
Comparison of Implant Stability between Regenerated and Non-Regenerated Bone. A Prospective Cohort Study


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
2.3. Sample Size
2.4. Pre-Surgery Phase
2.5. Surgical Phase
2.6. Stability Measurements
2.7. Statistical Analysis
3. Results
3.1. Descriptive Analysis
3.2. Clinical Parameters
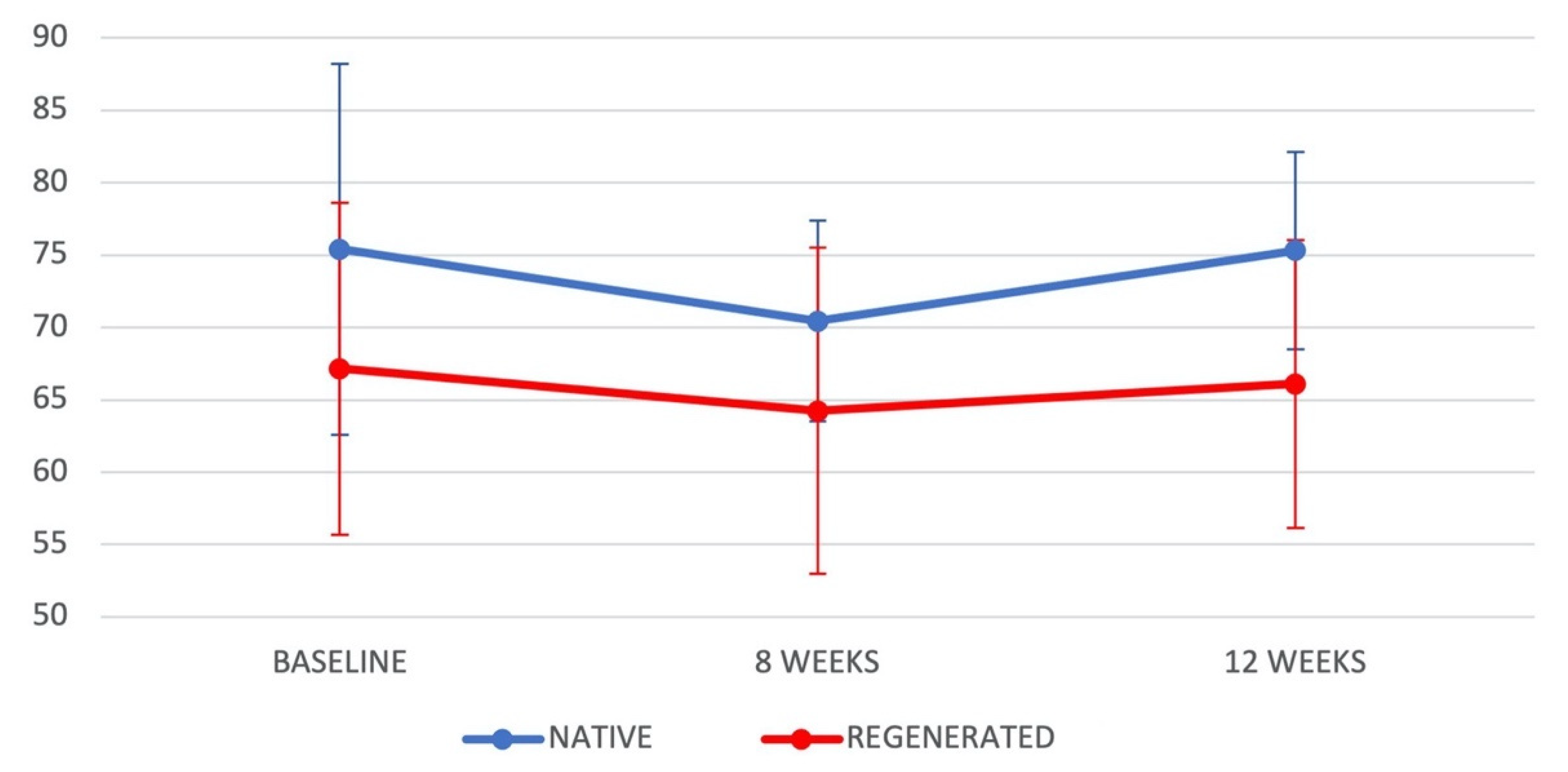
3.2.1. Bone Type (Native vs. Regenerated)
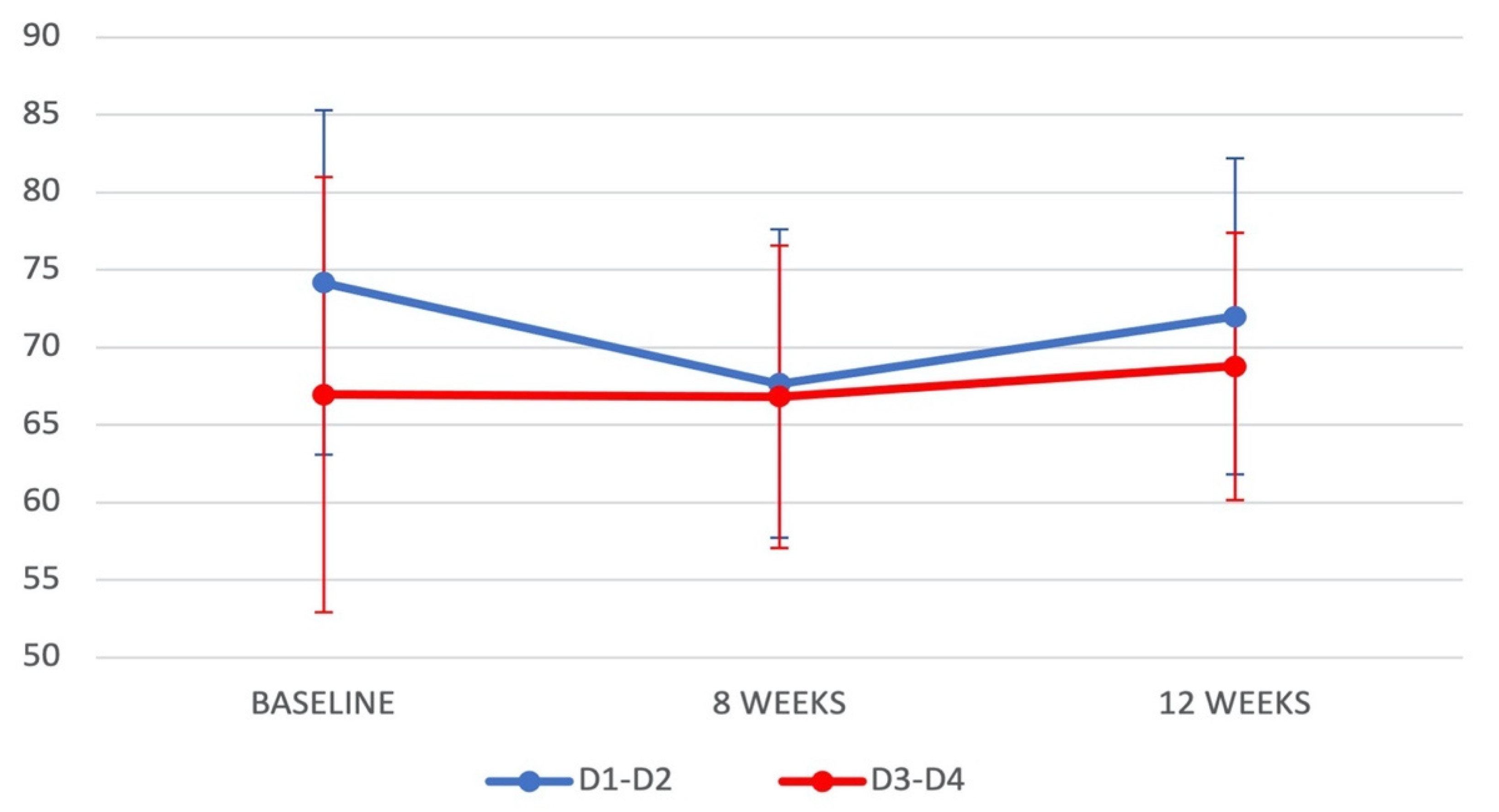
3.2.2. Bone Quality (D1–D2 vs. D3–D4)
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brånemark, P.I.; Hansson, B.O.; Adell, R.; Breine, U.; Lindström, J.; Hallén, O.; Ohman, A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-Year Period. Scand. J. Plast Reconstr. Surg. Suppl. 1977, 16, 1–132. [Google Scholar]
- Trindade, R.; Albrektsson, T.; Galli, S.; Prgomet, Z.; Tengvall, P.; Wennerberg, A. Osseointegration and foreign body reaction: Titanium implants activate the immune system and suppress bone resorption during the first 4 weeks after implantation. Clin. Implant. Dent. Relat. Res. 2018, 20, 82–91. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. On osseointegration in relation to implant surfaces. Clin. Implant. Dent. Relat. Res. 2019, 21 (Suppl. 1), 4–7. [Google Scholar] [CrossRef] [Green Version]
- Meredith, N. Assessment of Implant stability as a prognostic determinant. Int. J. Prosthodont. 1998, 11, 491–501. [Google Scholar]
- Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Xhajanka, E.; Romeo, D.M.; Romeo, M.; Zappone, C.M.F.; Malcangi, G.; Scarano, A.; Lorusso, F.; et al. The effectiveness of osseodensification drilling protocol for implant site osteotomy: A systematic review of the literature and meta-analysis. Materials 2021, 14, 1147. [Google Scholar] [CrossRef] [PubMed]
- Adell, R.; Eriksson, B.; Lekholm, U.; Brånemark, P.I.; Jemt, T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int. J. Oral Maxillofac. Implant. 1990, 5, 347–359. [Google Scholar]
- Quesada-García, M.-P.; Prados-Sánchez, E.; Olmedo-Gaya, M.-V.; Muñoz-Soto, E.; González-Rodríguez, M.-P.; Valllecillo-Capilla, M. Measurement of dental implant stability by resonance frequency analysis: A review of the literature. Med. Oral Patol. Oral Cir. Bucal 2009, 14, e538–e546. [Google Scholar] [CrossRef] [Green Version]
- Guo, C.Y.; Matinlinna, J.P.; Tang, A.T.H. Effects of surface charges on dental implants: Past, present, and future. Int. J. Biomater. 2012, 2012, 381535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javed, F.; Ahmed, H.B.; Crespi, R.; Romanos, G.E. Role of primary stability for successful osseointegration of dental implants: Factors of influence and evaluation. Interv. Med. Appl. Sci. 2013, 5, 162–167. [Google Scholar] [CrossRef]
- Lozano-Carrascal, N.; Salomó-Coll, O.; Gilabert-Cerdà, M.; Farré-Pagés, N.; Gargallo-Albiol, J.; Hernández-Alfaro, F. Effect of implant macro-design on primary stability: A prospective clinical study. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e214–e221. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Wu, G.; Hunziker, E. The clinical significance of Implant Stability Quotient (ISQ) measurements: A literature review. J. Oral Biol. Craniofac. Res. 2020, 10, 629–638. [Google Scholar] [CrossRef]
- Daher, F.I.; Abi-Aad, H.L.; Dimassi, H.I.; Baba, N.Z.; Majzoub, Z.A. Factors affecting implant stability quotients at immediately and conventionally loaded implants in the posterior maxilla: A split-mouth randomized controlled trial. J. Prosthodont. 2020. [Google Scholar] [CrossRef]
- Rozé, J.; Babu, S.; Saffarzadeh, A.; Gayet-Delacroix, M.; Hoornaert, A.; Layrolle, P. Correlating Implant stability to bone structure. Clin. Oral Implant. Res. 2009, 20, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Moreno, F.J.; Herrera-Briones, F.J.; Bassam, T.; Vallecillo-Capilla, M.F.; Reyes-Botella, C. Factors affecting dental implant stability measured using the ostell mentor device: A systematic review. Implant. Dent. 2015, 24, 565–577. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Lim, Y.-J.; Kim, B.; Lee, J. How Do Parameters of implant primary stability correspond with CT-evaluated bone quality in the posterior maxilla? A correlation analysis. Materials 2021, 14, 270. [Google Scholar] [CrossRef]
- Sennerby, L.; Meredith, N. Implant Stability Measurements Using Resonance Frequency Analysis: Biological and Biomechanical Aspects and Clinical Implications. Periodontol. 2020 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Coulthard, P.; Worthington, H.V. The efficacy of various bone augmentation procedures for dental implants: A cochrane systematic review of randomized controlled clinical trials. Int. J. Oral Maxillofac. Implant. 2006, 21, 696–710. [Google Scholar]
- Kola, M.Z.; Shah, A.H.; Khalil, H.S.; Rabah, A.M.; Harby, N.M.H.; Sabra, S.A.; Raghav, D. Surgical templates for dental implant positioning; current knowledge and clinical perspectives. Niger. J. Surg. 2015, 21, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Dos Anjos, T.L.M.R.; de Molon, R.S.; Paim, P.R.F.; Marcantonio, E.; Marcantonio, E.; Faeda, R.S. Implant stability after sinus floor augmentation with deproteinized bovine bone mineral particles of different sizes: A prospective, randomized and controlled split-mouth clinical trial. Int. J. Oral Maxillofac. Surg. 2016, 45, 1556–1563. [Google Scholar] [CrossRef] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE initiative the strengthening the reporting of observational studies in epidemiology (strobe) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [Green Version]
- Brånemark, P.-I.; Zarb, G.A.; Albrektsson, T. Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry; Quintessence: Chicago, IL, USA, 1985; ISBN 978-0-86715-129-9. [Google Scholar]
- Alghamdi, H.S. Methods to improve osseointegration of dental implants in low quality (Type-IV) bone: An overview. J. Funct. Biomater. 2018, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Atieh, M.A.; Baqain, Z.H.; Tawse-Smith, A.; Ma, S.; Almoselli, M.; Lin, L.; Alsabeeha, N.H.M. The influence of insertion torque values on the failure and complication rates of dental implants: A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2021, 23, 341–360. [Google Scholar] [CrossRef] [PubMed]
- Zita Gomes, R.; de Vasconcelos, M.R.; Lopes Guerra, I.M.; de Almeida, R.A.B.; de Campos Felino, A.C. Implant stability in the posterior maxilla: A Controlled clinical trial. BioMed Res. Int. 2017, 2017, 6825213. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Daprile, G.; Piattelli, A.; Carinci, F. Evaluation of factors influencing resonance frequency analysis values, at insertion surgery, of implants placed in sinus-augmented and nongrafted sites. Clin. Implant. Dent. Relat. Res. 2007, 9, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Deli, G.; Petrone, V.; De Risi, V.; Tadic, D.; Zafiropoulos, G.-G. Longitudinal implant stability measurements based on resonance frequency analysis after placement in healed or regenerated bone. J. Oral Implant. 2014, 40, 438–447. [Google Scholar] [CrossRef]
- Araújo, M.G.; Lindhe, J. Ridge Alterations following tooth extraction with and without flap elevation: An experimental study in the dog. Clin. Oral Implant. Res. 2009, 20, 545–549. [Google Scholar] [CrossRef]
- Artzi, Z.; Tal, H.; Dayan, D. Porous bovine bone mineral in healing of human extraction sockets. Part 1: Histomorphometric evaluations at 9 months. J. Periodontol. 2000, 71, 1015–1023. [Google Scholar] [CrossRef]
- Carmagnola, D.; Adriaens, P.; Berglundh, T. Healing of human extraction sockets filled with Bio-Oss. Clin. Oral Implant. Res. 2003, 14, 137–143. [Google Scholar] [CrossRef]
- Heinemann, F.; Hasan, I.; Bourauel, C.; Biffar, R.; Mundt, T. Bone stability around dental implants: Treatment related factors. Ann. Anat. 2015, 199, 3–8. [Google Scholar] [CrossRef]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of collagen membranes for bone regeneration: A literature review. Materials 2020, 13, 786. [Google Scholar] [CrossRef] [Green Version]
- Di Lallo, S.; Ricci, L.; Orecchioni, S.; Piattelli, A.; Iezzi, G.; Perrotti, V. Resonance frequency analysis assessment of implants placed with a simultaneous or a delayed approach in grafted and nongrafted sinus sites: A 12-month clinical study. Clin. Implant. Dent. Relat. Res. 2014, 16, 394–400. [Google Scholar] [CrossRef]
- Beck, T.M.; Mealey, B.L. Histologic analysis of healing after tooth extraction with ridge preservation using mineralized human bone allograft. J. Periodontol. 2010, 81, 1765–1772. [Google Scholar] [CrossRef] [Green Version]
- Monje, A.; Suarez, F.; Garaicoa, C.A.; Monje, F.; Galindo-Moreno, P.; García-Nogales, A.; Wang, H.-L. Effect of location on primary stability and healing of dental implants. Implant. Dent. 2014, 23, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Sim, C.P.C.; Lang, N.P. Factors influencing resonance frequency analysis assessed by osstell mentor during implant tissue integration: I. instrument positioning, bone structure, implant length. Clin. Oral Implant. Res. 2010, 21, 598–604. [Google Scholar] [CrossRef]
- O’Sullivan, D.; Sennerby, L.; Jagger, D.; Meredith, N. A comparison of two methods of enhancing implant primary stability. Clin. Implant. Dent. Relat. Res. 2004, 6, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.-G.; Heo, S.-J.; Koak, J.-Y.; Kim, S.-K.; Lee, S.-Y. Effect of bone quality and implant surgical technique on Implant Stability Quotient (ISQ) value. J. Adv. Prosthodont. 2011, 3, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Farré-Pagés, N.; Augé-Castro, M.L.; Alaejos-Algarra, F.; Mareque-Bueno, J.; Ferrés-Padró, E.; Hernández-Alfaro, F. Relation between bone density and primary implant stability. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e62–e67. [Google Scholar] [CrossRef] [Green Version]
- Herekar, M.; Sethi, M.; Ahmad, T.; Fernandes, A.S.; Patil, V.; Kulkarni, H. A Correlation between Bone (B), Insertion Torque (IT), and Implant Stability (S): BITS Score. J. Prosthet. Dent. 2014, 112, 805–810. [Google Scholar] [CrossRef]
- Valiyaparambil, J.V.; Yamany, I.; Ortiz, D.; Shafer, D.M.; Pendrys, D.; Freilich, M.; Mallya, S.M. Bone quality evaluation: Comparison of cone beam computed tomography and subjective surgical assessment. Int. J. Oral Maxillofac. Implant. 2012, 27, 1271–1277. [Google Scholar]
- Fanali, S.; Tumedei, M.; Pignatelli, P.; Inchingolo, F.; Pennacchietti, P.; Pace, G.; Piattelli, A. Implant primary stability with an osteocondensation drilling protocol in different density polyurethane blocks. Comput. Methods Biomech. Biomed. Eng. 2020, 14–20. [Google Scholar] [CrossRef]
- Comuzzi, L.; Tumedei, M.; Pontes, A.E.; Piattelli, A.; Iezzi, G. Primary stability of dental implants in low-density (10 and 20 pcf) polyurethane foam blocks: Conical vs. cylindrical implants. Int. J. Environ. Res. Public Health 2020, 17, 2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tumedei, M.; Piattelli, A.; Degidi, M.; Mangano, C.; Iezzi, G. A 30-Year (1988–2018) Retrospective Microscopical Evaluation of Dental Implants Retrieved for Different Causes: A Narrative Review. Int. J. Periodontics Restor. Dent. 2020, 40, e211–e227. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Piattelli, A. Primary Stability determination by means of insertion torque and RFA in a sample of 4135 implants. Clin. Implant. Dent. Relat. Res. 2012, 14, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.-Y.; Shin, S.-I.; Kye, S.-B.; Chang, S.-W.; Hong, J.; Paeng, J.-Y.; Yang, S.-M. Bone Cement grafting increases implant primary stability in circumferential cortical bone defects. J. Periodontal. Implant. Sci. 2015, 45, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsolaki, I.N.; Tonsekar, P.P.; Najafi, B.; Drew, H.J.; Sullivan, A.J.; Petrov, S.D. Comparison of osteotome and conventional drilling techniques for primary implant stability: An in vitro study. J. Oral Implant. 2016, 42, 321–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, A.; Marconcini, S.; Giammarinaro, E.; Mijiritsky, E.; Gelpi, F.; Covani, U. Clinical outcomes of implants placed in extraction sockets and immediately restored: A 7-year single-cohort prospective study. Clin. Implant. Dent. Relat. Res. 2016, 18, 1103–1112. [Google Scholar] [CrossRef]
- Buser, D.A.; Schroeder, A.; Sutter, F.; Lang, N.P. The new concept of iti hollow-cylinder and hollow-screw implants: Part 2. clinical aspects, indications, and early clinical results. Int. J. Oral Maxillofac. Implant. 1988, 3, 173–181. [Google Scholar]
- Lefkove, M.D.; Beals, R.P. Immediate loading of cylinder implants with overdentures in the mandibular symphysis: The Titanium Plasma-Sprayed Screw Technique. J. Oral Implant. 1990, 16, 265–271. [Google Scholar]
- Tarnow, D.P.; Emtiaz, S.; Classi, A. Immediate loading of threaded implants at stage 1 surgery in edentulous arches: Ten consecutive case reports with 1- to 5-year data. Int. J. Oral Maxillofac. Implant. 1997, 12, 319–324. [Google Scholar]
- Horiuchi, K.; Uchida, H.; Yamamoto, K.; Sugimura, M. Immediate loading of brånemark system implants following placement in edentulous patients: A clinical report. Int. J. Oral Maxillofac. Implant. 2000, 15, 824–830. [Google Scholar]
- Gapski, R.; Wang, H.-L.; Mascarenhas, P.; Lang, N.P. Critical review of immediate implant loading. Clin. Oral Implant. Res. 2003, 14, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Gatti, C.; Rossi, E.; Haefliger, W.; Markwalder, T.H. Implant-retained mandibular overdentures with immediate loading. a retrospective multicenter study on 226 consecutive cases. Clin. Oral Implant. Res. 1997, 8, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, I.; Nilson, H.; Lindh, T.; Nilner, K.; Randow, K. Immediate Functional loading of brånemark single tooth implants. an 18 months’ clinical pilot follow-up study. Clin. Oral Implant. Res. 2000, 11, 26–33. [Google Scholar] [CrossRef]
- Maló, P.; Rangert, B.; Dvärsäter, L. Immediate function of brånemark implants in the esthetic zone: A retrospective clinical study with 6 months to 4 years of follow-up. Clin. Implant. Dent. Relat. Res. 2000, 2, 138–146. [Google Scholar] [CrossRef]
- Park, K.-J.; Kwon, J.-Y.; Kim, S.-K.; Heo, S.-J.; Koak, J.-Y.; Lee, J.-H.; Lee, S.-J.; Kim, T.-H.; Kim, M.-J. The Relationship between implant stability quotient values and implant insertion variables: A clinical study. J. Oral Rehabil. 2012, 39, 151–159. [Google Scholar] [CrossRef]
- Gehrke, S.A.; da Silva, U.T.; Del Fabbro, M. Does implant design affect implant primary stability? A resonance frequency analysis-based randomized split-mouth clinical trial. J. Oral Implant. 2015, 41, e281–e286. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Implants | |||
|---|---|---|---|
| (n) | (%) | ||
| Sex | Male | 28 | 46.7 |
| Female | 32 | 53.3 | |
| Implant diameter | 3.7 | 24 | 40 |
| 4.1 | 36 | 60 | |
| Implant site | Maxillary anterior | 6 | 10 |
| Maxillary posterior | 17 | 28.3 | |
| Mandibular anterior | 5 | 8.3 | |
| Mandibular posterior | 32 | 53.3 | |
| Bone quality * | D1–D2 | 36 | 60 |
| D3–D4 | 24 | 40 | |
| Bone Type | |||||||
|---|---|---|---|---|---|---|---|
| n (Mean ± SD) | Standard Error | Median | Minimum | Maximum | p-Value | ||
| ISQ Baseline | Native | 30 (75.40 ± 12.80) | 2.34 | 76.50 | 25.00 | 91.00 | 0.011 * |
| Regenerated | 30 (67.17 ± 11.47) | 2.09 | 64.50 | 47.00 | 85.00 | ||
| ISQ 8 weeks | Native | 30 (70.43 ± 6.93) | 1.26 | 71.00 | 57.00 | 83.00 | 0.013 * |
| Regenerated | 30 (64.23 ± 11.27) | 2.06 | 62.50 | 44.00 | 88.00 | ||
| ISQ 12 weeks | Native | 30 (75.33 ± 6.82) | 1.25 | 75.50 | 63.00 | 87.00 | 0.000 * |
| Regenerated | 30 (66.10 ± 9.93) | 1.81 | 67.00 | 49.00 | 85.00 | ||
| Bone Quality | |||||||
|---|---|---|---|---|---|---|---|
| n (Mean ± SD) | Standard Error | Median | Minimum | Maximum | p-Value | ||
| ISQ Baseline | D1–D2 | 36 (74.17 ± 11.10) | 1.85 | 73.50 | 49.00 | 91.00 | 0.031 * |
| D3–D4 | 24 (66.96 ± 14.02) | 2.86 | 70.00 | 25.00 | 84.00 | ||
| ISQ 8 weeks | D1–D2 | 36 (67.67 ± 9.93) | 1.66 | 70.00 | 44.00 | 87.00 | 0.750 * |
| D3–D4 | 24 (66.83 ± 9.75) | 1.99 | 67.50 | 50.00 | 88.00 | ||
| ISQ 12 weeks | D1–D2 | 36 (72.00 ± 10.18) | 1.70 | 73.50 | 50.00 | 87.00 | 0.209 * |
| D3–D4 | 24 (68.79 ± 8.63) | 1.76 | 70.50 | 49.00 | 81.00 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallecillo-Rivas, M.; Reyes-Botella, C.; Vallecillo, C.; Lisbona-González, M.J.; Vallecillo-Capilla, M.; Olmedo-Gaya, M.V. Comparison of Implant Stability between Regenerated and Non-Regenerated Bone. A Prospective Cohort Study. J. Clin. Med. 2021, 10, 3220. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153220
Vallecillo-Rivas M, Reyes-Botella C, Vallecillo C, Lisbona-González MJ, Vallecillo-Capilla M, Olmedo-Gaya MV. Comparison of Implant Stability between Regenerated and Non-Regenerated Bone. A Prospective Cohort Study. Journal of Clinical Medicine. 2021; 10(15):3220. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153220
Chicago/Turabian StyleVallecillo-Rivas, Marta, Candela Reyes-Botella, Cristina Vallecillo, María Jesús Lisbona-González, Manuel Vallecillo-Capilla, and María Victoria Olmedo-Gaya. 2021. "Comparison of Implant Stability between Regenerated and Non-Regenerated Bone. A Prospective Cohort Study" Journal of Clinical Medicine 10, no. 15: 3220. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153220