
Effectiveness of Topical Anesthetics in Pain Management for Dermal Injuries: A Systematic Review

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methodology
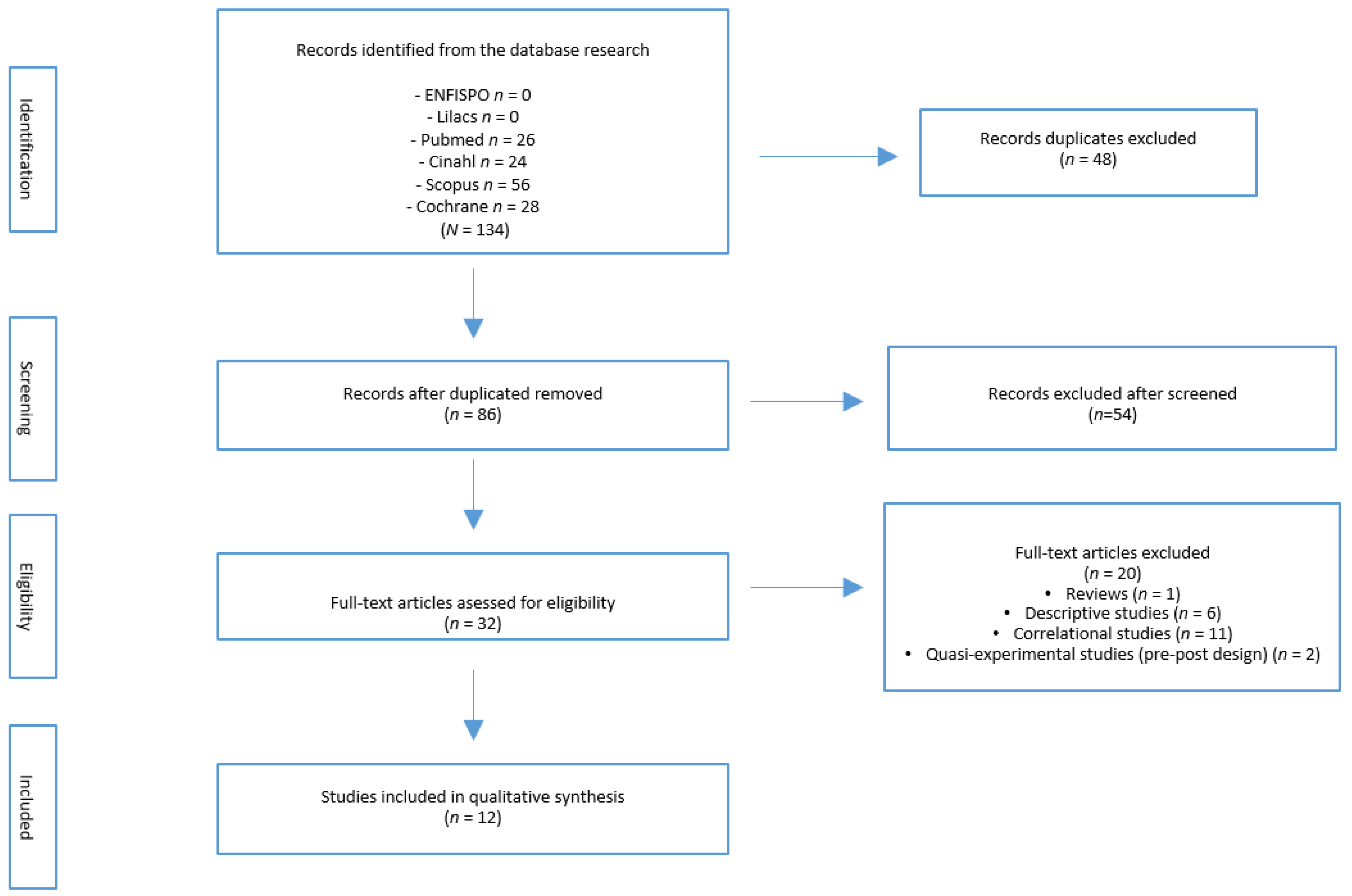
2.1. Search Strategy
2.2. Study Selection Criteria
2.3. Study Variables/Outcomes
2.4. Data Extraction
3. Results
3.1. Selection of Studies and Evaluation of Methodological Quality
3.2. Sociodemographic and Clinical Characteristics of the Population
3.3. Characteristics of the Intervention
3.4. Main Variable: Pain
3.5. Secondary Variable: Adverse Effects
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brennan, F.; Carr, D.B.; Cousins, M. Pain management: A fundamental human right. Anesth. Analg. 2007, 105, 205–221. Available online: https://journals.lww.com/anesthesia-analgesia/fulltext/2007/07000/pain_management__a_fundamental_human_right.37.aspx (accessed on 2 July 2019). [CrossRef] [Green Version]
- Trott, A.T. Heridas Y Cortes: Tratamiento Y Sutura De Urgencia; Elsevier: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Steele, K. Topical treatments for acute and chronic wound pain. J. Palliat. Med. 2017, 20, 560–561. Available online: http://online.liebertpub.com/doi/10.1089/jpm.2017.0010 (accessed on 9 November 2017). [CrossRef]
- Tuero, J.H.G.; Ramírez, R.R.; Pineda, M.M.; Quiala, M.J.G.; Salazar, J.C. Heridas: Métodos de tratamiento. Medisan 2004, 8, 33–42. [Google Scholar]
- Becker, D.E.; Reed, K.L. Essentials of local anesthetic pharmacology. Anesth Prog. 2006, 53, 98–109. [Google Scholar] [CrossRef]
- McNulty, R.; Handley, T.; Devlin, M. Reducing the need for general anaesthesia in children: Use of LAT gel in treating facial lacerations. Br. J. Oral Maxillofac. Surg. 2013, 51, e130-1. Available online: http://0-linkinghub-elsevier-com.brum.beds.ac.uk/retrieve/pii/S0266435612003907 (accessed on 13 June 2015). [CrossRef] [PubMed]
- Bonadio, W.A.; Wagner, V. Efficacy of TAC topical anesthetic for repair of pediatric lacerations. Arch. Pediatr. Adolesc. Med. 1988, 142, 203–205. [Google Scholar] [CrossRef]
- Ernst, A.A.; Marvez-Valls, E.; Nick, T.G.; Weiss, S.J. LAT (lidocaine-adrenaline-tetracaine) versus TAC (tetracaine-adrenaline-cocaine) for topical anesthesia in face and scalp lacerations. Am. J. Emerg. Med. 1995, 13, 151–154. [Google Scholar] [CrossRef]
- Rodríguez, E.O.; Aller, C.G.; Cortina, L.M.; Quiroga, P.S. Suturas y Cirugía Menor para Profesionales de Enfermería. 2a; Editorial Médica Panamericana: Madrid, Spain, 2007. [Google Scholar]
- Achar, S.; Kundu, S. Principles of office anesthesia: Part I. Infiltrative anesthesia. Am. Fam. Phys. 2002, 66, 91–95. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Reprint-preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Phys. Ther. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef]
- Bijur, P.E.; Latimer, C.T.; Gallagher, E.J. Validation of a verbally administered numerical rating scale of acute pain for use in the emergency department. Acad. Emerg. Med. 2003, 10, 390–392. [Google Scholar] [CrossRef]
- Garra, G.; Singer, A.J.; Taira, B.R.; Chohan, J.; Cardoz, H.; Chisena, E.; Thode, H.C., Jr. Validation of the wong-baker FACES pain rating scale in pediatric emergency department patients. Acad. Emerg. Med. 2010, 17, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The Validation of Visual Analogue Scales as Ratio Scale Measures for Chronic and Experimental Pain; Elsevier: Amsterdam, The Netherlands, 1983; Volume 17, pp. 45–56. [Google Scholar]
- Tomlinson, D.; von Baeyer, C.L.; Stinson, J.N.; Sung, L. A systematic review of faces scales for the self-report of pain intensity in children. Pediatrics 2010, 126, 1168–1198. [Google Scholar] [CrossRef] [Green Version]
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.C.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to assess the quality of randomized controlled trials: A systematic review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbas, A.M.; Hafiz, H.A.A.; Abdelhafez, A.M.; Michael, A.; Ismail, A.M. Topical lidocaine-prilocaine cream versus lidocaine infiltration for pain relief during repair of perineal tears after vaginal delivery: Randomized clinical trial. J. Matern. Neonatal Med. 2019, 32, 2182–2187. Available online: https://0-www-tandfonline-com.brum.beds.ac.uk/doi/full/10.1080/14767058.2018.1428304 (accessed on 24 October 2019). [CrossRef] [PubMed]
- Christensen, T.J.; Thorum, T.; Kubiak, E.N. Lidocaine analgesia for removal of wound vacuum-assisted closure dressings: A randomized double-blinded placebo-controlled trial. J. Orthop. Trauma 2013, 27, 107–112. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/23343829 (accessed on 9 November 2017). [CrossRef] [PubMed]
- Tseng, T.-H.; Jiang, C.-C.; Fu, S.-H.; Lee, T.-L.; Chuang, Y.-H.; Chiang, H. Topical anesthesia for staple removal from surgical wounds on the knee: A prospective, double-blind, randomized trial. J. Surg. Res. 2017, 215, 167–172. Available online: http://0-linkinghub-elsevier-com.brum.beds.ac.uk/retrieve/pii/S0022480417301889 (accessed on 9 November 2017). [CrossRef]
- Waldman, N.; Densie, I.K.; Herbison, P. Topical tetracaine used for 24 h is safe and rated highly effective by patients for the treatment of pain caused by corneal abrasions: A double-blind, randomized clinical trial. Acad. Emerg. Med. 2014, 21, 374–382. [Google Scholar] [CrossRef]
- Claeys, A.; Gaudy-Marqueste, C.; Pauly, V.; Pelletier, F.; Truchetet, F.; Boye, T.; Aubin, F.; Schmutz, J.L.; Grob, J.J.; Richard, M.A. Management of pain associated with debridement of leg ulcers: A randomized, multicentre, pilot study comparing nitrous oxide-oxygen mixture inhalation and lidocaine-prilocaine cream. J. Eur. Acad. Dermatol. Venerol. 2011, 25, 138–144. [Google Scholar] [CrossRef]
- Descroix, V.; Coudert, A.E.; Vigé, A.; Durand, J.-P.; Toupenay, S.; Molla, M.; Pompignoli, M.; Missika, P.; Allaert, F.-A. Efficacy of topical 1% lidocaine in the symptomatic treatment of pain associated with oral mucosal trauma or minor oral aphthous ulcer: A randomized, double-blind, placebo-controlled, parallel-group, single-dose study. J. Orofac. Pain 2011, 25, 327–332. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/22247928 (accessed on 24 October 2019).
- Franchi, M.; Cromi, A.; Scarperi, S.; Gaudino, F.; Siesto, G.; Ghezzi, F. Comparison between lidocaine-prilocaine cream (EMLA) and mepivacaine infiltration for pain relief during perineal repair after childbirth: A randomized trial. Am. J. Obstet. Gynecol. 2009, 201, 186.e1–186.e5. Available online: http://0-linkinghub-elsevier-com.brum.beds.ac.uk/retrieve/pii/S0002937809004098 (accessed on 9 November 2017). [CrossRef]
- Gaufberg, S.V.; Walta, M.J.; Workman, T.P. Expanding the use of topical anesthesia in wound management: Sequential layered application of topical lidocaine with epinephrine. Am. J. Emerg. Med. 2007, 25, 379–384. Available online: http://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/S0735675706003639 (accessed on 13 June 2015). [CrossRef]
- Harman, S.; Zemek, R.; Duncan, M.J.; Ying, Y.; Petrcich, W. Efficacy of pain control with topical lidocaine-epinephrine-tetracaine during laceration repair with tissue adhesive in children: A randomized controlled trial. Can. Med. Assoc. J. 2013, 185, E629–E634. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, M. Working with industry. In A Non-Inferiority Study of the Clinical-Effectiveness of Anaesthesia Obtained Via Application of Topical Anaesthetic Gel Compared to Infiltration of Lidocaine for the Treatment of Lacerations in the Emergency Department; SB Communications Group: London, UK, 2010; Volume 7, p. 2. [Google Scholar]
- Kargi, E.; Tekerekoğlu, B. Usage of lidocaine-prilocaine cream in the treatment of postburn pain in pediatric patients. Ulus Travma Acil Cerrahi Derg. 2010, 16, 229–232. [Google Scholar]
- Kasaj, A.; Heib, A.; Willershausen, B. Effectiveness of a topical salve (Dynexan®) on pain sensitivity and early wound healing following nonsurgical periodontal therapy. Eur. J. Med. Res. 2007, 12, 196–199. [Google Scholar]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Stern, I.; Giddon, D.B. Topical anesthesia for periodontal procedures. Anesth. Prog. 1975, 22, 105–108. [Google Scholar] [PubMed]
- Wang, B.; Hill, V.K.P.; Wilson, M.H.; Felstead, A.M. LAT gel, a powerful tool underused in the repair of paediatric lacerations. Int. J. Oral Maxillofac. Surg. 2014, 43, 955–956. [Google Scholar] [CrossRef] [PubMed]
- Desai, C.; Wood, F.M.; Schung, S.A.; Parsons, R.W.; Fridlender, C.; Sunderland, V.B. Effectiveness of a topical local anaesthetic spray as analgesia for dressing changes: A double-blinded randomised pilot trial comparing an emulsion with an aqueous lidocaine formulation. Burns 2014, 40, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Patterson, G.M.C. Regional Anesthesia, 2nd ed.; Adams, A.P., Hewitt, P.B., Grande, C.M., Eds.; Edward Arnold Publishers Limited: London, UK, 1998; pp. 289–306. [Google Scholar]
- Chale, S.; Singer, A.J.; Marchini, S.; McBride, M.J.; Kennedy, D. Digital versus local anesthesia for finger lacerations: A randomized controlled trial. Acad. Emerg. Med. 2006, 13, 1046–1050. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/16973640 (accessed on 9 November 2017). [CrossRef] [PubMed]
- Rui, W.; Long, G.; Li, G.; Yang, Y.; Hengjin, L.; Zhenhu, W. Effects of ethyl chloride spray on early recovery after total knee arthroplasty: A prospective study. J. Orthop. Sci. 2017, 22, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Kundu, S.; Achar, S. Principles of office anesthesia: Part II. Topical anesthesia. Am. Fam. Physician 2002, 66, 99–102. [Google Scholar] [PubMed]
- Blount, R.L.; Piira, T.; Cohen, L.L.; Cheng, P.S. Pediatric procedural pain. Behav. Modif. 2006, 30, 24–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors & Year | Was the Study Described as Randomized? | Was the Method of Randomization Appropriate? | Was the Study Described as Blinded? | Was the Method of Blinding Appropriate? | Was there a Description of Withdrawals and Dropouts? | Total |
|---|---|---|---|---|---|---|
| Abbas et al., 2019 [17] | 1 | 1 | 0 | 0 | 0 | 2 |
| Christensen et al., 2013 [18] | 1 | 0 | 1 | 0 | 0 | 2 |
| Claeys et al., 2010 [21] | 1 | 1 | 0 | 0 | 0 | 2 |
| Descroix et al., 2011 [22] | 1 | 1 | 1 | 1 | 0 | 4 |
| Franchi et al., 2009 [23] | 1 | 0 | 0 | 0 | 0 | 1 |
| Gaufberg et al., 2006 [24] | 1 | 0 | 0 | 0 | 0 | 1 |
| Harman et al., 2013 [25] | 1 | 1 | 1 | 0 | 0 | 3 |
| Jenkins, 2010 [26] | 1 | 1 | 0 | 0 | 0 | 2 |
| Kargi et al., 2010 [27] | 1 | 0 | 0 | 0 | 0 | 1 |
| Kasaj et al., 2007 [28] | 1 | 0 | 1 | 0 | 0 | 2 |
| Tseng et al., 2017 [19] | 1 | 0 | 1 | 0 | 0 | 2 |
| Waldman et al., 2014 [20] | 1 | 1 | 1 | 1 | 0 | 4 |
| Author and Year | Sample Size EG/CG | Intervention | Wound or Injury | Intervention | Outcomes | ||
|---|---|---|---|---|---|---|---|
| Primary | Secondary | ||||||
| Intervention 1 (EG) | Intervention 2 (CG) | Pain | Adverse Effects | ||||
| Abbas et al., 2019 [17] | n = 14 | Suture | Perineal tears | Lidocaine (25 mg/g) with prilocaine (25 mg/g) | mepivacaine infiltrated | Pain (VAS) | Evaluate |
| 72/72 | |||||||
| Christensen et al., 2013 [18] | n = 11 | Removal of wound Vacuum-Assisted Clousure dressing (VAC) | Venous leg ulcers | Lidocaine 1% | Normal saline | Pain (VAS) | Evaluate |
| 11/11 | |||||||
| Claeys et al., 2010 [21] | n = 41 | Debridement | Chronic arterial and venous leg ulcers | Lidocaine (25 mg/g) with prilocaine (25 mg/g) | Nitrous oxide oxygen mixture inhalated 9−12 L/min (max. 30 min) | Pain (VAS) | No Evaluate |
| 20/21 | Verbal Rating Scale (VRS) | ||||||
| Descroix et al., 2011 [22] | n = 59 | wound management | Oral mucosal trauma or oral aphthous ulcer | Lidocaína crema 1% Dosis 0.2 g | placebo cream | Pain (VAS) | No Evaluate |
| 29/30 | |||||||
| Franchi et al., 2009 [23] | n = 61 | Suture | Perineal tears | Lidocaine (25 mg/g) with prilocaine (25 mg/g) | mepivacaine infiltrated | Pain (VAS) | No Evaluate |
| 31/30 | |||||||
| Gaufberg et al., 2006 [24] | n = 100 | wound management | Wounds | Topical lidocaine 5% with epinephrine 0.025% | lidocaine infiltrated 2% | Pain (VAS) during repair of wound | Evaluate |
| 50/50 | |||||||
| Harman et al., 2013 [25] | n = 203 | Suture | Wounds | LET (lidocaine, epinephrine, tetracaine) | placebo | Pain (VAS) | No Evaluate |
| 105/98 | Face Scale of Pain (FSP) | ||||||
| Jenkins, 2010 [26] | n = 110 | Suture | Wounds | Topical lidocaine 4% | Lidocaine infiltrated 1% | Pain (VAS) | Evaluate: Wound infecction |
| 56/54 | Wound dehiscence | ||||||
| Resuture | |||||||
| Kargi et al., 2010 [27] | n = 30 | wound management | Burns | Lidocaine-prilocaine 5% | antibiotic cream | verbal Numerical Rating Scale (NRS) | No Evaluate |
| 15/15 | |||||||
| Kasaj et al., 2007 [28] | n = 40 | wound management | Chronic periodontitis | Lidocaine 20 mg/g gel | placebo | Pain (VAS) | Evaluate |
| 20/20 | |||||||
| Tseng et al., 2017 [19] | n = 60 | Staple removal | Surgical wounds on the knee | Lidocaine patch 5% (700 mg patch) | Placebo patch | Pain (VAS) | Evaluate: skin allergy wound infection |
| 30/30 | |||||||
| Waldman et al., 2014 [20] | n = 93 | Pain management | Corneal abrasions | Tetracaine 1% | Normal saline | Pain (VAS) | Evaluate |
| 46/47 | |||||||
| KERRYPNX | Intervention | Outcomes | ||||
|---|---|---|---|---|---|---|
| Primary | Secondary | |||||
| Pain | Adverse Effects | |||||
| Author and Year | Intervention 1 (EG) | Intervention 2 (CG) | EG | CG | EG | CG |
| Christensen et al., 2013 [18] | Lidocaine 1% | Normal saline | During remove (−2.4) p < 0.001. | Not evaluate | ||
| 5 min: (−2) p: 0.001. | ||||||
| 10 min: (−1.5) p: 0.036. | ||||||
| 20 min: (−1.8) p: 0.004 | ||||||
| Descroix et al., 2011 [22] | Lidocaine cream 1% | Placebo cream | VAS: T0: 55.3 (±8.4) | VAS: T0: 57.2 (±10.6) | Not evaluate | |
| VAS: T3: 25.9 (±17.6) | VAS: T3: 42.5 (±15.5) | |||||
| Harman et al., 2013 [25] | LET (lidocaine, epinephrine, tetracaine) | Placebo | VAS: 0.5 † | VAS: 1 † | Not evaluate | |
| FSP: 0 † | FSP: 2 † | |||||
| Kasaj et al., 2007 [28] | Lidocaine 20 mg/g gel | Placebo | VAS: during: 5.2 (±1.4) | VAS: during: 5.5 (±1.4) | No adverse effects | |
| VAS: 10 min: 0.3 (±0.1) | VAS: 10 min: 3.2 (±1.9) | |||||
| VAS: 20 min: 0.3 | VAS: 20 min: 2.1 (±1.6) | |||||
| VAS: 30 min: 0.3 | VAS: 30 min: 1.7 (±1) | |||||
| Tseng et al., 2017 [19] | Lidocaine patch 5% (700 mg patch) | Placebo patch | VAS: 4.7 (±1.6) | VAS: 6.5 (±1.9) | No adverse effects | |
| Waldman et al., 2014 [20] | Tetracaine 1% | Normal saline | VAS: baseline 5.46 | VAS: baseline: 4.8 | Retained rust rings: 22%. | Retained rust rings: 17.5%, p = 0.544) |
| Flurescein uptake: 23.9% | Flurescein uptake: 21.3%, p = 0.761 | |||||
| Persitent symptoms: 21.7% | Persitent symptoms: 21.3%, p = 0.957) | |||||
| VAS: 24 h: difference 0.44 | VAS: 24 h: difference 0.44 | Persistent symptoms after a week: 2.2% | Persistent symptoms after a week: 8.5%, p = 0.176. | |||
| VAS: 48 h: difference 0.53 | VAS: 48 h: difference 0.53 | |||||
| Author and Year | Intervention | Outcomes | ||||
|---|---|---|---|---|---|---|
| Primary | Secondary | |||||
| Pain | Adverse Effects | |||||
| Intervention 1 (EG) | Intervention 2 (CG) | EG | CG | EG | CG | |
| Abbas et al., 2019 [17] | Lidocaine (25 mg/g) with prilocaine (25 mg/g) | mepivacaine infiltrated 2% | VAS: 3.86 (±1.59) | VAS: 5.99 (±1.47) | Tingling: 2.8% | Tingling: 0% |
| Swelling: 0% | Swelling: 2.8% | |||||
| Burning sensation: 1.4% | Burning sensation: 0% | |||||
| Claeys et al., 2010 [21] | Lidocaine (25 mg/g) with prilocaine (25 mg/g) | Nitrous oxide oxygen mixture inhalated 9−12 l/min (max. 30 min) | VAS: 3.68 (±0.25) | VAS: 5.29 (±0.27) | Not evaluate | |
| VRS: 1.71 (±0.15) | VRS: 2.87 (±0.15) | Not evaluate | ||||
| Franchi et al., 2009 [23] | Lidocaine (25 mg/g) with prilocaine (25 mg/g) | mepivacaine infiltrated 1% | VAS: 1.7 (±2.4) | VAS: 3.9 (±2.4) | Not evaluate | |
| Gaufberg et al., 2006 [24] | Topical lidocaine 5% with con epinephrine 0.025% | lidocaine infiltrated 2% | VAS: 0.16 (±0.46) | VAS: 0.2 (±0.49) | No adverse effects | |
| Jenkins, 2010 [26] | Topical lidocaine 4% | lidocaine infiltrated 1% | VAS: 1.49 (±1.76) | VAS: 0.78 (±1.12) | Wound infection: 3.7% Wound | Wound infection: 7.1% Wound |
| 3.7% Deshiscence | 0% Deshiscence | |||||
| 1.8% Resuture | 1.8% Resuture | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Rodriguez, J.M.; Suarez-Serrano, C.; Martin-Valero, R.; Marcen-Roman, Y.; de-la-Casa-Almeida, M. Effectiveness of Topical Anesthetics in Pain Management for Dermal Injuries: A Systematic Review. J. Clin. Med. 2021, 10, 2522. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112522
Navarro-Rodriguez JM, Suarez-Serrano C, Martin-Valero R, Marcen-Roman Y, de-la-Casa-Almeida M. Effectiveness of Topical Anesthetics in Pain Management for Dermal Injuries: A Systematic Review. Journal of Clinical Medicine. 2021; 10(11):2522. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112522
Chicago/Turabian StyleNavarro-Rodriguez, Juan Manuel, Carmen Suarez-Serrano, Rocio Martin-Valero, Yolanda Marcen-Roman, and Maria de-la-Casa-Almeida. 2021. "Effectiveness of Topical Anesthetics in Pain Management for Dermal Injuries: A Systematic Review" Journal of Clinical Medicine 10, no. 11: 2522. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112522