Effect of Possible Osteoporosis on Parenchymal-Type Hemorrhagic Transformation in Patients with Cardioembolic Stroke

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. Skull HU and BMD Registry
2.3. Measuring Frontal Skull HU Values
2.4. Radiographic and Clinical Variables
2.5. Statistical Methods
3. Results
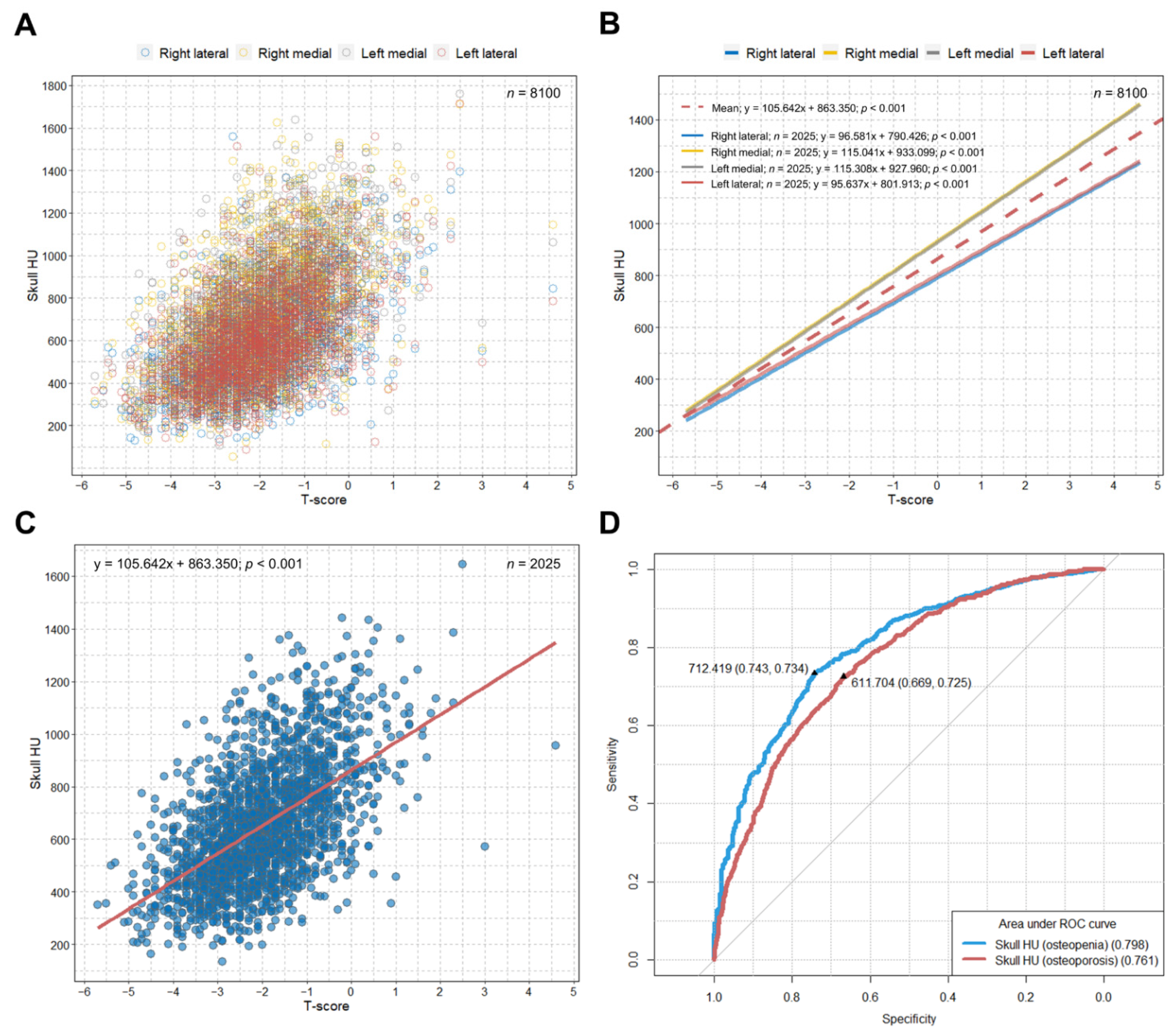
3.1. Optimal Skull HU Values Predicting Osteopenia and Osteoporosis
3.2. Characteristics of Patients in the Study Cohort
3.3. Skull HU Values and BMD in the Study and SHUB-Registry Cohorts
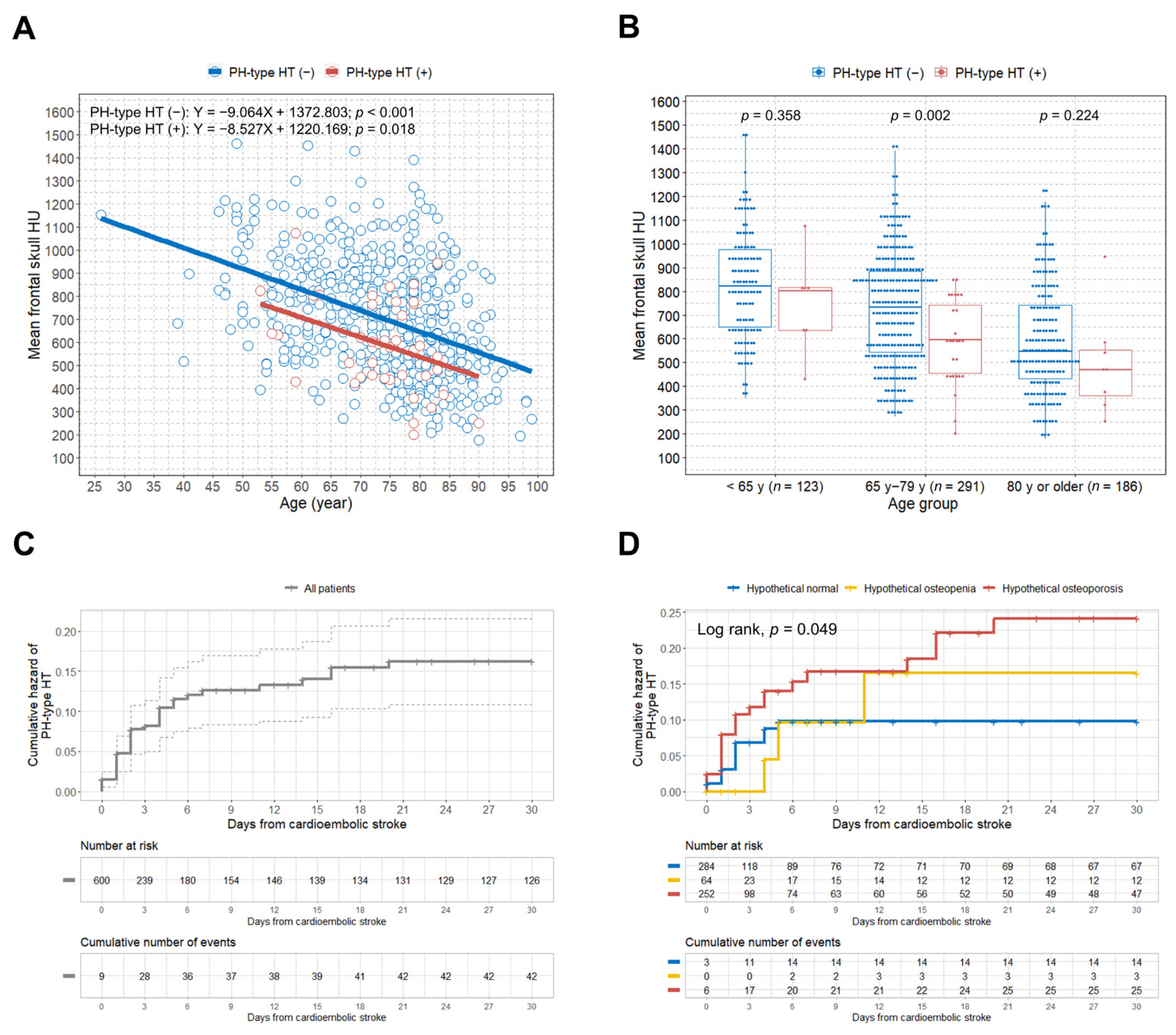
3.4. Relationship between Age and Skull HU according to the Development of PH-Type HT
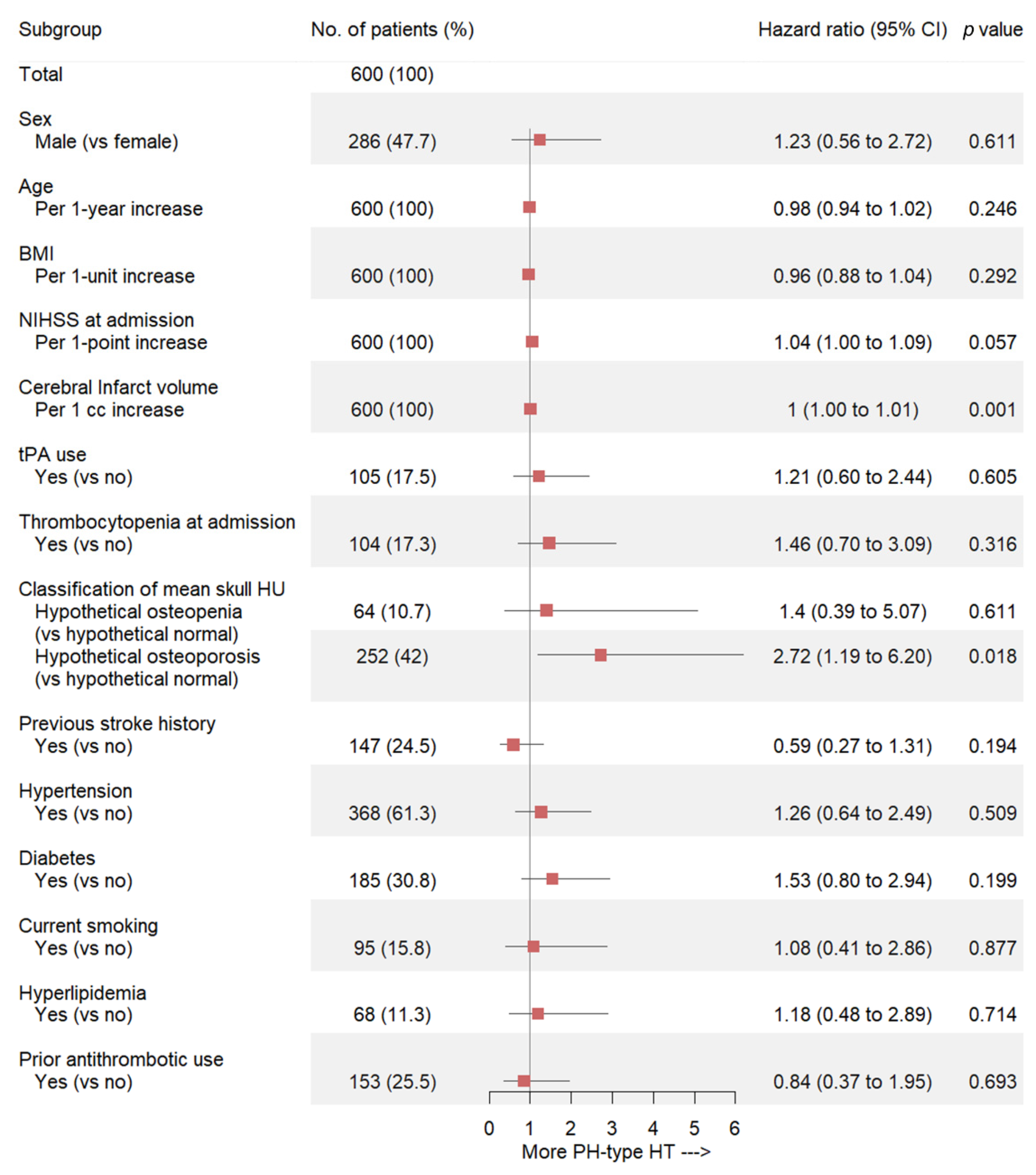
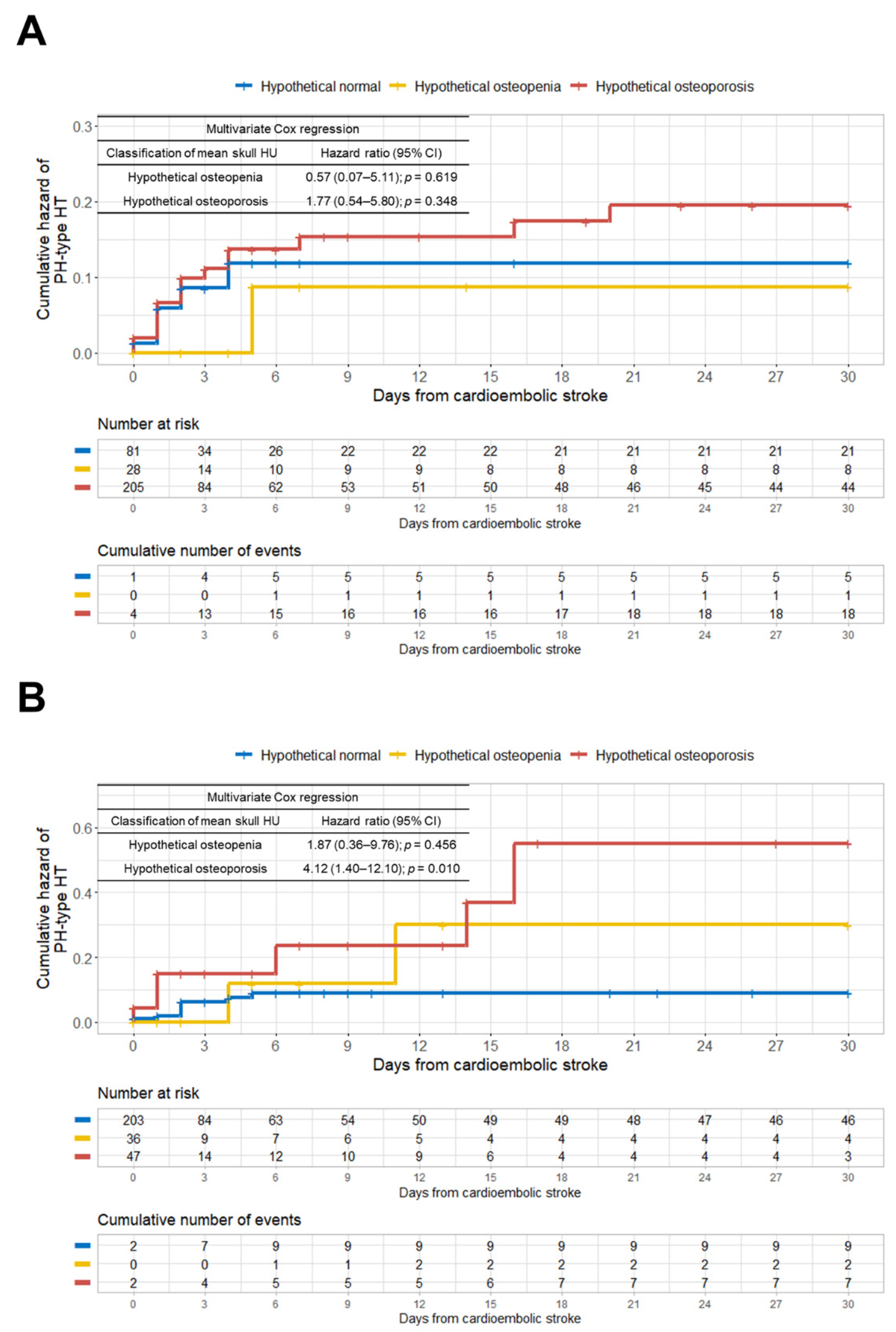
3.5. Association between Hypothetical Osteoporosis and PH-Type HT in Cardioembolic Stroke
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, J.; Yang, Y.; Sun, H.; Xing, Y. Hemorrhagic Transformation after Cerebral Infarction: Current Concepts and Challenges. Ann. Transl. Med. 2014, 2. [Google Scholar] [CrossRef]
- Fiorelli, M.; Bastianello, S.; von Kummer, R.; del Zoppo, G.J.; Larrue, V.; Lesaffre, E.; Ringleb, A.P.; Lorenzano, S.; Manelfe, C.; Bozzao, L. Hemorrhagic Transformation within 36 h of a Cerebral Infarct: Relationships with Early Clinical Deterioration and 3-Month Outcome in the European Cooperative Acute Stroke Study I (ECASS I) Cohort. Stroke 1999, 30, 2280–2284. [Google Scholar] [CrossRef]
- Pande, S.D.; Win, M.M.; Khine, A.A.; Zaw, E.M.; Manoharraj, N.; Lolong, L.; Tin, A.S. Haemorrhagic Transformation Following Ischaemic Stroke: A Retrospective Study. Sci. Rep. 2020, 10, 5319. [Google Scholar] [CrossRef] [Green Version]
- Berger, C.; Fiorelli, M.; Steiner, T.; Schäbitz, W.R.; Bozzao, L.; Bluhmki, E.; Hacke, W.; von Kummer, R. Hemorrhagic Transformation of Ischemic Brain Tissue: Asymptomatic or Symptomatic? Stroke 2001, 32, 1330–1335. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Park, K.-Y.; Shin, J.-H.; Cha, J.-K.; Kim, H.-Y.; Kwon, J.-H.; Oh, H.G.; Lee, K.B.; Kim, D.-E.; Ha, S.-W.; et al. Symptomatic Hemorrhagic Transformation and Its Predictors in Acute Ischemic Stroke with Atrial Fibrillation. Eur. Neurol. 2010, 64, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.F.; Reid, D.M.; Blake, G.; Herd, R.; Fogelman, I.; Ralston, S.H. Reduced Bone Density and Osteoporosis Associated with a Polymorphic Sp1 Binding Site in the Collagen Type I Alpha 1 Gene. Nat. Genet. 1996, 14, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Ha, B.J.; Bae, I.-S.; Kim, J.M.; Cheong, J.H.; Ryu, J.I.; Han, M.-H. Effects of Possible Osteoporotic Conditions on the Recurrence of Chronic Subdural Hematoma. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Oka, M.; Shimo, S.; Ohno, N.; Imai, H.; Abekura, Y.; Koseki, H.; Miyata, H.; Shimizu, K.; Kushamae, M.; Ono, I.; et al. Dedifferentiation of Smooth Muscle Cells in Intracranial Aneurysms and Its Potential Contribution to the Pathogenesis. Sci. Rep. 2020, 10, 8330. [Google Scholar] [CrossRef] [PubMed]
- Ponticos, M.; Partridge, T.; Black, C.M.; Abraham, D.J.; Bou-Gharios, G. Regulation of Collagen Type I in Vascular Smooth Muscle Cells by Competition between Nkx2.5 and DeltaEF1/ZEB1. Mol. Cell. Biol. 2004, 24, 6151–6161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10,172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Han, M.-H.; Won, Y.D.; Na, M.K.; Kim, C.H.; Kim, J.M.; Ryu, J.I.; Yi, H.-J.; Cheong, J.H. Association Between Possible Osteoporosis and Shunt-Dependent Hydrocephalus After Subarachnoid Hemorrhage. Stroke 2018, 49, 1850–1858. [Google Scholar] [CrossRef]
- Gourlay, M.L.; Fine, J.P.; Preisser, J.S.; May, R.C.; Li, C.; Lui, L.-Y.; Ransohoff, D.F.; Cauley, J.A.; Ensrud, K.E.; Study of Osteoporotic Fractures Research Group. Bone-Density Testing Interval and Transition to Osteoporosis in Older Women. N. Engl. J. Med. 2012, 366, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Won, Y.D.; Na, M.K.; Kim, C.H.; Kim, J.M.; Cheong, J.H.; Ryu, J.I.; Han, M.-H. The Frontal Skull Hounsfield Unit Value Can Predict Ventricular Enlargement in Patients with Subarachnoid Haemorrhage. Sci. Rep. 2018, 8, 10178. [Google Scholar] [CrossRef]
- Sims, J.R.; Gharai, L.R.; Schaefer, P.W.; Vangel, M.; Rosenthal, E.S.; Lev, M.H.; Schwamm, L.H. ABC/2 for Rapid Clinical Estimate of Infarct, Perfusion, and Mismatch Volumes. Neurology 2009, 72, 2104–2110. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Adair, L.S.; He, K.; Popkin, B.M. Optimal Cutoff Values for Overweight: Using Body Mass Index to Predict Incidence of Hypertension in 18- to 65-Year-Old Chinese Adults. J. Nutr. 2008, 138, 1377–1382. [Google Scholar] [CrossRef] [Green Version]
- Randolph, J.; Falbe, K.; Manuel, A.; Balloun, J. A Step-by-Step Guide to Propensity Score Matching in R. Pract. Assess. Res. Eval. 2019, 19. [Google Scholar] [CrossRef]
- Jain, S.; Self, W.H.; Wunderink, R.G.; Fakhran, S.; Balk, R.; Bramley, A.M.; Reed, C.; Grijalva, C.G.; Anderson, E.J.; Courtney, D.M.; et al. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. N. Engl. J. Med. 2015, 373, 415–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’ascanio, M.; Innammorato, M.; Pasquariello, L.; Pizzirusso, D.; Guerrieri, G.; Castelli, S.; Pezzuto, A.; De Vitis, C.; Anibaldi, P.; Marcolongo, A.; et al. Age Is Not the Only Risk Factor in COVID-19: The Role of Comorbidities and of Long Staying in Residential Care Homes. BMC Geriatr. 2021, 21, 63. [Google Scholar] [CrossRef] [PubMed]
- Alswat, K.A. Gender Disparities in Osteoporosis. J. Clin. Med. Res. 2017, 9, 382–387. [Google Scholar] [CrossRef] [Green Version]
- Biesheuvel, C.J.; Vergouwe, Y.; Oudega, R.; Hoes, A.W.; Grobbee, D.E.; Moons, K.G.M. Advantages of the Nested Case-Control Design in Diagnostic Research. BMC Med. Res. Methodol. 2008, 8, 48. [Google Scholar] [CrossRef] [Green Version]
- Hong, E.P.; Park, J.W. Sample Size and Statistical Power Calculation in Genetic Association Studies. Genom. Inform. 2012, 10, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Urata, M.; Kijima, Y.; Hirata, M.; Shinden, Y.; Arima, H.; Nakajo, A.; Koriyama, C.; Arigami, T.; Uenosono, Y.; Okumura, H.; et al. Computed Tomography Hounsfield Units Can Predict Breast Cancer Metastasis to Axillary Lymph Nodes. BMC Cancer 2014, 14, 730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tehlirian, C.V.; Bathon, J.M. Rheumatoid Arthritis. In Primer on the Rheumatic Diseases, 13th ed.; Klippel, J.H., Stone, J.H., Crofford, L.J., White, P.H., Eds.; Springer: New York, NY, USA, 2008; pp. 114–141. [Google Scholar]
- Pickhardt, P.J.; Pooler, B.D.; Lauder, T.; del Rio, A.M.; Bruce, R.J.; Binkley, N. Opportunistic Screening for Osteoporosis Using Abdominal Computed Tomography Scans Obtained for Other Indications. Ann. Intern. Med. 2013, 158, 588–595. [Google Scholar] [CrossRef]
- Choi, M.K.; Kim, S.M.; Lim, J.K. Diagnostic Efficacy of Hounsfield Units in Spine CT for the Assessment of Real Bone Mineral Density of Degenerative Spine: Correlation Study between T-Scores Determined by DEXA Scan and Hounsfield Units from CT. Acta Neurochir. 2016, 158, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.C.; Gausden, E.B.; Weiland, A.J.; Lane, J.M.; Schreiber, J.J. Using Hounsfield Units to Assess Osteoporotic Status on Wrist Computed Tomography Scans: Comparison With Dual Energy X-Ray Absorptiometry. J. Hand Surg. 2016, 41, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Upadhye, S.; Worster, A. Understanding Receiver Operating Characteristic (ROC) Curves. Can. J. Emerg. Med. 2006, 8, 19–20. [Google Scholar] [CrossRef]
- Brandi, M.L. Microarchitecture, the Key to Bone Quality. Rheumatol. Oxf. Engl. 2009, 48 (Suppl. 4), iv3–iv8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, T.L.; Ralston, S.H. Role of Genetic Factors in the Pathogenesis of Osteoporosis. J. Endocrinol. 2000, 166, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Grant, S.F.; Ralston, S.H. Genes and Osteoporosis. Trends Endocrinol. Metab. TEM 1997, 8, 232–236. [Google Scholar] [CrossRef]
- Gajko-Galicka, A. Mutations in Type I Collagen Genes Resulting in Osteogenesis Imperfecta in Humans. Acta Biochim. Pol. 2002, 49, 433–441. [Google Scholar] [CrossRef] [Green Version]
- Gooijer, K.; Rondeel, J.M.M.; van Dijk, F.S.; Harsevoort, A.G.J.; Janus, G.J.M.; Franken, A.A.M. Bleeding and Bruising in Osteogenesis Imperfecta: International Society on Thrombosis and Haemostasis Bleeding Assessment Tool and Haemostasis Laboratory Assessment in 22 Individuals. Br. J. Haematol. 2019, 187, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Mondal, R.K.; Mann, U.; Sharma, M. Osteogenesis Imperfecta with Bleeding Diathesis. Indian J. Pediatr. 2003, 70, 95–96. [Google Scholar] [CrossRef]
- Albayram, S.; Kizilkilic, O.; Yilmaz, H.; Tuysuz, B.; Kocer, N.; Islak, C. Abnormalities in the Cerebral Arterial System in Osteogenesis Imperfecta. AJNR Am. J. Neuroradiol. 2003, 24, 748–750. [Google Scholar]
- Rouvière, S.; Michelini, R.; Sarda, P.; Pagès, M. Spontaneous Carotid Artery Dissection in Two Siblings with Osteogenesis Imperfecta. Cerebrovasc. Dis. 2004, 17, 270–272. [Google Scholar] [CrossRef] [PubMed]
- Hirohata, T.; Miyawaki, S.; Mizutani, A.; Iwakami, T.; Yamada, S.; Nishido, H.; Suzuki, Y.; Miyamoto, S.; Hoya, K.; Murakami, M.; et al. Subarachnoid Hemorrhage Secondary to a Ruptured Middle Cerebral Aneurysm in a Patient with Osteogenesis Imperfecta: A Case Report. BMC Neurol. 2014, 14, 150. [Google Scholar] [CrossRef] [Green Version]
- Paciaroni, M.; Agnelli, G.; Corea, F.; Ageno, W.; Alberti, A.; Lanari, A.; Caso, V.; Micheli, S.; Bertolani, L.; Venti, M.; et al. Early Hemorrhagic Transformation of Brain Infarction: Rate, Predictive Factors, and Influence on Clinical Outcome: Results of a Prospective Multicenter Study. Stroke 2008, 39, 2249–2256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marini, S.; Morotti, A.; Ayres, A.M.; Crawford, K.; Kourkoulis, C.E.; Lena, U.K.; Gurol, E.M.; Viswanathan, A.; Goldstein, J.N.; Greenberg, S.M.; et al. Sex Differences in Intracerebral Hemorrhage Expansion and Mortality. J. Neurol. Sci. 2017, 379, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Center, J.R.; Nguyen, T.V.; Schneider, D.; Sambrook, P.N.; Eisman, J.A. Mortality after All Major Types of Osteoporotic Fracture in Men and Women: An Observational Study. Lancet Lond. Engl. 1999, 353, 878–882. [Google Scholar] [CrossRef]
- Roof, R.L.; Hall, E.D. Estrogen-Related Gender Difference in Survival Rate and Cortical Blood Flow after Impact-Acceleration Head Injury in Rats. J. Neurotrauma 2000, 17, 1155–1169. [Google Scholar] [CrossRef]
- O’Connor, C.A.; Cernak, I.; Vink, R. Both Estrogen and Progesterone Attenuate Edema Formation Following Diffuse Traumatic Brain Injury in Rats. Brain Res. 2005, 1062, 171–174. [Google Scholar] [CrossRef]
- Amantea, D.; Russo, R.; Bagetta, G.; Corasaniti, M.T. From Clinical Evidence to Molecular Mechanisms Underlying Neuroprotection Afforded by Estrogens. Pharmacol. Res. 2005, 52, 119–132. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PH-Type HT (−) | PH-Type HT(+) | Total | p |
|---|---|---|---|---|
| Number (%) | 558 (93.0) | 42 (7.0) | 600 (100) | |
| Time to PH-type HT development, median (IQR), day | N/A | 2.0 (1.0–4.0) | N/A | |
| Sex, male, n (%) | 268 (48.0) | 18 (42.9) | 286 (47.7) | 0.518 |
| Age, mean ± SD, y | 73.6 ± 11.1 | 73.6 ± 8.4 | 73.6 ± 11.0 | 0.980 |
| BMI, mean ± SD, kg/m2 | 23.5 ± 4.0 | 23.0 ± 3.4 | 23.4 ± 4.0 | 0.449 |
| Height, mean ± SD, cm | 160.5 ± 9.1 | 159.2 ± 7.1 | 160.4 ± 9.0 | 0.344 |
| Weight, mean ± SD, kg | 60.9 ± 12.9 | 58.4 ± 9.8 | 60.7 ± 12.7 | 0.220 |
| NIHSS at admission, mean ± SD | 7.5 ± 7.0 | 12.3 ± 6.3 | 7.8 ± 7.1 | <0.001 |
| NIHSS at admission, median (IQR) | 5.0 (2.0–12.0) | 12.5 (7.0–17.0) | 5.0 (2.0–12.0) | <0.001 |
| Cerebral infarct volume, mean ± SD, cc | 39.5 ± 76.3 | 108.8 ± 103.5 | 44.4 ± 80.3 | <0.001 |
| tPA use, n (%) | 93 (16.7) | 12 (28.6) | 105 (17.5) | 0.050 |
| Platelet count at admission, mean ± SD, × 103/μL | 203.1 ± 66.0 | 199.6 ± 64.0 | 202.8 ± 65.8 | 0.744 |
| Mean frontal skull HU, mean ± SD | 705.9 ± 247.6 | 592.4 ± 197.6 | 698.0 ± 246.0 | 0.004 |
| Classification of mean skull HU, n (%) | 0.058 | |||
| Hypothetical normal (>712.4) | 270 (48.4) | 14 (33.3) | 284 (47.3) | |
| Hypothetical osteopenia (>611.7 and ≤712.4) | 61 (10.9) | 3 (7.1) | 64 (10.7) | |
| Hypothetical osteoporosis (≤611.7) | 227 (40.7) | 25 (59.5) | 252 (42.0) | |
| Heart disease, n (%) | 0.375 | |||
| Arrhythmia | 399 (71.5) | 36 (85.7) | 435 (72.5) | |
| CHF, cardiomyopathy, valvular heart disease | 90 (16.1) | 3 (7.1) | 93 (15.5) | |
| Coronary artery disease | 34 (6.1) | 1 (2.4) | 35 (5.8) | |
| Previous MI | 34 (6.1) | 2 (4.8) | 36 (6.0) | |
| Cardiac myxoma | 1 (0.2) | 0 | 1 (0.2) | |
| Past medical history, n (%) | ||||
| Previous stroke history | 139 (24.9) | 8 (19.0) | 147 (24.5) | 0.394 |
| Hypertension | 340 (60.9) | 28 (66.7) | 368 (61.3) | 0.462 |
| Diabetes | 169 (30.3) | 16 (38.1) | 185 (30.8) | 0.291 |
| Current smoking | 88 (15.8) | 7 (16.7) | 95 (15.8) | 0.878 |
| Hyperlipidemia | 62 (11.1) | 6 (14.3) | 68 (11.3) | 0.531 |
| Prior antithrombotic use | 146 (26.2) | 7 (16.7) | 153 (25.5) | 0.173 |
| Variables | Study Cohort | SHUB Registry |
|---|---|---|
| Number | 600 | 2025 |
| Sex | ||
| Female, n (%) | 314 (52.3) | 1704 (84.1) |
| Age, median (IQR), y | 75.5 (67.0–81.0) | 69.0 (59.0–77.0) |
| Age, mean ± SD, y | 73.6 ± 11.0 | 67.9 ± 11.9 |
| Overall mean skull HU value, median (IQR) | 681.0 (507.6–872.6) | 625.7 (483.8–791.5) |
| Overall mean skull HU value, mean ± SD | 698.0 ± 246.0 | 653.0 ± 229.9 |
| Mean HU value at each of four sites in the frontal skull, mean ± SD | ||
| Right lateral | 642.9 ± 224.5 | 598.1 ± 220.4 |
| Right medial | 763.3 ± 294.0 | 704.1 ± 263.6 |
| Left medial | 750.0 ± 289.1 | 698.4 ± 262.4 |
| Left lateral | 635.8 ± 230.6 | 611.5 ± 224.8 |
| Average, medial | 756.7 ± 286.9 | 701.2 ± 257.9 |
| Average, lateral | 639.3 ± 221.0 | 604.8 ± 216.5 |
| Time interval between brain CT and BMD, median (IQR), days | N/A | 151.0 (9.0–487.0) |
| T-score, mean ± SD | N/A | −1.99 ± 1.22 |
| Lumbar spine | N/A | −1.65 ± 1.43 |
| Femur neck | N/A | −1.40 ± 1.20 |
| BMD categories, n (%) | ||
| Normal (T-score > −1.0) | N/A | 381 (18.8) |
| Osteopenia (T-score > −2.5 and ≤ 1.0) | N/A | 902 (44.5) |
| Osteoporosis (T-score ≤ −2.5) | N/A | 742 (36.6) |
| Characteristics | Before Propensity Score Matching | After Propensity Score Matching | ||||
|---|---|---|---|---|---|---|
| PH-Type HT (−) (n = 558) | PH-Type HT (+) (n = 42) | p | PH-Type HT (−) (n = 84) | PH-Type HT (+) (n = 42) | p | |
| Sex, male, n (%) | 268 (48.0) | 18 (42.9) | 0.518 | 37 (44.0) | 18 (42.9) | 0.899 |
| Age, mean ± SD, y | 73.6 ± 11.1 | 73.6 ± 8.4 | 0.980 | 75.1 ± 10.7 | 73.6 ± 8.4 | 0.434 |
| NIHSS at admission, mean ± SD | 7.5 ± 7.0 | 12.3 ± 6.3 | <0.001 | 13.7 ± 6.3 | 12.3 ± 6.3 | 0.226 |
| NIHSS at admission, median (IQR) | 5.0 (2.0–12.0) | 12.5 (7.0–17.0) | <0.001 | 13.5 (10.0–18.0) | 12.5 (7.0–17.0) | 0.226 |
| Cerebral infarct volume, mean ± SD, cc | 39.5 ± 76.3 | 108.8 ± 103.5 | <0.001 | 92.0 ± 103.3 | 108.8 ± 103.5 | 0.390 |
| Cerebral infarct volume, median (IQR) | 6.7 (0.4–40.6) | 88.5 (17.4–166.3) | <0.001 | 52.6 (11.0–133.4) | 88.5 (17.4–166.3) | 0.390 |
| Classification of mean skull HU, n (%) | 0.058 | 0.376 | ||||
| Hypothetical normal (>712.4) | 270 (48.4) | 14 (33.3) | 38 (45.2) | 14 (33.3) | ||
| Hypothetical osteopenia (>611.7 and ≤712.4) | 61 (10.9) | 3 (7.1) | 7 (8.3) | 3 (7.1) | ||
| Hypothetical osteoporosis (≤611.7) | 227 (40.7) | 25 (59.5) | 39 (46.4) | 25 (59.5) | ||
| Total (n = 126) | Female (n = 71) | Male (n = 55) | ||||
|---|---|---|---|---|---|---|
| Variable | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p |
| Sex | ||||||
| Male | 1.21 (0.57–2.56) | 0.618 | N/A | N/A | ||
| Female | Reference | N/A | N/A | |||
| Age (per 1–year increase) | 0.98 (0.95–1.02) | 0.296 | 0.98 (0.94–1.03) | 0.493 | 0.99 (0.94–1.04) | 0.663 |
| NIHSS at admission (per 1–point increase) | 0.96 (0.91–1.02) | 0.189 | 0.89 (0.81–0.98) | 0.015 | 1.02 (0.95–1.09) | 0.616 |
| Cerebral infarct volume (per 1 cc increase) | 1.00 (1.00–1.00) | 0.351 | 1.00 (1.00–1.01) | 0.091 | 1.00 (0.99–1.00) | 0.678 |
| Classification of mean skull HU, n (%) | ||||||
| Hypothetical normal (>712.4) | Reference | Reference | Reference | |||
| Hypothetical osteopenia (>611.7 and ≤712.4) | 1.29 (0.36–4.55) | 0.697 | 2.12 (0.23–19.94) | 0.511 | 1.23 (0.26–5.92) | 0.795 |
| Hypothetical osteoporosis (≤611.7) | 2.24 (0.99–5.09) | 0.054 | 1.62 (0.49–5.33) | 0.429 | 3.29 (1.18–9.17) | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Won, Y.-D.; Kim, J.-M.; Cheong, J.-H.; Ryu, J.-I.; Koh, S.-H.; Han, M.-H. Effect of Possible Osteoporosis on Parenchymal-Type Hemorrhagic Transformation in Patients with Cardioembolic Stroke. J. Clin. Med. 2021, 10, 2526. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112526
Won Y-D, Kim J-M, Cheong J-H, Ryu J-I, Koh S-H, Han M-H. Effect of Possible Osteoporosis on Parenchymal-Type Hemorrhagic Transformation in Patients with Cardioembolic Stroke. Journal of Clinical Medicine. 2021; 10(11):2526. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112526
Chicago/Turabian StyleWon, Yu-Deok, Jae-Min Kim, Jin-Hwan Cheong, Je-Il Ryu, Seong-Ho Koh, and Myung-Hoon Han. 2021. "Effect of Possible Osteoporosis on Parenchymal-Type Hemorrhagic Transformation in Patients with Cardioembolic Stroke" Journal of Clinical Medicine 10, no. 11: 2526. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112526