | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Any criteria aPL | 0 (0%) | 2 (4%) | 3 (9%) | 1 (3%) | 5 (4.3%) |
| Any aPS/PT | 5 (3.9%) | 8 (15%) | 6 (18.1%) | 5 (17%) | 19 (17%) |
| aPS/PT IgG | 2 (1.6%) | 4 (7.7%) | 0 (0%) | 4 (13.3%) | 8 (6.9%) |
| aPS/PT IgM | 3 (2.4%) | 4 (7.7%) | 6 (18.1%) | 1 (3.3%) | 11 (9.5%) |
| Early Miscarriage (EM) Group | Fetal Loss (FL) Group | Early Miscarriage (EM) Group | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value |
| Obesity | 0.54 | 0.24–1.21 | 0.135 | 0.69 | 0.27–1.79 | 0.456 | 0.17 | 0.03–0.78 | 0.022 |
| Smoking | 0.45 | 0.11–1.80 | 0.264 | 0.46 | 0.08–2.37 | 0.355 | 0.30 | 0.03–2.60 | 0.275 |
| aPS/PT | 4.44 | 1.34–14.70 | 0.014 | 5.68 | 1.54–20.88 | 0.008 | 4.51 | 1.14–17.73 | 0.031 |
| Patient No | aPS/PT IgG | aPS/PT IgM | aCL IgG | aCL IgM | aB2GPI IgG | aB2GPI IgM | LA—dRVVT Ratio | LA—SCT Ratio | ANA | ANTI-DNA | Age | P | M | PW of PL before Treatment | Treatment | LMWH | ASA | HCQ | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EM1 | 30.6 | 12.2 | 1.6 | 0.2 | 1.4 | 0.9 | 1.03 | 0.98 | N | N | 34 | 4 | 3 | 6, 9, 6 | Yes | Yes | Yes | Yes | Pregnancy and HN |
| EM2 | 47.3 | 23.3 | 1.6 | 4.1 | 1.5 | 5 | 0.99 | 1.08 | N | N | 40 | 4 | 3 | 6, 6, 8 | Yes | Yes | Yes | No | Pregnancy and HN |
| EM3 | 42.1 | 15.2 | 1.6 | 0.7 | 1.4 | 0.6 | 1.14 | 1.17 | N | N | 39 | 5 | 4 | VIP, 6, 5, 5, 6 | Yes | Yes | Yes | No | Pregnancy and HN |
| EM4 | 13.5 | 40 | 1.6 | 0.2 | 2.18 | 1.4 | 0.84 | 1 | N | N | 35 | 4 | 4 | 9, 7, 9 | |||||
| EM5 | 6.64 | 48 | 1.6 | 1.5 | 1.4 | 2.7 | 0.81 | 1.16 | N | N | 31 | 3 | 3 | 6, 8, 7 | |||||
| EM6 | 33.2 | 23.4 | 1.6 | 5.8 | 1.4 | 5.6 | 0.96 | 1 | N | N | 39 | 4 | 4 | 8, 8, 6, 7 | |||||
| EM7 | 12.5 | 59.5 | 1.6 | 0.2 | 1.4 | 0.3 | 0.98 | 0.94 | N | N | 40 | 4 | 3 | Delivery, 6, 8, 9, 5 | |||||
| EM8 | 6.06 | 42.5 | 1.6 | 2.4 | 1.4 | 2.8 | 0.95 | 0.93 | N | N | 4 | 4 | 6, 6, 9, 8 | ||||||
| EM9 | 8.05 | 38.2 | 14.5 | 52.4 | 12.6 | 56 | 1.03 | 1.09 | N | N | 35 | 6 | 6 | 6 PL < PW10 | Yes | Yes | Yes | Yes | Miscarriage at PW 8 |
| FL1 | 21.8 | 57.7 | 9.6 | 7.8 | 8.5 | 6.8 | 1.02 | 0.95 | N | N | 38 | 4 | 2 | 11, 13, 30 | Yes | Yes | Yes | No | Pregnancy and HN |
| FL2 | 7.87 | 53.3 | 1.6 | 2.5 | 1.4 | 2.2 | 0.85 | 0.82 | N | N | 33 | 2 | 2 | 20, 40 | Yes | Yes | Yes | No | Pregnancy and HN |
| FL3 | 11.3 | 71.6 | 1.6 | 0.5 | 1.4 | 0.5 | 1.13 | 1.27 | N | N | 31 | 5 | 4 | 12, 11, 12, 12 | |||||
| FL4 | 21.6 | 64.3 | 73.7 | 22.2 | 87.7 | 23.2 | 1.05 | 1.26 | N | N | 41 | 3 | 3 | 18, 18, 18 | |||||
| FL5 | 7.1 | 65.1 | 1.6 | 1.5 | 1.4 | 3.1 | 1.05 | 1.17 | N | N | 30 | 2 | 1 | 29 (Placental thrombi) | |||||
| FL6 | 7.47 | 74.8 | 1.6 | 8.6 | 1.4 | 8.6 | 0.99 | 1.13 | N | N | 38 | 5 | 3 | 12, 18, 15 | |||||
| FL7 | 19 | 8.57 | 2.1 | 4.9 | 29.3 | 1.4 | 0.96 | 0.82 | N | N | 40 | 3 | 3 | 11, 11, 14 | Yes | Yes | No | No | Pregnancy and HN |
| FL8 | 5.25 | 8.59 | 3.1 | 23.6 | 1.4 | 1.6 | 1 | 1.09 | N | N | 25 | 3 | 1 | VIP, 16 | Yes | Yes | No | No | Pregnancy and HN |
| EC1 | 40.1 | 20.3 | 1.6 | 0.2 | 1.4 | 0.2 | 0.87 | 0.96 | N | N | 32 | 2 | 2 | 7, 5 | Yes | Yes | Yes | No | Pregnancy and HN |
| EC2 | 45.2 | 11.6 | 1.6 | 2 | 1.4 | 1.9 | 1.06 | 0.97 | N | N | 44 | 2 | 2 | 8, 6 | Yes | Yes | Yes | Yes | Pregnancy and HN |
| EC3 | 53.5 | 33.8 | 1.6 | 1.6 | 1.4 | 2.5 | 1 | 1.1 | N | N | 38 | 2 | 2 | 8, 5 | Yes | Yes | Yes | Yes | Pregnancy and HN |
| EC4 | 5.87 | 52.7 | 1.6 | 0.6 | 1.4 | 0.5 | 0.89 | 1.17 | N | N | 35 | 2 | 2 | 9, 6 | |||||
| EC5 | 206 | 10.8 | 1.6 | 1.8 | 3.07 | 1.4 | 0.95 | 1.23 | N | N | 43 | 2 | 2 | 7, 8 | |||||
| EC6 | 9.05 | 9.47 | 2.5 | 47.1 | 1.4 | 6.8 | 0.97 | 1.19 | N | N | 34 | 4 | 2 | 2 Deliveries, 9, 6 | Yes | Yes | Yes | No | Pregnancy and HN |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pleguezuelo, D.E.; Cabrera-Marante, O.; Abad, M.; Rodriguez-Frias, E.A.; Naranjo, L.; Vazquez, A.; Villar, O.; Gil-Etayo, F.J.; Serrano, M.; Perez-Rivilla, A.; et al. Anti-Phosphatidylserine/Prothrombin Antibodies in Healthy Women with Unexplained Recurrent Pregnancy Loss. J. Clin. Med. 2021, 10, 2094. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102094
Pleguezuelo DE, Cabrera-Marante O, Abad M, Rodriguez-Frias EA, Naranjo L, Vazquez A, Villar O, Gil-Etayo FJ, Serrano M, Perez-Rivilla A, et al. Anti-Phosphatidylserine/Prothrombin Antibodies in Healthy Women with Unexplained Recurrent Pregnancy Loss. Journal of Clinical Medicine. 2021; 10(10):2094. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102094
Chicago/Turabian StylePleguezuelo, Daniel E., Oscar Cabrera-Marante, Magdalena Abad, Edgard Alfonso Rodriguez-Frias, Laura Naranjo, Alicia Vazquez, Olga Villar, Francisco Javier Gil-Etayo, Manuel Serrano, Alfredo Perez-Rivilla, and et al. 2021. "Anti-Phosphatidylserine/Prothrombin Antibodies in Healthy Women with Unexplained Recurrent Pregnancy Loss" Journal of Clinical Medicine 10, no. 10: 2094. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102094